
Intra-Individual Variations in How Insulin Sensitivity Responds to Long-Term Exercise: Predictions by Machine Learning Based on Large-Scale Serum Proteomics

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
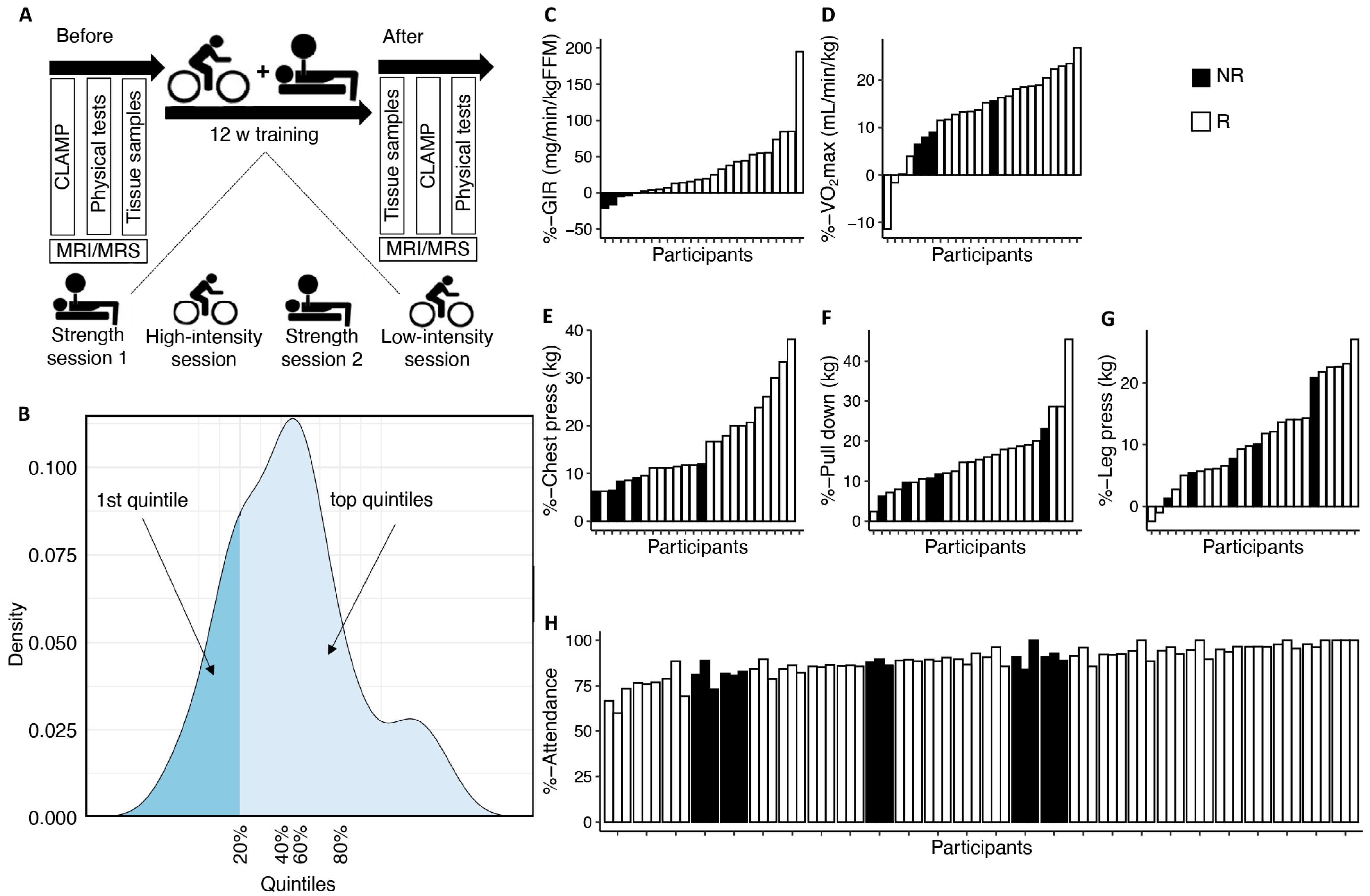
2.1. Insulin Sensitivity and Group Definition
2.2. Cardiovascular Fitness
2.3. Body Composition
2.4. Tissue Samples
2.5. mRNA Sequencing
2.6. Olink Proteomics
2.7. Analytic Approach
3. Results
3.1. Phenotypes of Insulin Sensitivity Non-Responders to Prolonged Exercise
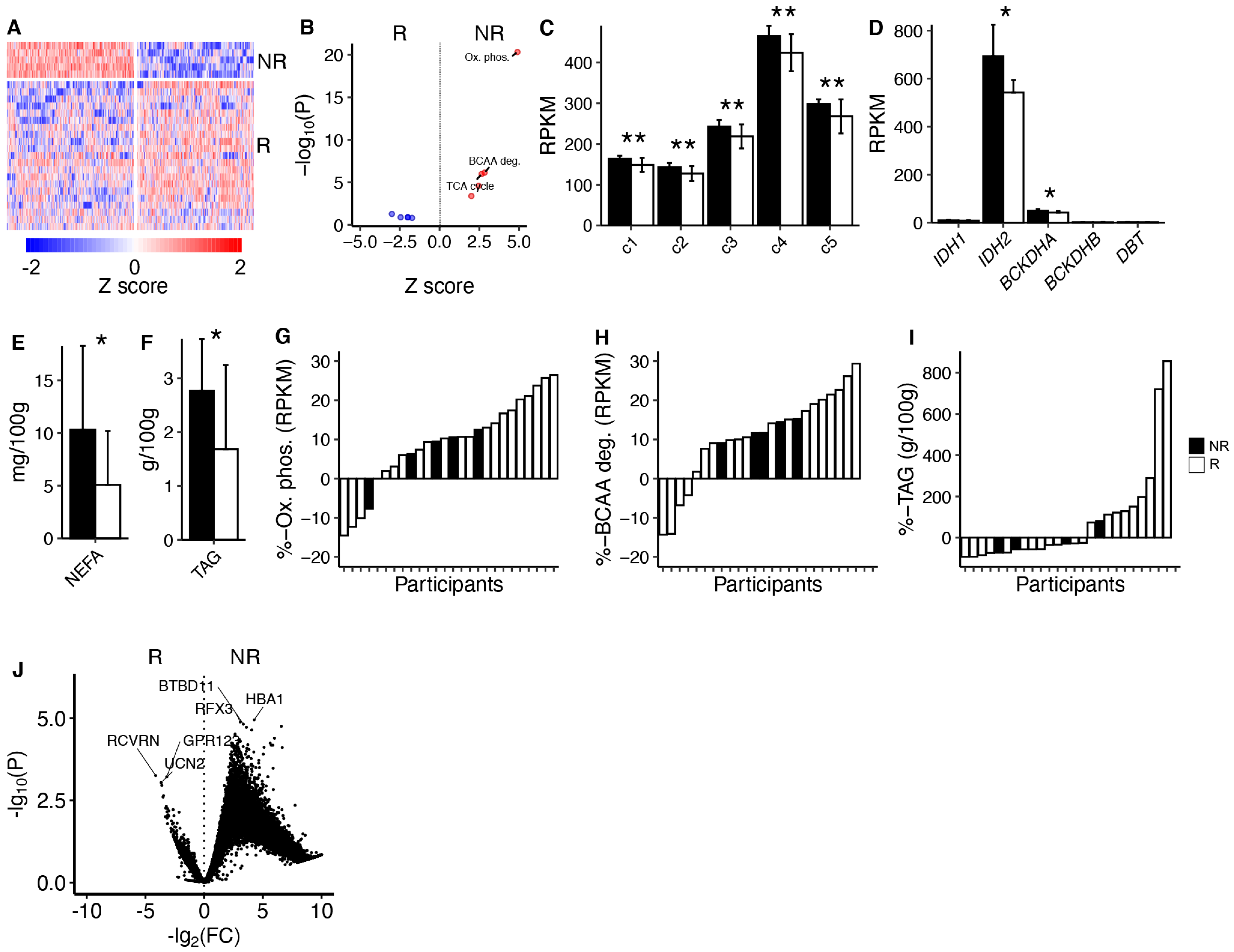
3.2. Skeletal Muscle Characteristics
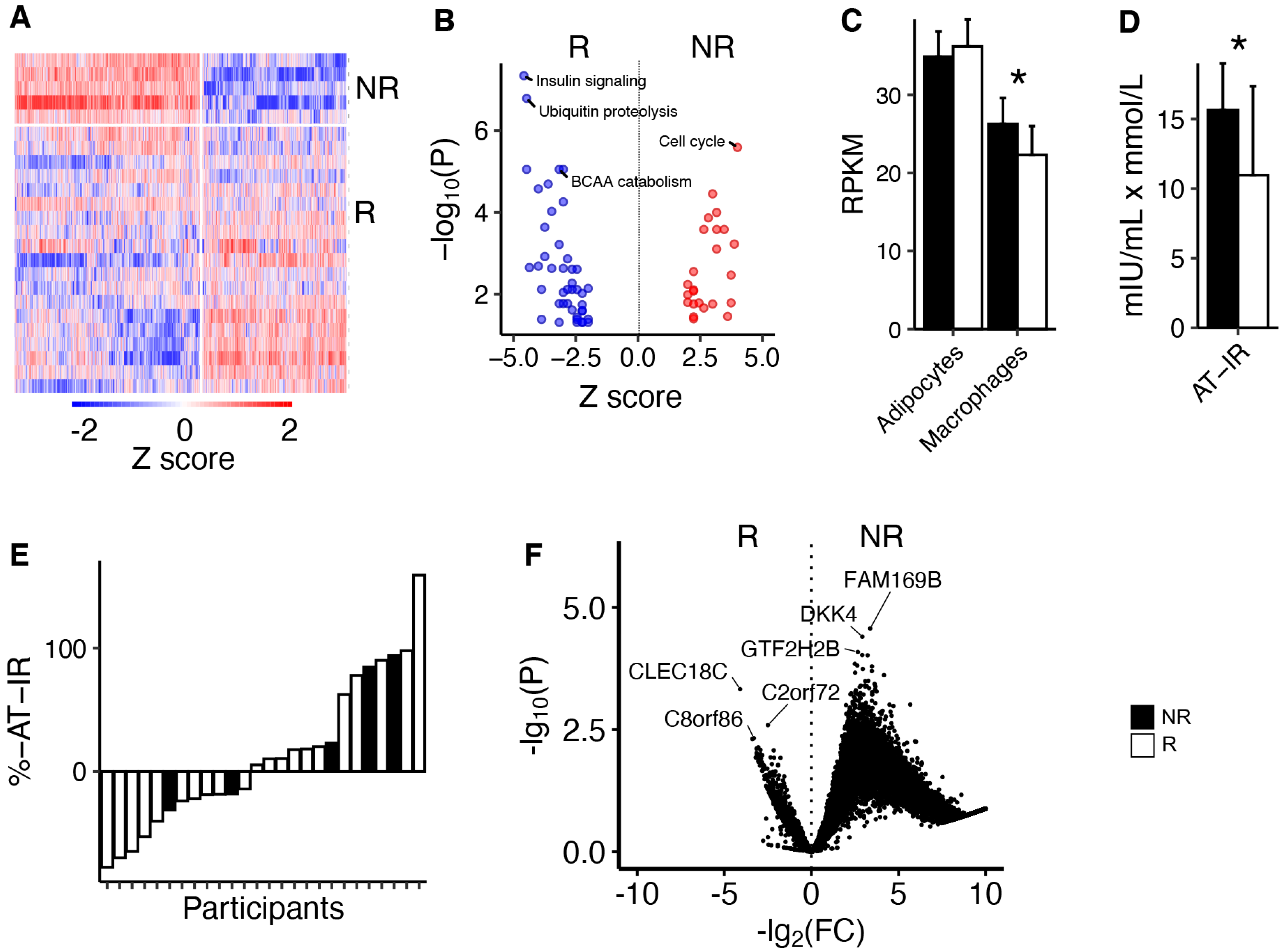
3.3. Adipose Tissue Characteristics
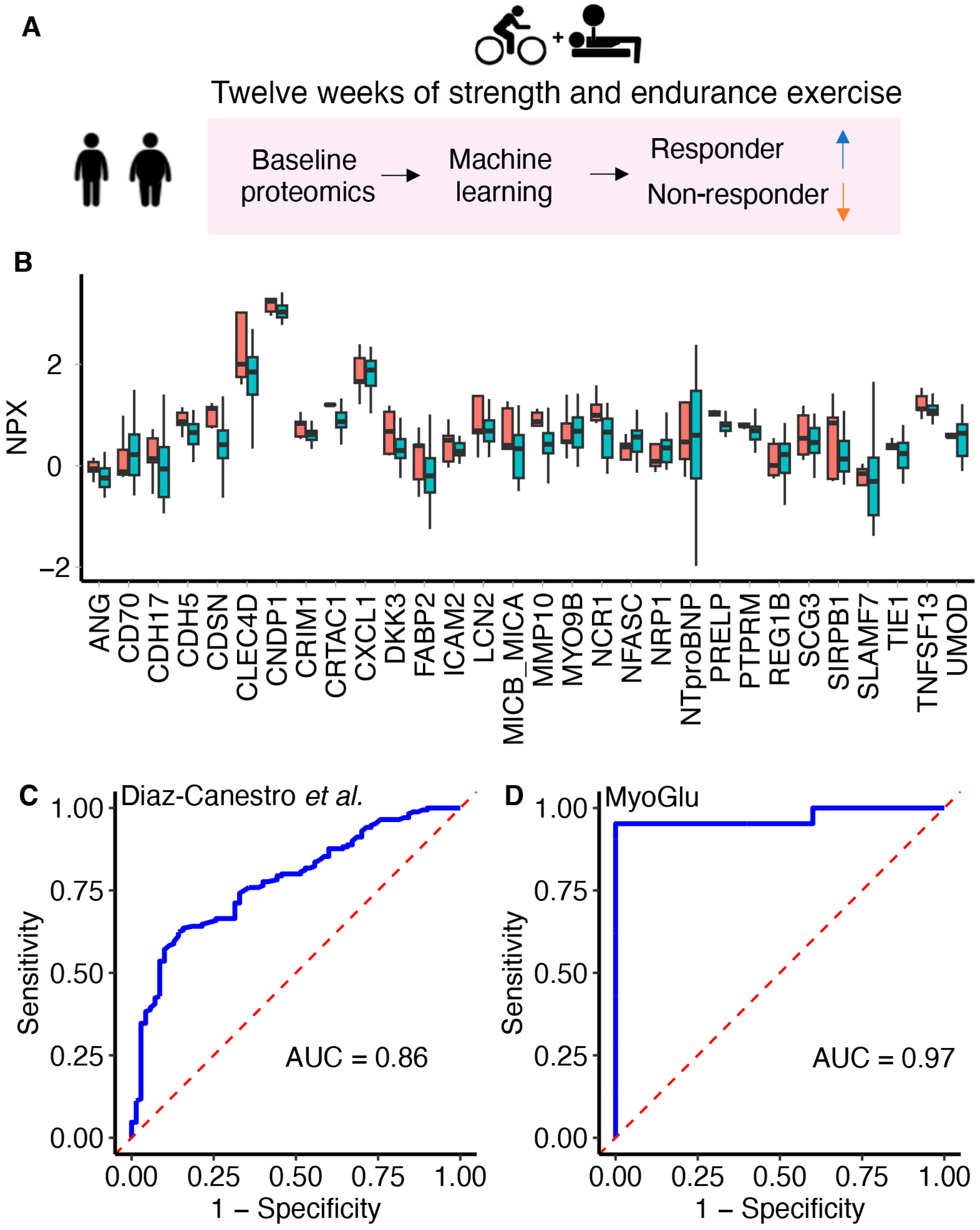
3.4. An ML Algorithm to Predict Variations in Insulin Sensitivity Responses by Serum Proteomics
3.5. Explorative Analyses of Serum Proteins Predicting Exercise Responses
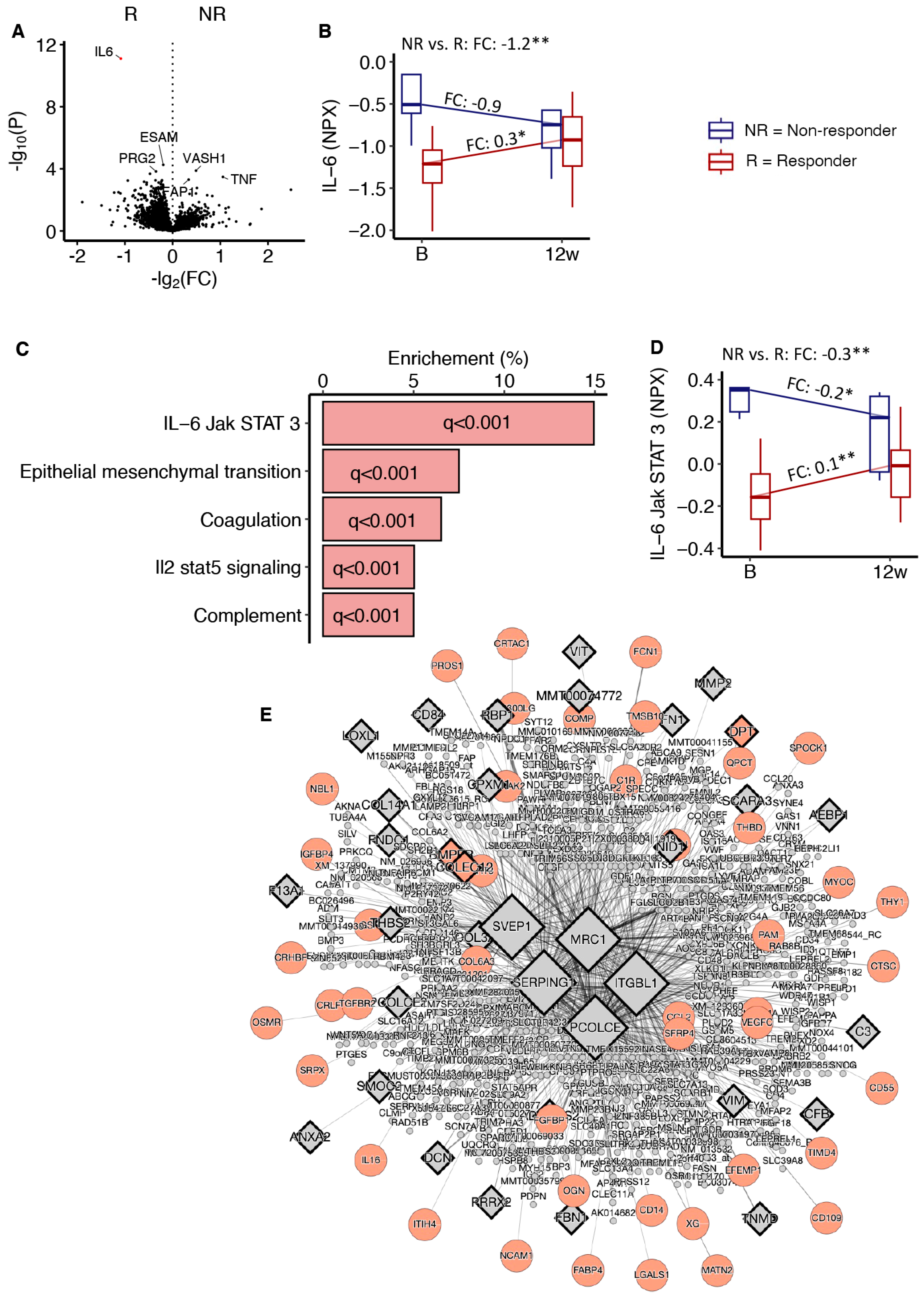
3.6. Serum Proteomics in Response to 12 Weeks of Exercise
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roden, M.; Shulman, G.I. The integrative biology of type 2 diabetes. Nature 2019, 576, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Lee-Ødegård, S.; Olsen, T.; Norheim, F.; Drevon, C.A.; Birkeland, K.I. Potential Mechanisms for How Long-Term Physical Activity May Reduce Insulin Resistance. Metabolites 2022, 12, 208. [Google Scholar] [CrossRef] [PubMed]
