
No Association of Hair Zinc Concentration with Coronary Artery Disease Severity and No Relation with Acute Coronary Syndromes

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Coronary Angiography
2.3. Laboratory Tests
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
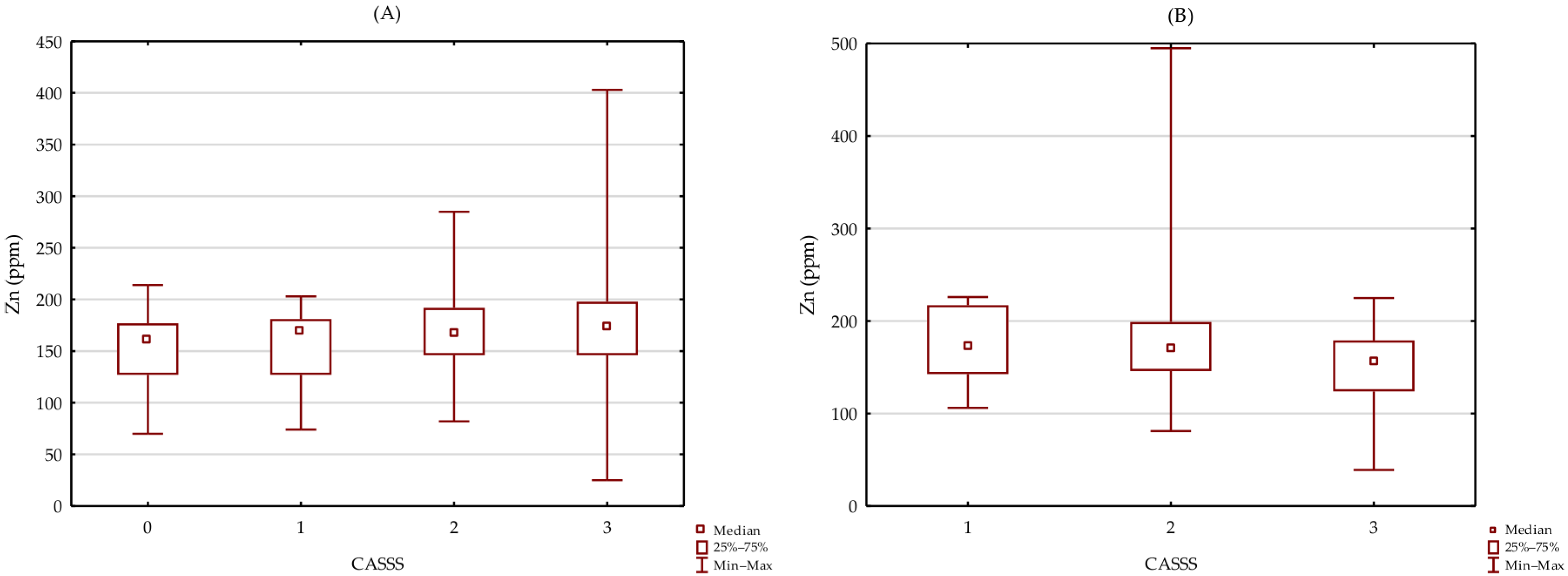
3.2. Association between Zn Level and Severity of CAD
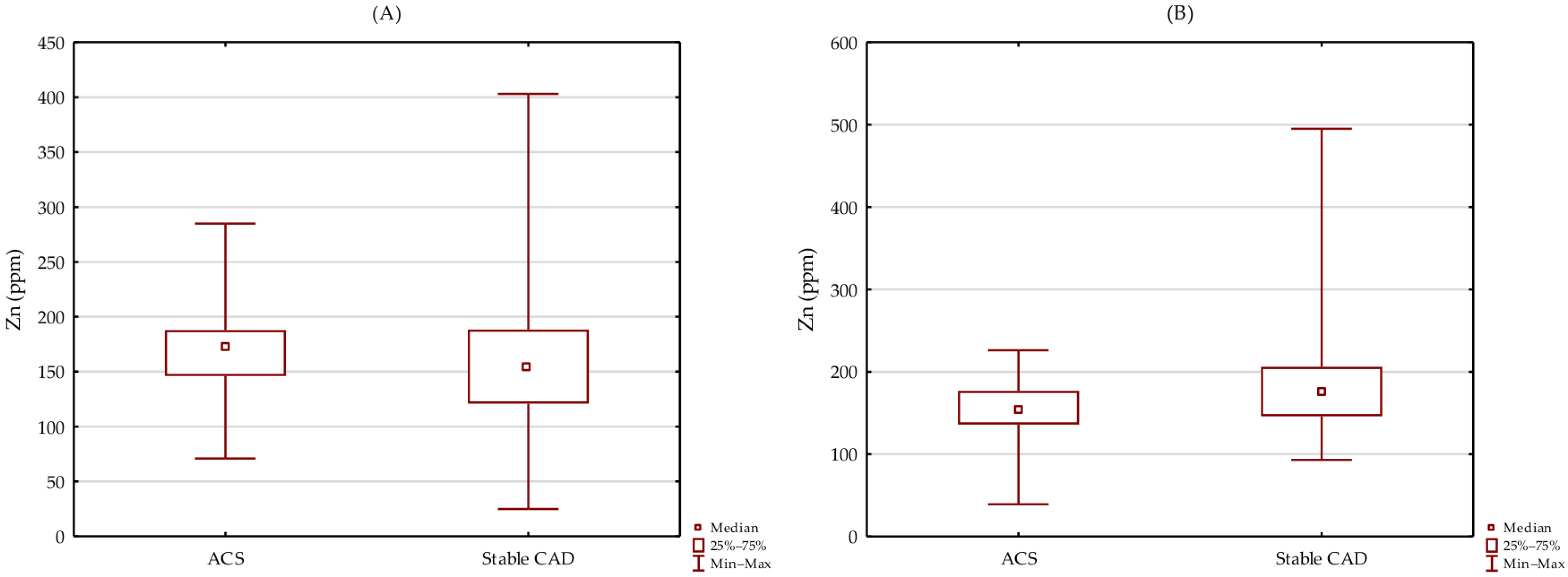
3.3. Difference in Zn Level between Patients with Stable CAD and Patients with ACS
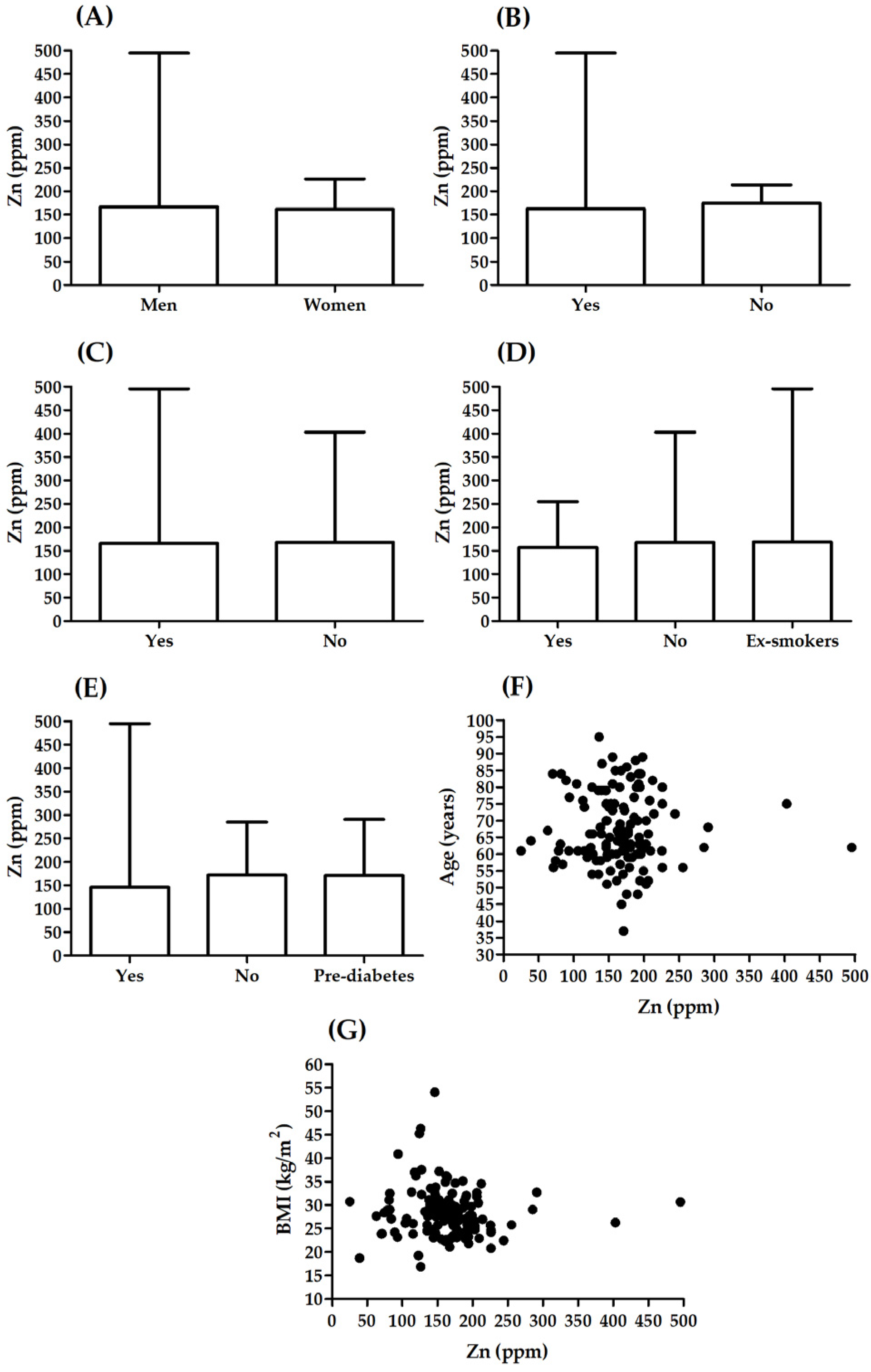
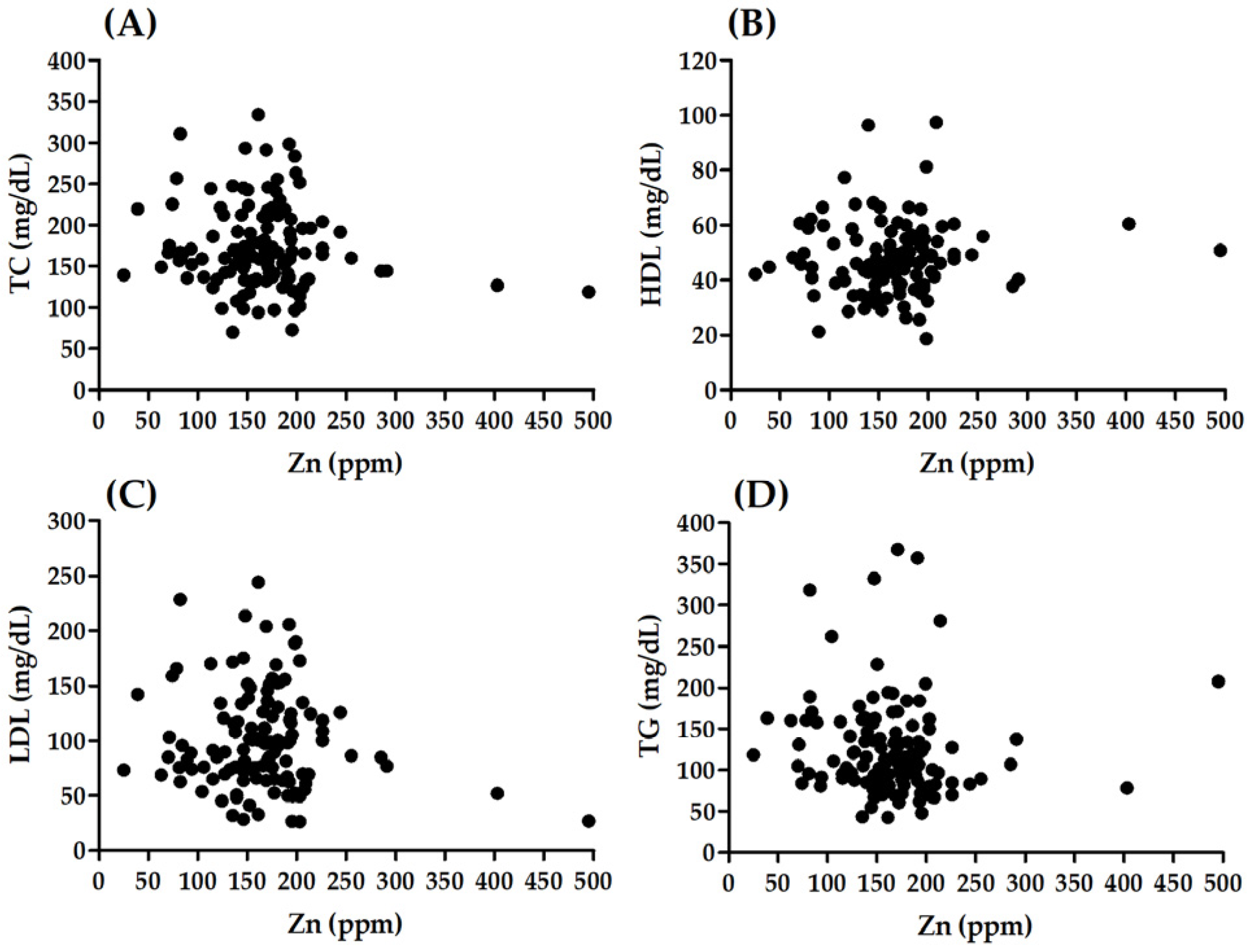
3.4. Association between Zn Level and Selected Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Global Health Estimates: Life Expectancy and Leading Causes of Death and Disability. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (accessed on 11 May 2022).
- Knez, M.; Glibetic, M. Zinc as a Biomarker of Cardiovascular Health. Front. Nutr. 2021, 8, 686078. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, M.; Poustchi, H.; Mohammadi-Nasrabadi, F.; Hekmatdoost, A. Systematic Review of Zinc Biochemical Indicators and Risk of Coronary Heart Disease. ARYA Atheroscler. 2015, 11, 357–365. [Google Scholar]
- Alexanian, I.; Parissis, J.; Farmakis, D.; Athanaselis, S.; Pappas, L.; Gavrielatos, G.; Mihas, C.; Paraskevaidis, I.; Sideris, A.; Kremastinos, D.; et al. Clinical and Echocardiographic Correlates of Serum Copper and Zinc in Acute and Chronic Heart Failure. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2014, 103, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Huang, L.; Zhao, J.; Wang, Z.; Yao, W.; Wu, X.; Huang, J.; Bian, B. The Relationship between Serum Zinc Level and Heart Failure: A Meta-Analysis. BioMed Res. Int. 2018, 2018, 2739014. [Google Scholar] [CrossRef] [PubMed]
- Alcantara, E.H.; Shin, M.Y.; Feldmann, J.; Nixon, G.F.; Beattie, J.H.; Kwun, I.S. Long-Term Zinc Deprivation Accelerates Rat Vascular Smooth Muscle Cell Proliferation Involving the down-Regulation of JNK1/2 Expression in MAPK Signaling. Atherosclerosis 2013, 228, 46–52. [Google Scholar] [CrossRef]
- Yoshihisa, A.; Abe, S.; Kiko, T.; Kimishima, Y.; Sato, Y.; Watanabe, S.; Kanno, Y.; Miyata-Tatsumi, M.; Misaka, T.; Sato, T.; et al. Association of Serum Zinc Level with Prognosis in Patients with Heart Failure. J. Card. Fail. 2018, 24, 375–383. [Google Scholar] [CrossRef]
- Huang, L.; Teng, T.; Bian, B.; Yao, W.; Yu, X.; Wang, Z.; Xu, Z.; Sun, Y. Zinc Levels in Left Ventricular Hypertrophy. Biol. Trace Elem. Res. 2017, 176, 48–55. [Google Scholar] [CrossRef]
- Beattie, J.H.; Kwun, I.-S. Is Zinc Deficiency a Risk Factor for Atherosclerosis? Br. J. Nutr. 2004, 91, 177–181. [Google Scholar] [CrossRef]
- Islamoglu, Y.; Evliyaoglu, O.; Tekbas, E.; Cil, H.; Elbey, M.A.; Atilgan, Z.; Kaya, H.; Bilik, Z.; Akyuz, A.; Alan, S. The Relationship between Serum Levels of Zn and Cu and Severity of Coronary Atherosclerosis. Biol. Trace Elem. Res. 2011, 144, 436–444. [Google Scholar] [CrossRef]
