Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis



 ,
, 

Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Laboratory Determinations
- NT (-SH), determined by spectrophotometric method, expressed as μmol/L serum;
- TT (-SH + -S-S-), determined by spectrophotometric method, expressed as μmol/L serum;
- DS (-S-S), determined by spectrophotometric method, expressed as μmol/L serum;
- DS/NT (-S-S- × 100 / -SH) was calculated;
- DS/TT (-S-S- × 100 / -SH + -S-S-) was calculated;
- NT/TT (-SH × 100 / -SH + -S-S-) was calculated.
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid peroxidation: Production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid. Med. Cell Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef] [PubMed]
- Semchyshyn, H.M.; Lushchak, V.I. Interplay between oxidative and carbonyl stresses: Molecular mechanisms, biological effects and therapeutic strategies of protection. In Oxidative Stress-Molecular Mechanisms and Biological Effects; Lushchak, V., Ed.; IntechOpen: Rijeka, Croatia, 2012; pp. 15–46. [Google Scholar]
- Hwang, S.W.; Lee, Y.M.; Aldini, G.; Yeum, K.J. Targeting reactive carbonyl species with natural sequestering agents. Molecules 2016, 21, 280. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, I.; Ene, C.D.; Georgescu, S.R.; Tampa, M.; Matei, C.; Ceausu, E. Effects of UV radiation and oxidative DNA adduct 8-hydroxy-2′-deoxiguanosine on the skin diseases. Rev. Chim. 2014, 65, 1036–1043. [Google Scholar]
- Georgescu, S.R.; Ene, C.D.; Tampa, M.; Matei, C.; Benea, V.; Nicolae, I. Oxidative stress-related markers and alopecia areata. Mater. Plast. 2016, 53, 522–526. [Google Scholar]
- Barrera, G.; Pizzimenti, S.; Daga, M.; Dianzani, C.; Arcaro, A.; Cetrangolo, G.P.; Giordano, G.; Cucci, M.A.; Graf, M.; Gentile, F. Lipid peroxidation-derived aldehydes, 4-hydroxynonenal and malondialdehyde in aging-related disorders. Antioxidants 2018, 7, 102. [Google Scholar] [CrossRef] [PubMed]
- Matschke, V.; Theiss, C.; Matschke, J. Oxidative stress: The lowest common denominator of multiple diseases. Neural Regen. Res. 2019, 14, 238–241. [Google Scholar] [CrossRef]
- Niki, E. Lipid peroxidation: Physiological levels and dual biological effects. Free Radic. Biol. Med. 2009, 47, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Niki, E. Lipid oxidation in the skin. Free Radic. Res. 2015, 49, 827–834. [Google Scholar] [CrossRef]
