
Unraveling the Evolutionary Diet Mismatch and Its Contribution to the Deterioration of Body Composition

 ,
,  ,
,  ,
, 
 ,
,
Abstract

1. Introduction
2. Whole Foods and Ancestral Diets
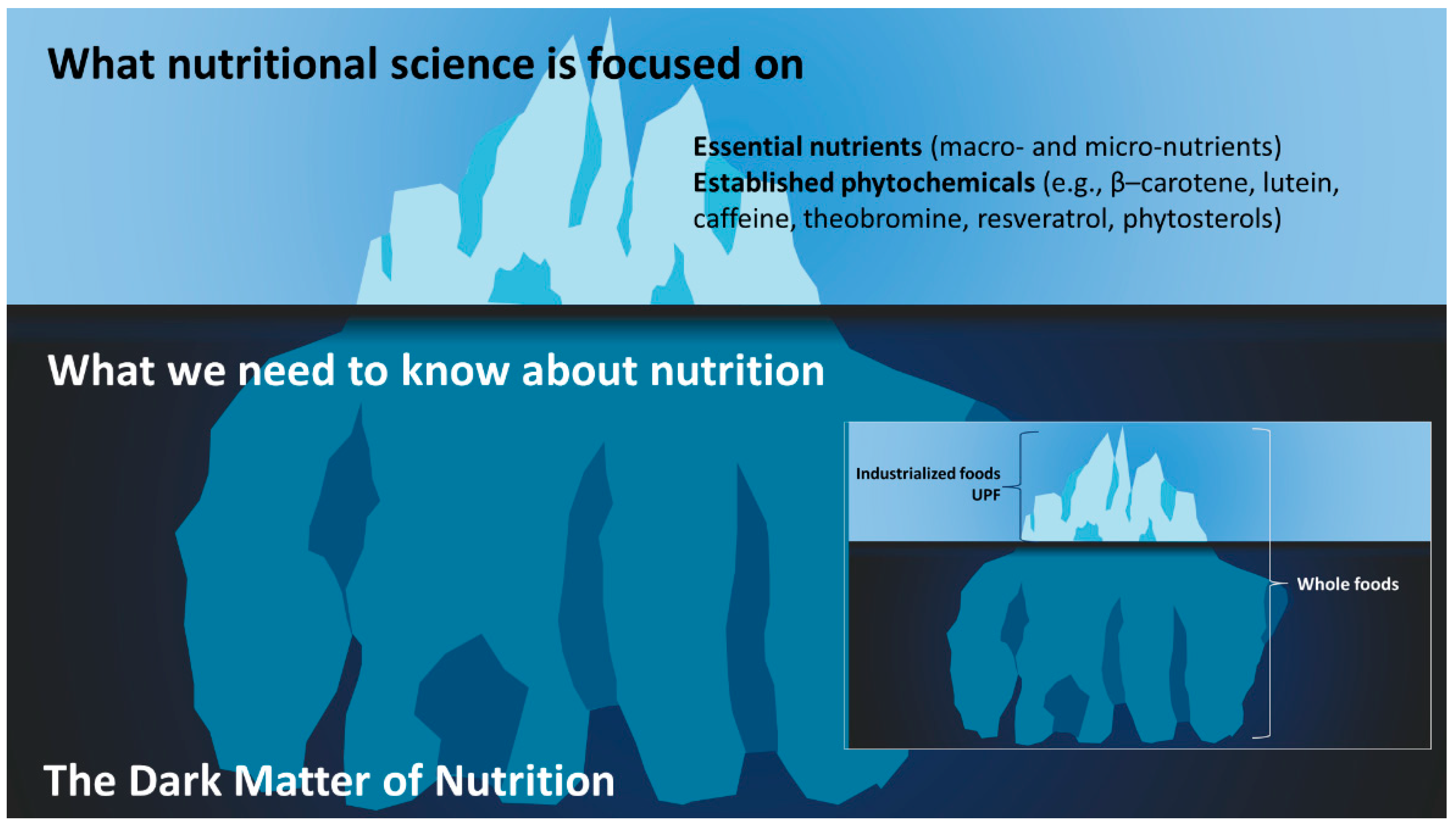
3. The Dark Matter of Nutrition and the Evolutionary Metabolome
3.1. Industrialization of Food and the Metabolome
3.2. Fermented Foods, the Gut, and the Metabolome
4. Ancestral Diets and Body Composition
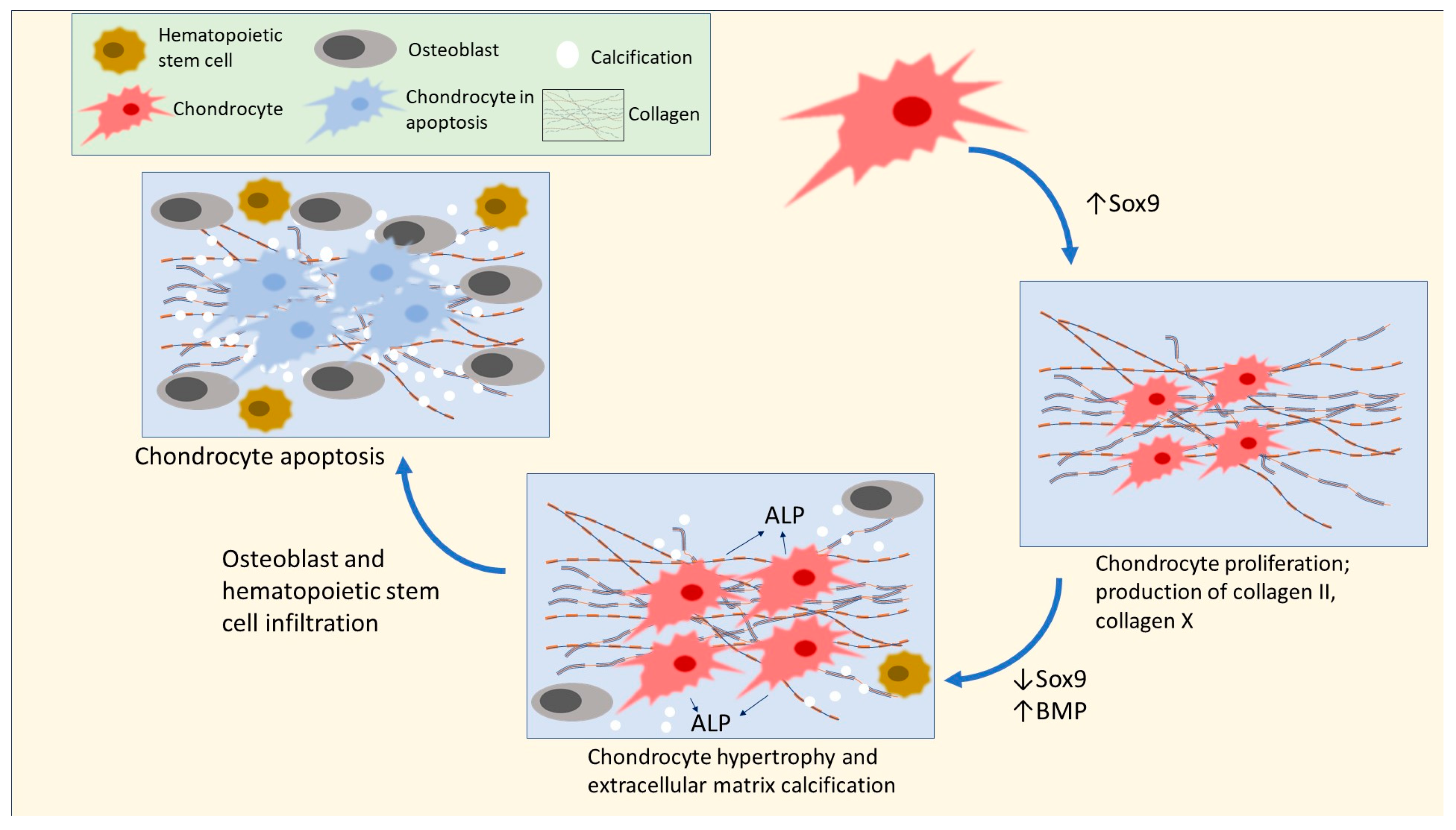
4.1. Focus on Bone
4.2. Focus on Muscle
4.3. Focus on Adipose
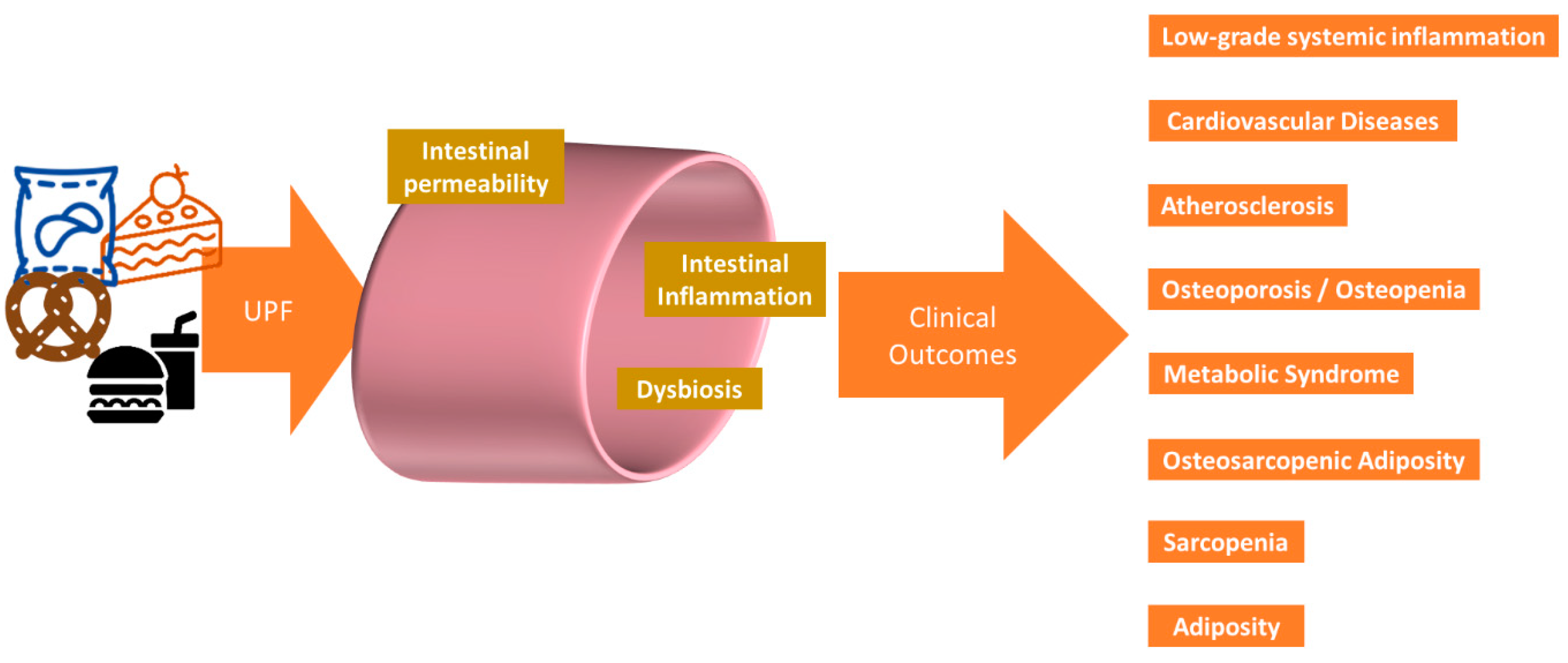
5. The Ultra-Processed Food Conundrum
In the year 4545
Ain’t gonna need your teeth, won’t need your eyes
You won’t find a thing to chew
Nobody’s gonna look at you(Zager and Evans, 1969) [253]
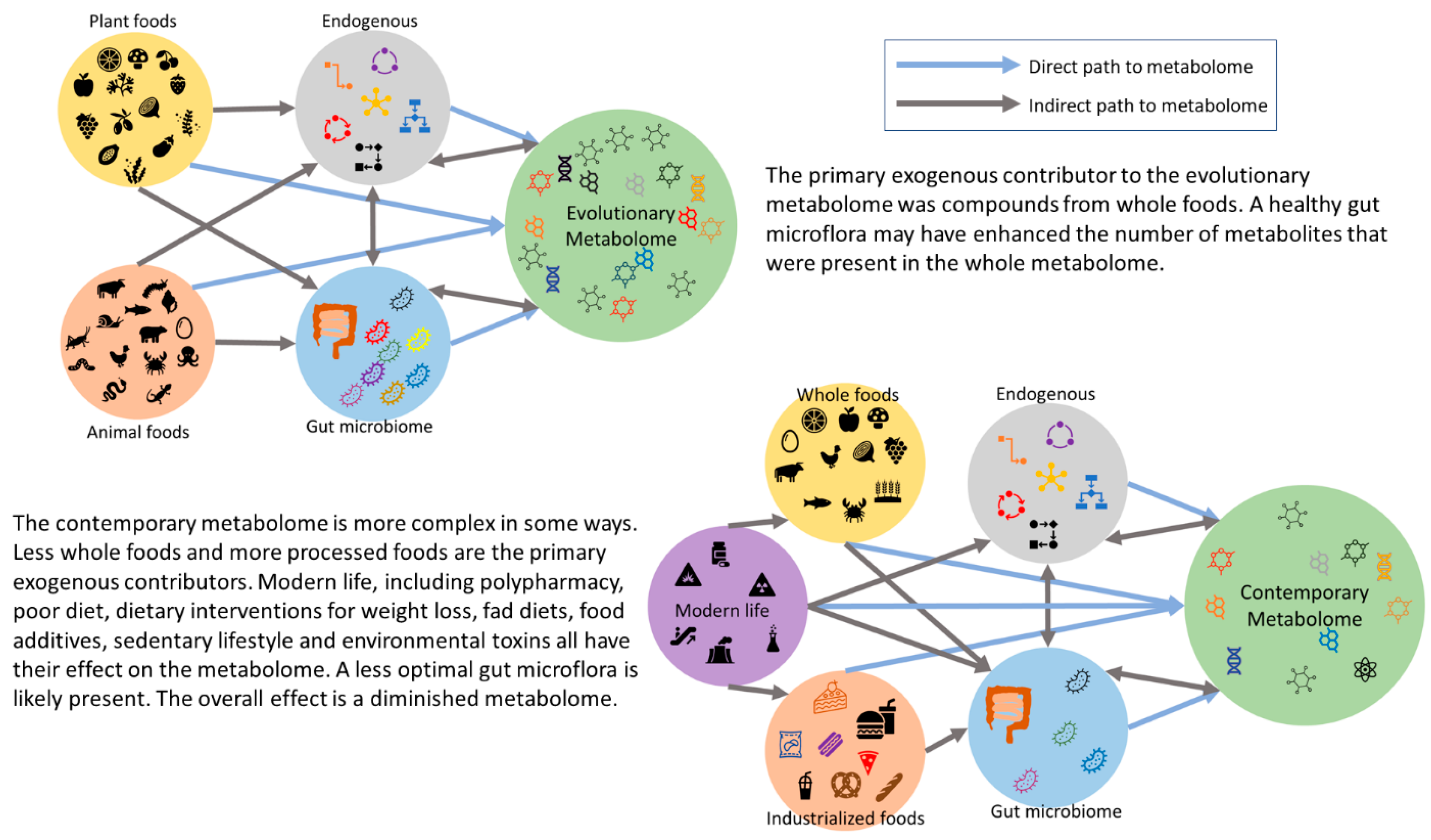
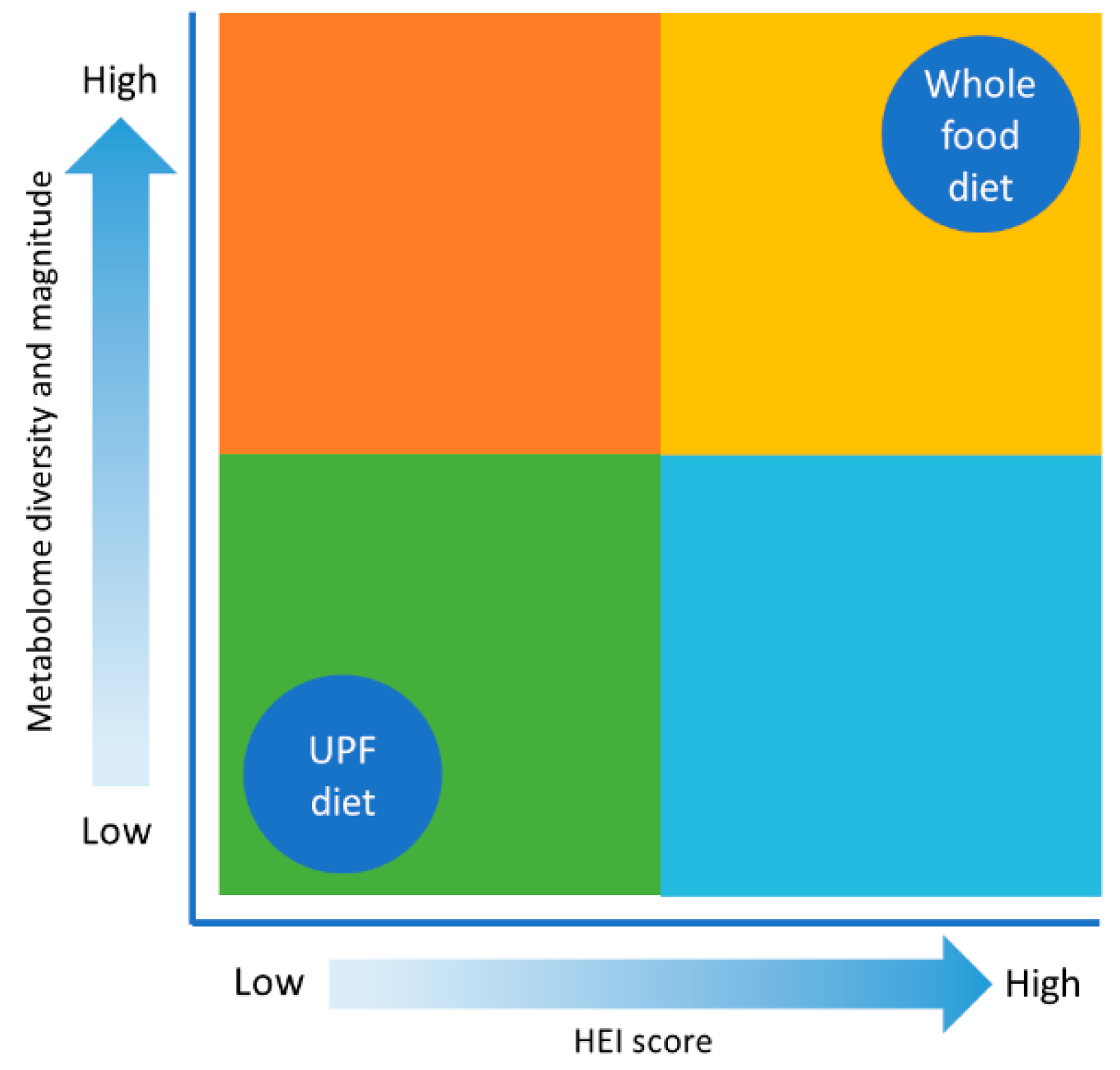
Illustrating How Whole Foods Contribute to the Metabolome
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Hublin, J.J. Paleoanthropology: How old is the oldest human? Curr. Biol. 2015, 25, R453–R455. [Google Scholar] [CrossRef] [PubMed]
- Galway-Witham, J.; Stringer, C. How did Homo sapiens evolve? Science 2018, 360, 1296–1298. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, S.; Hublin, J.-J.; Gunz, P. The evolution of modern human brain shape. Sci. Adv. 2018, 4, eaao5961. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.N. Rethinking the origins of agriculture. Introduction. Curr. Anthropol. 2009, 50, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Kluyver, T.; Preece, C.; Swarbrick, J.; Forster, E.; Wallace, M.; Charles, M.; Rees, M.; Osborne, C.P. The origins of agriculture: Intentions and consequences. J. Archaeol. Sci. 2021, 125, 105290. [Google Scholar] [CrossRef]
- Medicine, I.O. Improving Food Safety through a One Health Approach: Workshop Summary; The National Academies Press: Washington, DC, USA, 2012; p. 418. [Google Scholar]
- Monjotin, N.; Amiot, M.J.; Fleurentin, J.; Morel, J.M.; Raynal, S. Clinical Evidence of the Benefits of Phytonutrients in Human Healthcare. Nutrients 2022, 14, 1712. [Google Scholar] [CrossRef] [PubMed]
- Temple, N.J. The Origins of the Obesity Epidemic in the USA-Lessons for Today. Nutrients 2022, 14, 4253. [Google Scholar] [CrossRef] [PubMed]
- Andrews, P.; Johnson, R.J. Evolutionary basis for the human diet: Consequences for human health. J. Intern. Med. 2020, 287, 226–237. [Google Scholar] [CrossRef]
- Moles, L.; Otaegui, D. The Impact of Diet on Microbiota Evolution and Human Health. Is Diet an Adequate Tool for Microbiota Modulation? Nutrients 2020, 12, 1654. [Google Scholar] [CrossRef]
- Alt, K.W.; Al-Ahmad, A.; Woelber, J.P. Nutrition and Health in Human Evolution-Past to Present. Nutrients 2022, 14, 3594. [Google Scholar] [CrossRef]
- Larsen, C.S. The agricultural revolution as environmental catastrophe: Implications for health and lifestyle in the Holocene. Quat. Int. 2006, 150, 12–20. [Google Scholar] [CrossRef]
- Carlberg, C. Nutrigenomics in the context of evolution. Redox. Biol. 2023, 62, 102656. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez Olmo, B.M.; Butler, M.J.; Barrientos, R.M. Evolution of the Human Diet and Its Impact on Gut Microbiota, Immune Responses, and Brain Health. Nutrients 2021, 13, 196. [Google Scholar] [CrossRef]
- Ben-Dor, M.; Sirtoli, R.; Barkai, R. The evolution of the human trophic level during the Pleistocene. Am. J. Phys. Anthropol. 2021, 175 (Suppl. S72), 27–56. [Google Scholar] [CrossRef]
- Wishart, D.S.; Guo, A.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucleic Acids Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- Park, Y.W.; Nam, M.S. Bioactive Peptides in Milk and Dairy Products: A Review. Korean J. Food Sci. Anim. Resour. 2015, 35, 831–840. [Google Scholar] [CrossRef]
- Mosca, F.; Gianni, M.L. Human milk: Composition and health benefits. Pediatr. Med. Chir. 2017, 39, 155. [Google Scholar] [CrossRef]
- Ahuja, J.K.C.; Casavale, K.O.; Li, Y.; Hopperton, K.E.; Chakrabarti, S.; Hines, E.P.; Brooks, S.P.J.; Bondy, G.S.; MacFarlane, A.J.; Weiler, H.A.; et al. Perspective: Human Milk Composition and Related Data for National Health and Nutrition Monitoring and Related Research. Adv. Nutr. 2022, 13, 2098–2114. [Google Scholar] [CrossRef] [PubMed]
- Yi, D.Y.; Kim, S.Y. Human Breast Milk Composition and Function in Human Health: From Nutritional Components to Microbiome and MicroRNAs. Nutrients 2021, 13, 3094. [Google Scholar] [CrossRef]
