
Adipose Tissue Insulin Resistance in South Asian and Nordic Women after Gestational Diabetes Mellitus

 ,
,
Abstract

1. Introduction
2. Materials and Methods
3. Results
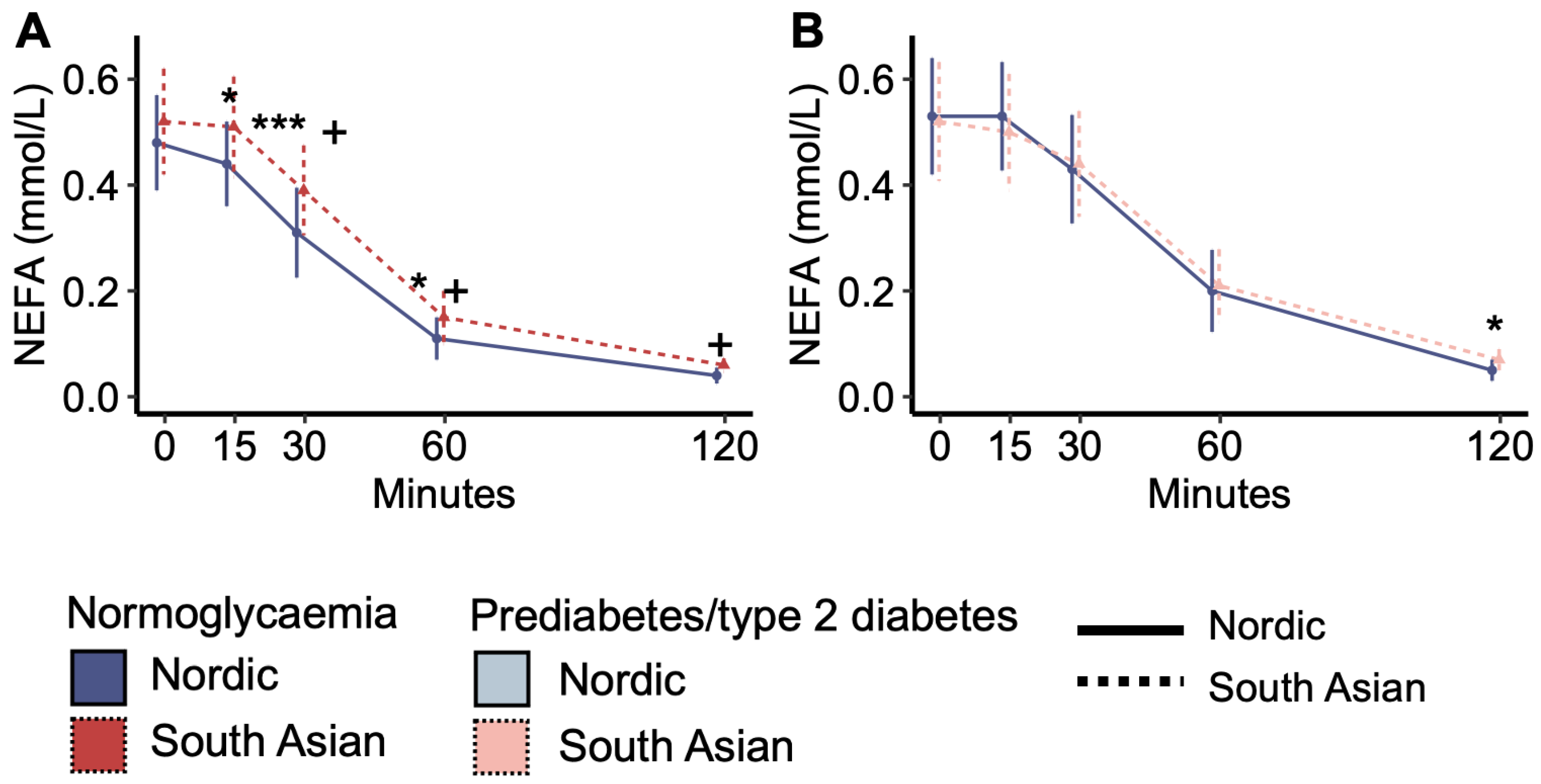
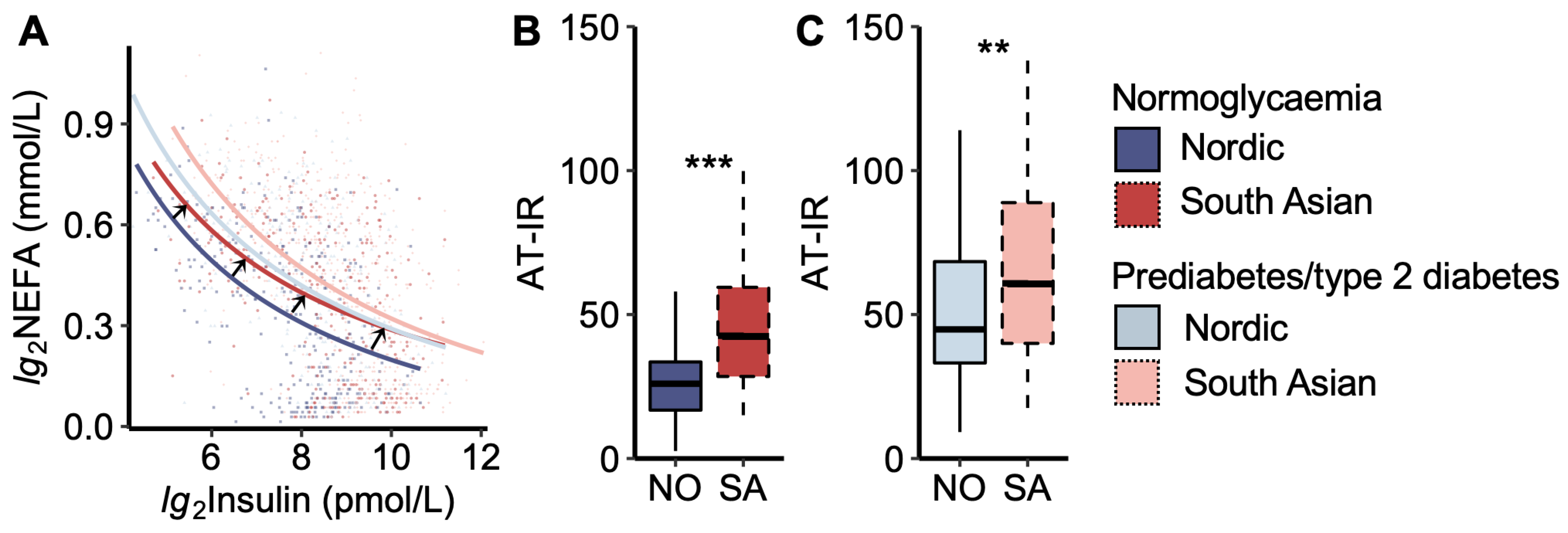
3.1. Markers of Adipose Tissue Insulin Resistance
3.2. Markers of Adipose Tissue Inflammation and Fat Mass
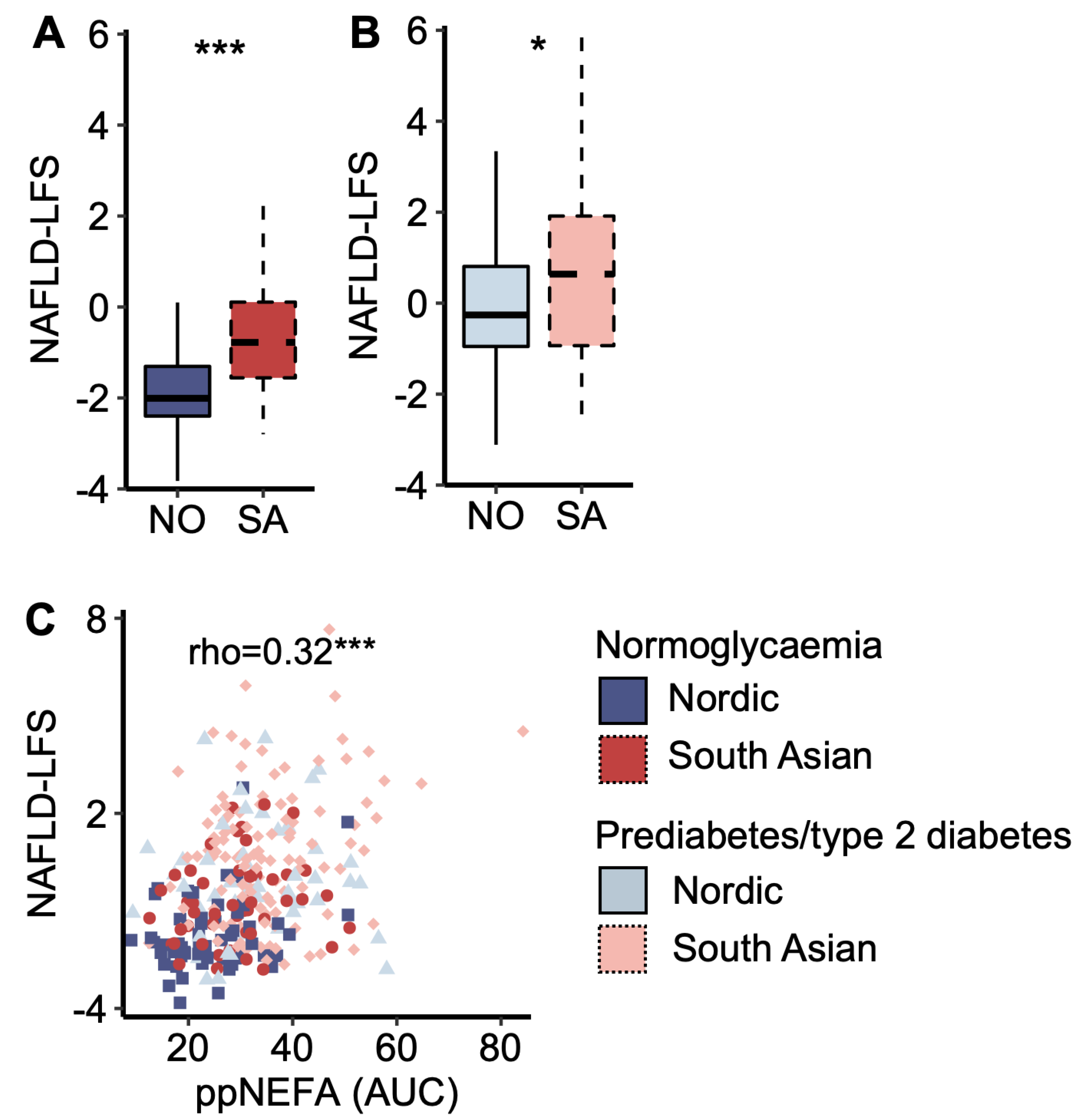
3.3. Markers of Liver Fat and Insulin Resistance and Associations with Post-Prandial Glucose Levels
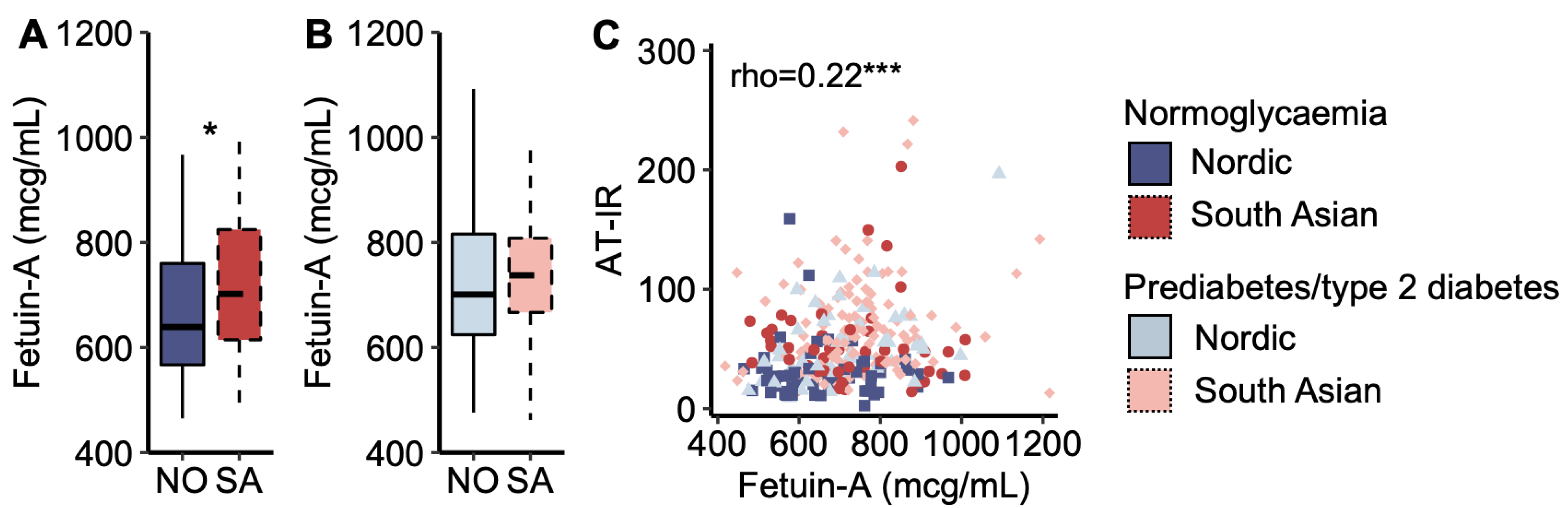
3.4. Fetuin-A and Adipose Tissue Insulin Resistance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Narayan, K.M.V.; Kanaya, A.M. Why are South Asians prone to type 2 diabetes? A hypothesis based on underexplored pathways. Diabetologia 2020, 63, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Gill, J.M. Type 2 diabetes in migrant south Asians: Mechanisms, mitigation, and management. Lancet Diabetes Endocrinol. 2015, 3, 1004–1016. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Nermoen, I.; Qvigstad, E.; Tran, A.T.; Sommer, C.; Sattar, N.; Gill, J.M.R.; Gulseth, H.L.; Sollid, S.T.; Birkeland, K.I. High prevalence and significant ethnic differences in actionable HbA1C after gestational diabetes mellitus in women living in Norway. BMC Med. 2022, 20, 318. [Google Scholar] [CrossRef] [PubMed]
