
Dexamethasone for Inner Ear Therapy: Biocompatibility and Bio-Efficacy of Different Dexamethasone Formulations In Vitro

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dexamethasone Formulations
2.2. Cell Lines and Culture Conditions
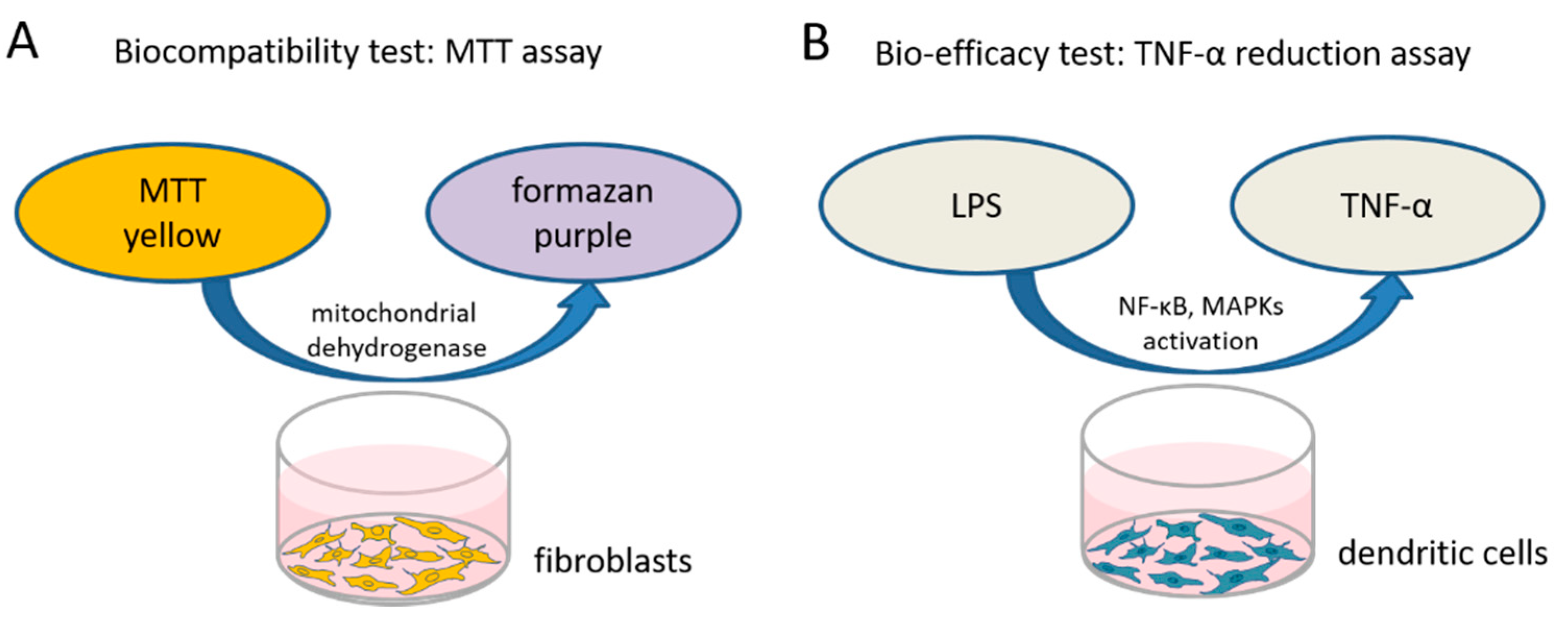
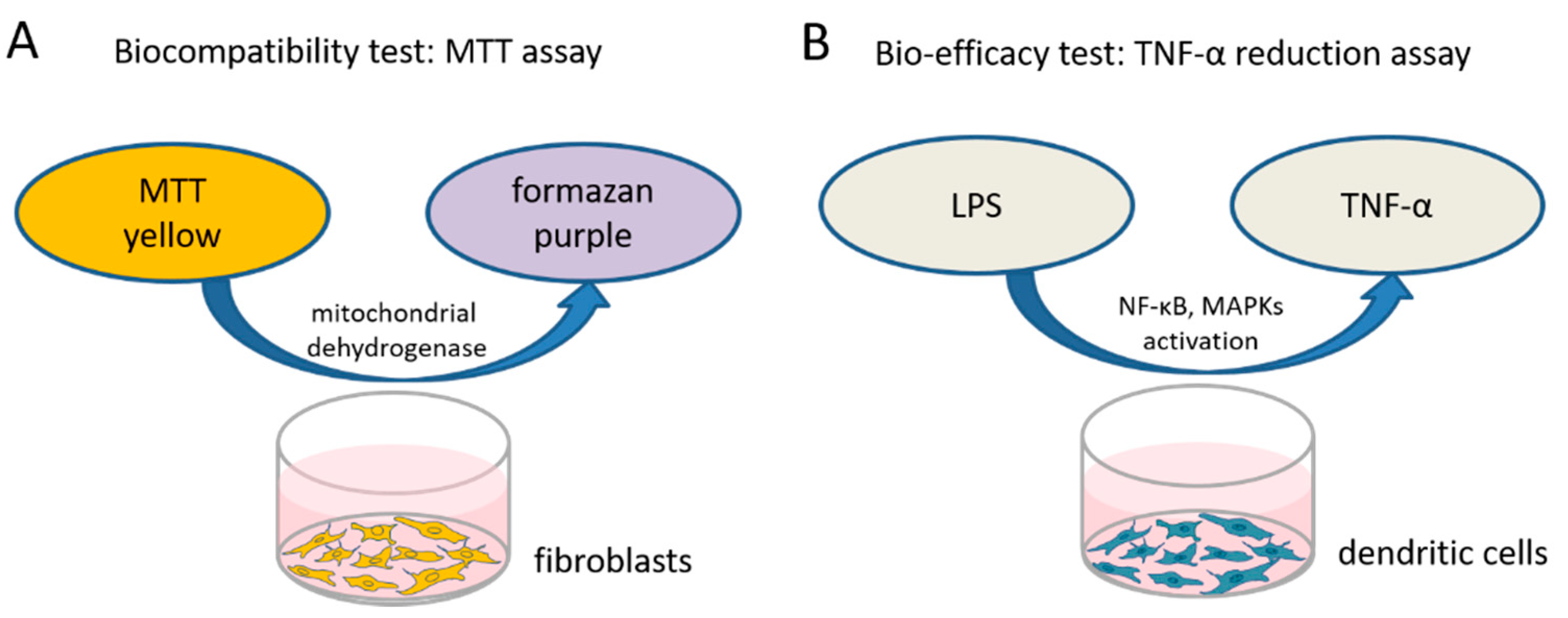
2.2.1. Biocompatibility Test
2.2.2. Bio-Efficacy
2.2.3. TNF-α Detection
2.2.4. Statistical Analysis
3. Results
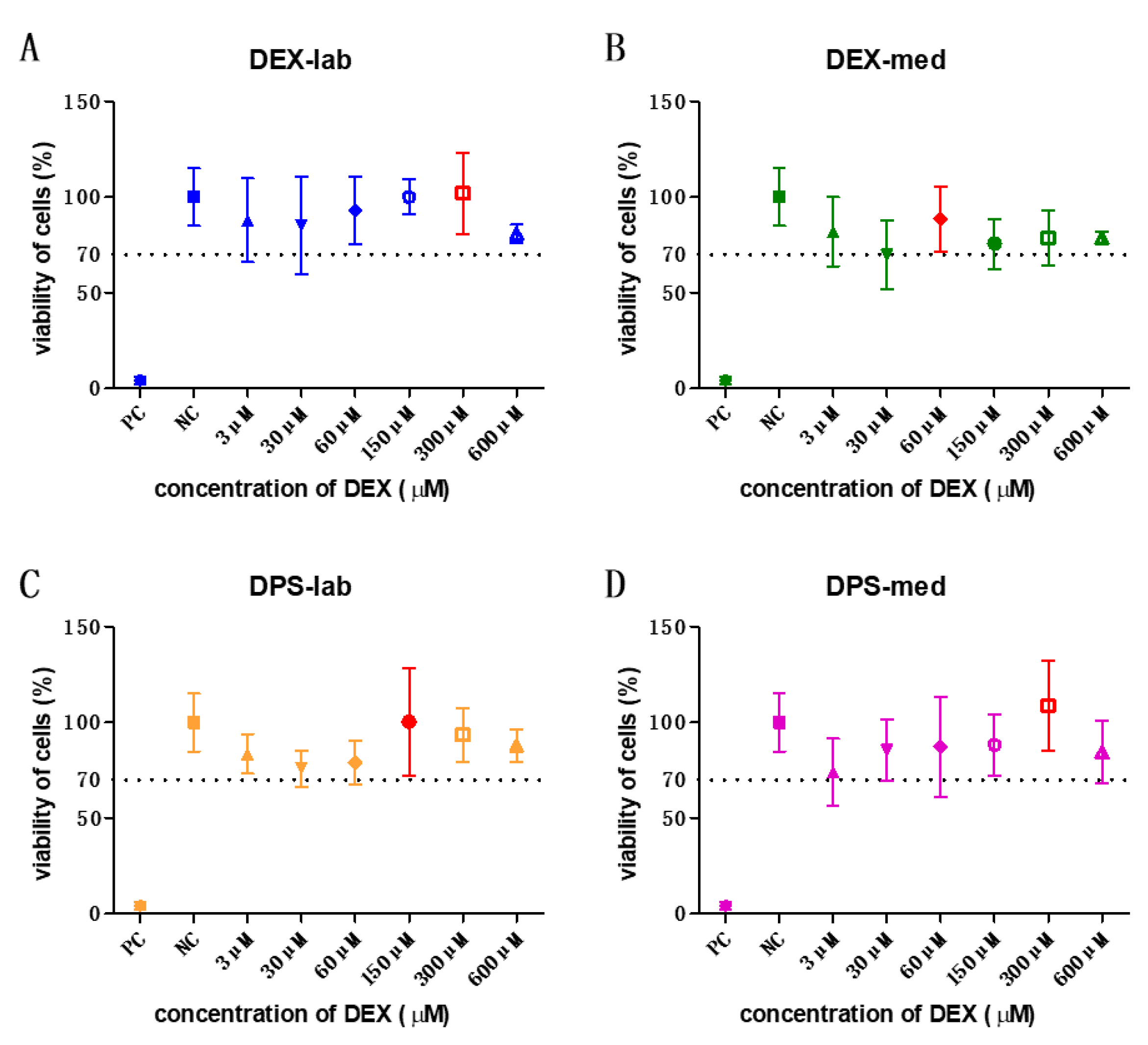
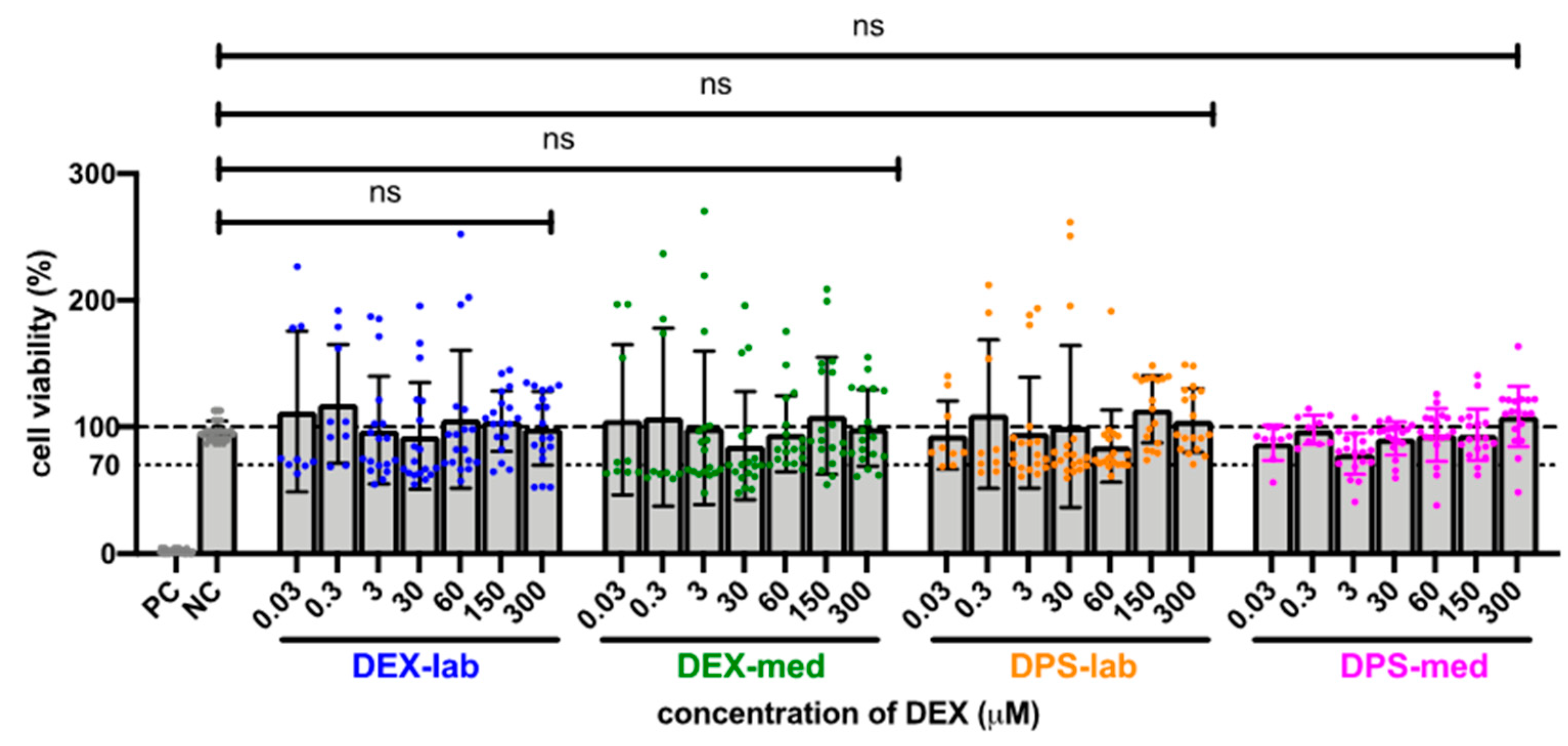
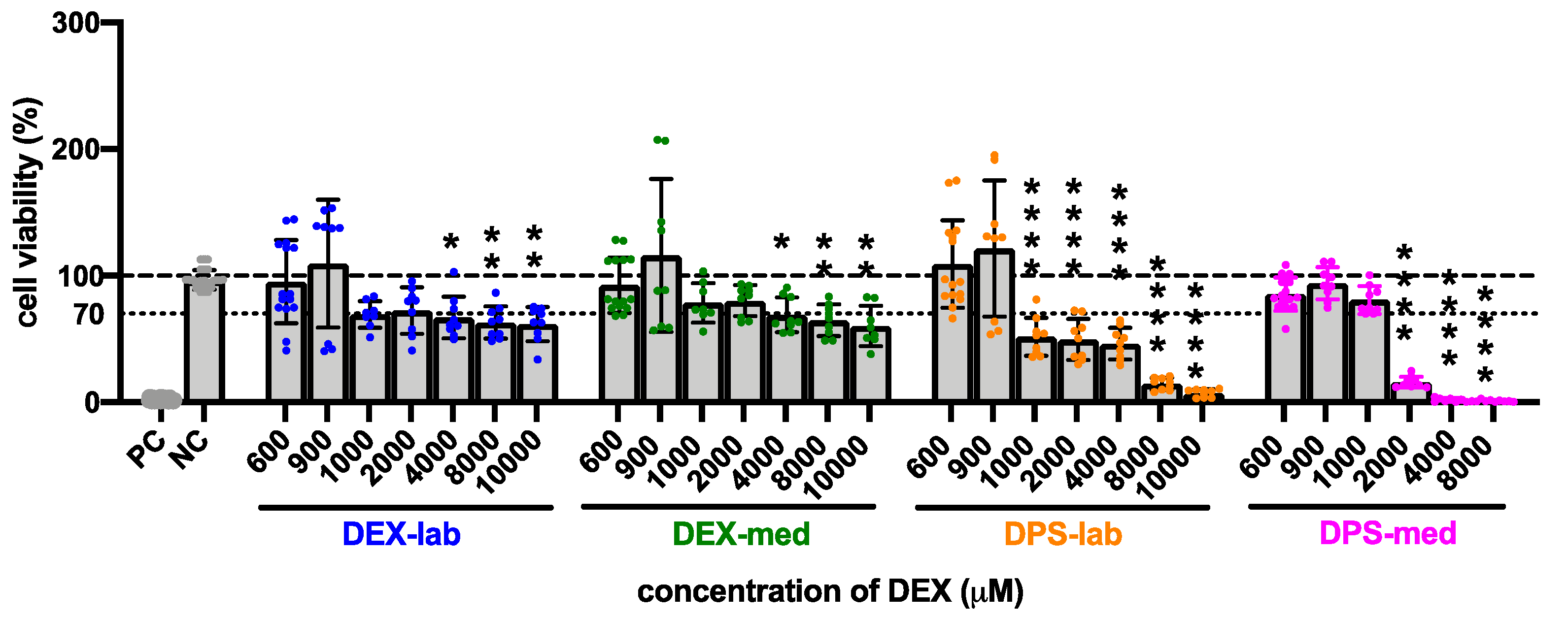
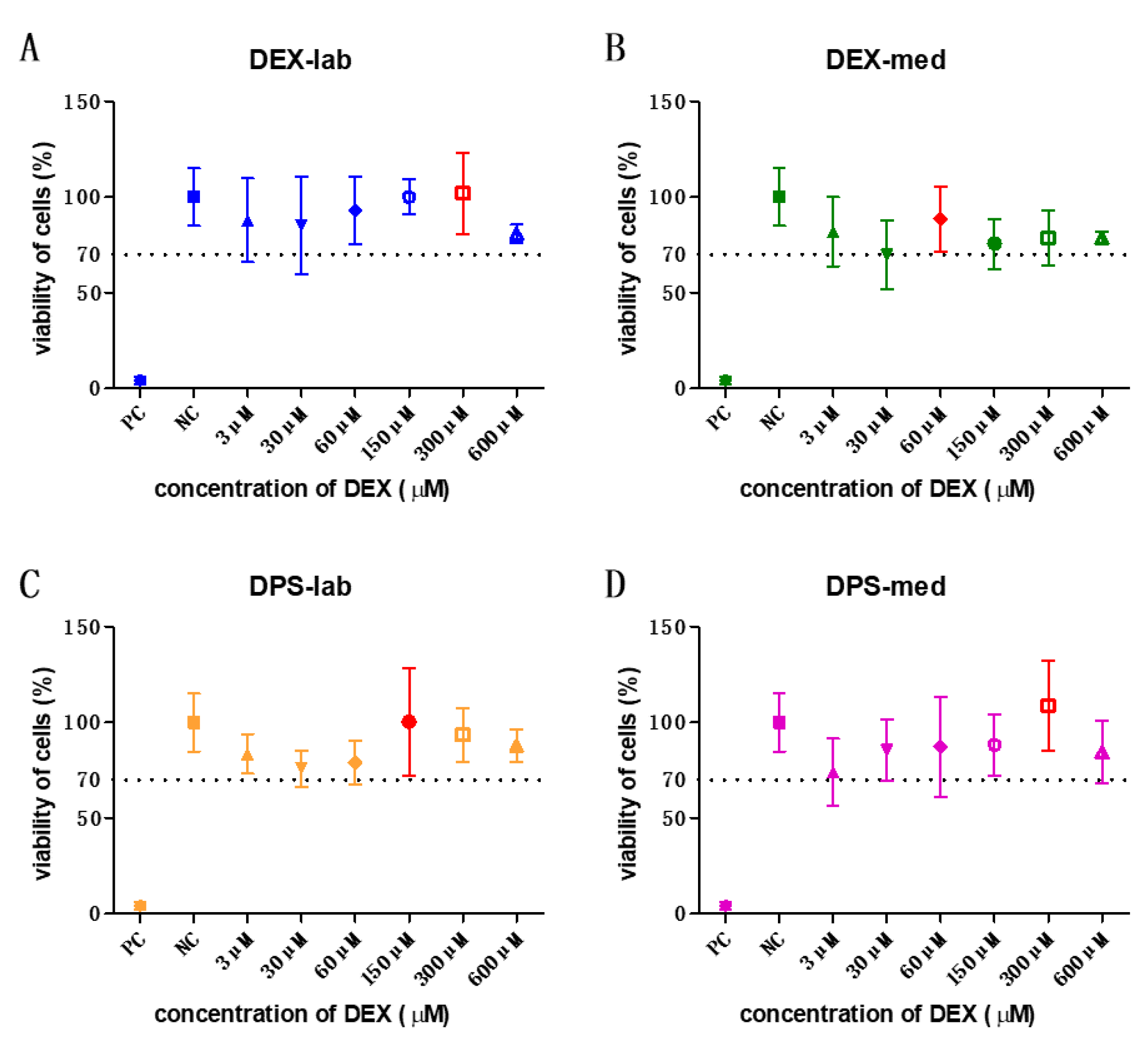
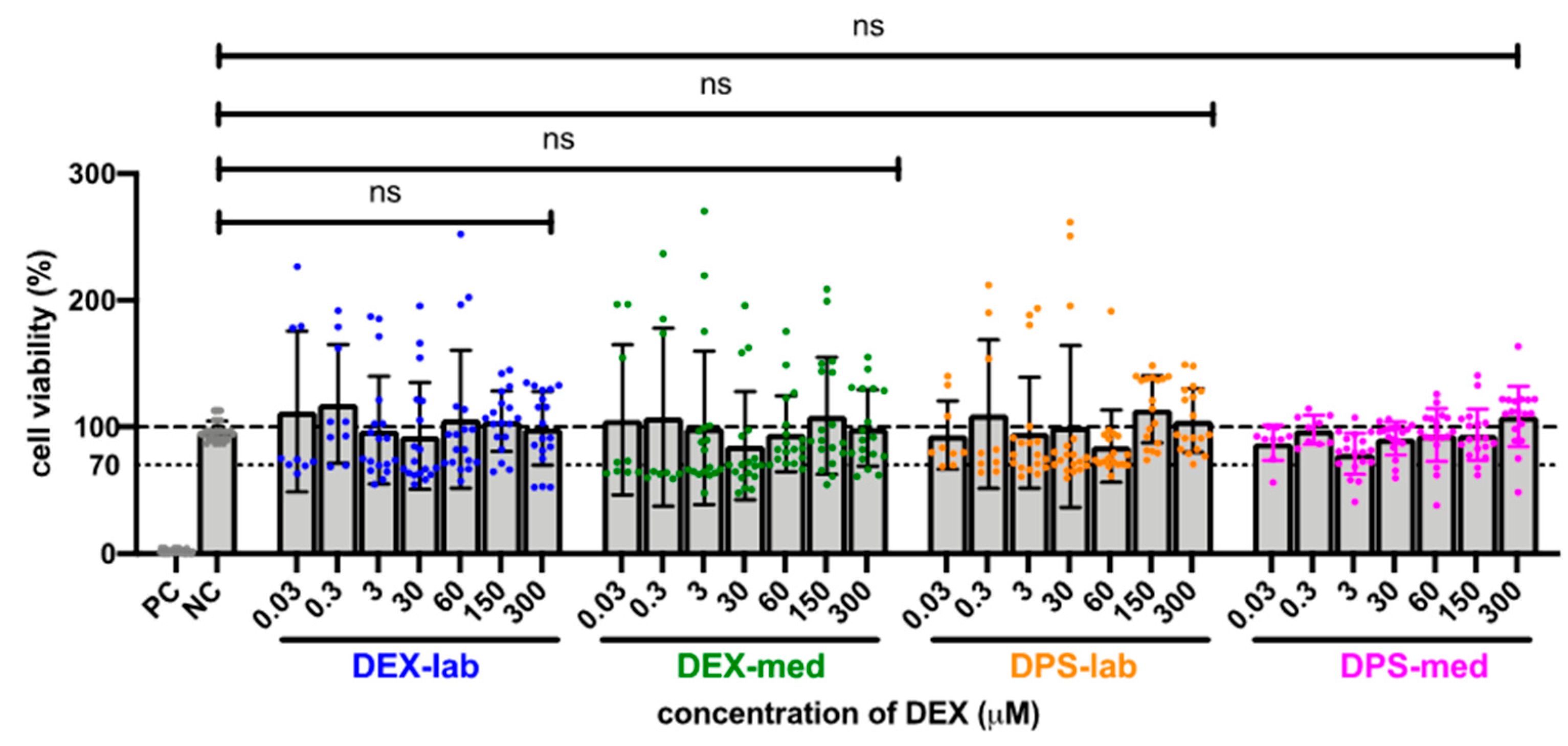
3.1. Cell Viability for Biocompatibility
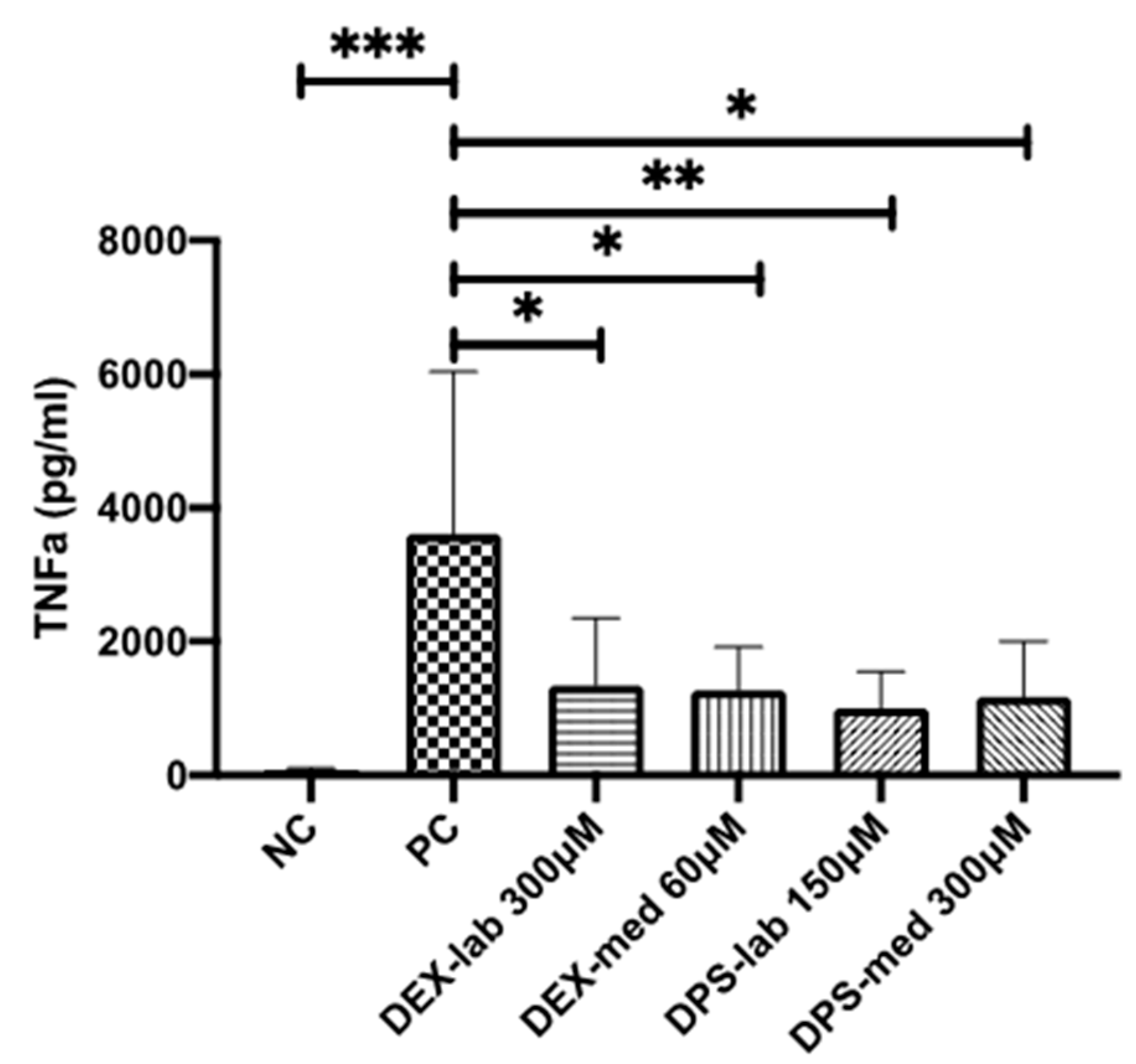
3.2. Bio-Efficiency Evaluation by TNF-α Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Cochlear implant |
| DEX-lab | Dexamethasone—laboratory grade |
| DEX-med | Dexamethasone—medical grade |
| DPS-med | Dexamethasone dihydrogen phosphate-disodium—medical grade |
| DPS-lab | Dexamethasone sodium phosphate—laboratory grade |
| DMEM | Dulbecco’s modified Eagle’s medium |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| FCS | Fetal calf serum |
| FBs | NIH/3T3 mouse fibroblasts |
| h | hour |
| HL | Hearing loss |
| i.c. | Intracochlear |
| i.p. | Intraperitoneal |
| i.t. | Intratympanic |
| i.v. | Intravenous |
| LPS | Lipopolysaccharides |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| NC | Negative control |
| OD | Optical density |
| PC | Positive control |
| RT | Room temperature |
| SSNHL | Sudden sensorineural hearing loss |
| SGN | Spiral ganglion neurons |
| SD | Standard deviation |
| TNF-α | Tumor necrosis factor alpha |
References
- WHO|Deafness and Hearing Loss. Available online: https://www.who.int/en/news-room/fact-sheets/detail/deafness-and-hearing-loss (accessed on 8 December 2021).
- Neumann, K.; Chadha, S.; Tavartkiladze, G.; Bu, X.; White, K.R. Newborn and Infant Hearing Screening Facing Globally Growing Numbers of People Suffering from Disabling Hearing Loss. Int. J. Neonatal Screen. 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, S.; Ye, Q.; Radeloff, A.; Kiefer, J.; Gstoettner, W.; Tillein, J. Protection of Inner Ear Function after Cochlear Implantation: Compound Action Potential Measurements after Local Application of Glucocorticoids in the Guinea Pig Cochlea. ORL 2011, 73, 219–228. [Google Scholar] [CrossRef]