- Böhm, A.; Weigert, C.; Staiger, H.; Häring, H.U. Exercise and diabetes: Relevance and causes for response variability. Endocrine 2016, 51, 390–401. [Google Scholar] [CrossRef]
- Solomon, T.P.J. Sources of Inter-individual Variability in the Therapeutic Response of Blood Glucose Control to Exercise in Type 2 Diabetes: Going Beyond Exercise Dose. Front. Physiol. 2018, 9, 896. [Google Scholar] [CrossRef]
- Bouchard, C.; An, P.; Rice, T.; Skinner, J.S.; Wilmore, J.H.; Gagnon, J.; Pérusse, L.; Leon, A.S.; Rao, D.C. Familial aggregation of VO(2max) response to exercise training: Results from the HERITAGE Family Study. J. Appl. Physiol. 1999, 87, 1003–1008. [Google Scholar] [CrossRef]
- Bouchard, C.; Sarzynski, M.A.; Rice, T.K.; Kraus, W.E.; Church, T.S.; Sung, Y.J.; Rao, D.C.; Rankinen, T. Genomic predictors of the maximal O2 uptake response to standardized exercise training programs. J. Appl. Physiol. 2010, 110, 1160–1170. [Google Scholar] [CrossRef] [PubMed]
- Langleite, T.M.; Jensen, J.; Norheim, F.; Gulseth, H.L.; Tangen, D.S.; Kolnes, K.J.; Heck, A.; Storas, T.; Grothe, G.; Dahl, M.A.; et al. Insulin sensitivity, body composition and adipose depots following 12 w combined endurance and strength training in dysglycemic and normoglycemic sedentary men. Arch. Physiol. Biochem. 