- Ke, C.; Narayan, K.M.V.; Chan, J.C.N.; Jha, P.; Shah, B.R. Pathophysiology, phenotypes and management of type 2 diabetes mellitus in Indian and Chinese populations. Nat. Rev. Endocrinol. 2022, 18, 413–432. [Google Scholar] [CrossRef] [PubMed]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef]
- Dennison, R.A.; Chen, E.S.; Green, M.E.; Legard, C.; Kotecha, D.; Farmer, G.; Sharp, S.J.; Ward, R.J.; Usher-Smith, J.A.; Griffin, S.J. The absolute and relative risk of type 2 diabetes after gestational diabetes: A systematic review and meta-analysis of 129 studies. Diabetes Res. Clin. Pract. 2021, 171, 108625. [Google Scholar] [CrossRef]
- Sharma, A.; Lee-Ødegård, S.; Qvigstad, E.; Sommer, C.; Sattar, N.; Gill, J.M.R.; Gulseth, H.L.; Sollid, S.T.; Nermoen, I.; Birkeland, K.I. β-Cell Function, Hepatic Insulin Clearance, and Insulin Sensitivity in South Asian and Nordic Women After Gestational Diabetes Mellitus. Diabetes 2022, 71, 2530–2538. [Google Scholar] [CrossRef]
- Abbasi, J. MASALA Study Probes Why People With South Asian Ancestry Have Increased Cardiovascular Disease Risks. JAMA 2022, 328, 511–514. [Google Scholar] [CrossRef]
- Iliodromiti, S.; McLaren, J.; Ghouri, N.; Miller, M.R.; Dahlqvist Leinhard, O.; Linge, J.; Ballantyne, S.; Platt, J.; Foster, J.; Hanvey, S.; et al. Liver, visceral and subcutaneous fat in men and women of South Asian and white European descent: A systematic review and meta-analysis of new and published data. Diabetologia 2023, 66, 44–56. [Google Scholar] [CrossRef]