- Maini, S.; Lisnichuk, H.; Eastwood, H.; Pinder, D.; James, D.; Richardson, R.T.; Chang, A.; Connolly, T.; Sly, D.; Kel, G.; et al. Targeted Therapy of the Inner Ear. Audiol. Neurotol. 2009, 14, 402–410. [Google Scholar] [CrossRef]
- Schilder, A.G.M.; Su, M.; Blackshaw, H.; Lustig, L.; Staecker, H.; Lenarz, T.; Safieddine, S.; Gomes-Santos, C.S.; Holme, R.; Warnecke, A. Hearing Protection, Restoration, and Regeneration: An Overview of Emerging Therapeutics for Inner Ear and Central Hearing Disorders. Otol. Neurotol. 2019, 40, 559–570. [Google Scholar] [CrossRef]
- Kuthubutheen, J.; Coates, H.; Rowsell, C.; Nedzelski, J.; Chen, J.M.; Lin, V. The role of extended preoperative steroids in hearing preservation cochlear implantation. Hear. Res. 2015, 327, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Plontke, S.K.; Löwenheim, H.; Mertens, J.; Engel, C.; Meisner, C.; Weidner, A.; Zimmermann, R.; Preyer, S.; Koitschev, A.; Zenner, H.-P. Randomized, double blind, placebo controlled trial on the safety and efficacy of continuous intratympanic dexamethasone delivered via a round window catheter for severe to profound sudden idiopathic sensorineural hearing loss after failure of systemic therapy. Laryngoscope 2009, 119, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Erdur, O.; Kayhan, F.T.; Cirik, A.A. Effectiveness of intratympanic dexamethasone for refractory sudden sensorineural hearing loss. Eur. Arch. Oto-Rhino-Laryngol. 2013, 271, 1431–1436. [Google Scholar] [CrossRef] [PubMed]
- Musavi, A.; Berjis, N.; Soheilipour, S.; Hashemi, S.M. Intratympanic dexamethasone injection vs methylprednisolone for the treatment of refractory sudden sensorineural hearing loss. Adv. Biomed. Res. 2016, 5, 111. [Google Scholar] [CrossRef]
- Li, X.; Chen, W.-J.; Xu, J.; Yi, H.-J.; Ye, J.-Y. Clinical Analysis of Intratympanic Injection of Dexamethasone for Treating Sudden Deafness. Int. J. Gen. Med. 2021, 14, 2575–2579. [Google Scholar] [CrossRef] [PubMed]
- Albu, S.; Nagy, A.; Doros, C.; Marceanu, L.; Cozma, S.; Musat, G.; Trabalzini, F. Treatment of Meniere’s disease with intratympanic dexamethazone plus high dosage of betahistine. Am. J. Otolaryngol. 2015, 37, 225–230. [Google Scholar] [CrossRef]
- Al Attrache, N.A.; Krstulovic, C.; Guillen, V.P.; Pérez, C.M.; Garrigues, H.P. Response Over Time of Vertigo Spells to Intratympanic Dexamethasone Treatment in Meniere’s Disease Patients. J. Int. Adv. Otol. 2016, 12, 92–97. [Google Scholar] [CrossRef]
- Silverstein, H.; Isaacson, J.E.; Olds, M.J.; Rowan, P.T.; Rosenberg, S. Dexamethasone inner ear perfusion for the treatment of Meniere’s disease: A prospective, randomized, double-blind, crossover trial. Am. J. Otol. 1998, 19, 196–201. [Google Scholar] [PubMed]