- El-Mahdy, R.I.; Mostafa, M.M.; El-Deen, H.S. Serum Zinc Measurement, Total Antioxidant Capacity, and Lipid Peroxide Among Acute Coronary Syndrome Patients with and Without ST Elevation. Appl. Biochem. Biotechnol. 2019, 188, 208–224. [Google Scholar] [CrossRef]
- de Paula, R.C.S.; Aneni, E.C.; Costa, A.P.R.; Figueiredo, V.N.; Moura, F.A.; Freitas, W.M.; Quaglia, L.A.; Santos, S.N.; Soares, A.A.; Nadruz, W.; et al. Low Zinc Levels Is Associated with Increased Inflammatory Activity but Not with Atherosclerosis, Arteriosclerosis or Endothelial Dysfunction among the Very Elderly. BBA Clin. 2014, 2, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Wang, Y.; Zhou, F.; Ruan, J.; Duan, M.; Wang, X.; Yu, Q.; Yang, P.; Chen, W.; Meng, F. Reduced Serum Zinc Ion Concentration Is Associated with Coronary Heart Disease. Biol. Trace Elem. Res. 2021, 199, 4109–4118. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhu, H.; Zhai, T.; Pan, H.; Wang, L.; Yang, H.; Yan, K.; Zeng, Y.; Gong, F. Serum Zinc-A2-Glycoprotein Levels Were Decreased in Patients with Premature Coronary Artery Disease. Front. Endocrinol. 2019, 10, 197. [Google Scholar] [CrossRef] [PubMed]
- Arsenault, J.E.; Wuehler, S.E.; de Romaña, D.L.; Penny, M.E.; Sempértegui, F.; Brown, K.H. The Time of Day and the Interval since Previous Meal Are Associated with Plasma Zinc Concentrations and Affect Estimated Risk of Zinc Deficiency in Young Children in Peru and Ecuador. Eur. J. Clin. Nutr. 2011, 65, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.A.; Chatt, A. Hair Analysis: Applications in the Biomedical and Environmental Sciences; VCH Publishers: New York, NY, USA, 1988; ISBN 978-0-89573-310-8. [Google Scholar]
- Pozebon, D.; Scheffler, G.L.; Dressler, V.L. Elemental Hair Analysis: A Review of Procedures and Applications. Anal. Chim. Acta 2017, 992, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Mesko, M.F.; Henn, A.S.; Novo, D.L.R.; Wilhelm, E.A.; Flores, E.M.M. Elemental Determination for Clinical Diagnosis and Prognosis: Challenges and Trends in Sample Preparation. In Comprehensive Analytical Chemistry; Elsevier: Amsterdam, The Netherlands, 2022; Volume 97, pp. 1–52. ISBN 978-0-444-64347-6. [Google Scholar]
- Suliburska, J. A Comparison of Levels of Select Minerals in Scalp Hair Samples with Estimated Dietary Intakes of These Minerals in Women of Reproductive Age. Biol. Trace Elem. Res. 2011, 144, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Klevay, L.M.; Christopherson, D.M.; Shuler, T.R. Hair as a Biopsy Material: Trace Element Data on One Man over Two Decades. Eur. J. Clin. Nutr. 2004, 58, 1359–1364. [Google Scholar] [CrossRef][Green Version]