- Milkovic, L.; Cipak Gasparovic, A.; Zarkovic, N. Overview on major lipid peroxidation bioactive factor 4-hydroxynonenal as pluripotent growth-regulating factor. Free Radic. Res. 2015, 49, 850–860. [Google Scholar] [CrossRef]
- Jankovic, A.; Saso, L.; Korac, A.; Korac, B. Relation of redox and structural alterations of rat skin in the function of chronological aging. Oxid. Med. Cell Longev. 2019, 2019, 2471312. [Google Scholar] [CrossRef]
- Gladyshev, V.N. The free radical theory of aging is dead. Long live the damage theory! Antioxid. Redox Signal. 2014, 20, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Birlouez-Aragon, I.; Morales, F.; Fogliano, V.; Pain, J.P. The health and technological implications of a better control of neoformed contaminants by the food industry. Pathol. Biol. 2010, 58, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Colombo, G.; Aldini, G.; Orioli, M.; Giustarini, D.; Gornati, R.; Rossi, R.; Dalle-Donne, I. Water-soluble α-, β-unsaturated aldehydes of cigarette smoke induce carbonylation of human serum albumin. Antioxid. Redox Signal. 2010, 12, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Dini, L. Phagocytosis of dying cells: Influence of smoking and static magnetic fields. Apoptosis 2010, 15, 1147–1164. [Google Scholar] [CrossRef] [PubMed]
- Becalski, A.; Lau, B.P.; Lewis, D.; Seaman, S.W. Acrylamide in foods: Occurrence, sources, and modeling. J. Agric. Food Chem. 2003, 51, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.; Lee, M.G. Oxidative stress and antioxidant strategies in dermatology. Redox Rep. 2016, 21, 164–169. [Google Scholar] [CrossRef]
- Mishra, S.S.; Maheswari, T.U. Evaluation of oxidative stress in oral lichen planus using malonaldehyde: A systematic review. J. Dermatol. Dermatol. Surg. 2014, 18, 2–7. [Google Scholar] [CrossRef]
- Tavangar, A.; Ghalayani, G.; Alikhani, M.; Amrollahi, N. Assessment of salivary MDA and antioxidant vitamins in patients with erosive type of oral lichen planus and lichenoid reaction. OHDM 2016, 15, 89–92. [Google Scholar]
- Georgescu, S.R.; Ene, C.D.; Nicolae, I.; Musetescu, A.; Matei, C.; Tampa, M. Quantification of urine test strips through reflectometric analysis. Identification of various pathological conditions associated with lichen planus. Rev. Chim. 2017, 68, 1103–1108. [Google Scholar]