- Takeda, T.; Takeda, S.; Kakigi, A. Effects of Glucocorticoids on the Inner Ear. Front. Surg. 2021, 7, 157. [Google Scholar] [CrossRef]
- Elzayat, S.; Elsherif, H.; Hegazy, H.; Gabr, T.; El-Tahan, A.-R. Tinnitus: Evaluation of Intratympanic Injection of Combined Lidocaine and Corticosteroids. ORL 2016, 78, 159–166. [Google Scholar] [CrossRef]
- Qnouch, A.; Solarczyk, V.; Verin, J.; Tourrel, G.; Stahl, P.; Danede, F.; Willart, J.; Lemesre, P.; Vincent, C.; Siepmann, J. Dexamethasone-loaded cochlear implants: How to provide a desired “burst release”. Int. J. Pharm. X 2021, 3, 100088. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, H.A.; Pich, A.; Schröder, A.; Scheper, V.; Lilli, G.; Reuter, G.; Lenarz, T. Proteome Analysis of Human Perilymph Using an Intraoperative Sampling Method. J. Proteome Res. 2017, 16, 1911–1923. [Google Scholar] [CrossRef]
- O’Leary, S.; Monksfield, P.; Kel, G.; Connolly, T.; Souter, M.; Chang, A.; Marovic, P.; O’Leary, J.; Richardson, R.; Eastwood, H. Relations between cochlear histopathology and hearing loss in experimental cochlear implantation. Hear. Res. 2013, 298, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadol, J.B.; Burgess, B.J.; Gantz, B.; Coker, N.J.; Ketten, D.R.; Kos, I.; Roland, J.J.T.; Shiao, J.Y.; Eddington, D.K.; Montandon, P.; et al. Histopathology of Cochlear Implants in Humans. Ann. Otol. Rhinol. Laryngol. 2001, 110, 883–891. [Google Scholar] [CrossRef]
- Kamakura, T.; Nadol, J.B. Correlation between word recognition score and intracochlear new bone and fibrous tissue after cochlear implantation in the human. Hear. Res. 2016, 339, 132–141. [Google Scholar] [CrossRef] [Green Version]
- Maeda, K.; Yoshida, K.; Ichimiya, I.; Suzuki, M. Dexamethasone inhibits tumor necrosis factor-α-induced cytokine secretion from spiral ligament fibrocytes. Hear. Res. 2005, 202, 154–160. [Google Scholar] [CrossRef]
- Wilk, M.; Hessler, R.; Mugridge, K.; Jolly, C.; Fehr, M.; Lenarz, T.; Scheper, V. Impedance Changes and Fibrous Tissue Growth after Cochlear Implantation Are Correlated and Can Be Reduced Using a Dexamethasone Eluting Electrode. PLoS ONE 2016, 11, e0147552. [Google Scholar] [CrossRef]