- Gellein, K.; Lierhagen, S.; Brevik, P.S.; Teigen, M.; Kaur, P.; Singh, T.; Flaten, T.P.; Syversen, T. Trace Element Profiles in Single Strands of Human Hair Determined by HR-ICP-MS. Biol. Trace Elem. Res. 2008, 123, 250–260. [Google Scholar] [CrossRef]
- Khan, S.R.; Sharma, B.; Chawla, P.A.; Bhatia, R. Inductively Coupled Plasma Optical Emission Spectrometry (ICP-OES): A Powerful Analytical Technique for Elemental Analysis. Food Anal. Methods 2022, 15, 666–688. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e4–e17. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Vasak, M. Metallothioneins: New Functional and Structural Insights. Curr. Opin. Chem. Biol. 2000, 4, 177–183. [Google Scholar] [CrossRef]
- Chasapis, C.T.; Loutsidou, A.C.; Spiliopoulou, C.A.; Stefanidou, M.E. Zinc and Human Health: An Update. Arch. Toxicol. 2012, 86, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Wessells, K.R.; Brown, K.H. Estimating the Global Prevalence of Zinc Deficiency: Results Based on Zinc Availability in National Food Supplies and the Prevalence of Stunting. PLoS ONE 2012, 7, e50568. [Google Scholar] [CrossRef] [PubMed]
- Rink, L.; Gabriel, P. Zinc and the Immune System. Proc. Nutr. Soc. 2000, 59, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Beyersmann, D. Homeostasis and Cellular Functions of Zinc. Mater. Werkst. 2002, 33, 764–769. [Google Scholar] [CrossRef]
- Fagerberg, L.; Hallström, B.M.; Oksvold, P.; Kampf, C.; Djureinovic, D.; Odeberg, J.; Habuka, M.; Tahmasebpoor, S.; Danielsson, A.; Edlund, K.; et al. Analysis of the Human Tissue-Specific Expression by Genome-Wide Integration of Transcriptomics and Antibody-Based Proteomics. Mol. Cell. Proteom. MCP 2014, 13, 397–406. [Google Scholar] [CrossRef]
- Zalewski, P.D.; Beltrame, J.F.; Wawer, A.A.; Abdo, A.I.; Murgia, C. Roles for Endothelial Zinc Homeostasis in Vascular Physiology and Coronary Artery Disease. Crit. Rev. Food Sci. Nutr. 2019, 59, 3511–3525. [Google Scholar] [CrossRef]
- Choi, S.; Liu, X.; Pan, Z. Zinc Deficiency and Cellular Oxidative Stress: Prognostic Implications in Cardiovascular Diseases. Acta Pharmacol. Sin. 2018, 39, 1120–1132. [Google Scholar] [CrossRef]
- Chu, A.; Foster, M.; Samman, S. Zinc Status and Risk of Cardiovascular Diseases and Type 2 Diabetes Mellitus-A Systematic Review of Prospective Cohort Studies. Nutrients 2016, 8, 707. [Google Scholar] [CrossRef]
- Masley, S.C.; Roetzheim, R.; Masley, L.V.; McNamara, T.; Schocken, D.D. Emerging Risk Factors as Markers for Carotid Intima Media Thickness Scores. J. Am. Coll. Nutr. 2015, 34, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Shokrzadeh, M.; Ghaemian, A.; Salehifar, E.; Aliakbari, S.; Saravi, S.S.S.; Ebrahimi, P. Serum Zinc and Copper Levels in Ischemic Cardiomyopathy. Biol. Trace Elem. Res. 2009, 127, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Little, P.J.; Bhattacharya, R.; Moreyra, A.E.; Korichneva, I.L. Zinc and Cardiovascular Disease. Nutr. Burbank Los Angel. Cty. Calif 2010, 26, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Pae, M.; Meydani, S.N.; Wu, D. The Role of Nutrition in Enhancing Immunity in Aging. Aging Dis. 2012, 3, 91–129. [Google Scholar] [PubMed]