- Georgescu, S.R.; Tampa, M.; Mitran, M.I.; Mitran, C.I.; Sarbu, M.I.; Nicolae, I.; Matei, C.; Caruntu, C.; Neagu, M.; Popa, M.I. Potential pathogenic mechanisms involved in the association between lichen planus and hepatitis C virus infection. Exp. Ther. Med. 2019, 17, 1045–1051. [Google Scholar] [CrossRef]
- Gorouhi, F.; Davari, P.; Fazel, N. Cutaneous and mucosal lichen planus: A comprehensive review of clinical subtypes, risk factors, diagnosis, and prognosis. Sci. World J. 2014, 2014, 742826. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, P.A.; Carneiro, S.; Ramos-e-Silva, M. Oral lichen planus: An update on its pathogenesis. Int. J. Dermatol. 2015, 54, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Roopashree, M.R.; Gondhalekar, R.V.; Shashikanth, M.C.; George, J.; Thippeswamy, S.H.; Shukla, A. Pathogenesis of oral lichen planus—A review. J. Oral Pathol. Med. 2010, 39, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Asch, S.; Goldenberg, G. Systemic treatment of cutaneous lichen planus: An update. Cutis 2011, 87, 129–134. [Google Scholar] [PubMed]
- Tvarijonaviciute, A.; Aznar-Cayuela, C.; Rubio, C.P.; Tecles, F.; Ceron, J.J.; López-Jornet, P. Salivary antioxidant status in patients with oral lichen planus: Correlation with clinical signs and evolution during treatment with chamaemelum nobile. Biomed. Res. Int. 2018, 2018, 5187549. [Google Scholar] [CrossRef]
- Jayasekharan, V.P.; Ramya, R.; Rajkumar, K.; Dinesh Kumar, T.; Nandhini, G.; Satish Kumar, S. Estimation of nitric oxide and malondialdehyde in serum and saliva of patients with oral lichen planus. SRM J. Res. Dent. Sci. 2014, 5, 230–236. [Google Scholar] [CrossRef]
- Strange, R.C.; Jones, P.W.; Fryer, A.A. Glutathione S-transferase: Genetics and role in toxicology. Toxicol. Lett. 2000, 112, 357–363. [Google Scholar] [CrossRef]
- Nam, D.H.; Lee, D.W.; Kim, C.H.; Kang, S.G.; Shin, H.S.; Lee, Y.M. Expression of AKR1C3 protein in human keloid skin tissue. Arch. Aesthet. Plast. Surg. 2016, 22, 35–39. [Google Scholar] [CrossRef]
- Mitran, M.I.; Nicolae, I.; Ene, C.D.; Mitran, C.I.; Matei, C.; Ene, C.; Tampa, M.; Georgescu, S.R. Relationship between gamma-glutamyltranspeptidase activity and inflammatory response in lichen planus. Rev. Chim. 2018, 69, 739–743. [Google Scholar]