- Dinh, C.; Haake, S.; Chen, S.; Hoang, K.; Nong, E.; Eshraghi, A.; Balkany, T.; Van De Water, T. Dexamethasone protects organ of corti explants against tumor necrosis factor-alpha–induced loss of auditory hair cells and alters the expression levels of apoptosis-related genes. Neuroscience 2008, 157, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Connolly, T.M.; Eastwood, H.; Kel, G.; Lisnichuk, H.; Richardson, R.; O’Leary, S. Pre-Operative Intravenous Dexamethasone Prevents Auditory Threshold Shift in a Guinea Pig Model of Cochlear Implantation. Audiol. Neurotol. 2011, 16, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Jolly, C.; Braun, S.; Janssen, T.; Scherer, E.; Steinhoff, J.; Ebenhoch, H.; Lohner, A.; Stark, T.; Kiefer, J. Effects of a dexamethasone-releasing implant on cochleae: A functional, morphological and pharmacokinetic study. Hear. Res. 2015, 327, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Bas, E.; Bohorquez, J.; Goncalves, S.; Perez, E.; Dinh, C.T.; Garnham, C.; Hessler, R.; Eshraghi, A.A.; Van De Water, T.R. Electrode array-eluted dexamethasone protects against electrode insertion trauma induced hearing and hair cell losses, damage to neural elements, increases in impedance and fibrosis: A dose response study. Hear. Res. 2016, 337, 12–24. [Google Scholar] [CrossRef]
- Hütten, M.; Dhanasingh, A.; Hessler, R.; Stöver, T.; Esser, K.-H.; Möller, M.; Lenarz, T.; Jolly, C.; Groll, J.; Scheper, V. In Vitro and In Vivo Evaluation of a Hydrogel Reservoir as a Continuous Drug Delivery System for Inner Ear Treatment. PLoS ONE 2014, 9, e104564. [Google Scholar] [CrossRef] [PubMed]
- Manrique-Huarte, R.; Zulueta-Santos, C.; Calavia, D.; de Linera-Alperi, M.; Gallego, M.A.; Jolly, C.; Manrique, M. Cochlear Implantation With a Dexamethasone Eluting Electrode Array: Functional and Anatomical Changes in Non-Human Primates. Otol. Neurotol. 2020, 41, e812–e822. [Google Scholar] [CrossRef]
- Hyakumura, T.; McDougall, S.; Finch, S.; Needham, K.; Dottori, M.; Nayagam, B.A. Organotypic Cocultures of Human Pluripotent Stem Cell Derived-Neurons with Mammalian Inner Ear Hair Cells and Cochlear Nucleus Slices. Stem Cells Int. 2019, 2019, 8419493. [Google Scholar] [CrossRef] [Green Version]
- Scheper, V.; Hessler, R.; Hütten, M.; Wilk, M.; Jolly, C.; Lenarz, T.; Paasche, G. Local inner ear application of dexamethasone in cochlear implant models is safe for auditory neurons and increases the neuroprotective effect of chronic electrical stimulation. PLoS ONE 2017, 12, e812–e822. [Google Scholar] [CrossRef] [Green Version]
