
Association of Dietary Protein Sources and Their Adequacy, Body Composition and Risk of Sarcopenic Obesity in South Korean Populations: A Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Definition of Sarcopenia and SO
2.3. Dietary Assessment
2.4. Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prado, C.; Wells, J.; Smith, S.; Stephan, B.; Siervo, M. Sarcopenic obesity: A Critical appraisal of the current evidence. Clin. Nutr. 2012, 31, 583–601. [Google Scholar] [CrossRef]
- Silveira, E.A.; Filho, R.R.d.S.; Spexoto, M.C.B.; Haghighatdoost, F.; Sarrafzadegan, N.; de Oliveira, C. The Role of Sarcopenic Obesity in Cancer and Cardiovascular Disease: A Synthesis of the Evidence on Pathophysiological Aspects and Clinical Implications. Int. J. Mol. Sci. 2021, 22, 4339. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Atkins, J.L. Muscle loss and obesity: The health implications of sarcopenia and sarcopenic obesity. Proc. Nutr. Soc. 2015, 74, 405–412. [Google Scholar] [CrossRef]
- Arango-Lopera, V.E.; Arroyo, P.; Gutiérrez-Robledo, L.M.; Perez-Zepeda, M.U.; Cesari, M. Mortality as an adverse outcome of sarcopenia. J. Nutr. Health Aging 2013, 17, 259–262. [Google Scholar] [CrossRef]
- Stenholm, S.; Rantanen, T.; Visser, M.; Kritchevsky, S.B.; Ferrucci, L. Sarcopenic obesity: Definition, cause and consequences. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 693–700. [Google Scholar] [CrossRef]
- Cantero, I.; Abete, I.; Babio, N.; Arós, F.; Corella, D.; Estruch, R.; Fitó, M.; Hebert, J.R.; Martínez-González, M.Á.; Pintó, X.; et al. Dietary Inflammatory Index and liver status in subjects with different adiposity levels within the PREDIMED trial. Clin. Nutr. 2018, 37, 1736–1743. [Google Scholar] [CrossRef]
- Freisling, H.; Viallon, V.; Lennon, H.; Bagnardi, V.; Ricci, C.; Butterworth, A.S.; Sweeting, M.; Muller, D.; Romieu, I.; Bazelle, P.; et al. Lifestyle factors and risk of multimorbidity of cancer and cardiometabolic diseases: A multinational cohort study. BMC Med. 2020, 18, 5. [Google Scholar] [CrossRef]
- Baek, Y.; Seo, B.-N.; Jeong, K.; Yoo, H.; Lee, S. Lifestyle, genomic types and non-communicable diseases in Korea: A protocol for the Korean Medicine Daejeon Citizen Cohort study (KDCC). BMJ Open 2020, 10, e034499. [Google Scholar] [CrossRef]