- Buettner, R.G. Superoxide dismutase in redox biology: The roles of superoxide and hydrogen peroxide. Anticancer Agents Med. Chem. 2011, 11, 341–346. [Google Scholar] [CrossRef]
- Singh, R.; Lemire, J.; Mailloux, R.J.; Appanna, V.D. A novel strategy involved in anti-oxidative defense: The conversion of NADH into NADPH by a metabolic network. PLoS ONE 2008, 3, e2682. [Google Scholar] [CrossRef]
- Kalkan, G.; Emre, S.; Alisik, M.; Aktaş, A.; Baran, P. Dynamic thiol/disulfide homeostasis in patients with lichen planus. J. Clin. Lab. Anal. 2019, 33, e22642. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.C.; Khosla, C. Thiol–Disulfide exchange reactions in the mammalian extracellular environment. Annu. Rev. Chem. Biomol. Eng. 2016, 7, 197–222. [Google Scholar] [CrossRef]
- Kilic, A.; Yorulmaz, A.; Erdogan, S.; Cakmak, S.K.; Guney, E.; Sen, O.; Erel, O. An evaluation of thiol/disulphide homeostasis in patients with psoriasis. Postepy Dermatol. Alergol. 2017, 34, 464–467. [Google Scholar] [CrossRef]
- Akoglu, G.; Neselioglu, S.; Karaismailoglu, E.; Aktas, A.; Erel, O. Plasma thiol levels are associated with disease severity in nonsegmental vitiligo. Indian J. Dermatol. 2018, 63, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Uysal, P.; Avcil, S.; Neşelioğlu, S.; Biçer, C.; Çatal, F. Association of oxidative stress and dynamic thiol-disulphide homeostasis with atopic dermatitis severity and chronicity in children: A prospective study. Clin. Exp. Dermatol. 2018, 43, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Battino, M.; Greabu, M.; Totan, A.; Bullon, P.; Bucur, A.; Tovaru, S.; Mohora, M.; Didilescu, A.; Parlatescu, I.; Spinu, T.; et al. Oxidative stress markers in oral lichen planus. Biofactors 2008, 33, 301–310. [Google Scholar] [CrossRef]
- Shiva, A.; Arab, S. Evaluation of uric acid, total antioxidant and lipid peroxidation parameters in serum and saliva of patients with oral lichen planus. Glob. J. Health Sci. 2016, 8, 225. [Google Scholar] [CrossRef][Green Version]
- Batu, Ş.; Ofluoğlu, D.; Ergun, S.; Warnakulasuriya, S.; Uslu, E.; Güven, Y.; Tanyeri, H. Evaluation of prolidase activity and oxidative stress in patients with oral lichen planus and oral lichenoid contact reactions. J. Oral Pathol. Med. 2016, 45, 281–288. [Google Scholar] [CrossRef]