- Vizzari, G.; Morniroli, D.; Ceroni, F.; Verduci, E.; Consales, A.; Colombo, L.; Cerasani, J.; Mosca, F.; Gianni, M.L. Human Milk, More Than Simple Nourishment. Children 2021, 8, 863. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, M.; Alvarez-Sanchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef] [PubMed]
- Shams-White, M.M.; Pannucci, T.E.; Lerman, J.L.; Herrick, K.A.; Zimmer, M.; Meyers Mathieu, K.; Stoody, E.E.; Reedy, J. Healthy Eating Index-2020: Review and Update Process to Reflect the Dietary Guidelines for Americans,2020–2025. J. Acad. Nutr. Diet. 2023, 123, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, S.M.; Kelly, O.J.; Krok-Schoen, J.L.; Taylor, C.A. Low Protein Intakes and Poor Diet Quality Associate with Functional Limitations in US Adults with Diabetes: A 2005–2016 NHANES Analysis. Nutrients 2021, 13, 2582. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, S.M.; Jonnalagadda, S.S.; Pisegna, J.L.; Kelly, O.J.; Krok-Schoen, J.L.; Taylor, C.A. Poorer Diet Quality Observed among US Adults with a Greater Number of Clinical Chronic Disease Risk Factors. J. Prim. Care Community Health 2020, 11, 2150132720945898. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; Ruggiero, E.; Esposito, S.; Persichillo, M.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; et al. Ultraprocessed food consumption is associated with all-cause and cardiovascular mortality in participants with type 2 diabetes independent of diet quality: A prospective observational cohort study. Am. J. Clin. Nutr. 2023, 118, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Singh, D. The Paleolithic Diet. Cureus 2023, 15, e34214. [Google Scholar] [CrossRef]
- Alvarez, S.A.; Rocha-Guzman, N.E.; Gonzalez-Laredo, R.F.; Gallegos-Infante, J.A.; Moreno-Jimenez, M.R.; Bravo-Munoz, M. Ancestral Food Sources Rich in Polyphenols, Their Metabolism, and the Potential Influence of Gut Microbiota in the Management of Depression and Anxiety. J. Agric. Food Chem. 2022, 70, 944–956. [Google Scholar] [CrossRef]
- Crittenden, A.N.; Schnorr, S.L. Current views on hunter-gatherer nutrition and the evolution of the human diet. Am. J. Phys. Anthropol. 2017, 162 (Suppl. S63), 84–109. [Google Scholar] [CrossRef]
- Konner, M.; Eaton, S.B. Hunter-gatherer diets and activity as a model for health promotion: Challenges, responses, and confirmations. Evol. Anthropol. 2023, 32, 206–222. [Google Scholar] [CrossRef]
- Lieberman, D.E.; Worthington, S.; Schell, L.D.; Parkent, C.M.; Devinsky, O.; Carmody, R.N. Comparing measured dietary variation within and between tropical hunter-gatherer groups to the Paleo Diet. Am. J. Clin. Nutr. 2023, 118, 549–560. [Google Scholar] [CrossRef]
- Kabukcu, C.; Hunt, C.; Hill, E.; Pomeroy, E.; Reynolds, T.; Barker, G.; Asouti, E. Cooking in caves: Palaeolithic carbonised plant food remains from Franchthi and Shanidar. Antiquity 2023, 97, 12–28. [Google Scholar] [CrossRef]
- Moubtahij, Z.; McCormack, J.; Bourgon, N.; Trost, M.; Sinet-Mathiot, V.; Fuller, B.T.; Smith, G.M.; Temming, H.; Steinbrenner, S.; Hublin, J.J.; et al. Isotopic evidence of high reliance on plant food among Later Stone Age hunter-gatherers at Taforalt, Morocco. Nat. Ecol. Evol. 2024, 8, 1035–1045. [Google Scholar] [CrossRef]
- Olivadese, M.; Dindo, M.L. Edible Insects: A Historical and Cultural Perspective on Entomophagy with a Focus on Western Societies. Insects 2023, 14, 690. [Google Scholar] [CrossRef] [PubMed]
- Fraczek, B.; Pieta, A.; Burda, A.; Mazur-Kurach, P.; Tyrala, F. Paleolithic Diet-Effect on the Health Status and Performance of Athletes? Nutrients 2021, 13, 1019. [Google Scholar] [CrossRef] [PubMed]
- Spreadbury, I. Comparison with ancestral diets suggests dense acellular carbohydrates promote an inflammatory microbiota, and may be the primary dietary cause of leptin resistance and obesity. Diabetes Metab Syndr. Obes. 2012, 5, 175–189. [Google Scholar] [CrossRef]
- Lindeberg, S.; Lundh, B. Apparent absence of stroke and ischaemic heart disease in a traditional Melanesian island: A clinical study in Kitava. J. Intern. Med. 1993, 233, 269–275. [Google Scholar] [CrossRef]
- Lindeberg, S.; Nilsson-Ehle, P.; Terent, A.; Vessby, B.; Schersten, B. Cardiovascular risk factors in a Melanesian population apparently free from stroke and ischaemic heart disease: The Kitava study. J. Intern. Med. 1994, 236, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Amaya-Castellanos, C.; Gamboa-Delgado, E.M.; Santacruz-Chasoy, E.; Pelcastre-Villafuerte, B.E. Loss of ancestral food practices and perception of its effect on children’s health among Inga indigenous grandmothers, Narino, Colombia. BMC Public Health 2022, 22, 1452. [Google Scholar] [CrossRef]