- Jang, E.; Baek, Y.; Park, K.; Lee, S. Could the Sasang constitution itself be a risk factor of abdominal obesity? BMC Complement. Altern. Med. 2013, 13, 72. [Google Scholar] [CrossRef]
- Choi, K.; Lee, J.; Yoo, J.; Lee, E.; Koh, B.; Lee, J. Sasang constitutional types can act as a risk factor for insulin resistance. Diabetes Res. Clin. Pr. 2011, 91, e57–e60. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; Baek, Y. Effects of Life Style on Metabolic Syndrome Stage according to the Sasang Constitution. J. Sasang Const. Med. 2017, 29, 232–241. [Google Scholar]
- Kim, J.; Jeong, K.; Lee, S.; Seo, B.N.; Baek, Y. Low nutritional status links to the prevalence of pre-metabolic syndrome and its cluster in metabolically high-risk Korean adults: A cross-sectional study. Medicine 2021, 100, e25905. [Google Scholar] [CrossRef]
- Kim, J.; Jeong, K.; Lee, S.; Baek, Y. Relationship between Low Vegetable Consumption, Increased High-Sensitive C-Reactive Protein Level, and Cardiometabolic Risk in Korean Adults with Tae-Eumin: A Cross-Sectional Study. Evid. Based Complement. Altern. Med. 2021, 2021, 3631445. [Google Scholar] [CrossRef]
- Andreoli, A.; Garaci, F.; Cafarelli, F.P.; Guglielmi, G. Body composition in clinical practice. Eur. J. Radiol. 2016, 85, 1461–1468. [Google Scholar] [CrossRef]
- Stefanaki, C.; Pervanidou, P.; Boschiero, D.; Chrousos, G.P. Chronic stress and body composition disorders: Implications for health and disease. Hormones 2018, 17, 33–43. [Google Scholar] [CrossRef]
- Miljkovic, I.; Zmuda, J.M. Epidemiology of myosteatosis. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 260–264. [Google Scholar] [CrossRef]
- Apostolopoulos, V.; de Courten, M.P.J.; Stojanovska, L.; Blatch, G.L.; Tangalakis, K.; de Courten, B. The complex immunological and inflammatory network of adipose tissue in obesity. Mol. Nutr. Food Res. 2016, 60, 43–57. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Caterson, I.; Seidell, J.C.; James, W.P. Adipose tissue dysfunction contributes to obesity related metabolic diseases. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 163–177. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef]
- Haghighat, N.; Ashtary-Larky, D.; Bagheri, R.; Wong, A.; Cheraghloo, N.; Moradpour, G.; Nordvall, M.; Asbaghi, O.; Moeinvaziri, N.; Amini, M.; et al. Effects of 6 Months of Soy-Enriched High Protein Compared to Eucaloric Low Protein Snack Replacement on Appetite, Dietary Intake, and Body Composition in Normal-Weight Obese Women: A Randomized Controlled Trial. Nutrients 2021, 13, 2266. [Google Scholar] [CrossRef]