- Korichneva, I. Zinc Dynamics in the Myocardial Redox Signaling Network. Antioxid. Redox Signal. 2006, 8, 1707–1721. [Google Scholar] [CrossRef]
- Allen-Redpath, K.; Ou, O.; Beattie, J.H.; Kwun, I.-S.; Feldmann, J.; Nixon, G.F. Marginal Dietary Zinc Deficiency In Vivo Induces Vascular Smooth Muscle Cell Apoptosis in Large Arteries. Cardiovasc. Res. 2013, 99, 525–534. [Google Scholar] [CrossRef]
- Prasad, A.S.; Beck, F.W.J.; Bao, B.; Fitzgerald, J.T.; Snell, D.C.; Steinberg, J.D.; Cardozo, L.J. Zinc Supplementation Decreases Incidence of Infections in the Elderly: Effect of Zinc on Generation of Cytokines and Oxidative Stress. Am. J. Clin. Nutr. 2007, 85, 837–844. [Google Scholar] [CrossRef]
- Eide, D.J. The Oxidative Stress of Zinc Deficiency. Met. Integr. Biomet. Sci. 2011, 3, 1124–1129. [Google Scholar] [CrossRef]
- Cortese, M.M.; Suschek, C.V.; Wetzel, W.; Kröncke, K.-D.; Kolb-Bachofen, V. Zinc Protects Endothelial Cells from Hydrogen Peroxide via Nrf2-Dependent Stimulation of Glutathione Biosynthesis. Free Radic. Biol. Med. 2008, 44, 2002–2012. [Google Scholar] [CrossRef]
- Li, H.-T.; Jiao, M.; Chen, J.; Liang, Y. Roles of Zinc and Copper in Modulating the Oxidative Refolding of Bovine Copper, Zinc Superoxide Dismutase. Acta Biochim. Biophys. Sin. 2010, 42, 183–194. [Google Scholar] [CrossRef]
- Jenner, A.; Ren, M.; Rajendran, R.; Ning, P.; Huat, B.T.K.; Watt, F.; Halliwell, B. Zinc Supplementation Inhibits Lipid Peroxidation and the Development of Atherosclerosis in Rabbits Fed a High Cholesterol Diet. Free Radic. Biol. Med. 2007, 42, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Cortese-Krott, M.M.; Kulakov, L.; Opländer, C.; Kolb-Bachofen, V.; Kröncke, K.-D.; Suschek, C.V. Zinc Regulates INOS-Derived Nitric Oxide Formation in Endothelial Cells. Redox Biol. 2014, 2, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.P.; Ho, E. Zinc and Its Role in Age-Related Inflammation and Immune Dysfunction. Mol. Nutr. Food Res. 2012, 56, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Beattie, J.H.; Gordon, M.-J.; Duthie, S.J.; McNeil, C.J.; Horgan, G.W.; Nixon, G.F.; Feldmann, J.; Kwun, I.-S. Suboptimal Dietary Zinc Intake Promotes Vascular Inflammation and Atherogenesis in a Mouse Model of Atherosclerosis. Mol. Nutr. Food Res. 2012, 56, 1097–1105. [Google Scholar] [CrossRef]
- Jurowski, K.; Szewczyk, B.; Nowak, G.; Piekoszewski, W. Biological Consequences of Zinc Deficiency in the Pathomechanisms of Selected Diseases. J. Biol. Inorg. Chem. JBIC Publ. Soc. Biol. Inorg. Chem. 2014, 19, 1069–1079. [Google Scholar] [CrossRef]