- Dicken, S.J.; Batterham, R.L. The Role of Diet Quality in Mediating the Association between Ultra-Processed Food Intake, Obesity and Health-Related Outcomes: A Review of Prospective Cohort Studies. Nutrients 2021, 14, 23. [Google Scholar] [CrossRef]
- Holmboe-Ottesen, G.; Wandel, M. Changes in dietary habits after migration and consequences for health: A focus on South Asians in Europe. Food Nutr. Res. 2012, 56, 18891. [Google Scholar] [CrossRef] [PubMed]
- Berggreen-Clausen, A.; Hseing Pha, S.; Molsted Alvesson, H.; Andersson, A.; Daivadanam, M. Food environment interactions after migration: A scoping review on low- and middle-income country immigrants in high-income countries. Public Health Nutr. 2022, 25, 136–158. [Google Scholar] [CrossRef] [PubMed]
- Eaton, S.B.; Konner, M. Paleolithic nutrition. A consideration of its nature and current implications. N. Engl. J. Med. 1985, 312, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Boyd Eaton, S.; Shostak, M.; Konner, M. The Paleolithic Prescription: A Program of Diet & Exercise and a Design for Living; Harper Collins: New York City, NY, USA, 1989; p. 320. [Google Scholar]
- Cordain, L. The Paleo Diet: Lose Weight and Get Healthy by Eating the Food You Were Designed to Eat; Wiley: Hoboken, NJ, USA, 2002. [Google Scholar]
- Cordain, L. The Paleo Diet Revised: Lose Weight and Get Healthy by Eating the Foods You Were Designed to Eat; John Wiley & Sons: Hoboken, NJ, USA, 2010; p. 288. [Google Scholar]
- Eaton, S.B.; Cordain, L.; Lindeberg, S. Evolutionary health promotion: A consideration of common counterarguments. Prev. Med. 2002, 34, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Agoulnik, D.; Lalonde, M.P.; Ellmore, G.S.; McKeown, N.M. Part 1: The Origin and Evolution of the Paleo Diet. Nutr. Today 2021, 56, 94–104. [Google Scholar] [CrossRef]
- Bland, J.S. Why the Pegan Diet Makes Sense. Integr. Med. 2021, 20, 16–19. [Google Scholar]
- Voegtlin, W.L. The Stone Age Diet: Based on In-Depth Studies of Human Ecology and the Diet of Man; Vantage Press: Visalia, CA, USA, 1975. [Google Scholar]
- Tahreem, A.; Rakha, A.; Rabail, R.; Nazir, A.; Socol, C.T.; Maerescu, C.M.; Aadil, R.M. Fad Diets: Facts and Fiction. Front. Nutr. 2022, 9, 960922. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K. Popular fad diets: An evidence-based perspective. Prog. Cardiovasc. Dis. 2023, 77, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Wood, B.; Williams, O.; Baker, P.; Sacks, G. Behind the ‘creative destruction’ of human diets: An analysis of the structure and market dynamics of the ultra-processed food manufacturing industry and implications for public health. J. Agrarian Chang. 2023, 23, 811–843. [Google Scholar] [CrossRef]
- Crimarco, A.; Landry, M.J.; Gardner, C.D. Ultra-processed Foods, Weight Gain, and Co-morbidity Risk. Curr. Obes. Rep. 2022, 11, 80–92. [Google Scholar] [CrossRef]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Vitale, M.; Costabile, G.; Testa, R.; D’Abbronzo, G.; Nettore, I.C.; Macchia, P.E.; Giacco, R. Ultra-Processed Foods and Human Health: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2024, 15, 100121. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, S.; Spiro, A.; Berry, S.; He, J.; Loth, S.; Martinez-Inchausti, A.; Mellor, D.; Raats, M.; Sokolovic, M.; Vijaykumar, S.; et al. How do we differentiate not demonise—Is there a role for healthier processed foods in an age of food insecurity? Proceedings of a roundtable event. Nutr. Bull. 2023, 48, 278–295. [Google Scholar] [CrossRef] [PubMed]
- Valicente, V.M.; Peng, C.H.; Pacheco, K.N.; Lin, L.; Kielb, E.I.; Dawoodani, E.; Abdollahi, A.; Mattes, R.D. Ultraprocessed Foods and Obesity Risk: A Critical Review of Reported Mechanisms. Adv. Nutr. 2023, 14, 718–738. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A. Nutrition and health. The issue is not food, nor nutrients, so much as processing. Public Health Nutr. 2009, 12, 729–731. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Menichetti, G.; Ravandi, B.; Mozaffarian, D.; Barabasi, A.L. Machine learning prediction of the degree of food processing. Nat. Commun. 2023, 14, 2312. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e3. [Google Scholar] [CrossRef] [PubMed]
- Agricultural Research Service. What We Eat in America. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweianhanes-overview/ (accessed on 24 June 2024).