- Kim, I.-S. Current Perspectives on the Beneficial Effects of Soybean Isoflavones and Their Metabolites for Humans. Antioxidants 2021, 10, 1064. [Google Scholar] [CrossRef]
- Islam, S.U.; Ahmed, M.B.; Ahsan, H.; Lee, Y.-S. Recent Molecular Mechanisms and Beneficial Effects of Phytochemicals and Plant-Based Whole Foods in Reducing LDL-C and Preventing Cardiovascular Disease. Antioxidants 2021, 10, 784. [Google Scholar] [CrossRef]
- Norde, M.M.; Collese, T.S.; Giovannucci, E.; Rogero, M.M. A posteriori dietary patterns and their association with systemic low-grade inflammation in adults: A systematic review and meta-analysis. Nutr. Rev. 2021, 79, 331–350. [Google Scholar] [CrossRef]
- Barazzoni, R.; Bischoff, S.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic Obesity: Time to Meet the Challenge. Obes. Facts 2018, 11, 294–305. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Chen, L.-K.; Liu, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Bahyah, K.S.; Chou, M.-Y.; Chen, L.-Y.; Hsu, P.-S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Lee, H.; Park, S. Regional differences in the associations of diet quality, obesity, and possible sarcopenia using the seventh Korea National Health and Nutrition Examination Survey (2016–2018). Epidemiol. Health 2023, 45, e2023059. [Google Scholar] [CrossRef]
- Hwang, J. Prevalence, Anthropometric Risk Factors, and Clinical Risk Factors in Sarcopenic Women in Their 40s. J. Korean Soc. Phys. Med. 2023, 18, 22–31. [Google Scholar] [CrossRef]
- Morton, R.W.; Murphy, K.T.; McKellar, S.R.; Schoenfeld, B.J.; Henselmans, M.; Helms, E.; Aragon, A.A.; Devries, M.C.; Banfield, L.; Krieger, J.W.; et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. Br. J. Sports Med. 2018, 52, 376–384. [Google Scholar] [CrossRef]
- Baek, Y.-H.; Jang, E.-S.; Park, K.-H.; Yoo, J.-H.; Jin, H.-J.; Lee, S.-W. Development and Validation of Brief KS-15 (Korea Sasang Constitutional Diagnostic Questionnaire) Based on Body Shape, Temperament and Symptoms. J. Sasang Const. Med. 2015, 27, 211–221. [Google Scholar] [CrossRef]