2016, 122, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Swift, D.L.; McGuire, D.K.; Ayers, C.R.; Neeland, I.J.; Blair, S.N.; Johannsen, N.; Earnest, C.P.; Berry, J.D.; Church, T.S. Metabolic Effects of Exercise Training Among Fitness-Nonresponsive Patients With Type 2 Diabetes: The HART-D Study. Diabetes Care 2015, 38, 1494–1501. [Google Scholar] [CrossRef] [PubMed]
- Kacerovsky-Bielesz, G.; Kacerovsky, M.; Chmelik, M.; Farukuoye, M.; Ling, C.; Pokan, R.; Tschan, H.; Szendroedi, J.; Schmid, A.I.; Gruber, S.; et al. A single nucleotide polymorphism associates with the response of muscle ATP synthesis to long-term exercise training in relatives of type 2 diabetic humans. Diabetes Care 2012, 35, 350–357. [Google Scholar] [CrossRef]
- Stephens, N.A.; Brouwers, B.; Eroshkin, A.M.; Yi, F.; Cornnell, H.H.; Meyer, C.; Goodpaster, B.H.; Pratley, R.E.; Smith, S.R.; Sparks, L.M. Exercise Response Variations in Skeletal Muscle PCr Recovery Rate and Insulin Sensitivity Relate to Muscle Epigenomic Profiles in Individuals With Type 2 Diabetes. Diabetes Care 2018, 41, 2245–2254. [Google Scholar] [CrossRef]