- Bao, B.; Prasad, A.S.; Beck, F.W.J.; Fitzgerald, J.T.; Snell, D.; Bao, G.W.; Singh, T.; Cardozo, L.J. Zinc Decreases C-Reactive Protein, Lipid Peroxidation, and Inflammatory Cytokines in Elderly Subjects: A Potential Implication of Zinc as an Atheroprotective Agent. Am. J. Clin. Nutr. 2010, 91, 1634–1641. [Google Scholar] [CrossRef]
- Kritchevsky, D. Diet and Atherosclerosis. J. Nutr. Health Aging 2001, 5, 155–159. [Google Scholar]
- Singh, R.B.; Niaz, M.A.; Rastogi, S.S.; Bajaj, S.; Gaoli, Z.; Shoumin, Z. Current Zinc Intake and Risk of Diabetes and Coronary Artery Disease and Factors Associated with Insulin Resistance in Rural and Urban Populations of North India. J. Am. Coll. Nutr. 1998, 17, 564–570. [Google Scholar] [CrossRef]
- Giannoglou, G.D.; Konstantinou, D.M.; Kovatsi, L.; Chatzizisis, Y.S.; Mikhailidis, D.P. Association of Reduced Zinc Status with Angiographically Severe Coronary Atherosclerosis: A Pilot Study. Angiology 2010, 61, 449–455. [Google Scholar] [CrossRef]
- Meng, H.; Wang, Y.; Ruan, J.; Chen, Y.; Wang, X.; Zhou, F.; Meng, F. Decreased Iron Ion Concentrations in the Peripheral Blood Correlate with Coronary Atherosclerosis. Nutrients 2022, 14, 319. [Google Scholar] [CrossRef]
- Gao, J.-W.; Zhang, S.-L.; Hao, Q.-Y.; Huang, F.-F.; Liu, Z.-Y.; Zhang, H.-F.; Yan, L.; Wang, J.-F.; Liu, P.-M. Association of Dietary Zinc Intake with Coronary Artery Calcium Progression: The Multi-Ethnic Study of Atherosclerosis (MESA). Eur. J. Nutr. 2021, 60, 2759–2767. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Choi, B.Y.; Chun, B.-Y.; Kweon, S.-S.; Lee, Y.-H.; Park, P.S.; Kim, M.K. Dietary Zinc Intake Is Inversely Related to Subclinical Atherosclerosis Measured by Carotid Intima-Media Thickness. Br. J. Nutr. 2010, 104, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Low, W.I.; Ikram, H. Plasma Zinc in Acute Myocardial Infarction. Diagnostic and Prognostic Implications. Br. Heart J. 1976, 38, 1339–1342. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Cai, Z.-Q.; Zhou, Y.-M. Deficient Zinc Levels and Myocardial Infarction: Association between Deficient Zinc Levels and Myocardial Infarction: A Meta-Analysis. Biol. Trace Elem. Res. 2015, 165, 41–50. [Google Scholar] [CrossRef]
- Huang, L.; Teng, T.; Zhao, J.; Bian, B.; Yao, W.; Yu, X.; Wang, Z.; Xu, Z.; Sun, Y. The Relationship Between Serum Zinc Levels, Cardiac Markers and the Risk of Acute Myocardial Infarction by Zinc Quartiles. Heart Lung Circ. 2018, 27, 66–72. [Google Scholar] [CrossRef]
- Lal, A. Effect of Zinc Sulphate on Infarct Size in Experimental Myocardial Infarction in Dogs. Indian J. Med. Res. 1991, 94, 316–319. [Google Scholar]
- Karagulova, G.; Yue, Y.; Moreyra, A.; Boutjdir, M.; Korichneva, I. Protective Role of Intracellular Zinc in Myocardial Ischemia/Reperfusion Is Associated with Preservation of Protein Kinase C Isoforms. J. Pharmacol. Exp. Ther. 2007, 321, 517–525. [Google Scholar] [CrossRef]