- Lim, S.; Kim, J.H.; Yoon, J.W.; Kang, S.M.; Choi, S.H.; Park, Y.J.; Kim, K.W.; Lim, J.Y.; Park, K.S.; Jang, H.C. Sarcopenic Obesity: Prevalence and Association with Metabolic Syndrome in the Korean Longitudinal Study on Health and Aging (KLoSHA). Diabetes Care 2010, 33, 1652–1654. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Lee, Y.; Chung, Y.-S.; Lee, D.-J.; Joo, N.-S.; Hong, D.; Song, G.E.; Kim, H.-J.; Choi, Y.J.; Kim, K.-M. Prevalence of Sarcopenia and Sarcopenic Obesity in the Korean Population Based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. Ser. A 2012, 67, 1107–1113. [Google Scholar] [CrossRef]
- Sakuma, K.; Yamaguchi, A. Sarcopenic Obesity and Endocrinal Adaptation with Age. Int. J. Endocrinol. 2013, 2013, 204164. [Google Scholar] [CrossRef]
- An, K.O.; Kim, J. Association of Sarcopenia and Obesity with Multimorbidity in Korean Adults: A Nationwide Cross-Sectional Study. J. Am. Med. Dir. Assoc. 2016, 17, 960.e1–960.e7. [Google Scholar] [CrossRef]
- Stefanaki, C.; Peppa, M.; Boschiero, D.; Chrousos, G.P. Healthy overweight/obese youth: Early osteosarcopenic obesity features. Eur. J. Clin. Investig. 2016, 46, 767–778. [Google Scholar] [CrossRef]
- Rogeri, P.S.; Zanella, R.; Martins, G.L.; Garcia, M.D.A.; Leite, G.; Lugaresi, R.; Gasparini, S.O.; Sperandio, G.A.; Ferreira, L.H.B.; Souza-Junior, T.P.; et al. Strategies to Prevent Sarcopenia in the Aging Process: Role of Protein Intake and Exercise. Nutrients 2021, 14, 52. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-related and disease-related muscle loss: The effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef]
- Kim, J.; Baek, Y.; Jeong, K.; Lee, S. Association of Dietary Factors with Grip Strength, Body Fat, and Prevalence of Sarcopenic Obesity in Rural Korean Elderly with Cardiometabolic Multimorbidity. Front. Nutr. 2022, 9, 910481. [Google Scholar] [CrossRef]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of Animal and Plant Protein Intake with All-Cause and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Zheng, J.; Zhu, T.; Yang, G.; Zhao, L.; Li, F.; Park, Y.-M.; Tabung, F.K.; Steck, S.E.; Li, X.; Wang, H. The Isocaloric Substitution of Plant-Based and Animal-Based Protein in Relation to Aging-Related Health Outcomes: A Systematic Review. Nutrients 2022, 14, 272. [Google Scholar] [CrossRef]
- Rasaei, N.; Kashavarz, S.A.; Yekaninejad, M.S.; Mirzaei, K. The association between sarcopenic obesity (SO) and major dietary patterns in overweight and obese adult women. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2519–2524. [Google Scholar] [CrossRef]