- Stephens, N.A.; Xie, H.; Johannsen, N.M.; Church, T.S.; Smith, S.R.; Sparks, L.M. A transcriptional signature of “exercise resistance” in skeletal muscle of individuals with type 2 diabetes mellitus. Metabolism 2015, 64, 999–1004. [Google Scholar] [CrossRef]
- Kacerovsky-Bielesz, G.; Chmelik, M.; Ling, C.; Pokan, R.; Szendroedi, J.; Farukuoye, M.; Kacerovsky, M.; Schmid, A.I.; Gruber, S.; Wolzt, M.; et al. Short-term exercise training does not stimulate skeletal muscle ATP synthesis in relatives of humans with type 2 diabetes. Diabetes 2009, 58, 1333–1341. [Google Scholar] [CrossRef]
- Böhm, A.; Hoffmann, C.; Irmler, M.; Schneeweiss, P.; Schnauder, G.; Sailer, C.; Schmid, V.; Hudemann, J.; Machann, J.; Schick, F.; et al. TGF-β Contributes to Impaired Exercise Response by Suppression of Mitochondrial Key Regulators in Skeletal Muscle. Diabetes 2016, 65, 2849–2861. [Google Scholar] [CrossRef]
- Lee-Ødegård, S.; Hjorth, M.; Olsen, T.; Moen, G.-H.; Daubney, E.; Evans, D.M.; Hevener, A.; Lusis, A.J.; Zhou, M.; Seldin, M.M.; et al. Serum proteomic profiling of physical activity reveals CD300LG as a novel exerkine with a potential causal link to glucose homeostasis. eLife 2024. [Google Scholar] [CrossRef]