- Xu, Z.; Kim, S.; Huh, J. Zinc Plays a Critical Role in the Cardioprotective Effect of Postconditioning by Enhancing the Activation of the RISK Pathway in Rat Hearts. J. Mol. Cell. Cardiol. 2014, 66, 12–17. [Google Scholar] [CrossRef]
- Lee, D.-H.; Folsom, A.R.; Jacobs, D.R. Iron, Zinc, and Alcohol Consumption and Mortality from Cardiovascular Diseases: The Iowa Women’s Health Study. Am. J. Clin. Nutr. 2005, 81, 787–791. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Boeing, H.; Stelmach-Mardas, M.; Gottschald, M.; Dietrich, S.; Hoffmann, G.; Chaimani, A. Dietary Supplements and Risk of Cause-Specific Death, Cardiovascular Disease, and Cancer: A Systematic Review and Meta-Analysis of Primary Prevention Trials. Adv. Nutr. Bethesda Md 2017, 8, 27–39. [Google Scholar] [CrossRef]
- Ruz, M.; Carrasco, F.; Rojas, P.; Basfi-Fer, K.; Hernández, M.C.; Pérez, A. Nutritional Effects of Zinc on Metabolic Syndrome and Type 2 Diabetes: Mechanisms and Main Findings in Human Studies. Biol. Trace Elem. Res. 2019, 188, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Sujatha, P. Trace Elements in Diabetes Mellitus. J. Clin. Diagn. Res. 2013, 7, 1863–1865. [Google Scholar] [CrossRef] [PubMed]
- Maret, W. Zinc in Pancreatic Islet Biology, Insulin Sensitivity, and Diabetes. Prev. Nutr. Food Sci. 2017, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chabosseau, P.; Rutter, G.A. Zinc and Diabetes. Arch. Biochem. Biophys. 2016, 611, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Garg, V.K.; Gupta, R.; Goyal, R.K. Hypozincemia in Diabetes Mellitus. J. Assoc. Physicians India 1994, 42, 720–721. [Google Scholar]
- Pidduck, H.G.; Wren, P.J.J.; Price Evans, D.A. Hyperzincuria of Diabetes Mellitus and Possible Genetical Implications of This Observation. Diabetes 1970, 19, 240–247. [Google Scholar] [CrossRef]
- Fernández-Cao, J.C.; Warthon-Medina, M.; H Moran, V.; Arija, V.; Doepking, C.; Serra-Majem, L.; Lowe, N.M. Zinc Intake and Status and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 1027. [Google Scholar] [CrossRef]
- Capdor, J.; Foster, M.; Petocz, P.; Samman, S. Zinc and Glycemic Control: A Meta-Analysis of Randomised Placebo Controlled Supplementation Trials in Humans. J. Trace Elem. Med. Biol. Organ Soc. Miner. Trace Elem. GMS 2013, 27, 137–142. [Google Scholar] [CrossRef]
- Desmarchelier, C.; Borel, P.; Lairon, D.; Maraninchi, M.; Valéro, R. Effect of Nutrient and Micronutrient Intake on Chylomicron Production and Postprandial Lipemia. Nutrients 2019, 11, 1299. [Google Scholar] [CrossRef]
- Olechnowicz, J.; Tinkov, A.; Skalny, A.; Suliburska, J. Zinc Status Is Associated with Inflammation, Oxidative Stress, Lipid, and Glucose Metabolism. J. Physiol. Sci. JPS 2018, 68, 19–31. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Wathurapatha, W.S.; Ishara, M.H.; Jayawardana, R.; Galappatthy, P.; Katulanda, P.; Constantine, G.R. Effects of Zinc Supplementation on Serum Lipids: A Systematic Review and Meta-Analysis. Nutr. Metab. 2015, 12, 26. [Google Scholar] [CrossRef]