- Starr, K.N.P.; Connelly, M.A.; Orenduff, M.C.; McDonald, S.R.; Sloane, R.; Huffman, K.M.; Kraus, W.E.; Bales, C.W. Impact on cardiometabolic risk of a weight loss intervention with higher protein from lean red meat: Combined results of 2 randomized controlled trials in obese middle-aged and older adults. J. Clin. Lipidol. 2019, 13, 920–931. [Google Scholar] [CrossRef]
- Wen, S.; Zhou, G.; Song, S.; Xu, X.; Voglmeir, J.; Liu, L.; Zhao, F.; Li, M.; Yu, X.; Bai, Y.; et al. Discrimination of in vitro and in vivo digestion products of meat proteins from pork, beef, chicken, and fish. Proteomics 2015, 15, 3688–3698. [Google Scholar] [CrossRef]
- Becerra-Tomás, N.; Babio, N.; Martínez-González, M.; Corella, D.; Estruch, R.; Ros, E.; Fitó, M.; Serra-Majem, L.; Salaverria, I.; Lamuela-Raventós, R.M.; et al. Replacing red meat and processed red meat for white meat, fish, legumes or eggs is associated with lower risk of incidence of metabolic syndrome. Clin. Nutr. 2016, 35, 1442–1449. [Google Scholar] [CrossRef]
- Bohrer, B.M. Review: Nutrient density and nutritional value of meat products and non-meat foods high in protein. Trends Food Sci. Technol. 2017, 65, 103–112. [Google Scholar] [CrossRef]

{kind=link}
| General Characteristics | SO (n = 199) | OB (n = 313) | S (n = 81) | Normal (n = 1374) | p-Value |
|---|---|---|---|---|---|
| Age (years) (mean ± SE) | 0.279 | ||||
| 30–39 years (n, %) | 71 (35.7) | 87 (27.8) | 24 (29.6) | 304 (29.7) | |
| 40–55 years | 128 (64.3) | 226 (72.2) | 57 (70.4) | 509 (70.3) | |
| Sex (%) | <0.0001 | ||||
| Male | 68 (34.2) | 152 (48.6) | 27 (33.3) | 356 (25.9) | |
| Female | 131 (65.8) | 161 (51.4) | 54 (66.7) | 1018 (74.1) | |
| KM type 1 (%) | <0.0001 | ||||
| Taeeum | 198 (99.5) | 296 (94.6) | 49 (60.5) | 457 (33.3) | |
| Soeum | 0 (0.0) | 0 (0.0) | 14 (17.3) | 375 (27.3) | |
| Soyang | 1 (0.5) | 17 | (5.4) | 18 (22.2) | |
| Smoking (%) | <0.0001 | ||||
| Past or not | 150 (75.4) | 218 (69.6) | 63 (77.8) | 1133 (82.5) | |
| Current | 49 (24.6) | 95 (30.4) | 18 (22.2) | 241 (17.5) | |
| Drinking (%) | 0.07 | ||||
| Past or not | 69 (34.7) | 111 (35.5) | 36 (44.4) | 570 (41.5) | |
| Current | 130 (65.3) | 202 (64.5) | 45 (55.6) | 804 (58.5) | |
| Physical activity 2 (%) | 0.598 | ||||