- Mozaffarian, D.; Rosenberg, I.; Uauy, R. History of modern nutrition science-implications for current research, dietary guidelines, and food policy. BMJ 2018, 361, k2392. [Google Scholar] [CrossRef]
- Bland, J.S. The Dark Matter of Nutrition: Dietary Signals beyond Traditional Nutrients. Integr. Med. 2019, 18, 12–15. [Google Scholar]
- Barabási, A.-L.; Menichetti, G.; Loscalzo, J. The unmapped chemical complexity of our diet. Nat. Food 2019, 1, 33–37. [Google Scholar] [CrossRef]
- Petroski, W.; Minich, D.M. Is There Such a Thing as "Anti-Nutrients"? A Narrative Review of Perceived Problematic Plant Compounds. Nutrients 2020, 12, 2929. [Google Scholar] [CrossRef]
- Craig, W.J.; Mangels, A.R.; Fresan, U.; Marsh, K.; Miles, F.L.; Saunders, A.V.; Haddad, E.H.; Heskey, C.E.; Johnston, P.; Larson-Meyer, E.; et al. The Safe and Effective Use of Plant-Based Diets with Guidelines for Health Professionals. Nutrients 2021, 13, 4144. [Google Scholar] [CrossRef]
- Hundal, R.S.; Inzucchi, S.E. Metformin: New understandings, new uses. Drugs 2003, 63, 1879–1894. [Google Scholar] [CrossRef] [PubMed]
- Chaachouay, N.; Zidane, L. Plant-Derived Natural Products: A Source for Drug Discovery and Development. Drugs Drug Candidates 2024, 3, 184–207. [Google Scholar] [CrossRef]
- Townsend, J.R.; Kirby, T.O.; Sapp, P.A.; Gonzalez, A.M.; Marshall, T.M.; Esposito, R. Nutrient synergy: Definition, evidence, and future directions. Front. Nutr. 2023, 10, 1279925. [Google Scholar] [CrossRef] [PubMed]
- Ayyadurai, V.A.S.; Deonikar, P. In Silico Modeling and Quantification of Synergistic Effects of Multi-Combination Compounds: Case Study of the Attenuation of Joint Pain Using a Combination of Phytonutrients. Appl. Sci. 2022, 12, 10013. [Google Scholar] [CrossRef]
- Chen, X.; Li, H.; Zhang, B.; Deng, Z. The synergistic and antagonistic antioxidant interactions of dietary phytochemical combinations. Crit. Rev. Food Sci. Nutr. 2022, 62, 5658–5677. [Google Scholar] [CrossRef]
- Zamboni, N.; Saghatelian, A.; Patti, G.J. Defining the metabolome: Size, flux, and regulation. Mol. Cell 2015, 58, 699–706. [Google Scholar] [CrossRef]
- Handakas, E.; Chang, K.; Khandpur, N.; Vamos, E.P.; Millett, C.; Sassi, F.; Vineis, P.; Robinson, O. Metabolic profiles of ultra-processed food consumption and their role in obesity risk in British children. Clin. Nutr. 2022, 41, 2537–2548. [Google Scholar] [CrossRef]
- Newgard, C.B. Metabolomics and Metabolic Diseases: Where Do We Stand? Cell Metab. 2017, 25, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Su, D.; Chen, J.; Du, S.; Kim, H.; Yu, B.; Wong, K.E.; Boerwinkle, E.; Rebholz, C.M. Metabolomic Markers of Ultra-Processed Food and Incident CKD. Clin. J. Am. Soc. Nephrol. 2023, 18, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Capozzi, F. NMR-Based Metabolomics: The Foodome and the Assessment of Dietary Exposure as a Key Step to Evaluate the Effect of Diet on Health. In Modern Magnetic Resonance; Webb, G.A., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 1687–1707. [Google Scholar]
- Menichetti, G.; Barabasi, A.-L.; Loscalzo, J. Decoding the Foodome: Molecular Networks Connecting Diet and Health; ResearchGate: Berlin, Germany, 2023. [Google Scholar]
- do Valle, I.F.; Roweth, H.G.; Malloy, M.W.; Moco, S.; Barron, D.; Battinelli, E.; Loscalzo, J.; Barabasi, A.L. Network medicine framework shows that proximity of polyphenol targets and disease proteins predicts therapeutic effects of polyphenols. Nat. Food 2021, 2, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Westerman, K.E.; Harrington, S.; Ordovas, J.M.; Parnell, L.D. PhyteByte: Identification of foods containing compounds with specific pharmacological properties. BMC Bioinform. 2020, 21, 238. [Google Scholar] [CrossRef] [PubMed]
- Forde, C.G. Processing the evidence to evaluate mechanisms, costs and future solutions. Nutr. Bull. 2023, 48, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.F.M.; Consolo, N.R.B.; Antonelo, D.S.; Beline, M.; Gagaoua, M.; Higuera-Padilla, A.; Colnago, L.A.; Gerrard, D.E.; Silva, S.L. Impact of Cattle Feeding Strategy on the Beef Metabolome. Metabolites 2022, 12, 640. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; Sanchez-Garcia, C. Nutritional Composition of Game Meat from Wild Species HArvested in Europe; Intechopen: London, UK, 2021; p. 232. [Google Scholar]
- Nogoy, K.M.C.; Sun, B.; Shin, S.; Lee, Y.; Zi Li, X.; Choi, S.H.; Park, S. Fatty Acid Composition of Grain- and Grass-Fed Beef and Their Nutritional Value and Health Implication. Food Sci. Anim. Resour. 2022, 42, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Bishehkolaei, M.; Pathak, Y. Influence of omega n-6/n-3 ratio on cardiovascular disease and nutritional interventions. Human Nutr. Metab. 2024, 37, 200275. [Google Scholar] [CrossRef]
- Guo, Y.; Ma, B.; Li, X.; Hui, H.; Zhou, Y.; Li, N.; Xie, X. n-3 PUFA can reduce IL-6 and TNF levels in patients with cancer. Br. J. Nutr. 2023, 129, 54–65. [Google Scholar] [CrossRef]
- Berntssen, M.H.G.; Ornsrud, R.; Hamre, K.; Lie, K.K. Polyaromatic hydrocarbons in aquafeeds, source, effects and potential implications for vitamin status of farmed fish species: A review. Aquacult. Nutr. 2015, 21, 257–273. [Google Scholar] [CrossRef]
- Bibus, D.M. Long-chain omega-3 from low-trophic-level fish provides value to farmed seafood. Lipid Technol. 2015, 27, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Shahid, M.; Singh, U.B.; Khan, M.S. Metabolomics-Based Mechanistic Insights into Revealing the Adverse Effects of Pesticides on Plants: An Interactive Review. Metabolites 2023, 13, 246. [Google Scholar] [CrossRef] [PubMed]
- Momtaz, M.; Bubli, S.Y.; Khan, M.S. Mechanisms and Health Aspects of Food Adulteration: A Comprehensive Review. Foods 2023, 12, 199. [Google Scholar] [CrossRef] [PubMed]
- De Flaviis, R.; Sacchetti, G.; Mastrocola, D. Wheat classification according to its origin by an implemented volatile organic compounds analysis. Food Chem. 2021, 341, 128217. [Google Scholar] [CrossRef] [PubMed]
- Heilpern, S.A.; Almeida, R.M.; Fiorella, K.J.; Flecker, A.S.; Williams, D.; Mcintyre, P.B. Nutritional challenges of substituting farmed animals for wild fish in human diets. Environ. Res. Lett. 2023, 18, 114030. [Google Scholar] [CrossRef]
- Astrup, A.; Teicholz, N.; Magkos, F.; Bier, D.M.; Brenna, J.T.; King, J.C.; Mente, A.; Ordovas, J.M.; Volek, J.S.; Yusuf, S.; et al. Dietary Saturated Fats and Health: Are the U.S. Guidelines Evidence-Based? Nutrients 2021, 13, 3305. [Google Scholar] [CrossRef] [PubMed]
- Mercola, J.; D’Adamo, C.R. Linoleic Acid: A Narrative Review of the Effects of Increased Intake in the Standard American Diet and Associations with Chronic Disease. Nutrients 2023, 15, 3129. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients 2016, 8, 128. [Google Scholar] [CrossRef] [PubMed]
- Mathur, K.; Agrawal, R.K.; Nagpure, S.; Deshpande, D. Effect of artificial sweeteners on insulin resistance among type-2 diabetes mellitus patients. J. Family Med. Prim. Care 2020, 9, 69–71. [Google Scholar] [CrossRef]
- Aguayo-Guerrero, J.A.; Mendez-Garcia, L.A.; Solleiro-Villavicencio, H.; Viurcos-Sanabria, R.; Escobedo, G. Sucralose: From Sweet Success to Metabolic Controversies-Unraveling the Global Health Implications of a Pervasive Non-Caloric Artificial Sweetener. Life 2024, 14, 323. [Google Scholar] [CrossRef]
- Walczak-Nowicka, L.J.; Herbet, M. Sodium Benzoate-Harmfulness and Potential Use in Therapies for Disorders Related to the Nervous System: A Review. Nutrients 2022, 14, 1497. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Geng, Y.; Yao, J.; Ji, J.; Chen, F.; Xiao, J.; Hu, X.; Ma, L. N-nitrosamines in processed meats: Exposure, formation and mitigation strategies. J. Agric. Food Res. 2023, 13, 100645. [Google Scholar] [CrossRef]
- Cyr, A.R.; Huckaby, L.V.; Shiva, S.S.; Zuckerbraun, B.S. Nitric Oxide and Endothelial Dysfunction. Crit. Care Clin. 2020, 36, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Wang, S. Protective roles of inorganic nitrate in health and diseases. Curr. Med. 2022, 1, 4. [Google Scholar] [CrossRef]
- Mindang, E.L.N.; Awounfack, C.F.; Ndinteh, D.T.; Krause, R.W.M.; Njamen, D. Effects of Tartrazine on Some Sexual Maturation Parameters in Immature Female Wistar Rats. Int. J. Environ. Res. Public Health 2022, 19, 10410. [Google Scholar] [CrossRef] [PubMed]
- Ameur, F.Z.; Mehedi, N.; Soler Rivas, C.; Gonzalez, A.; Kheroua, O.; Saidi, D. Effect of tartrazine on digestive enzymatic activities: In vivo and in vitro studies. Toxicol. Res. 2020, 36, 159–166. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, J.R.; de Sousa Soares, L.; Soares, B.M.; de Gomes Farias, M.; de Oliveira, V.A.; de Sousa, N.A.B.; Negreiros, H.A.; da Silva, F.C.C.; Peron, A.P.; Pacheco, A.C.L.; et al. Cytotoxic and mutagenic effects of the food additive tartrazine on eukaryotic cells. BMC Pharmacol. Toxicol. 2022, 23, 95. [Google Scholar] [CrossRef]
- De Siena, M.; Raoul, P.; Costantini, L.; Scarpellini, E.; Cintoni, M.; Gasbarrini, A.; Rinninella, E.; Mele, M.C. Food Emulsifiers and Metabolic Syndrome: The Role of the Gut Microbiota. Foods 2022, 11, 2205. [Google Scholar] [CrossRef]
- Scholliers, P. Convenience foods. What, why, and when. Appetite 2015, 94, 2–6. [Google Scholar] [CrossRef]
- Jackson, P.; Viehoff, V. Reframing convenience food. Appetite 2016, 98, 1–11. [Google Scholar] [CrossRef]
- Leeuwendaal, N.K.; Stanton, C.; O’Toole, P.W.; Beresford, T.P. Fermented Foods, Health and the Gut Microbiome. Nutrients 2022, 14, 1527. [Google Scholar] [CrossRef]