- Knez, M.; Pantovic, A.; Zekovic, M.; Pavlovic, Z.; Glibetic, M.; Zec, M. Is There a Link between Zinc Intake and Status with Plasma Fatty Acid Profile and Desaturase Activities in Dyslipidemic Subjects? Nutrients 2019, 12, 93. [Google Scholar] [CrossRef] [PubMed]
- Kelishadi, R.; Hashemipour, M.; Adeli, K.; Tavakoli, N.; Movahedian-Attar, A.; Shapouri, J.; Poursafa, P.; Rouzbahani, A. Effect of Zinc Supplementation on Markers of Insulin Resistance, Oxidative Stress, and Inflammation among Prepubescent Children with Metabolic Syndrome. Metab. Syndr. Relat. Disord. 2010, 8, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Afridi, H.; Kazi, T.; Kazi, N.; Talpur, F.; Naeemullah; Arain, S.; Brahman, K.; Wadhwa, S.; Shah, F. Distribution of Copper, Iron, and Zinc in Biological Samples of Pakistani Hypertensive Patients and Referent Subjects of Different Age Groups. Clin. Lab. 2013, 59. [Google Scholar] [CrossRef]
- Ghayour-Mobarhan, M.; Shapouri-Moghaddam, A.; Azimi-Nezhad, M.; Esmaeili, H.; Parizadeh, S.M.R.; Safarian, M.; Kazemi-Bajestani, S.M.R.; Khodaei, G.H.; Hosseini, S.J.; Parizadeh, S.M.J.; et al. The Relationship between Established Coronary Risk Factors and Serum Copper and Zinc Concentrations in a Large Persian Cohort. J. Trace Elem. Med. Biol. 2009, 23, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Knez, M.; Nikolic, M.; Zekovic, M.; Stangoulis, J.C.; Gurinovic, M.; Glibetic, M. The Influence of Food Consumption and Socio-Economic Factors on the Relationship between Zinc and Iron Intake and Status in a Healthy Population. Public Health Nutr. 2017, 20, 2486–2498. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Otto, M.C.; Alonso, A.; Lee, D.-H.; Delclos, G.L.; Bertoni, A.G.; Jiang, R.; Lima, J.A.; Symanski, E.; Jacobs, D.R.; Nettleton, J.A. Dietary Intakes of Zinc and Heme Iron from Red Meat, but Not from Other Sources, Are Associated with Greater Risk of Metabolic Syndrome and Cardiovascular Disease. J. Nutr. 2012, 142, 526–533. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CASSS 0 | CASSS 1 | CASSS 2 | CASSS 3 | p-Value | |
|---|---|---|---|---|---|
| N | 22 | 34 | 46 | 31 | - |
| Sex (♀/♂) | 10/12 | 12/22 | 6/40 | 9/22 | 0.025 |
| Age (years) | 66 (54–85) | 66 (48–89) | 63 (37–84) | 68 (52–95) | 0.455 |
| BMI (kg/m2) | 28.5 (21.1–46.3) | 27.7 (16.9–40.9) | 27.9 (22.3–54.1) | 26.8 (18.7–45.3) | 0.476 |
| Cause of hospitalization (ACS/stable CAD) | 5/17 | 22/12 | 22/24 | 18/13 | 0.016 |
| t2DM (no/yes/pre-diabetes) ** | 17/4/1 | 21/13/0 | 29/13/4 | 17/12/2 | --- |
| t2DM (no/yes) | 17/4 | 21/13 | 29/13 | 17/12 | 0.355 |
| Hyperlipidaemia (no/yes) * | 10/8 | 17/16 | 24/20 | 17/11 | 0.911 |
| HDL (mg/dL) * | 46.6 (28.6–66.5) | 47.3 (25.7–97.4) | 47.1 (21.3–77.5) | 44.5 (18.6–81.3) | 0.292 |