- Wei, B.P.C.; Stathopoulos, D.; O’Leary, S. Steroids for idiopathic sudden sensorineural hearing loss. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Jia, H.; François, F.; Bourien, J.; Eybalin, M.; Lloyd, R.; Van De Water, T.; Puel, J.-L.; Venail, F. Prevention of trauma-induced cochlear fibrosis using intracochlear application of anti-inflammatory and antiproliferative drugs. Neuroscience 2016, 316, 261–278. [Google Scholar] [CrossRef] [PubMed]
- Salt, A.N.; Plontke, S.K. Steroid Nomenclature in Inner Ear Therapy. Otol. Neurotol. 2020, 41, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.E.; Frangou-Polyzois, M.J.; Polyzois, G.L. In vitro biocompatibility of denture relining materials. Gerodontology 2006, 23, 17–22. [Google Scholar] [CrossRef]
- Devi, N.; Dutta, J. Preparation and characterization of chitosan-bentonite nanocomposite films for wound healing application. Int. J. Biol. Macromol. 2017, 104, 1897–1904. [Google Scholar] [CrossRef]
- Bas, E.; Gupta, C.; Van De Water, T.R. A Novel Organ of Corti Explant Model for the Study of Cochlear Implantation Trauma. Anat. Rec. Adv. Integr. Anat. Evol. Biol. 2012, 295, 1944–1956. [Google Scholar] [CrossRef] [PubMed]
- Zia, K.; Ashraf, S.; Jabeen, A.; Saeed, M.; Nur-E-Alam, M.; Ahmed, S.; Al-Rehaily, A.J.; Ul-Haq, Z. Identification of potential TNF-α inhibitors: From in silico to in vitro studies. Sci. Rep. 2020, 10, 20974. [Google Scholar] [CrossRef]
- Lien, K.-C.; Mooney, B.; DeLancey, J.O.L.; Ashton-Miller, J.A. Levator ani muscle stretch induced by simulated vaginal birth. Obstet. Gynecol. 2004, 103, 31–40. [Google Scholar] [CrossRef]
- Ahmadi, N.; Gausterer, J.C.; Honeder, C.; Mötz, M.; Schöpper, H.; Zhu, C.; Saidov, N.; Gabor, F.; Arnoldner, C. Long-term effects and potential limits of intratympanic dexamethasone-loaded hydrogels combined with dexamethasone-eluting cochlear electrodes in a low-insertion trauma Guinea pig model. Hear. Res. 2019, 384, 107825. [Google Scholar] [CrossRef] [PubMed]
- James, D.P.; Eastwood, H.; Richardson, R.; O’Leary, S.J. Effects of Round Window Dexamethasone on Residual Hearing in a Guinea Pig Model of Cochlear Implantation. Audiol. Neurotol. 2007, 13, 86–96. [Google Scholar] [CrossRef]
- Souter, M.; Eastwood, H.; Marovic, P.; Kel, G.; Wongprasartsuk, S.; Ryan, A.F.; O’Leary, S.J. Systemic Immunity Influences Hearing Preservation in Cochlear Implantation. Otol. Neurotol. 2012, 33, 532–538. [Google Scholar] [CrossRef] [Green Version]