- Tampa, M.; Nicolae, I.; Ene, C.D.; Sarbu, I.; Matei, C.; Georgescu, S.R. Vitamin C and TBARS in psoriasis vulgaris related to PASI. Rev. Chim. 2017, 68, 43–47. [Google Scholar]
- Ashraf, M.Z.; Srivastava, S. Oxidized phospholipids: Introduction and biological significance. In Lipoproteins—Role in Health and Diseases; InotechOpen: Rijeka, Croatia, 2012; pp. 409–430. [Google Scholar]
- Deigner, H.P.; Hermetter, A. Oxidized phospholipids: Emerging lipid mediators in pathophysiology. Curr. Opin. Lipidol. 2008, 19, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Bochkov, V.; Gesslbauer, B.; Mauerhofer, C.; Philippova, M.; Erne, P.; Oskolkova, O.V. Pleiotropic effects of oxidized phospholipids. Free Radic. Biol. Med. 2017, 111, 6–24. [Google Scholar] [CrossRef] [PubMed]
- Bochkov, V.N.; Oskolkova, O.V.; Birukov, K.G.; Levonen, A.L.; Binder, C.J.; Stöckl, J. Generation and biological activities of oxidized phospholipids. Antioxid. Redox Signal. 2010, 12, 1009–1059. [Google Scholar] [CrossRef] [PubMed]
- Narzt, M.S.; Nagelreiter, I.M.; Oskolkova, O.; Bochkov, V.N.; Latreille, J.; Fedorova, M.; Ni, Z.; Sialana, F.J.; Lubec, G.; Filzwieser, M.; et al. A novel role for NUPR1 in the keratinocyte stress response to UV oxidized phospholipids. Redox Biol. 2019, 20, 467–482. [Google Scholar] [CrossRef] [PubMed]
- Rahal, A.; Kumar, A.; Singh, V.; Yadav, B.; Tiwari, R.; Chakraborty, S.; Dhama, K. Oxidative stress, prooxidants, and antioxidants: The interplay. Biomed. Res. Int. 2014, 2014, 761264. [Google Scholar] [CrossRef] [PubMed]
- Hashemy, S.I.; Gharaei, S.; Vasigh, S.; Kargozar, S.; Alirezaei, B.; Keyhani, F.J.; Amirchghmaghi, M. Oxidative stress factors and C-reactive protein in patients with oral lichen planus before and 2 weeks after treatment. J. Oral Pathol. Med. 2016, 45, 35–40. [Google Scholar] [CrossRef]
- Abdolsamadi, H.; Rafieian, N.; Goodarzi, M.T.; Feradmal, J.; Davoodi, P.; Jazayeri, M.; Taghavi, Z.; Hoseyni, S.M.; Ahmadi-Motamayel, F. Levels of salivary antioxidant vitamins and lipid peroxidation in patients with oral lichen planus and healthy individuals. Chonnam Med. J. 2014, 50, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Mitran, M.I.; Mitran, C.I.; Sarbu, M.I.; Matei, C.; Nicolae, I.; Caruntu, A.; Tocut, S.M.; Popa, M.I.; Caruntu, C.; Georgescu, S.R. Mediators of inflammation—A potential source of biomarkers in oral squamous cell carcinoma. J. Immunol. Res. 2018, 2018, 1061780. [Google Scholar]