- Stiemsma, L.T.; Nakamura, R.E.; Nguyen, J.G.; Michels, K.B. Does Consumption of Fermented Foods Modify the Human Gut Microbiota? J. Nutr. 2020, 150, 1680–1692. [Google Scholar] [CrossRef]
- Valentino, V.; Magliulo, R.; Farsi, D.; Cotter, P.D.; O’Sullivan, O.; Ercolini, D.; De Filippis, F. Fermented foods, their microbiome and its potential in boosting human health. Microb. Biotechnol. 2024, 17, e14428. [Google Scholar] [CrossRef]
- Tachie, C.Y.E.; Onuh, J.O.; Aryee, A.N.A. Nutritional and potential health benefits of fermented food proteins. J. Sci. Food Agri. 2024, 104, 1223–1233. [Google Scholar] [CrossRef]
- Amato, K.R.; Mallott, E.K.; Maia, P.D.; Sardaro, M.L.S. Predigestion as an Evolutionary Impetus for Human Use of Fermented Food. Curr. Anthropol. 2021, 62, S207–S219. [Google Scholar] [CrossRef]
- Clites, B.L.; Hofmann, H.A.; Pierce, J.T. The Promise of an Evolutionary Perspective of Alcohol Consumption. Neurosci. Insights 2023, 18, 26331055231163589. [Google Scholar] [CrossRef]
- Dimidi, E.; Cox, S.R.; Rossi, M.; Whelan, K. Fermented Foods: Definitions and Characteristics, Impact on the Gut Microbiota and Effects on Gastrointestinal Health and Disease. Nutrients 2019, 11, 1806. [Google Scholar] [CrossRef]
- Kojima, A.; Ikehara, S.; Kamiya, K.; Kajita, E.; Sato, Y.; Kouda, K.; Tamaki, J.; Kagamimori, S.; Iki, M. Natto Intake is Inversely Associated with Osteoporotic Fracture Risk in Postmenopausal Japanese Women. J. Nutr. 2020, 150, 599–605. [Google Scholar] [CrossRef]
- Vieira, C.P.; Rosario, A.; Lelis, C.A.; Rekowsky, B.S.S.; Carvalho, A.P.A.; Rosario, D.K.A.; Elias, T.A.; Costa, M.P.; Foguel, D.; Conte-Junior, C.A. Bioactive Compounds from Kefir and Their Potential Benefits on Health: A Systematic Review and Meta-Analysis. Oxid. Med. Cell Longev. 2021, 2021, 9081738. [Google Scholar] [CrossRef]
- Kim, M.E.; Lee, J.S. The Potential of Korean Bioactive Substances and Functional Foods for Immune Enhancement. Int. J. Mol. Sci. 2024, 25, 1334. [Google Scholar] [CrossRef]
- Nugroho, D.; Thinthasit, A.; Surya, E.; Hartati; Oh, J.-S.; Jang, J.-G.; Benchawattananon, R.; Surya, R. Immunoenhancing and antioxidant potentials of kimchi, an ethnic food from Korea, as a probiotic and postbiotic food. J. Ethnic Foods 2024, 11, 12. [Google Scholar] [CrossRef]
- Wishart, D.S.; Oler, E.; Peters, H.; Guo, A.; Girod, S.; Han, S.; Saha, S.; Lui, V.W.; LeVatte, M.; Gautam, V.; et al. MiMeDB: The Human Microbial Metabolome Database. Nucleic Acids Res. 2023, 51, D611–D620. [Google Scholar] [CrossRef]
- Neveu, V.; Nicolas, G.; Amara, A.; Salek, R.M.; Scalbert, A. The human microbial exposome: Expanding the Exposome-Explorer database with gut microbial metabolites. Sci. Rep. 2023, 13, 1946. [Google Scholar] [CrossRef]
- Rahman, S.; O’Connor, A.L.; Becker, S.L.; Patel, R.K.; Martindale, R.G.; Tsikitis, V.L. Gut microbial metabolites and its impact on human health. Ann. Gastroenterol. 2023, 36, 360–368. [Google Scholar] [CrossRef]
- da Silva, R.R.; Dorrestein, P.C.; Quinn, R.A. Illuminating the dark matter in metabolomics. Proc. Natl. Acad. Sci. USA 2015, 112, 12549–12550. [Google Scholar] [CrossRef]
- Van Treuren, W.; Dodd, D. Microbial Contribution to the Human Metabolome: Implications for Health and Disease. Annu. Rev. Pathol. 2020, 15, 345–369. [Google Scholar] [CrossRef]
- Moeller, A.H.; Li, Y.; Mpoudi Ngole, E.; Ahuka-Mundeke, S.; Lonsdorf, E.V.; Pusey, A.E.; Peeters, M.; Hahn, B.H.; Ochman, H. Rapid changes in the gut microbiome during human evolution. Proc. Natl. Acad. Sci. USA 2014, 111, 16431–16435. [Google Scholar] [CrossRef]
- Carter, M.M.; Olm, M.R.; Merrill, B.D.; Dahan, D.; Tripathi, S.; Spencer, S.P.; Yu, F.B.; Jain, S.; Neff, N.; Jha, A.R.; et al. Ultra-deep sequencing of Hadza hunter-gatherers recovers vanishing gut microbes. Cell 2023, 186, 3111–3124.e3. [Google Scholar] [CrossRef]
- Schnorr, S.L.; Candela, M.; Rampelli, S.; Centanni, M.; Consolandi, C.; Basaglia, G.; Turroni, S.; Biagi, E.; Peano, C.; Severgnini, M.; et al. Gut microbiome of the Hadza hunter-gatherers. Nat. Commun. 2014, 5, 3654. [Google Scholar] [CrossRef]
- Morrison, D.J.; Preston, T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes 2016, 7, 189–200. [Google Scholar] [CrossRef]
- Facchin, S.; Bertin, L.; Bonazzi, E.; Lorenzon, G.; De Barba, C.; Barberio, B.; Zingone, F.; Maniero, D.; Scarpa, M.; Ruffolo, C.; et al. Short-Chain Fatty Acids and Human Health: From Metabolic Pathways to Current Therapeutic Implications. Life 2024, 14, 559. [Google Scholar] [CrossRef]
- Zhang, D.; Jian, Y.-P.; Zhang, Y.-N.; Li, Y.; Gu, L.-T.; Sun, H.-H.; Liu, M.-D.; Zhou, H.-L.; Wang, Y.-S.; Xu, Z.-X. Short-chain fatty acids in diseases. Cell Comm. Signal. 2023, 21, 212. [Google Scholar] [CrossRef]
- Pressman, P.; Clemens, R.; Hayes, W.; Reddy, C. Food additive safety. Tox. Res. Appl. 2017, 1, 2397847317723572. [Google Scholar] [CrossRef]
- Zhou, X.; Qiao, K.; Wu, H.; Zhang, Y. The Impact of Food Additives on the Abundance and Composition of Gut Microbiota. Molecules 2023, 28, 631. [Google Scholar] [CrossRef]
- Chassaing, B.; Van de Wiele, T.; De Bodt, J.; Marzorati, M.; Gewirtz, A.T. Dietary emulsifiers directly alter human microbiota composition and gene expression ex vivo potentiating intestinal inflammation. Gut 2017, 66, 1414–1427. [Google Scholar] [CrossRef]
- Abou-Donia, M.B.; El-Masry, E.M.; Abdel-Rahman, A.A.; McLendon, R.E.; Schiffman, S.S. Splenda alters gut microflora and increases intestinal p-glycoprotein and cytochrome p-450 in male rats. J. Toxicol. Environ. Health A 2008, 71, 1415–1429. [Google Scholar] [CrossRef]
- Palmnas, M.S.; Cowan, T.E.; Bomhof, M.R.; Su, J.; Reimer, R.A.; Vogel, H.J.; Hittel, D.S.; Shearer, J. Low-dose aspartame consumption differentially affects gut microbiota-host metabolic interactions in the diet-induced obese rat. PLoS ONE 2014, 9, e109841. [Google Scholar] [CrossRef]
- Zhao, J.; Liang, R.; Song, Q.; Song, S.; Yue, J.; Wu, C. Investigating association between gut microbiota and sarcopenia-related traits: A Mendelian randomization study. Precis. Clin. Med. 2023, 6, pbad010. [Google Scholar] [CrossRef]
- Gomez-Arango, L.F.; Barrett, H.L.; Wilkinson, S.A.; Callaway, L.K.; McIntyre, H.D.; Morrison, M.; Dekker Nitert, M. Low dietary fiber intake increases Collinsella abundance in the gut microbiota of overweight and obese pregnant women. Gut Microbes 2018, 9, 189–201. [Google Scholar] [CrossRef]
- Ilich, J.Z.; Kelly, O.J.; Inglis, J.E.; Panton, L.B.; Duque, G.; Ormsbee, M.J. Interrelationship among muscle, fat, and bone: Connecting the dots on cellular, hormonal, and whole body levels. Ageing Res. Rev. 2014, 15, 51–60. [Google Scholar] [CrossRef]
- Tu, Y.; Yang, R.; Xu, X.; Zhou, X. The microbiota-gut-bone axis and bone health. J. Leukoc. Biol. 2021, 110, 525–537. [Google Scholar] [CrossRef]
- de Sire, A.; de Sire, R.; Curci, C.; Castiglione, F.; Wahli, W. Role of Dietary Supplements and Probiotics in Modulating Microbiota and Bone Health: The Gut-Bone Axis. Cells 2022, 11, 743. [Google Scholar] [CrossRef]
- He, Y.; Chen, Y. The potential mechanism of the microbiota-gut-bone axis in osteoporosis: A review. Osteoporos. Int. 2022, 33, 2495–2506. [Google Scholar] [CrossRef]
- Zhao, J.; Huang, Y.; Yu, X. A Narrative Review of Gut-Muscle Axis and Sarcopenia: The Potential Role of Gut Microbiota. Int. J. Gen. Med. 2021, 14, 1263–1273. [Google Scholar] [CrossRef]
- Prokopidis, K.; Chambers, E.; Ni Lochlainn, M.; Witard, O.C. Mechanisms Linking the Gut-Muscle Axis with Muscle Protein Metabolism and Anabolic Resistance: Implications for Older Adults at Risk of Sarcopenia. Front. Physiol. 2021, 12, 770455. [Google Scholar] [CrossRef]
- Liao, X.; Wu, M.; Hao, Y.; Deng, H. Exploring the Preventive Effect and Mechanism of Senile Sarcopenia Based on “Gut-Muscle Axis”. Front. Bioeng. Biotechnol. 2020, 8, 590869. [Google Scholar] [CrossRef]
- Xiao, H.; Kang, S. The Role of the Gut Microbiome in Energy Balance with a Focus on the Gut-Adipose Tissue Axis. Front. Genet. 2020, 11, 297. [Google Scholar] [CrossRef]
- Lundgren, P.; Thaiss, C.A. The microbiome-adipose tissue axis in systemic metabolism. Am. J. Physiol. Gastrointest. Liver Physiol. 2020, 318, G717–G724. [Google Scholar] [CrossRef]
- Wachsmuth, H.R.; Weninger, S.N.; Duca, F.A. Role of the gut-brain axis in energy and glucose metabolism. Exp. Mol. Med. 2022, 54, 377–392. [Google Scholar] [CrossRef]
- Zihlman, A.L.; Bolter, D.R. Body composition in Pan paniscus compared with Homo sapiens has implications for changes during human evolution. Proc. Natl. Acad. Sci. USA 2015, 112, 7466–7471. [Google Scholar] [CrossRef]
- Mauldin, K.; May, M.; Clifford, D. The consequences of a weight-centric approach to healthcare: A case for a paradigm shift in how clinicians address body weight. Nutr. Clin. Pract. 2022, 37, 1291–1306. [Google Scholar] [CrossRef]
- Tanne, J.H. Obesity: Avoid using BMI alone when evaluating patients, say US doctors’ leaders. BMJ 2023, 381, 1400. [Google Scholar] [CrossRef]
- Bluher, M. Metabolically Healthy Obesity. Endocr. Rev. 2020, 41, bnaa004. [Google Scholar] [CrossRef]
- Tanriover, C.; Copur, S.; Gaipov, A.; Ozlusen, B.; Akcan, R.E.; Kuwabara, M.; Hornum, M.; Van Raalte, D.H.; Kanbay, M. Metabolically healthy obesity: Misleading phrase or healthy phenotype? Eur. J. Intern. Med. 2023, 111, 5–20. [Google Scholar] [CrossRef]
- Wang, J.S.; Xia, P.F.; Ma, M.N.; Li, Y.; Geng, T.T.; Zhang, Y.B.; Tu, Z.Z.; Jiang, L.; Zhou, L.R.; Zhang, B.F.; et al. Trends in the Prevalence of Metabolically Healthy Obesity Among US Adults, 1999–2018. JAMA Netw. Open. 2023, 6, e232145. [Google Scholar] [CrossRef]
- Wijayatunga, N.N.; Dhurandhar, E.J. Normal weight obesity and unaddressed cardiometabolic health risk-a narrative review. Int. J. Obes. 2021, 45, 2141–2155. [Google Scholar] [CrossRef]