- Roden, M.; Shulman, G.I. The integrative biology of type 2 diabetes. Nature 2019, 576, 51–60. [Google Scholar] [CrossRef]
- Petersen, M.C.; Shulman, G.I. Mechanisms of Insulin Action and Insulin Resistance. Physiol. Rev. 2018, 98, 2133–2223. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; McGuire, D.K.; Gill, J.M.R. High Circulating Triglycerides Are Most Commonly a Marker of Ectopic Fat Accumulation: Connecting the Clues to Advance Lifestyle Interventions. Circulation 2022, 146, 77–79. [Google Scholar] [CrossRef] [PubMed]
- Skurk, T.; Alberti-Huber, C.; Herder, C.; Hauner, H. Relationship between adipocyte size and adipokine expression and secretion. J. Clin. Endocrinol. Metab. 2007, 92, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Musso, G.; Cassader, M.; Rosina, F.; Gambino, R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of randomised trials. Diabetologia 2012, 55, 885–904. [Google Scholar] [CrossRef] [PubMed]
- Raddatz, K.; Frangioudakis, G.; Diakanastasis, B.; Liao, B.M.; Leitges, M.; Schmitz-Peiffer, C. Deletion of protein kinase Cε in mice has limited effects on liver metabolite levels but alters fasting ketogenesis and gluconeogenesis. Diabetologia 2012, 55, 2789–2793. [Google Scholar] [CrossRef] [PubMed]