- Alexander, T.H.; Harris, J.P.; Nguyen, Q.T.; Vorasubin, N. Dose Effect of Intratympanic Dexamethasone for Idiopathic Sudden Sensorineural Hearing Loss. Otol. Neurotol. 2015, 36, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Lyu, A.-R.; Kim, D.H.; Lee, S.H.; Shin, D.-S.; Shin, S.-A.; Park, Y.-H. Effects of dexamethasone on intracochlear inflammation and residual hearing after cochleostomy: A comparison of administration routes. PLoS ONE 2018, 13, e0195230. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, R.S.; Loquet, G.; Leib, S.L. Limited Efficacy of Adjuvant Therapy with Dexamethasone in Preventing Hearing Loss Due to Experimental Pneumococcal Meningitis in the Infant Rat. Pediatr. Res. 2007, 62, 291–294. [Google Scholar] [CrossRef] [Green Version]
- Plontke, S.K.; Glien, A.; Rahne, T.; Mäder, K.; Salt, A. Controlled Release Dexamethasone Implants in the Round Window Niche for Salvage Treatment of Idiopathic Sudden Sensorineural Hearing Loss. Otol. Neurotol. 2014, 35, 1168–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salt, A.N.; Plontke, S.K. Pharmacokinetic principles in the inner ear: Influence of drug properties on intratympanic applications. Hear. Res. 2018, 368, 28–40. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviation | Formula | Molecular Weight(g/mol) | CAS-No. | Manufacturer, Article-No. | Comment |
|---|---|---|---|---|---|
| DEX-med | C22H29FO5 | 392.46 | 50-02-2 | Caesar & Loretz GmbH, Hilden, Germany; 2211 | Recipe substance for pharmaceutical formulations or active pharmaceutical ingredients; powder |
| DEX-lab | C22H29FO5 | 392.46 | 50-02-2 | Sigma-Aldrich, St. Louis, MO, USA; PHR1526 | Laboratory chemical; powder |
| DPS-med | C22H28FNa2O8P | 516.4 | 50-02-2 | MerckSerono, Darmstadt, Germany; 7880135315 | Fortecortin® Inject 4 mg; approved drug, solution |
| DPS-lab | C22H28FNa2O8P | 516.4 | 2392-39-4 | Sigma-Aldrich, St. Louis, MO, USA; D0720000 | Laboratory chemical, manufactural substances; powder |
| DEX Formulation | ||||
|---|---|---|---|---|
| Concentration | DEX-Med, DEX-Lab; 392.46 g/mol | DPS-Med, DPS-Lab; 516.4 g/mol | ||
| µM | mg/mL | µg/mL | mg/mL | µg/mL |
| 0.03 | 1.18 × 10−5 | 0.0118 | 1.55 × 10−5 | 0.0155 |
| 0.3 | 1.18 × 10−4 | 0.1177 | 1.55 × 10−4 | 0.1549 |
| 3 | 1.18 × 10−3 | 1.177 | 1.55 × 10−3 | 1.5492 |
| 30 | 1.18 × 10−2 | 11.77 | 1.55 × 10−2 | 1.5492 |
| 60 | 2.36 × 10−2 | 23.55 | 3.10 × 10−2 | 30.984 |
| 150 | 5.89 × 10−2 | 23.55 | 7.75 × 10−2 | 77.46 |
| 300 | 0.118 | 117.74 | 0.155 | 154.92 |
| 600 | 0.235 | 235.48 | 0.310 | 154.92 |
| 900 | 0.353 | 353.21 | 0.465 | 464.76 |
| 1000 | 0.392 | 392.46 | 0.516 | 516.4 |
| 2000 | 0.784 | 784.92 | 1.03 | 1032.8 |
| 4000 | 1.60 | 1569.84 | 2.07 | 2065.6 |