- Hu, K.; Deya Edelen, E.; Zhuo, W.; Khan, A.; Orbegoso, J.; Greenfield, L.; Rahi, B.; Griffin, M.; Ilich, J.Z.; Kelly, O.J. Understanding the Consequences of Fatty Bone and Fatty Muscle: How the Osteosarcopenic Adiposity Phenotype Uncovers the Deterioration of Body Composition. Metabolites 2023, 13, 1056. [Google Scholar] [CrossRef]
- Li, W.; Li, X.; Huang, T.; Chen, Y.; Zhang, H.; Dai, H.; Wen, Y. Normative reference data for body composition in healthy indigenous populations on the Qinghai-Tibet Plateau. Front. Public Health 2022, 10, 986720. [Google Scholar] [CrossRef]
- Wang, D.; Li, Y.; Lee, S.G.; Wang, L.; Fan, J.; Zhang, G.; Wu, J.; Ji, Y.; Li, S. Ethnic differences in body composition and obesity related risk factors: Study in Chinese and white males living in China. PLoS ONE 2011, 6, e19835. [Google Scholar] [CrossRef]
- Rush, E.C.; Freitas, I.; Plank, L.D. Body size, body composition and fat distribution: Comparative analysis of European, Maori, Pacific Island and Asian Indian adults. Br. J. Nutr. 2009, 102, 632–641. [Google Scholar] [CrossRef]
- Ghosh, S. A comparative analysis of dietary intake and body composition among two ethnically distinct tribal populations from India. Eur. J. Clin. Nutr. 2022, 76, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Pomeroy, E.; Mushrif-Tripathy, V.; Cole, T.J.; Wells, J.C.K.; Stock, J.T. Ancient origins of low lean mass among South Asians and implications for modern type 2 diabetes susceptibility. Sci. Rep. 2019, 9, 10515. [Google Scholar] [CrossRef] [PubMed]
- Eaton, S.B.; Cordain, L.; Sparling, P.B. Evolution, body composition, insulin receptor competition, and insulin resistance. Prev. Med. 2009, 49, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R.; Chevalley, T. Bone health: Biology and nutrition. Curr. Opin. Clin. Nutr. Metab. Care 2024, 27, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Dismore, L.; Hurst, C.; Robinson, S.M.; Sayer, A.A. Myoprotective Whole Foods, Muscle Health and Sarcopenia: A Systematic Review of Observational and Intervention Studies in Older Adults. Nutrients 2020, 12, 2257. [Google Scholar] [CrossRef] [PubMed]
- Isanejad, M.; Steffen, L.M.; Terry, J.G.; Shikany, J.M.; Zhou, X.; So, Y.; Jacobs, D.R., Jr.; Carr, J.J.; Steffen, B.T. Diet quality is associated with adipose tissue and muscle mass: The Coronary Artery Risk Development in Young Adults (CARDIA) study. J. Cachexia Sarcopenia Muscle 2024, 15, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Nowlan, N.C.; Jepsen, K.J.; Morgan, E.F. Smaller, weaker, and less stiff bones evolve from changes in subsistence strategy. Osteoporos. Int. 2011, 22, 1967–1980. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.M.; Shaw, C.N. Gracility of the modern Homo sapiens skeleton is the result of decreased biomechanical loading. Proc. Natl. Acad. Sci. USA 2015, 112, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Kralick, A.E.; Zemel, B.S. Evolutionary Perspectives on the Developing Skeleton and Implications for Lifelong Health. Front. Endocrinol. 2020, 11, 99. [Google Scholar] [CrossRef]
- Srivastava, R.K.; Sapra, L.; Mishra, P.K. Osteometabolism: Metabolic Alterations in Bone Pathologies. Cells 2022, 11, 3943. [Google Scholar] [CrossRef]
- Zhao, Z.; Cai, Z.; Chen, A.; Cai, M.; Yang, K. Application of metabolomics in osteoporosis research. Front. Endocrinol. 2022, 13, 993253. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Xu, H.; Li, G.H.; Long, M.T.; Cheung, C.L.; Vasan, R.S.; Hsu, Y.H.; Kiel, D.P.; Liu, C.T. Metabolomics Insights into Osteoporosis through Association with Bone Mineral Density. J. Bone Miner. Res. 2021, 36, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Moayyeri, A.; Cheung, C.L.; Tan, K.C.; Morris, J.A.; Cerani, A.; Mohney, R.P.; Richards, J.B.; Hammond, C.; Spector, T.D.; Menni, C. Metabolomic Pathways to Osteoporosis in Middle-Aged Women: A Genome-Metabolome-Wide Mendelian Randomization Study. J. Bone Miner. Res. 2018, 33, 643–650. [Google Scholar] [CrossRef] [PubMed]
- You, Y.S.; Lin, C.Y.; Liang, H.J.; Lee, S.H.; Tsai, K.S.; Chiou, J.M.; Chen, Y.C.; Tsao, C.K.; Chen, J.H. Association between the metabolome and low bone mineral density in Taiwanese women determined by (1)H NMR spectroscopy. J. Bone Miner. Res. 2014, 29, 212–222. [Google Scholar] [CrossRef]
- Deng, D.; Pan, C.; Wu, Z.; Sun, Y.; Liu, C.; Xiang, H.; Yin, P.; Shang, D. An Integrated Metabolomic Study of Osteoporosis: Discovery and Quantification of Hyocholic Acids as Candidate Markers. Front. Pharmacol. 2021, 12, 725341. [Google Scholar] [CrossRef] [PubMed]
- Haseltine, K.N.; Chukir, T.; Smith, P.J.; Jacob, J.T.; Bilezikian, J.P.; Farooki, A. Bone Mineral Density: Clinical Relevance and Quantitative Assessment. J. Nucl. Med. 2021, 62, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.S.; Sinha, P.; Rosen, H. To repeat or not to repeat? Measuring bone mineral density during anti-resorptive therapy or a drug holiday. Cleve Clin. J. Med. 2023, 90, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Ballock, R.T.; O’Keefe, R.J. The Biology of the Growth Plate. JBJS 2003, 85, 715–726. [Google Scholar] [CrossRef]
- Olsen, B.R.; Reginato, A.M.; Wang, W. Bone development. Annu. Rev. Cell Dev. Biol. 2000, 16, 191–220. [Google Scholar] [CrossRef] [PubMed]
- Ortega, N.; Behonick, D.J.; Werb, Z. Matrix remodeling during endochondral ossification. Trends Cell Biol. 2004, 14, 86–93. [Google Scholar] [CrossRef]
- Samsa, W.E.; Zhou, X.; Zhou, G. Signaling pathways regulating cartilage growth plate formation and activity. Semin. Cell Dev. Biol. 2017, 62, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Zaretsky, J.; Griess-Fishheimer, S.; Carmi, A.; Travinsky Shmul, T.; Ofer, L.; Sinai, T.; Penn, S.; Shahar, R.; Monsonego-Ornan, E. Ultra-processed food targets bone quality via endochondral ossification. Bone Res. 2021, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Martinez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef]
- Houshialsadat, Z.; Cediel, G.; Sattamini, I.; Scrinis, G.; Machado, P. Ultra-processed foods, dietary diversity and micronutrient intakes in the Australian population. Eur. J. Nutr. 2024, 63, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Hattori, T.; Muller, C.; Gebhard, S.; Bauer, E.; Pausch, F.; Schlund, B.; Bosl, M.R.; Hess, A.; Surmann-Schmitt, C.; von der Mark, H.; et al. SOX9 is a major negative regulator of cartilage vascularization, bone marrow formation and endochondral ossification. Development 2010, 137, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Reeves, P.G.; Nielsen, F.H.; Fahey, G.C., Jr. AIN-93 purified diets for laboratory rodents: Final report of the American Institute of Nutrition ad hoc writing committee on the reformulation of the AIN-76A rodent diet. J. Nutr. 1993, 123, 1939–1951. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.; Ard, J.; Bazzano, L.; Heymsfield, S.; Mayer-Davis, E.; Sabate, J.; Snetselaar, L.; Van Horn, L.; Schneeman, B.; English, L.K.; et al. Dietary Patterns and Bone Health: A Systematic Review; USDA Nutrition Evidence Systematic Reviews: Alexandria, Egypt, 2020. [Google Scholar]
- Movassagh, E.Z.; Vatanparast, H. Current Evidence on the Association of Dietary Patterns and Bone Health: A Scoping Review. Adv. Nutr. 2017, 8, 1–16. [Google Scholar] [CrossRef]
- Rizzoli, R.; Biver, E.; Brennan-Speranza, T.C. Nutritional intake and bone health. Lancet Diabetes Endocrinol. 2021, 9, 606–621. [Google Scholar] [CrossRef]
- Tayyem, R.; Abuhijleh, H.; Al-Khammash, A. Lifestyle and Dietary Patterns as Risk Factors for Osteoporosis: A Literature Review. Curr. Nutr. Food Sci. 2023, 19, 806–816. [Google Scholar] [CrossRef]
- Key, T.J.; Papier, K.; Tong, T.Y.N. Plant-based diets and long-term health: Findings from the EPIC-Oxford study. Proc. Nutr. Soc. 2022, 81, 190–198. [Google Scholar] [CrossRef]
- Falchetti, A.; Cavati, G.; Valenti, R.; Mingiano, C.; Cosso, R.; Gennari, L.; Chiodini, I.; Merlotti, D. The effects of vegetarian diets on bone health: A literature review. Front. Endocrinol. 2022, 13, 899375. [Google Scholar] [CrossRef] [PubMed]
- Menzel, J.; Abraham, K.; Stangl, G.I.; Ueland, P.M.; Obeid, R.; Schulze, M.B.; Herter-Aeberli, I.; Schwerdtle, T.; Weikert, C. Vegan Diet and Bone Health-Results from the Cross-Sectional RBVD Study. Nutrients 2021, 13, 685. [Google Scholar] [CrossRef] [PubMed]
- Hsu, E. Plant-based diets and bone health: Sorting through the evidence. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Kraselnik, A. Risk of Bone Fracture on Vegetarian and Vegan Diets. Curr. Nutr. Rep. 2024, 13, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Lang, T.; Streeper, T.; Cawthon, P.; Baldwin, K.; Taaffe, D.R.; Harris, T.B. Sarcopenia: Etiology, clinical consequences, intervention, and assessment. Osteoporos. Int. 2010, 21, 543–559. [Google Scholar] [CrossRef]
- Behera, J.; Bala, J.; Nuru, M.; Tyagi, S.C.; Tyagi, N. Homocysteine as a Pathological Biomarker for Bone Disease. J. Cell. Physiol. 2017, 232, 2704–2709. [Google Scholar] [CrossRef] [PubMed]
- Thaler, R.; Agsten, M.; Spitzer, S.; Paschalis, E.P.; Karlic, H.; Klaushofer, K.; Varga, F. Homocysteine suppresses the expression of the collagen cross-linker lysyl oxidase involving IL-6, Fli1, and epigenetic DNA methylation. J. Biol. Chem. 2011, 286, 5578–5588. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.L.; Shih, C.C.; Huang, T.C.; Chen, J.Y. The Relationship between Elevated Homocysteine and Metabolic Syndrome in a Community-Dwelling Middle-Aged and Elderly Population in Taiwan. Biomedicines 2023, 11, 378. [Google Scholar] [CrossRef]