- Najjar, S.M.; Abdolahipour, R.; Ghadieh, H.E.; Jahromi, M.S.; Najjar, J.A.; Abuamreh, B.A.M.; Zaidi, S.; Kumarasamy, S.; Muturi, H.T. Regulation of Insulin Clearance by Non-Esterified Fatty Acids. Biomedicines 2022, 10, 1899. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Schick, F.; Birkenfeld, A.L.; Häring, H.U.; White, M.F. The role of hepatokines in NAFLD. Cell Metab. 2023, 35, 236–252. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Haring, H.U. Circulating fetuin-A and free fatty acids interact to predict insulin resistance in humans. Nat. Med. 2013, 19, 394–395. [Google Scholar] [CrossRef] [PubMed]
- Pal, D.; Dasgupta, S.; Kundu, R.; Maitra, S.; Das, G.; Mukhopadhyay, S.; Ray, S.; Majumdar, S.S.; Bhattacharya, S. Fetuin-A acts as an endogenous ligand of TLR4 to promote lipid-induced insulin resistance. Nat. Med. 2012, 18, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Norheim, F.; Gulseth, H.L.; Langleite, T.M.; Kolnes, K.J.; Tangen, D.S.; Stadheim, H.K.; Gilfillan, G.D.; Holen, T.; Birkeland, K.I.; et al. Interaction between plasma fetuin-A and free fatty acids predicts changes in insulin sensitivity in response to long-term exercise. Physiol. Rep. 2017, 5, e13183. [Google Scholar] [CrossRef]
- Lee-Ødegård, S.; Ueland, T.; Thorsby, P.M.; Aukrust, P.; Michelsen, A.E.; Halvorsen, B.; Drevon, C.A.; Birkeland, K.I. Fetuin-A mediates the difference in adipose tissue insulin resistance between young adult pakistani and norwegian patients with type 2 diabetes. BMC Endocr. Disord. 2022, 22, 208. [Google Scholar] [CrossRef] [PubMed]