- Sezer, E.; Ozugurlu, F.; Ozyurt, H.; Sahin, S.; Etikan, I. Lipid peroxidation and antioxidant status in lichen planus. Clin. Exp. Dermatol. 2007, 32, 430–434. [Google Scholar] [CrossRef]
- Hassan, I.; Keen, A.; Majid, S.; Hassan, T. Evaluation of the antioxidant status in patients of lichen planus in Kashmir valley—A hospital based study. J. Saudi. Soc. Dermatol. Dermatol. Surg. 2013, 17, 13–16. [Google Scholar] [CrossRef]
- Aly, D.G.; Shahin, R.S. Oxidative stress in lichen planus. Acta Dermatovenerol. Alp. Pannonica Adriat. 2010, 19, 3–11. [Google Scholar] [PubMed]
- Panchal, F.H.; Ray, S.; Munshi, R.P.; Bhalerao, S.S.; Nayak, C.S. Alterations in lipid metabolism and antioxidant status in lichen planus. Indian J. Dermatol. 2015, 60, 439–444. [Google Scholar] [PubMed]
- Barikbin, B.; Yousefi, M.; Rahimi, H.; Hedayati, M.; Razavi, S.M.; Lotfi, S. Antioxidant status in patients with lichen planus. Clin. Exp. Dermatol. 2011, 36, 851–854. [Google Scholar] [CrossRef] [PubMed]
- Sander, C.S.; Cooper, S.M.; Ali, I.; Dean, D.; Thiele, J.J.; Wojnarowska, F. Decreased antioxidant enzyme expression and increased oxidative damage in erosive lichen planus of the vulva. BJOG 2005, 112, 1572–1575. [Google Scholar] [CrossRef] [PubMed]
- Kienhöfer, D.; Boeltz, S.; Hoffmann, M.H. Reactive oxygen homeostasis—The balance for preventing autoimmunity. Lupus 2016, 25, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Sharma, R.; Sharma, A.; Awasthi, S.; Awasthi, Y.C. Lipid peroxidation and cell cycle signaling: 4-Hydroxynonenal, a key molecule in stress mediated signaling. Acta Biochim. Pol. 2003, 50, 319–336. [Google Scholar] [PubMed]
- Ellis, E.M. Reactive carbonyls and oxidative stress: Potential for therapeutic intervention. Pharmacol. Ther. 2007, 115, 13–24. [Google Scholar] [CrossRef]
- Forman, H.J. Reactive oxygen species and α-, β-unsaturated aldehydes as second messengers in signal transduction. Ann. N.Y. Acad. Sci. 2010, 1203, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Breitzig, M.; Bhimineni, C.; Lockey, R.; Kolliputi, N. 4-Hydroxy-2-Nonenal: A critical target in oxidative stress? Am. J. Physiol. Cell Physiol. 2016, 311, C537–C543. [Google Scholar] [CrossRef] [PubMed]