| LDL (mg/dL) * | 106.9 (26.6–171.7) | 100.4 (26.2–175.3) | 88.7 (26.9–244.3) | 76.3 (31.8–228.3) | 0.418 |
| TG (mg/dL) * | 124.8 (47.8–281.0) | 104.2 (60.6–357.6) | 111.6 (42.6–367.8) | 110.3 (43.4–332.4) | 0.545 |
| TC (mg/dL) * | 178.2 (73.3–255.9) | 166.9 (101.7–256.7) | 159.9 (94.1–334.1) | 154.5 (70.0–310.8) | 0.316 |
| Hypertension (no/yes) | 5/17 | 6/28 | 4/42 | 4/27 | 0.421 |
| History of MI (no/yes) | 22/0 | 26/8 | 27/19 | 18/13 | 0.002 |
| Smoking (no/yes/ex-smokers) ** | 16/5/1 | 22/10/2 | 19/17/10 | 19/8/4 | --- |
| Smoking (no/yes) | 16/5 | 22/10 | 19/17 | 19/8 | 0.254 |
| Zn (ppm) | 161 (70–214) | 169 (74–226) | 169 (81–495) | 166 (25–403) | 0.670 |
| ACS | Stable CAD | p-Value | |
|---|---|---|---|
| N | 67 | 66 | - |
| Sex (♀/♂) | 16/51 | 21/45 | 0.307 |
| Age (years) | 66 (37–95) | 63 (51–85) | 0.345 |
| BMI (kg/m2) | 27.7 (16.9–45.3) | 27.6 (19.3–54.1) | 0.791 |
| t2DM (no/yes/pre-diabetes) ** | 44/19/4 | 40/23/3 | --- |
| t2DM (no/yes) | 44/19 | 40/23 | 0.449 |
| Hyperlipidaemia (no/yes) * | 35/26 | 33/29 | 0.643 |
| HDL (mg/dL) * | 46.6 (25.7–81.3) | 46.0 (18.6–97.4) | 0.279 |
| LDL (mg/dL) * | 101.5 (26.6–244.3) | 78.6 (26.2–204.0) | 0.008 |
| TG (mg/dL) * | 103.3 (42.6–367.8) | 124.7 (66.6–357.6) | 0.008 |
| TC (mg/dL) * | 168.3 (70.0–334.1) | 159.6 (96.4–291.1) | 0.142 |
| Hypertension (no/yes) | 8/59 | 11/55 | 0.436 |
| History of MI (no/yes) | 49/18 | 44/22 | 0.416 |
| Smoking (no/yes/ex-smokers) ** | 43/22/2 | 33/18/15 | --- |
| Smoking (no/yes) | 43/22 | 33/18 | 0.871 |
| Zn (ppm) | 166.0 (39.0–285.0) | 166.5 (25.0–495.0) | 0.937 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziedzic, E.A.; Gąsior, J.S.; Tuzimek, A.; Paleczny, J.; Kwaśny, M.; Dąbrowski, M.; Jankowski, P. No Association of Hair Zinc Concentration with Coronary Artery Disease Severity and No Relation with Acute Coronary Syndromes. Biomolecules 2022, 12, 862. https://doi.org/10.3390/biom12070862
Dziedzic EA, Gąsior JS, Tuzimek A, Paleczny J, Kwaśny M, Dąbrowski M, Jankowski P. No Association of Hair Zinc Concentration with Coronary Artery Disease Severity and No Relation with Acute Coronary Syndromes. Biomolecules. 2022; 12(7):862. https://doi.org/10.3390/biom12070862
Chicago/Turabian StyleDziedzic, Ewelina A., Jakub S. Gąsior, Agnieszka Tuzimek, Justyna Paleczny, Mirosław Kwaśny, Marek Dąbrowski, and Piotr Jankowski. 2022. "No Association of Hair Zinc Concentration with Coronary Artery Disease Severity and No Relation with Acute Coronary Syndromes" Biomolecules 12, no. 7: 862. https://doi.org/10.3390/biom12070862
APA StyleDziedzic, E. A., Gąsior, J. S., Tuzimek, A., Paleczny, J., Kwaśny, M., Dąbrowski, M., & Jankowski, P. (2022). No Association of Hair Zinc Concentration with Coronary Artery Disease Severity and No Relation with Acute Coronary Syndromes. Biomolecules, 12(7), 862. https://doi.org/10.3390/biom12070862