- Diaz-Canestro, C.; Chen, J.; Liu, Y.; Han, H.; Wang, Y.; Honoré, E.; Lee, C.H.; Lam, K.S.L.; Tse, M.A.; Xu, A. A machine-learning algorithm integrating baseline serum proteomic signatures predicts exercise responsiveness in overweight males with prediabetes. Cell Rep. Med. 2023, 4, 100944. [Google Scholar] [CrossRef]
- Chung, W.K.; Erion, K.; Florez, J.C.; Hattersley, A.T.; Hivert, M.F.; Lee, C.G.; McCarthy, M.I.; Nolan, J.J.; Norris, J.M.; Pearson, E.R.; et al. Precision medicine in diabetes: A Consensus Report from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2020, 63, 1671–1693. [Google Scholar] [CrossRef] [PubMed]
- Group, N. AI in Medicine. Available online: https://www.nejm.org/ai-in-medicine (accessed on 3 January 2024).
- Mizani, M.A.; Dashtban, A.; Pasea, L.; Zeng, Q.; Khunti, K.; Valabhji, J.; Mamza, J.B.; Gao, H.; Morris, T.; Banerjee, A. Identifying subtypes of type 2 diabetes mellitus with machine learning: Development, internal validation, prognostic validation and medication burden in linked electronic health records in 420 448 individuals. BMJ Open Diabetes Res. Care 2024, 12, e004191. [Google Scholar] [CrossRef]
- Montesanto, A.; Lagani, V.; Spazzafumo, L.; Tortato, E.; Rosati, S.; Corsonello, A.; Soraci, L.; Sabbatinelli, J.; Cherubini, A.; Conte, M.; et al. Physical performance strongly predicts all-cause mortality risk in a real-world population of older diabetic patients: Machine learning approach for mortality risk stratification. Front. Endocrinol. 2024, 15, 1359482. [Google Scholar] [CrossRef]