| 8000 | 3.14 | 3139.68 | 4.13 | 4131.2 |
| 10,000 | 3.92 | 3924.6 | 5.16 * | 5164 * |
| Concentration (µM) | ||||||||
|---|---|---|---|---|---|---|---|---|
| 0.03–300 | 600 | 900 | 1000 | 2000 | 4000 | 8000 | 10,000 | |
| DEX-lab | n.s. | 0.9998 | 0.9546 | 0.0562 | 0.0990 | 0.0140 | 0.0024 | 0.0013 |
| DEX-med | n.s. | 0.9994 | 0.4153 | 0.6045 | 0.6919 | 0.0293 | 0.0053 | 0.0014 |
| DPS-lab | n.s. | 0.8198 | 0.0926 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| DPS-med | n.s. | 0.9161 | 0.9997 | 0.7436 | <0.0001 | <0.0001 | <0.0001 | - |
| Dexamethasone Formulation, Molecular Weight | Reference | Study Type | Delivery Method | Concentration (mg/mL) * | Remarks |
|---|---|---|---|---|---|
| DEX-lab, 392.46 g/mol | Connolly et al., 2011 [24] | In vivo | i.v. prior to CI | 0.0002; 0.002 | Lower dose failed to maintain ABR thresholds. High-dose treatment resulted in a reduction of ABR threshold shift. |
| Kuthubutheen et al., 2014 [6] | In vivo | i.p. | 0.002 | Spiral ganglion neuron (SGN) density was increased compared to traumatized controls. | |
| Jia et al., 2016 [32] | In vitro; in vivo | explants; pump based delivery (1 µL/h, 7 days); | 0.00117; 0.0117; 0.117; 0.117 | In vitro: 0.00117 and 0.0117 mg/mL start to have toxic effects on outer hair cells, 0.117 mg/mL is toxic for inner and outer hair cells; in vivo: 0.117 mg/mL is toxic for SGN but improves ABR thresholds at selected frequencies. | |
| Takeda et al., 2021 [14] | In vivo | i.p. | 0.002 | No effect. | |
| DEX-med, 392.46 g/mol | Serrano Cardona et al., 2013 [38] | Clinical | DEX in PLGA polymer | 0.7 | Mean hearing threshold improved. |
| Bas et al., 2016 [26] | In vivo | DEX in CI silicone; 0.1% = 13 ng/day, 1.0% = 60 ng/day and 10% = 161 ng/day | 1; 10; 100 | 10% and 1.0% protected against electrode insertion-induced HC loss, but increased ABR and CAP thresholds and impedance, fibrosis and loss of cochlear nerve elements. | |
| Wilk et al., 2016 [22] | In vivo | DEX in CI silicone (16 ng/day and 49 ng/day) | 10; 100 | Reduced impedances and fibrous tissue growth; increased hearing thresholds. | |
| Scheper et al., 2017 [30] | In vivo | DEX in CI silicone (16 ng/day and 49 ng/day; i.e., 0.66 ng/h and 2.04 ng/h) | 10; 100 | Normal SGN number and increased soma diameter. | |
| Ahmadi et al., 2019 [39] | In vivo | 6% DEX loaded hydrogel and DEX containing CI | 60 | Auditory nerve fiber protection. | |
| DPS-lab, 516.40 g/mol | James et al., 2008 [40] | In vivo | i.t.; 5 µL of 2% | 20 | Residual hearing preservation. |