- Chiyomaru, K.; Nagano, T.; Nishigori, C. Polymorphisms of glutathione S-transferase in skin cancers in a Japanese population. Kobe J. Med. Sci. 2011, 57, E11–E16. [Google Scholar]
- Biswas, S.; Chida, A.S.; Rahman, I. Redox modifications of protein-thiols: Emerging roles in cell signaling. Biochem. Pharmacol. 2006, 71, 551–564. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, J. (Ed.) Oxidative Injury in Dermatopathology; Springer: Berlin, Germany, 1992. [Google Scholar]
- Persson, B.; Andersson, A.; Hultberg, B.; Hansson, C. The redox state of glutathione, cysteine and homocysteine in the extracellular fluid in the skin. Free Radic. Res. 2002, 36, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, R.B.; Carnelio, S.; Shenoy, R.P.; Gyawali, P.; Mukherjee, M. Oxidative stress and antioxidant defense in oral lichen planus and oral lichenoid reaction. Scand. J. Clin. Lab. Invest. 2010, 70, 225–228. [Google Scholar] [CrossRef]
- Mitran, C.I.; Nicolae, I.; Tampa, M.; Mitran, M.I.; Ene, C.D.; Georgescu, S.R. The effect of hepatitis C virus on pro-oxidant status of gamma-glutamyl transpeptidase in patients with lichen planus. Infectio. Ro. 2017, 50, 10–13. [Google Scholar]
- Chuykin, S.V.; Akmalova, G.M.; Izosimov, A.A.; Yegorova, E.G.; Galeev, R.V. The role of iron in the pathogenesis of lichen planus of oral mucosa. J. Pharm. Sci. Res. 2017, 9, 2252–2255. [Google Scholar]
- Erel, O.; Neselioglu, S. A novel and automated assay for thiol/disulphide homeostasis. Clin. Biochem. 2014, 47, 326–332. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| RCSs | Stable Compounds |
|---|---|
| Saturated Monoaldehydes: ethanal, propanal, hexanal | Ketones: acetone, butanone; |
| Unsaturated Aldehydes: acrolein | Alkanes: hexane, heptane, cyclobutane |
| Dicarbonyls: malondialdehyde, glyoxal, methylglyoxal, isolevuglandine, 4-oxo-2-nonenal; | - |
| Hydroxydialdehydes: 4-hydroxy-2-nonenal, 4-hydroxy-2-hexenal: | - |
| Oxidized phospholipids: 1-palmitoyl-2-(5′-oxo-valeroyl)-sn-glycero-3-phosphocholine, 1-palmitoyl- 2-epoxyisoprostane-sn-glycero-3-phosphorylcholine. | - |
| Favourable Effects | Toxic Effects |
|---|---|
| Modulate the Signalling Pathways | Alter the cell signalling pathways |
| Modulate the Cell Proliferation Act as Cytotoxic Agents against Pathogens | Generate ALEs Produce cell dysfunction |
| Parameter | LP Patients | Controls | p Value |