- Long, J.; Fang, Q.; Shi, Z.; Miao, Z.; Yan, D. Integrated biomarker profiling for predicting the response of type 2 diabetes to metformin. Diabetes Obes. Metab. 2024. [Google Scholar] [CrossRef]
- Tin Kam, H. The random subspace method for constructing decision forests. IEEE Trans. Pattern Anal. Mach. Intell. 1998, 20, 832–844. [Google Scholar] [CrossRef]
- Lee, S.; Gulseth, H.L.; Langleite, T.M.; Norheim, F.; Olsen, T.; Refsum, H.; Jensen, J.; Birkeland, K.I.; Drevon, C.A. Branched-chain amino acid metabolism, insulin sensitivity and liver fat response to exercise training in sedentary dysglycaemic and normoglycaemic men. Diabetologia 2021, 64, 410–423. [Google Scholar] [CrossRef]
- Lee, S.; Norheim, F.; Langleite, T.M.; Gulseth, H.L.; Birkeland, K.I.; Drevon, C.A. Effects of long-term exercise on plasma adipokine levels and inflammation-related gene expression in subcutaneous adipose tissue in sedentary dysglycaemic, overweight men and sedentary normoglycaemic men of healthy weight. Diabetologia 2019, 62, 1048–1064. [Google Scholar] [CrossRef] [PubMed]
- Broad Institute, I. MSigDB. Available online: https://www.gsea-msigdb.org/gsea/msigdb/ (accessed on 3 January 2024).