| Souter et al., 2009 [41] | In vivo | i.t., 20% in sponge | 200 | Hearing protection at lower concentrations. | |
| Hütten et al., 2014 [27] | In vitro, In vivo | StarPEG-hydrogel filled reservoir, (50 µg DEX/µL hydrogel, 0.35 μg DEX/h) | 50; 50 | Hearing protection, reduced fibrosis. | |
| Alexander et al., 2015 [42] | Clinical | DEX i.t., four injections in two weeks | 10; 24 | Recovery of hearing threshold after SSNHL. | |
| Scheper et al., 2017 [30] | In vivo | StarPEG-hydrogel filled reservoir, (50 µg DPS-lab/µL hydrogel, 0.35 μg DEX/h) | 50 | Biocompatible regarding SGN number and soma diameter. | |
| Lyu et al., 2018 [43] | In vivo | i.c., i.t. and i.p. | 5; 5; 0.01 | 5 but not 0.01 mg/mL preserved hearing in cochlear implanted animals. | |
| Ahmadi et al., 2018 [39] | Clinical | Temporarily implanted catheter (4 mg/mL/day) | 4 | No effect. | |
| DPS-med, 516.40 g/mol | Coimbra et al., 2007 [44] | In vivo | i.p. every 8 h | 0.0007 | Not effective in preventing neuron loss in pneumococcal meningitis-induced hearing loss. |
| Berjis et al., 2016 [9] | Clinical | i.t. (4 mg/mL/day) | 4 | Hearing improvement. | |
| Scheper et al., 2017 [30] | In vivo | osmotic pump (25 pg/h) | 0.0001 | Biocompatible regarding SGN number, decreased soma diameter; with electrical stimulation: increased SGN number. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Z.; Schwieger, J.; Matin-Mann, F.; Behrens, P.; Lenarz, T.; Scheper, V. Dexamethasone for Inner Ear Therapy: Biocompatibility and Bio-Efficacy of Different Dexamethasone Formulations In Vitro. Biomolecules 2021, 11, 1896. https://doi.org/10.3390/biom11121896
Gao Z, Schwieger J, Matin-Mann F, Behrens P, Lenarz T, Scheper V. Dexamethasone for Inner Ear Therapy: Biocompatibility and Bio-Efficacy of Different Dexamethasone Formulations In Vitro. Biomolecules. 2021; 11(12):1896. https://doi.org/10.3390/biom11121896
Chicago/Turabian StyleGao, Ziwen, Jana Schwieger, Farnaz Matin-Mann, Peter Behrens, Thomas Lenarz, and Verena Scheper. 2021. "Dexamethasone for Inner Ear Therapy: Biocompatibility and Bio-Efficacy of Different Dexamethasone Formulations In Vitro" Biomolecules 11, no. 12: 1896. https://doi.org/10.3390/biom11121896
APA StyleGao, Z., Schwieger, J., Matin-Mann, F., Behrens, P., Lenarz, T., & Scheper, V. (2021). Dexamethasone for Inner Ear Therapy: Biocompatibility and Bio-Efficacy of Different Dexamethasone Formulations In Vitro. Biomolecules, 11(12), 1896. https://doi.org/10.3390/biom11121896