| Insufficient | 131 (65.8) | 217 (69.3) | 59 (72.8) | 922 (67.1) | |
| Sufficient | 68 (34.2) | 96 (30.7) | 22 (27.2) | 452 (32.9) | |
| Body composition | |||||
| ASM, kg/m2 | |||||
| Male | 11.14 ± 0.09 b | 11.51 ± 0.06 a | 9.14 ± 0.15 c | 10.51 ± 0.04 c | <0.0001 |
| Female | 9.08 ± 0.06 b | 9.31 ± 0.05 a | 7.78 ± 0.09 d | 8.14 ± 0.02 c | <0.0001 |
| ASM, % | |||||
| Male | 36.39 ± 0.30 c | 41.18 ± 0.20 b | 40.85 ± 0.47 b | 43.82 ± 0.13 a | <0.0001 |
| Female | 30.32 ± 0.19 d | 33.99 ± 0.18 b | 31.63 ± 0.30 c | 36.65 ± 0.07 a | <0.0001 |
| Body fat mass, kg | |||||
| Male | 32.06 ± 0.50 a | 23.03 ± 0.34 b | 17.42 ± 0.80 c | 15.78 ± 0.22 c | <0.0001 |
| Female | 32.95 ± 0.36 a | 26.60 ± 0.32 c | 24.77 ± 0.56 b | 17.98 ± 0.13 d | <0.0001 |
| Body fat mass, kg | |||||
| Male | 35.36 ± 0.51 a | 27.33 ± 0.34 b | 26.33 ± 0.81 b | 22.16 ± 0.22 c | <0.0001 |
| Female | 44.14 ± 0.36 a | 37.78 ± 0.32 c | 40.66 ± 0.56 b | 31.84 ± 0.13 d | <0.0001 |
| BMI, kg/m 2§ | 30.50 ± 0.16 a | 27.71 ± 0.13 b | 24.27 ± 0.25 c | 23.04 ± 0.07 d | <0.0001 |
| Dietary Intake and Protein Sources | SO (n = 199) | OB (n = 313) | S (n = 81) | Normal (n = 1374) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Energy intake (kcal/day) 1 | |||||||||
| Male | 2201.81 | ±79.89 | 2253.52 | ±53.44 | 2182.85 | ±126.80 | 2274.73 | ±34.91 | 0.782 |
| Female | 2129.64 | ±60.66 | 2079.72 | ±54.82 | 2017.14 | ±94.65 | 2063.95 | ±27.77 | 0.708 |
| Macronutrients (g/day) | |||||||||
| Carbohydrates (g) | 317.99 | ±2.99 | 316.69 | ±2.41 | 321.21 | ±4.69 | 319.71 | ±1.14 | 0.658 |
| Fat (g) | 52.76 | ±0.99 | 54.00 | ±0.80 | 53.56 | ±1.55 | 52.80 | ±0.38 | 0.569 |
| Protein (g) | 71.46 | ±0.73 | 72.57 | ±0.59 | 72.30 | ±1.14 | 71.52 | ±0.28 | 0.398 |
| Protein (g/kg) | 0.92 | ±0.02 c | 1.00 | ±0.01 b | 1.20 | ±0.02 a | 1.20 | ±0.01 a | <0.0001 |
| C: F: P (%) | 59.8: 22.2: 13.4 | 59.5: 22.8: 13.6 | 60.2: 22.7: 13.5 | 60.2: 22.3: 13.4 | N/S | ||||
| Dietary protein sources (g/day) 2 | |||||||||
| Beans and tofu | 31.08 | ±2.52 | 34.93 | ±2.03 | 29.31 | ±3.95 | 34.41 | ±0.97 | 0.370 |
| Poultry and eggs | 85.34 | ±6.37 | 93.77 | ±5.15 | 81.35 | ±9.99 | 85.90 | ±2.43 | 0.293 |
| Beef and pork | 102.29 | ±7.19 | 108.37 | ±5.80 | 112.91 | ±11.28 | 109.58 | ±2.75 | 0.793 |
| Fish | 5.70 | ±0.59 | 6.04 | ±0.48 | 5.73 | ±0.93 | 6.34 | ±0.23 | 0.671 |