- WHO. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of a WHO Consultation. Part 1, Diagnosis and Classification of Diabetes Mellitus. Available online: https://apps.who.int/iris/handle/10665/66040 (accessed on 30 November 2020).
- Norwegian Directorate of Health. Nasjonal Faglig Retningslinjer Svangerskapsdiabetes [National Guidelines Gestational Diabetes Mellitus]. Available online: https://www.helsedirektoratet.no/retningslinjer/svangerskapsdiabetes (accessed on 30 August 2020).
- Jung, T.Y.; Kim, M.S.; Hong, H.P.; Kang, K.A.; Jun, D.W. Comparative Assessment and External Validation of Hepatic Steatosis Formulae in a Community-Based Setting. J. Clin. Med. 2020, 9, 2851. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.P.; Misra, A.; Nigam, P.; Guleria, R.; Pasha, M.A. Phenotype, Body Composition, and Prediction Equations (Indian Fatty Liver Index) for Non-Alcoholic Fatty Liver Disease in Non-Diabetic Asian Indians: A Case-Control Study. PLoS ONE 2015, 10, e0142260. [Google Scholar] [CrossRef]
- The International Expert Committee. International Expert Committee Report on the Role of the A1C Assay in the Diagnosis of Diabetes. Diabetes Care 2009, 32, 1327. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S15. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Use of Glycated Haemoglobin (HbA1c) in Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation. Available online: https://apps.who.int/iris/handle/10665/70523 (accessed on 25 October 2021).