- Crider, K.S.; Yang, T.P.; Berry, R.J.; Bailey, L.B. Folate and DNA methylation: A review of molecular mechanisms and the evidence for folate’s role. Adv. Nutr. 2012, 3, 21–38. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Rodriguez-Artalejo, F.; Fung, T.T.; Meyer, H.E.; Hu, F.B.; Willett, W.C.; Bhupathiraju, S.N. Plant-Based Diets and Risk of Hip Fracture in Postmenopausal Women. JAMA Netw. Open. 2024, 7, e241107. [Google Scholar] [CrossRef]
- Weikert, C.; Trefflich, I.; Menzel, J.; Obeid, R.; Longree, A.; Dierkes, J.; Meyer, K.; Herter-Aeberli, I.; Mai, K.; Stangl, G.I.; et al. Vitamin and Mineral Status in a Vegan Diet. Dtsch. Arztebl. Int. 2020, 117, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Sacco, S.M.; Horcajada, M.N.; Offord, E. Phytonutrients for bone health during ageing. Br. J. Clin. Pharmacol. 2013, 75, 697–707. [Google Scholar] [CrossRef]
- Quek, Y.Y.; Cheng, L.J.; Ng, Y.X.; Hey, H.W.D.; Wu, X.V. Effectiveness of anthocyanin-rich foods on bone remodeling biomarkers of middle-aged and older adults at risk of osteoporosis: A systematic review, meta-analysis, and meta-regression. Nutr. Rev. 2023. [Google Scholar] [CrossRef] [PubMed]
- Alam, W.; Khan, H.; Ahmad, I. Acid-base and electrolyte balance regulations with phytonutrients. In The Role of Phytonutrients in Metabolic Disorders; Khan, H., Akkol, E.K., Daglia, M., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 291–311. [Google Scholar]
- Freese, J.; Klement, R.J.; Ruiz-Nunez, B.; Schwarz, S.; Lotzerich, H. The sedentary (r)evolution: Have we lost our metabolic flexibility? F1000Res 2017, 6, 1787. [Google Scholar] [CrossRef]
- Little, M.A. Evolutionary Strategies for Body Size. Front. Endocrinol. 2020, 11, 107. [Google Scholar] [CrossRef]
- Dembitzer, J.; Barkai, R.; Ben-Dor, M.; Meiri, S. Levantine overkill: 1.5 million years of hunting down the body size distribution. Quat. Sci. Rev. 2022, 276, 107316. [Google Scholar] [CrossRef]
- Karakelides, H.; Nair, K.S. Sarcopenia of aging and its metabolic impact. Curr. Top. Dev. Biol. 2005, 68, 123–148. [Google Scholar] [CrossRef]
- Yang, Q.; Chan, P. Skeletal Muscle Metabolic Alternation Develops Sarcopenia. Aging Dis. 2022, 13, 801–814. [Google Scholar] [CrossRef]
- Marques, J.; Shokry, E.; Uhl, O.; Baber, L.; Hofmeister, F.; Jarmusch, S.; Bidlingmaier, M.; Ferrari, U.; Koletzko, B.; Drey, M. Sarcopenia: Investigation of metabolic changes and its associated mechanisms. Skelet Muscle 2023, 13, 2. [Google Scholar] [CrossRef]
- Opazo, R.; Angel, B.; Marquez, C.; Lera, L.; Cardoso Dos Santos, G.R.; Monnerat, G.; Albala, C. Sarcopenic metabolomic profile reflected a sarcopenic phenotype associated with amino acid and essential fatty acid changes. Metabolomics 2021, 17, 83. [Google Scholar] [CrossRef]
- Shin, H.E.; Won, C.W.; Kim, M. Metabolomic profiles to explore biomarkers of severe sarcopenia in older men: A pilot study. Exp. Gerontol. 2022, 167, 111924. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, K.; Hirayama, A.; Sato, Y.; Ikeda, S.; Maruyama, M.; Soga, T.; Tomita, M.; Nakamura, M.; Matsumoto, M.; Yoshimura, N.; et al. A Metabolomic Profile Predictive of New Osteoporosis or Sarcopenia Development. Metabolites 2021, 11, 278. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Shen, H.; Liu, J.; Chiu, C.Y.; Su, K.J.; Tian, Q.; Kakhniashvili, D.; Qiu, C.; Zhao, L.J.; Luo, Z.; et al. Pathway-based metabolomics study of sarcopenia-related traits in two US cohorts. Aging 2022, 14, 2101–2112. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Shen, H.; Su, K.J.; Tian, Q.; Zhao, L.J.; Qiu, C.; Garrett, T.J.; Liu, J.; Kakhniashvili, D.; Deng, H.W. A joint analysis of metabolomic profiles associated with muscle mass and strength in Caucasian women. Aging 2018, 10, 2624–2635. [Google Scholar] [CrossRef]
- Bagheri, A.; Hashemi, R.; Heshmat, R.; Motlagh, A.D.; Esmaillzadeh, A. Patterns of Nutrient Intake in Relation to Sarcopenia and Its Components. Front. Nutr. 2021, 8, 645072. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Granic, A.; Cruz-Jentoft, A.J.; Sayer, A.A. The role of nutrition in the prevention of sarcopenia. Am. J. Clin. Nutr. 2023, 118, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Domic, J.; Grootswagers, P.; van Loon, L.J.C.; de Groot, L. Perspective: Vegan Diets for Older Adults? A Perspective on the Potential Impact on Muscle Mass and Strength. Adv. Nutr. 2022, 13, 712–725. [Google Scholar] [CrossRef] [PubMed]
- Qu, Z.; Zhou, S.; Li, P.; Liu, C.; Yuan, B.; Zhang, S.; Liu, A. Natural products and skeletal muscle health. J. Nutr. Biochem. 2021, 93, 108619. [Google Scholar] [CrossRef] [PubMed]
- Bluher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Salam, M.; Yousuf, R.; Salam, M.; Haque, M. Obesity and Overweight: A Global Public Health Issue. Adv. Hum. Biol. 2023, 13, 154–156. [Google Scholar]
- Dicken, S.J.; Batterham, R.L. Ultra-processed Food and Obesity: What Is the Evidence? Curr. Nutr. Rep. 2024, 13, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Allaire, B.T.; Tjaden, A.H.; Venditti, E.M.; Apolzan, J.W.; Dabelea, D.; Delahanty, L.M.; Edelstein, S.L.; Hoskin, M.A.; Temple, K.A.; Wylie-Rosett, J.; et al. Diet quality, weight loss, and diabetes incidence in the Diabetes Prevention Program (DPP). BMC Nutr. 2020, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Pascual, R.W.; Phelan, S.; La Frano, M.R.; Pilolla, K.D.; Griffiths, Z.; Foster, G.D. Diet Quality and Micronutrient Intake among Long-Term Weight Loss Maintainers. Nutrients 2019, 11, 3046. [Google Scholar] [CrossRef] [PubMed]
- Harb, A.A.; Shechter, A.; Koch, P.A.; St-Onge, M.P. Ultra-processed foods and the development of obesity in adults. Eur. J. Clin. Nutr. 2023, 77, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Pontzer, H.; Raichlen, D.A.; Wood, B.M.; Mabulla, A.Z.; Racette, S.B.; Marlowe, F.W. Hunter-gatherer energetics and human obesity. PLoS ONE 2012, 7, e40503. [Google Scholar] [CrossRef] [PubMed]
- Azzolino, D.; Spolidoro, G.C.I.; Saporiti, E.; Luchetti, C.; Agostoni, C.; Cesari, M. Musculoskeletal Changes across the Lifespan: Nutrition and the Life-Course Approach to Prevention. Front. Med. 2021, 8, 697954. [Google Scholar] [CrossRef] [PubMed]
- Boutari, C.; Mantzoros, C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef] [PubMed]
- Lemos, T.; Gallagher, D. Current body composition measurement techniques. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 310–314. [Google Scholar] [CrossRef]
- Fruh, S.M. Obesity: Risk factors, complications, and strategies for sustainable long-term weight management. J. Am. Assoc. Nurse Pract. 2017, 29, S3–S14. [Google Scholar] [CrossRef]
- Pontzer, H.; Wood, B.M.; Raichlen, D.A. Hunter-gatherers as models in public health. Obes. Rev. 2018, 19 (Suppl. S1), 24–35. [Google Scholar] [CrossRef]
- Kramer, K.L.; Campbell, B.C.; Achenbach, A.; Hackman, J.V. Sex differences in adipose development in a hunter-gatherer population. Am. J. Hum. Biol. 2022, 34, e23688. [Google Scholar] [CrossRef]
- Belinchón-deMiguel, P.; Ramos-Campo, D.J.; Clemente-Suárez, V.J. Exploring the Evolutionary Disparities: A Case Study on the Psychophysiological Response to Recreating the Hunter–Gatherer Lifestyle through Physical Activity and Caloric Restriction. Appl. Sci. 2023, 13, 11140. [Google Scholar] [CrossRef]
- Øvretveit, K. The Quantified Caveman: A Yearlong Case Study of the Paleolithic Diet. Nutr. Today 2022, 57, 79–87. [Google Scholar] [CrossRef]
- Siddiqui, S.A.; Azmy Harahap, I.; Suthar, P.; Wu, Y.S.; Ghosh, N.; Castro-Munoz, R. A Comprehensive Review of Phytonutrients as a Dietary Therapy for Obesity. Foods 2023, 12, 3610. [Google Scholar] [CrossRef] [PubMed]
- Urasaki, Y.; Le, T.T. Functional Complementation of Anti-Adipogenic Phytonutrients for Obesity Prevention and Management. Nutrients 2022, 14, 4325. [Google Scholar] [CrossRef]
- Sohn, M.J.; Chae, W.; Ko, J.S.; Cho, J.Y.; Kim, J.E.; Choi, J.Y.; Jang, H.B.; Lee, H.J.; Park, S.I.; Park, K.H.; et al. Metabolomic Signatures for the Effects of Weight Loss Interventions on Severe Obesity in Children and Adolescents. Metabolites 2021, 12, 27. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.E.; Larson, M.G.; Ghorbani, A.; Cheng, S.; Chen, M.H.; Keyes, M.; Rhee, E.P.; Clish, C.B.; Vasan, R.S.; Gerszten, R.E.; et al. Metabolomic Profiles of Body Mass Index in the Framingham Heart Study Reveal Distinct Cardiometabolic Phenotypes. PLoS ONE 2016, 11, e0148361. [Google Scholar] [CrossRef] [PubMed]
- Kwee, L.C.; Ilkayeva, O.; Muehlbauer, M.J.; Bihlmeyer, N.; Wolfe, B.; Purnell, J.Q.; Xavier Pi-Sunyer, F.; Chen, H.; Bahnson, J.; Newgard, C.B.; et al. Metabolites and diabetes remission after weight loss. Nutr. Diabetes 2021, 11, 10. [Google Scholar] [CrossRef]
- Cheng, D.; Zhao, X.; Yang, S.; Cui, H.; Wang, G. Metabolomic Signature Between Metabolically Healthy Overweight/Obese and Metabolically Unhealthy Overweight/Obese: A Systematic Review. Diabetes Metab. Syndr. Obes. 2021, 14, 991–1010. [Google Scholar] [CrossRef]
- Boone, S.; Mook-Kanamori, D.; Rosendaal, F.; den Heijer, M.; Lamb, H.; de Roos, A.; le Cessie, S.; Willems van Dijk, K.; de Mutsert, R. Metabolomics: A search for biomarkers of visceral fat and liver fat content. Metabolomics 2019, 15, 139. [Google Scholar] [CrossRef]
- Attie, A.D.; Scherer, P.E. Adipocyte metabolism and obesity. J. Lipid Res. 2009, 50, S395–S399. [Google Scholar] [CrossRef] [PubMed]
- Richard, A.J.; White, U.; Elks, C.M.; Stephens, J.M. Adipose Tissue: Physiology to Metabolic Dysfunction. Endotext 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK555602/ (accessed on 27 June 2024).