|---|---|---|---|
| 4-HNE (µg/mL) | 7.81 ± 1.96 | 6.15 ± 1.17 | <0.05 * |
| TBARS (µmol/L) MDA (ng/mL) | 4.23 ± 0.59 32.3 ± 6.26 | 1.99 ± 0.23 21.26 ± 2.36 | <0.05 * <0.05 * |
| Parameter | LP Patients | Controls | p Value |
|---|---|---|---|
| TAS (µmol/L) NT (μmol/L) | 269.83 ± 42.63 388.10 ± 11.32 | 316.46 ± 28.76 406.85 ± 9.32 | p < 0.05 * p < 0.05 * |
| TT (μmol/L) DS (μmol/L) DS/NT DS/TT NT/TT | 430.23 ± 9.93 21.06 ± 1.76 5.44 ± 0.58 4.90 ± 0.46 90.20 ± 0.91 | 445.88 ± 9.01 19.52 ± 0.77 4.80 ± 0.24 4.38 ± 0.20 91.24 ± 0.40 | p < 0.05 * p < 0.05 * p < 0.05 * p < 0.05 * p < 0.05 * |
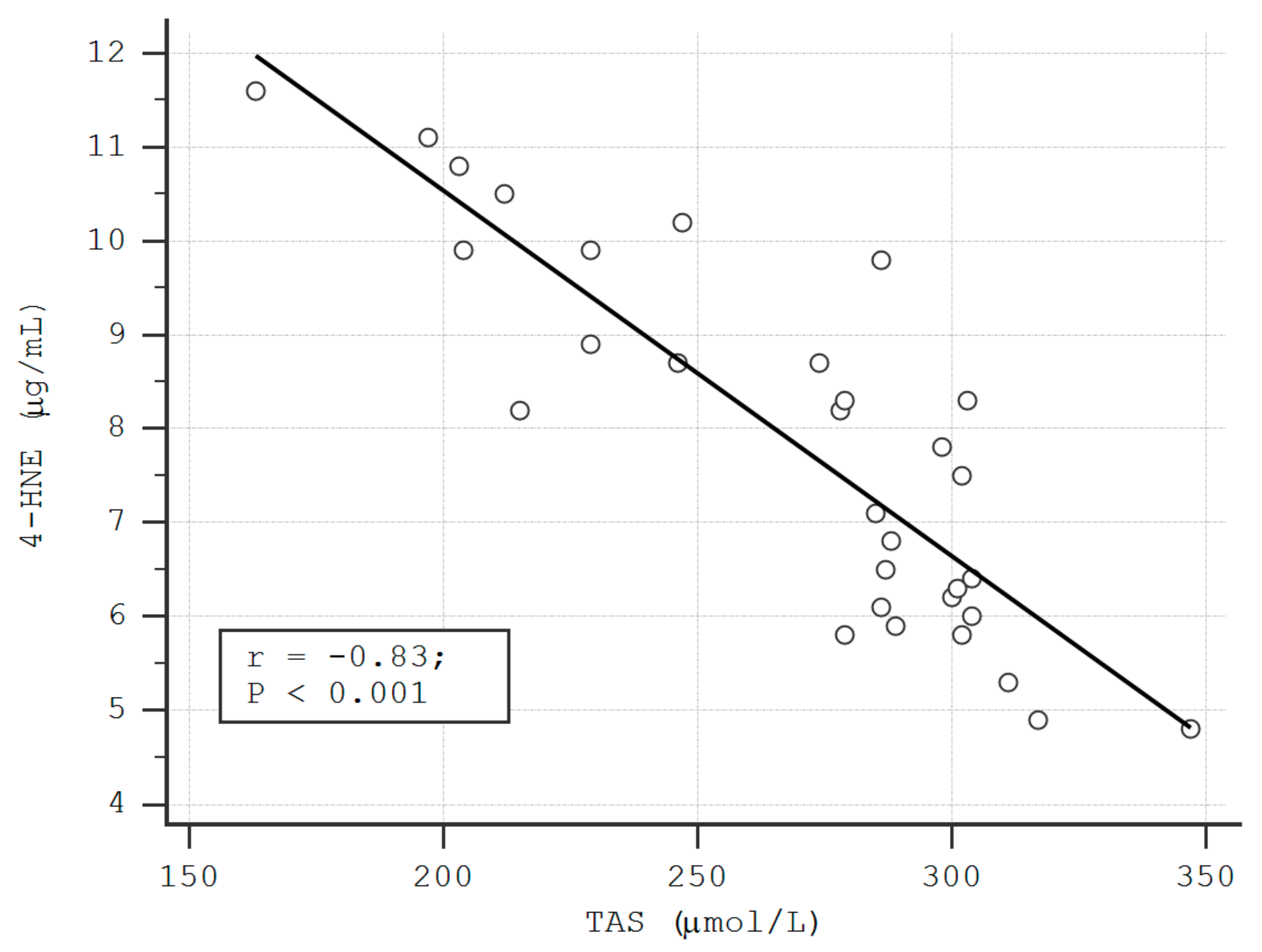
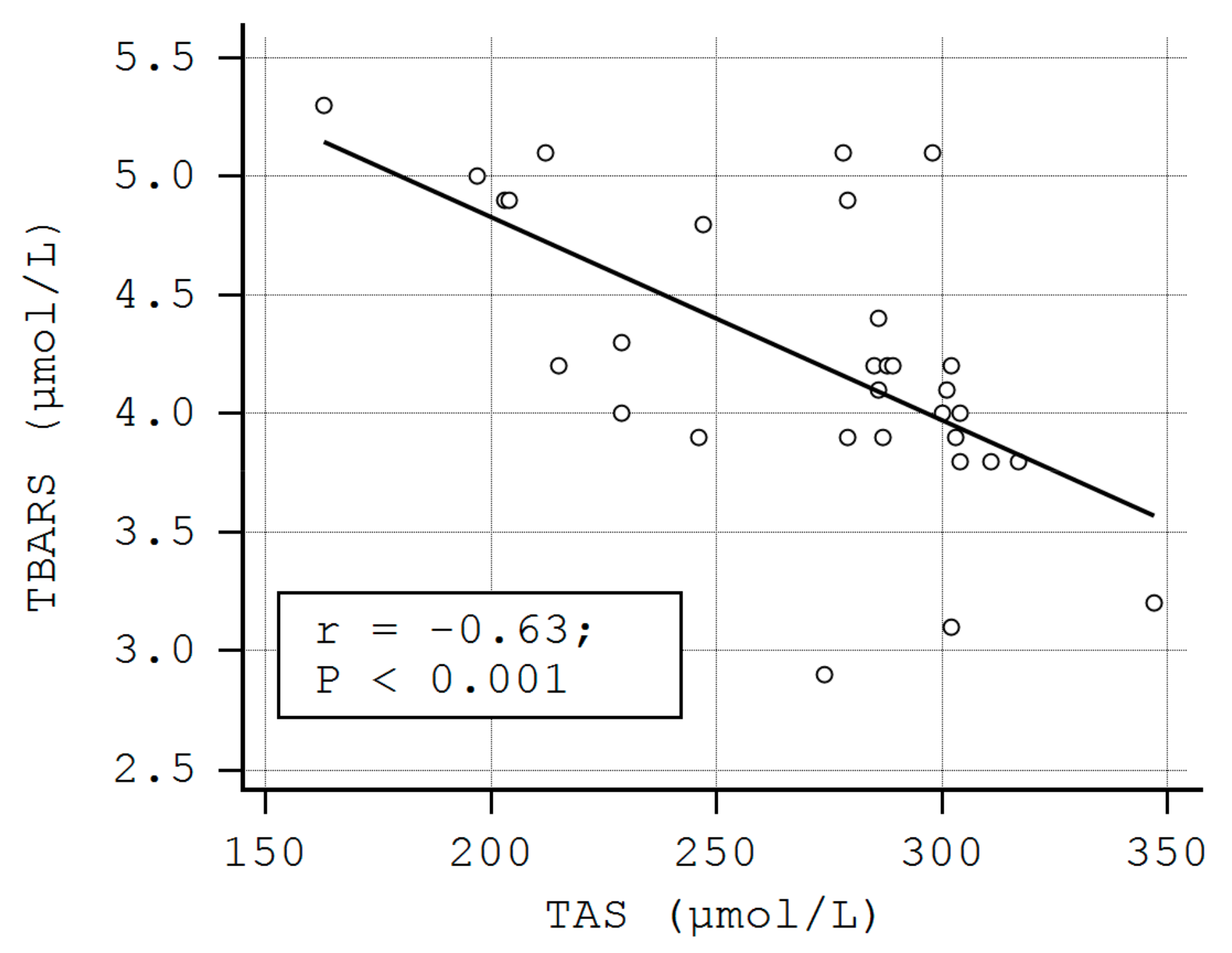
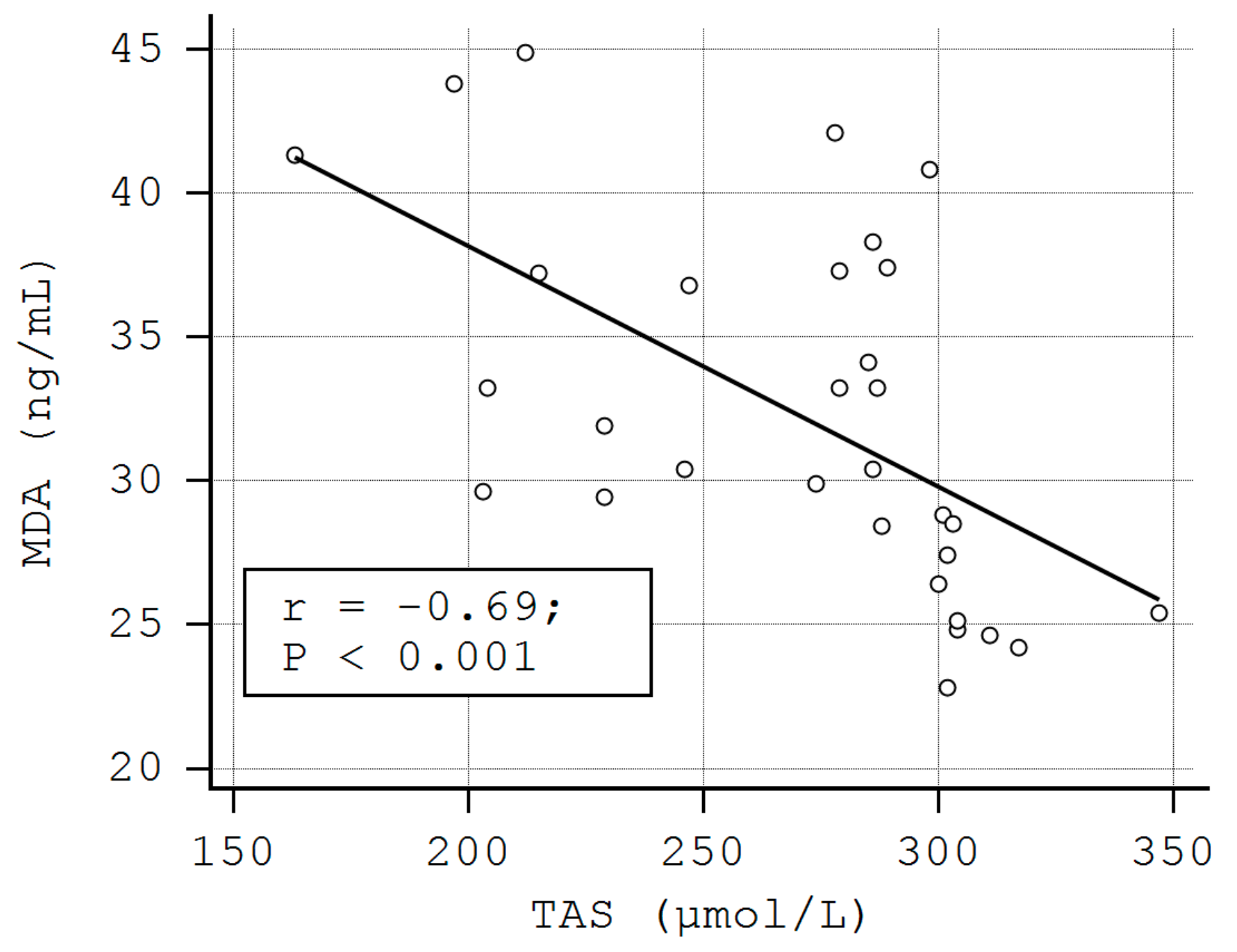
| Parameter | 4-HNE | TBARS | MDA | |||
|---|---|---|---|---|---|---|
| - | rho | p | rho | p | rho | p |
| TAS NT | −0.83 −0.11 | < 0.01 * 0.54 | −0.63 −0.32 | < 0.01 * 0.08 | −0.69 −0.22 | < 0.01 * 0.22 |
| TT | −0.11 | 0.54 | −0.27 | 0.12 | −0.26 | 0.14 |
| DS | 0.14 | 0.43 | 0.20 | 0.26 | 0.03 | 0.86 |
| DS/NT | 0.15 | 0.41 | 0.26 | 0.15 | 0.07 | 0.67 |
| DS/TT | 0.15 | 0.41 | 0.26 | 0.15 | 0.07 | 0.67 |
| NT/TT | −0.15 | 0.41 | −0.26 | 0.15 | −0.07 | 0.67 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitran, M.I.; Nicolae, I.; Tampa, M.; Mitran, C.I.; Caruntu, C.; Sarbu, M.I.; Ene, C.D.; Matei, C.; Georgescu, S.R.; Popa, M.I. Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis. Metabolites 2019, 9, 213. https://doi.org/10.3390/metabo9100213
Mitran MI, Nicolae I, Tampa M, Mitran CI, Caruntu C, Sarbu MI, Ene CD, Matei C, Georgescu SR, Popa MI. Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis. Metabolites. 2019; 9(10):213. https://doi.org/10.3390/metabo9100213
Chicago/Turabian StyleMitran, Madalina Irina, Ilinca Nicolae, Mircea Tampa, Cristina Iulia Mitran, Constantin Caruntu, Maria Isabela Sarbu, Corina Daniela Ene, Clara Matei, Simona Roxana Georgescu, and Mircea Ioan Popa. 2019. "Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis" Metabolites 9, no. 10: 213. https://doi.org/10.3390/metabo9100213
APA StyleMitran, M. I., Nicolae, I., Tampa, M., Mitran, C. I., Caruntu, C., Sarbu, M. I., Ene, C. D., Matei, C., Georgescu, S. R., & Popa, M. I. (2019). Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis. Metabolites, 9(10), 213. https://doi.org/10.3390/metabo9100213