- Ding, J.; Blencowe, M.; Nghiem, T.; Ha, S.; Chen, Y.; Li, G.; Yang, X. Mergeomics 2.0: A web server for multi-omics data integration to elucidate disease networks and predict therapeutics. Nucleic Acids Research. 2021, 49, 375–387. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuhn, M. Building Predictive Models in R Using the caret Package. J. Stat. Softw. 2008, 28, 1–26. [Google Scholar] [CrossRef]
- Hassija, V.; Chamola, V.; Mahapatra, A.; Singal, A.; Goel, D.; Huang, K.; Scardapane, S.; Spinelli, I.; Mahmud, M.; Hussain, A. Interpreting Black-Box Models: A Review on Explainable Artificial Intelligence. Cogn. Comput. 2024, 16, 45–74. [Google Scholar] [CrossRef]
- Benjamini, Y. Discovering the false discovery rate. J. R. Stat. Soc. Ser. B (Stat. Methodol.) 2010, 72, 405–416. [Google Scholar] [CrossRef]
- Benjamini, Y.; Yekutieli, D. The Control of the False Discovery Rate in Multiple Testing under Dependency. Ann. Stat. 2001, 29, 1165–1188. [Google Scholar] [CrossRef]
- Sparks, L.M. Exercise training response heterogeneity: Physiological and molecular insights. Diabetologia 2017, 60, 2329–2336. [Google Scholar] [CrossRef]
- Thamer, C.; Machann, J.; Stefan, N.; Haap, M.; Schäfer, S.; Brenner, S.; Kantartzis, K.; Claussen, C.; Schick, F.; Haring, H.; et al. High visceral fat mass and high liver fat are associated with resistance to lifestyle intervention. Obesity 2007, 15, 531–538. [Google Scholar] [CrossRef]
- Montero, D.; Diaz-Cañestro, C.; Lundby, C. Endurance Training and V˙O2max: Role of Maximal Cardiac Output and Oxygen Extraction. Med. Sci. Sports Exerc. 2015, 47, 2024–2033. [Google Scholar] [CrossRef]
- Montero, D.; Cathomen, A.; Jacobs, R.A.; Flück, D.; de Leur, J.; Keiser, S.; Bonne, T.; Kirk, N.; Lundby, A.K.; Lundby, C. Haematological rather than skeletal muscle adaptations contribute to the increase in peak oxygen uptake induced by moderate endurance training. J. Physiol. 2015, 593, 4677–4688. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Sui, X.; Lobelo, F.; Lee, D.C.; Morrow, J.R., Jr.; Jackson, A.W.; Hébert, J.R.; Matthews, C.E.; Sjöström, M.; Blair, S.N. Muscular strength and adiposity as predictors of adulthood cancer mortality in men. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. Association between muscle strength and type 2 diabetes mellitus in adults in Korea: Data from the Korea national health and nutrition examination survey (KNHANES) VI. Medicine 2018, 97, e10984. [Google Scholar] [CrossRef]
- Hjorth, M.; Norheim, F.; Meen, A.J.; Pourteymour, S.; Lee, S.; Holen, T.; Jensen, J.; Birkeland, K.I.; Martinov, V.N.; Langleite, T.M.; et al. The effect of acute and long-term physical activity on extracellular matrix and serglycin in human skeletal muscle. Physiol. Rep. 2015, 3, e12473. [Google Scholar] [CrossRef]
- Echouffo-Tcheugui, J.B.; Zhang, S.; McEvoy, J.W.; Juraschek, S.P.; Fang, M.; Ndumele, C.E.; Christenson, R.H.; Selvin, E. Insulin Resistance and N-Terminal Pro-B-Type Natriuretic Peptide Among Healthy Adults. JAMA Cardiol. 2023, 8, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Moresi, V.; Adamo, S.; Berghella, L. The JAK/STAT Pathway in Skeletal Muscle Pathophysiology. Front. Physiol. 2019, 10, 500. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Lang, X.; Li, X. The role of IL-6/JAK2/STAT3 signaling pathway in cancers. Front. Oncol. 2022, 12, 1023177. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Training | Post-Training (Δ) | |||
|---|---|---|---|---|