- Mu, M.; Xu, L.F.; Hu, D.; Wu, J.; Bai, M.J. Dietary Patterns and Overweight/Obesity: A Review Article. Iran J. Public Health 2017, 46, 869–876. [Google Scholar] [PubMed]
- Muscogiuri, G.; Verde, L.; Sulu, C.; Katsiki, N.; Hassapidou, M.; Frias-Toral, E.; Cucalon, G.; Pazderska, A.; Yumuk, V.D.; Colao, A.; et al. Mediterranean Diet and Obesity-related Disorders: What is the Evidence? Curr. Obes. Rep. 2022, 11, 287–304. [Google Scholar] [CrossRef] [PubMed]
- Iacobini, C.; Pugliese, G.; Blasetti Fantauzzi, C.; Federici, M.; Menini, S. Metabolically healthy versus metabolically unhealthy obesity. Metabolism 2019, 92, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Bosch-Sierra, N.; Grau-Del Valle, C.; Salom, C.; Zaragoza-Villena, B.; Perea-Galera, L.; Falcon-Tapiador, R.; Rovira-Llopis, S.; Morillas, C.; Monleon, D.; Banuls, C. Effect of a Very Low-Calorie Diet on Oxidative Stress, Inflammatory and Metabolomic Profile in Metabolically Healthy and Unhealthy Obese Subjects. Antioxidants 2024, 13, 302. [Google Scholar] [CrossRef] [PubMed]
- Bardanzellu, F.; Puddu, M.; Peroni, D.G.; Fanos, V. The Human Breast Milk Metabolome in Overweight and Obese Mothers. Front. Immunol. 2020, 11, 1533. [Google Scholar] [CrossRef] [PubMed]
- Juarez-Fernandez, M.; Roman-Saguillo, S.; Porras, D.; Garcia-Mediavilla, M.V.; Linares, P.; Ballesteros-Pomar, M.D.; Urioste-Fondo, A.; Alvarez-Cuenllas, B.; Gonzalez-Gallego, J.; Sanchez-Campos, S.; et al. Long-Term Effects of Bariatric Surgery on Gut Microbiota Composition and Faecal Metabolome Related to Obesity Remission. Nutrients 2021, 13, 2519. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.-J. Fruit intake and osteosarcopenic obesity in Korean postmenopausal women aged 50–64 years. Maturitas 2020, 134, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Kelly, O.J.; Gilman, J.C.; Kim, Y.; Ilich, J.Z. Micronutrient Intake in the Etiology, Prevention and Treatment of Osteosarcopenic Obesity. Curr. Aging Sci. 2016, 9, 260–278. [Google Scholar] [CrossRef]
- Kelly, O.J.; Gilman, J.C.; Kim, Y.; Ilich, J.Z. Macronutrient Intake and Distribution in the Etiology, Prevention and Treatment of Osteosarcopenic Obesity. Curr. Aging Sci. 2017, 10, 83–105. [Google Scholar] [CrossRef]
- Zager, D.; Evans, R. In the Year 2525 (Exordium & Terminus). 2525 (Exordium & Terminus) 1969.
- Institute of Medicine (US) Committee on Use of Dietary Reference Intakes in Nutrition Labeling. A Brief Review of the History and Concepts of the Dietary Reference Intakes. In Dietary Reference Intakes: Guiding Principles for Nutrition Labeling and Fortification; National Academies Press: Cambridge, MA, USA, 2003. [Google Scholar]
- Boyland, E.J.; Nolan, S.; Kelly, B.; Tudur-Smith, C.; Jones, A.; Halford, J.C.; Robinson, E. Advertising as a cue to consume: A systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. Am. J. Clin. Nutr. 2016, 103, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Kubik, M.Y.; Wall, M.; Shen, L.; Nanney, M.S.; Nelson, T.F.; Laska, M.N.; Story, M. State but not district nutrition policies are associated with less junk food in vending machines and school stores in US public schools. J. Am. Diet. Assoc. 2010, 110, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, L.G.; Martinez Steele, E.; Canella, D.S.; Monteiro, C.A. Consumption of ultra-processed foods and associated sociodemographic factors in the USA between 2007 and 2012: Evidence from a nationally representative cross-sectional study. BMJ Open 2018, 8, e020574. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef]
- Academy of Nutrition Sciences. Understanding Ultra Processed Foods and Human Health: A Journey without a Plan? Available online: https://www.academynutritionsciences.org.uk/outputs/blog-post-title-one-5td6z (accessed on 27 June 2024).
- Scientific Advisory Committee on Nutrition. SACN Statement on Processed Foods and Health—Summary Report. Available online: https://www.gov.uk/government/publications/sacn-statement-on-processed-foods-and-health/sacn-statement-on-processed-foods-and-health-summary-report (accessed on 27 June 2024).
- Wirt, A.; Collins, C.E. Diet quality--what is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total * | Exogenous | Endogenous | Food | Plant | Microbial | Toxin or Pollutant | Cosmetic | Drug | Drug Metabolite |
|---|---|---|---|---|---|---|---|---|---|
| 248,097 | 35,830 | 221,039 | 32,366 | 146 | 172 | 157 | 17 | 2379 | 909 |
| Foods | Food Compounds (No.) | FooDB ID | FooDB Name |
|---|---|---|---|
| ULTRA-PROCESSED FOOD DIET (24 h INTAKE) | |||
| Breakfast | |||
| Coffee, brewed | 4433 | FOOD00059 | Coffee |
| Sugar coated flakes of corn | 80 | FOOD00270 | Breakfast cereal |
| Liquid coffee creamer | 11 | Not listed | |
| Almond milk, sweetened | 80 | FOOD00937 | Almond milk |
| Morning snack | |||
| Glazed donut | 3969 | FOOD00799 | Flour |
| Cola drink | 6 | Not listed | |
| Lunch | |||
| Chicken nuggets, 6 pieces | 42,460 | FOOD00329 | Chicken |
| French fries, large | 4470 | FOOD00175 | Potato |
| Diet cola drink | 8 | Not listed | |
| Afternoon snack | |||
| Protein bar 30 g, chocolate flavor | 60 | Not listed | |
| Tap water | N/A | ||
| Dinner | |||
| Pizza, cheese topping, thin crispy crust, frozen, baked | 39 | FOOD00933 | Mozzarella |
| 4194 | FOOD00171 | Tomato | |
| 3969 | FOOD00799 | Flour | |
| Chocolate chip cookies | 3969 | FOOD00799 | Flour |
| Tap water | N/A | ||
| Evening snack | |||
| Pretzels, hard | 3969 | FOOD00799 | Flour |
| TOTAL | 71,717 | ||
| WHOLE FOOD DIET (24 h INTAKE) | |||
| Breakfast (omelet with spinach, shallots and mushrooms) | |||
| Eggs, fried | 98 | FOOD00619 | Egg |
| Spinach, cooked, from fresh, fat added in cooking, NS as to type of fat | 4227 | FOOD00178 | Spinach |
| Shallots | 4013 | FOOD00243 | Shallot |
| Mushrooms, cooked, from fresh, fat added in cooking, NS as to type of fat | 4505 | FOOD00547 | Common mushroom |
| Coffee, brewed | 4433 | FOOD00059 | Coffee |
| Morning snack | |||
| Peanuts, Spanish, raw | 4130 | FOOD00016 | Peanut |
| Tap water | N/A | ||
| Orange | 4333 | FOOD00057 | Sweet orange |
| Lunch (grilled chicken breast with mixed vegetables, mixed fruit for desert) | |||
| Chicken breast, grilled, meat and skin | 42,460 | FOOD00329 | Chicken |
| Pepper, bell or sweet, red | 4391 | FOOD00880 | Red bell pepper |
| Onions, chopped | 4514 | FOOD00006 | Garden onion |
| Onions, scallion, or spring green | 4262 | FOOD00241 | Welsh onion |
| Tomatoes, cherry, fresh | 3977 | FOOD00172 | Cherry tomato |
| Spinach, cooked, from fresh, fat added in cooking, NS as to type of fat | 4227 | FOOD00178 | Spinach |
| Oil, olive | 8 | FOOD00909 | Olive oil |
| Cantaloupe | 4010 | FOOD00984 | Cantaloupe melon |
| Strawberries | 4079 | FOOD00083 | Strawberry |
| Blueberries | 3985 | FOOD00211 | Canada blueberry |
| Blackberries | 4252 | FOOD00906 | Blackberry |
| Tap water | N/A | ||
| Coffee, brewed | 4433 | FOOD00059 | Coffee |
| Afternoon snack | |||
| Tap water | N/A | ||
| Apple, medium | 4318 | FOOD00105 | Apple |
| Walnuts, NFS | 4029 | FOOD00608 | Walnut |
| Dinner | |||
| Beef, top sirloin, choice, separable lean, 1/4″ fat, pan fried | 42,522 | FOOD00495 | Cattle (Beef, Veal) |
| Beans, string, green, raw | 4223 | FOOD00883 | Green bean |
| Asparagus | 4192 | FOOD00021 | Asparagus |
| Squash, butternut | 4013 | FOOD00317 | Butternut squash |
| Oil, olive | 8 | FOOD00909 | Olive oil |
| Tap water | N/A | ||
| Kiwi fruit, raw | 4062 | FOOD00004 | Kiwi |
| Evening snack | |||
| Tap water | N/A | ||
| Figs, raw | 4197 | FOOD00081 | Fig |
| Banana | 4036 | FOOD00208 | Banana |
| TOTAL | 185,937 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assaf, S.; Park, J.; Chowdhry, N.; Ganapuram, M.; Mattathil, S.; Alakeel, R.; Kelly, O.J. Unraveling the Evolutionary Diet Mismatch and Its Contribution to the Deterioration of Body Composition. Metabolites 2024, 14, 379. https://doi.org/10.3390/metabo14070379
Assaf S, Park J, Chowdhry N, Ganapuram M, Mattathil S, Alakeel R, Kelly OJ. Unraveling the Evolutionary Diet Mismatch and Its Contribution to the Deterioration of Body Composition. Metabolites. 2024; 14(7):379. https://doi.org/10.3390/metabo14070379
Chicago/Turabian StyleAssaf, Sandi, Jason Park, Naveed Chowdhry, Meghasree Ganapuram, Shelbin Mattathil, Rami Alakeel, and Owen J. Kelly. 2024. "Unraveling the Evolutionary Diet Mismatch and Its Contribution to the Deterioration of Body Composition" Metabolites 14, no. 7: 379. https://doi.org/10.3390/metabo14070379
APA StyleAssaf, S., Park, J., Chowdhry, N., Ganapuram, M., Mattathil, S., Alakeel, R., & Kelly, O. J. (2024). Unraveling the Evolutionary Diet Mismatch and Its Contribution to the Deterioration of Body Composition. Metabolites, 14(7), 379. https://doi.org/10.3390/metabo14070379