- Catalano, P.M. Obesity, insulin resistance, and pregnancy outcome. Reproduction 2010, 140, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Jocken, J.W.E.; Goossens, G.H.; Boon, H.; Mason, R.R.; Essers, Y.; Havekes, B.; Watt, M.J.; van Loon, L.J.; Blaak, E.E. Insulin-mediated suppression of lipolysis in adipose tissue and skeletal muscle of obese type 2 diabetic men and men with normal glucose tolerance. Diabetologia 2013, 56, 2255–2265. [Google Scholar] [CrossRef]
- Hill, A.A.; Reid Bolus, W.; Hasty, A.H. A decade of progress in adipose tissue macrophage biology. Immunol. Rev. 2014, 262, 134–152. [Google Scholar] [CrossRef]
- Peters, M.J.; Ghouri, N.; McKeigue, P.; Forouhi, N.G.; Sattar, N. Circulating IL-6 concentrations and associated anthropometric and metabolic parameters in South Asian men and women in comparison to European whites. Cytokine 2013, 61, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Sommer, C.; Jenum, A.K.; Waage, C.W.; Mørkrid, K.; Sletner, L.; Birkeland, K.I. Ethnic differences in BMI, subcutaneous fat, and serum leptin levels during and after pregnancy and risk of gestational diabetes. Eur. J. Endocrinol. 2015, 172, 649–656. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Sattar, N.; McKeigue, P.M. Relation of C-reactive protein to body fat distribution and features of the metabolic syndrome in Europeans and South Asians. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 1327–1331. [Google Scholar] [CrossRef]
- Holt, H.B.; Wild, S.H.; Wood, P.J.; Zhang, J.; Darekar, A.A.; Dewbury, K.; Poole, R.B.; Holt, R.I.G.; Phillips, D.I.; Byrne, C.D. Non-esterified fatty acid concentrations are independently associated with hepatic steatosis in obese subjects. Diabetologia 2006, 49, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstråle, M.; Groop, L.; et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef] [PubMed]
- ter Horst, K.W.; Gilijamse, P.W.; Versteeg, R.I.; Ackermans, M.T.; Nederveen, A.J.; la Fleur, S.E.; Romijn, J.A.; Nieuwdorp, M.; Zhang, D.; Samuel, V.T.; et al. Hepatic Diacylglycerol-Associated Protein Kinase Cε Translocation Links Hepatic Steatosis to Hepatic Insulin Resistance in Humans. Cell Rep. 2017, 19, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Barbour, L.A. Metabolic Culprits in Obese Pregnancies and Gestational Diabetes Mellitus: Big Babies, Big Twists, Big Picture: The 2018 Norbert Freinkel Award Lecture. Diabetes Care 2019, 42, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Bhattacharya, S.; Biswas, A.; Majumdar, S.S.; Mukhopadhyay, S.; Ray, S.; Bhattacharya, S. NF-kappaB mediates lipid-induced fetuin-A expression in hepatocytes that impairs adipocyte function effecting insulin resistance. Biochem. J. 2010, 429, 451–462. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normoglycaemia | p | Prediabetes/Type 2 Diabetes | p | |||
|---|---|---|---|---|---|---|
| Nordics | South Asians | Nordics | South Asians | |||
| Participants, n (%) | 57/108 [52.7] | 55/178 [30.9] | 51/108 [47.2] | 123/178 [69.1] | <0.001 * | |
| Age (years) | 36.7 (4.9) | 34.4 (3.9) | <0.001 | 36.2 (4.8) | 34.6 (4.2) | 0.031 |
| Years since index pregnancy | 1.4 [0.9] | 1.3 [1.2] | 0.093 | 1.6 [1.1] | 1.3 [1.0] | 0.159 |
| HbA1c (mmol/mol) | 35.0 (0.3) | 36.6 (0.5) | <0.001 | 38.0 (0.6) | 40.4 (0.4) | 0.004 |