| Non-Responders | Responders | Non-Responders | Responders | |
| Sex (m/f) | 5/0 | 21/0 | ||
| Caucasian race | 5 | 21 | ||
| Age (years) | 55.2 (3.9) | 50.2 (6.8) | ||
| Strength attendance (%) | 86.2 (9.8) | 87.9 (8.3) | ||
| Endurance attendance (%) | 87.2 (4.8) | 90.6 (9.4) | ||
| Total attendance (%) | 86.5 (4.8) | 89.3 (8.0) | ||
| HbA1c (mmol/mol) | 38 (2.2) | 34 (4.4) | N.A. | N.A. |
| HbA1c (%) | 5.6 (0.2) | 5.3 (0.4) | N.A. | N.A. |
| GIR (mg/kgFFM/min) | 11.7 (2.5) | 13.9 (5.4) | −1.2 (1.4) A | 4.5 (3.3) * A |
| Fasting plasma glucose (mmol/L) | 5.6 (0.7) | 5.6 (0.5) | 0.2 (0.2) | 0.1 (0.3) |
| Fasting insulin (pmol/mL) | 65.3 (31.6) | 48.7 (25.0) | 25.5 (35.1) | 1.3 (20.0) |
| Fasting C-peptide (pmol/mL) | 906.8 (399.5) | 725.6 (213.5) | 127.4 (315.7) | 15.0 (163.9) |
| VO2max (mL/kg/min) | 38.9 (6.2) | 41.0 (5.8) | 2.9 (2.2) * A | 5.8 (3.5) * A |
| Chest press (kg) | 67.0 (11.1) | 67.1 (16.1) | 5.5 (1.1) * A | 11.4 (4.9) * A |
| Pull down (kg) | 75.5 (8.0) | 71.4 (13.7) | 9.0 (3.8) * | 11.3 (5.2) * |
| Leg press (kg) | 247.0 (36.0) | 218.7 (41.5) | 23.0 (17.6) * | 24.3 (15.9) * |
| Total cholesterol (mmol/L) | 5.4 (0.4) | 5.3 (0.7) | 0.0 (0.4) | 0.0 (0.6) |
| HDL-C (mmol/L) | 1.1 (0.2) A | 1.4 (0.3) A | 0.1 (0.1) | 0.0 (0.2) |
| LDL-C (mmol/L) | 3.4 (0.5) | 3.3 (0.6) | 0.1 (0.5) | −0.1 (0.4) |
| Triglycerides (mmol/L) | 3.0 (1.6) A | 1.6 (0.7) A | −0.8 (2.1) | 0.1 (0.9) |
| Plasma free fatty acids (mmol/L) | 0.3 (0.1) | 0.2 (0.1) | −0.1 (0.1) | 0.0 (0.1) |
| Body weight (kg) | 92.5 (13.2) | 85.6 (12.3) | −1.0 (2.5) | −1.0 (2.0) * |
| Fat mass (L) | 42.4 (10.7) | 37.4 (9.1) | −3.2 (2.6) * | −2.8 (2.2) * |
| Fat free mass (L) | 38.9 (5.3) | 36.9 (4.4) | 2.6 (1.6) * | 2.0 (1.0) * |
| SAT (AU) | 8034.6 (51.9) | 6848.1 (50.3) | −427.0 (22.6) | −582.4 (24.7) |
| IAAT (AU) | 4411.6 (38.3) A | 2886.0 (40.1) A | −677.8 (24.5) * | −556.1 (19.4) * |
| Plasma leptin (ng/mL) | 15.5 (8.3) | 11.3 (5.8) | −1.8 (2.3) | −3.2 (2.8) * |
| Plasma adiponectin (ng/mL) | 45.5 (15.2) | 48.4 (21.0) | −6.8 (8.1) A | −1.6 (3.0) * A |
| Plasma CRP (ng/mL) | 3.9 (3.5) A | 1.5 (2.1) A | 0.3 (1.0) A | −2.3 (3.7) A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viken, J.K.; Olsen, T.; Drevon, C.A.; Hjorth, M.; Birkeland, K.I.; Norheim, F.; Lee-Ødegård, S. Intra-Individual Variations in How Insulin Sensitivity Responds to Long-Term Exercise: Predictions by Machine Learning Based on Large-Scale Serum Proteomics. Metabolites 2024, 14, 335. https://doi.org/10.3390/metabo14060335
Viken JK, Olsen T, Drevon CA, Hjorth M, Birkeland KI, Norheim F, Lee-Ødegård S. Intra-Individual Variations in How Insulin Sensitivity Responds to Long-Term Exercise: Predictions by Machine Learning Based on Large-Scale Serum Proteomics. Metabolites. 2024; 14(6):335. https://doi.org/10.3390/metabo14060335
Chicago/Turabian StyleViken, Jonas Krag, Thomas Olsen, Christian André Drevon, Marit Hjorth, Kåre Inge Birkeland, Frode Norheim, and Sindre Lee-Ødegård. 2024. "Intra-Individual Variations in How Insulin Sensitivity Responds to Long-Term Exercise: Predictions by Machine Learning Based on Large-Scale Serum Proteomics" Metabolites 14, no. 6: 335. https://doi.org/10.3390/metabo14060335
APA StyleViken, J. K., Olsen, T., Drevon, C. A., Hjorth, M., Birkeland, K. I., Norheim, F., & Lee-Ødegård, S. (2024). Intra-Individual Variations in How Insulin Sensitivity Responds to Long-Term Exercise: Predictions by Machine Learning Based on Large-Scale Serum Proteomics. Metabolites, 14(6), 335. https://doi.org/10.3390/metabo14060335