| HbA1c (%) | 5.4 (2.1) | 5.5 (2.2) | 5.6 (2.2) | 5.8 (2.2) | ||
| Weight [kg] | 72.0 [24.0] | 68.8 [17.6] | <0.001 | 86.0 [21.0] | 72.9 [19.3] | <0.001 |
| Height (cm) | 167.9 (6.0) | 158.1(6.0) | <0.001 | 165.8 (6.0) | 160.0 (6.6) | <0.001 |
| BMI [kg/m2] | 25.5 [8.4] | 27.6 [5.4] | 0.663 | 31.9 [6.9] | 28.8 [6.4] | 0.007 |
| Waist circumference (cm) | 92.2 (14.3) | 93.6 (12.6) | 0.777 | 100.5 (12.4) | 97.9 (11.5) | 0.185 |
| Waist–hip ratio | 0.87 (0.09) | 0.88 (0.06) | 0.018 | 0.89 (0.08) | 0.91 (0.07) | 0.069 |
| Waist–height ratio | 0.55 (0.86) | 0.59 (0.77) | 0.002 | 0.61 (0.08) | 0.61 (0.07) | 0.657 |
| Total cholesterol (mmol/L) | 4.24 (0.82) | 4.2 (0.6) | 0.358 | 4.3 (0.8) | 4.4 (0.7) | 0.397 |
| ASAT (U/L) | 20.7 (4.3) | 24.3 (5.9) | 0.004 | 23.8 (7.7) | 24.2 (5.2) | 0.685 |
| ALAT (U/L) | 16.3 (6.1) | 20.4 (9.1) | 0.065 | 22.8 (13.9) | 22.1 (8.4) | 0.668 |
| Parity (no.) | 1.7 (0.7) | 2.1 (1.0) | <0.001 | 1.7 (0.7) | 2.2 (1.0) | 0.001 |
| Prior GDM (yes/no [%]) | 9/57 [16] | 13/54 [24] | 0.100 | 15/51 [29] | 42/121 [35] | 0.503 |
| Family history of diabetes (yes/no [%]) | 10/46 [22] | 38/51 [75] | <0.001 | 12/45 [27] | 87/117 [74] | <0.001 |
| Insulin use in pregnancy (yes/no [%]) | 11/57 [19] | 19/55 [35] | 0.138 | 23/51 [45] | 53/123 [43] | 0.809 |
| Years of education | 17.2 (2.8) | 14.4 (3.3) | <0.001 | 16.3 (3.1) | 15.0 (3.5) | 0.022 |
| Smoking | <0.001 | <0.001 | ||||
| Daily (yes/no [%]) | 1/57 (1.8) | 2/55 (3.6) | 7/51 (13.7) | 2/123 (1.6) | ||
| Earlier (yes/no [%]) | 18/57 (31.6) | 2/55 (3.6) | 20/51 (39.2) | 2/123 (1.6) | ||
| Never (yes/no [%]) | 38/57 (66.7) | 51/55 (92.7) | 24/51 (47.1) | 119/123 (96.8) | ||
| Alcohol consumption | <0.001 | <0.001 | ||||
| Weekly (yes/no [%]) | 18/57 (31.6) | 1/55 (1.8) | 10/51 (19.6) | 2/123 (1.6) | ||
| Less than weekly (yes/no [%]) | 38/57 (66.7) | 8/55 (14.6) | 38/51 (74.5) | 12/123 (9.8) | ||
| Never (yes/no [%]) | 1/57 (1.8) | 46/55 (83.6) | 3/51 (5.9) | 109/123 (88.6) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kvist, A.A.S.; Sharma, A.; Sommer, C.; Qvigstad, E.; Gulseth, H.L.; Sollid, S.T.; Nermoen, I.; Sattar, N.; Gill, J.; Tannæs, T.M.; et al. Adipose Tissue Insulin Resistance in South Asian and Nordic Women after Gestational Diabetes Mellitus. Metabolites 2024, 14, 288. https://doi.org/10.3390/metabo14050288
Kvist AAS, Sharma A, Sommer C, Qvigstad E, Gulseth HL, Sollid ST, Nermoen I, Sattar N, Gill J, Tannæs TM, et al. Adipose Tissue Insulin Resistance in South Asian and Nordic Women after Gestational Diabetes Mellitus. Metabolites. 2024; 14(5):288. https://doi.org/10.3390/metabo14050288
Chicago/Turabian StyleKvist, Ahalya Anita Suntharalingam, Archana Sharma, Christine Sommer, Elisabeth Qvigstad, Hanne Løvdal Gulseth, Stina Therese Sollid, Ingrid Nermoen, Naveed Sattar, Jason Gill, Tone Møller Tannæs, and et al. 2024. "Adipose Tissue Insulin Resistance in South Asian and Nordic Women after Gestational Diabetes Mellitus" Metabolites 14, no. 5: 288. https://doi.org/10.3390/metabo14050288
APA StyleKvist, A. A. S., Sharma, A., Sommer, C., Qvigstad, E., Gulseth, H. L., Sollid, S. T., Nermoen, I., Sattar, N., Gill, J., Tannæs, T. M., Birkeland, K. I., & Lee-Ødegård, S. (2024). Adipose Tissue Insulin Resistance in South Asian and Nordic Women after Gestational Diabetes Mellitus. Metabolites, 14(5), 288. https://doi.org/10.3390/metabo14050288