| SO (n = 199) | OB (n = 313) | S (n = 81) | Normal (n = 1374) | |||||
|---|---|---|---|---|---|---|---|---|
| Protein Sources (g/Day) | Beta | p-Value | Beta | p-Value | Beta | p-Value | Beta | p-Value |
| Beans and tofu | ||||||||
| ASM, kg/m2 | 0.001 | 0.68 | 0.000 | 0.80 | 0.000 | 0.80 | −0.002 | 0.60 |
| ASM, % | 0.002 | 0.62 | −0.004 | 0.07 | −0.008 | 0.59 | −0.003 | 0.13 |
| BFM, kg | 0.004 | 0.78 | 0.006 | 0.22 | 0.006 | 0.81 | 0.005 | 0.06 |
| PBF, % | −0.002 | 0.78 | 0.008 | 0.05 | 0.014 | 0.62 | 0.005 | 0.14 |
| Poultry and eggs | ||||||||
| ASM, kg/m2 | 0.000 | 0.23 | 0.000 | 0.97 | 0.000 | 0.74 | 0.000 | 0.92 |
| ASM, % | 0.001 | 0.37 | 0.001 | 0.57 | 0.004 | 0.59 | −0.002 | 0.03 |
| BFM, kg | 0.001 | 0.76 | 0.000 | 0.90 | −0.002 | 0.86 | 0.002 | 0.13 |
| PBF, % | −0.001 | 0.56 | −0.001 | 0.67 | −0.004 | 0.72 | 0.003 | 0.05 |
| Beef and pork | ||||||||
| ASM, kg/m2 | 0.002 | 0.02 | 0.000 | 0.81 | 0.000 | 0.91 | −0.001 | 0.35 |
| ASM, % | 0.000 | 0.80 | 0.000 | 0.59 | 0.001 | 0.73 | −0.002 | 0.01 |
| BFM, kg | 0.012 | 0.03 | 0.000 | 0.94 | −0.002 | 0.68 | 0.002 | 0.07 |
| PBF, % | 0.001 | 0.80 | 0.000 | 0.74 | −0.002 | 0.79 | 0.003 | 0.02 |
| Fish | ||||||||
| ASM, kg/m2 | −0.014 | 0.14 | −0.003 | 0.61 | 0.008 | 0.58 | −0.002 | 0.22 |
| ASM, % | 0.009 | 0.54 | 0.009 | 0.52 | −0.146 | 0.04 | −0.016 | 0.03 |
| BFM, kg | −0.060 | 0.32 | −0.030 | 0.31 | 0.203 | 0.06 | 0.001 | 0.21 |
| PBF, % | −0.019 | 0.49 | −0.023 | 0.37 | 0.263 | 0.04 | 0.025 | 0.06 |
| SO (n = 199) | S (n = 81) | |
|---|---|---|
| Dietary protein sources | ||
| Beans and tofu | ||
| (ref, lowest: 7.1 g/day) | ORs (CI) | |
| intermediate: 20.5 g/day | 0.74 (0.45–1.20) | 0.79 (0.40–1.58) |
| highest: 74.1 g/day | 0.56 (0.29–1.09) | 0.87 (0.41–1.84) |
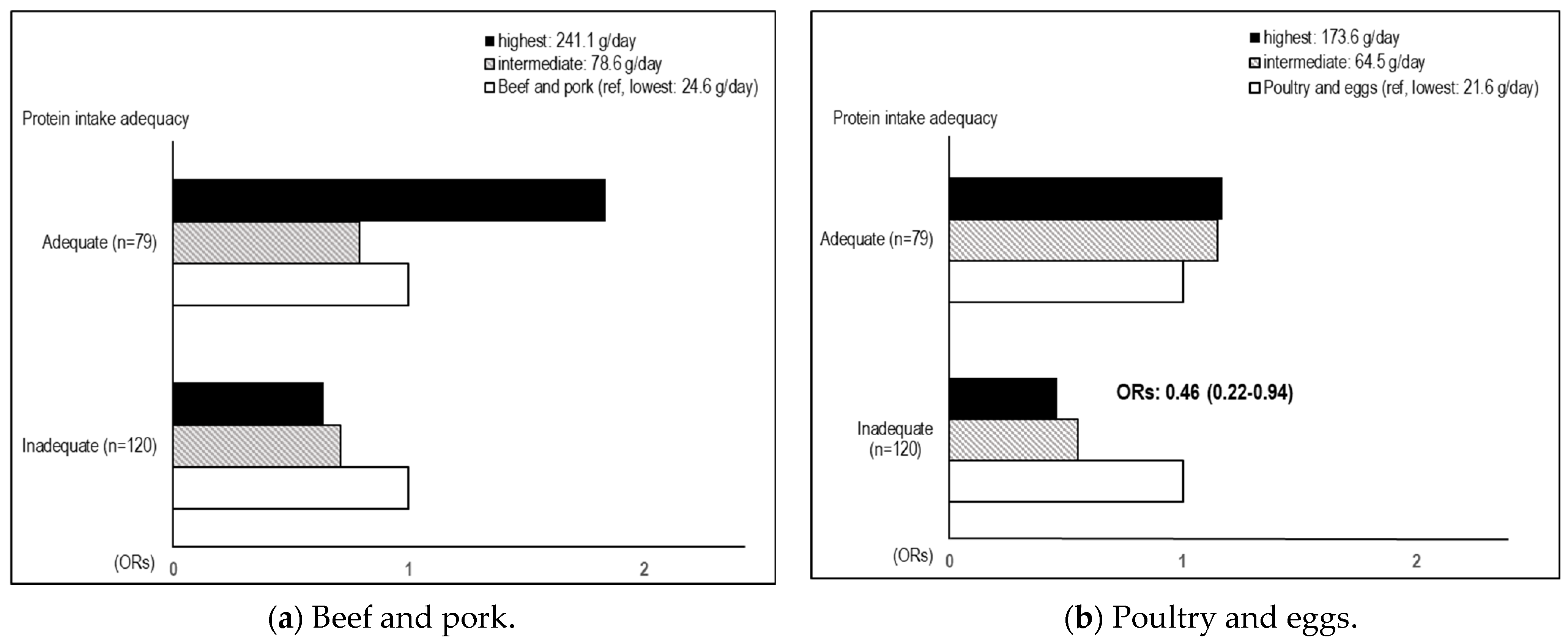
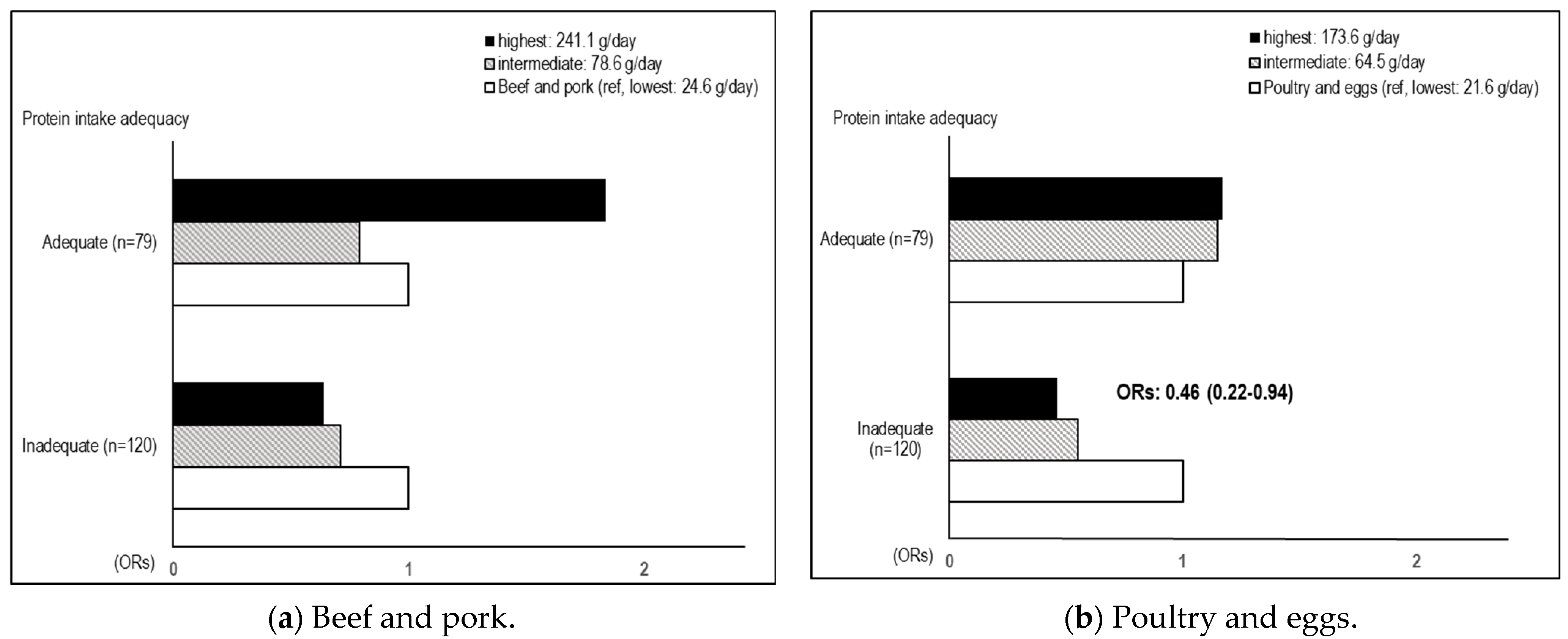
| Poultry and eggs | ||
| (ref, lowest: 21.6 g/day) | ORs (CI) | |
| intermediate: 64.5 g/day | 0.62 (0.37–1.02) | 1.05 (0.49–2.23) |
| highest: 173.6 g/day | 0.52 (0.30–0.90) | 0.95 (0.40–2.24) |
| Beef and pork | ||
| (ref, lowest: 24.6 g/day) | ORs (CI) | |
| intermediate: 78.6 g/day | 0.68 (0.41–1.13) | 1.09 (0.57–2.08) |
| highest: 241.1 g/day | 0.83 (0.46–1.49) | 0.92 (0.40–2.12) |
| Fish | ||
| (ref, lowest: 0.7 g/day) | ORs (CI) | |
| intermediate: 3.5 g/day | 0.84 (0.49–1.43) | 0.81 (0.41–1.60) |
| highest: 16.2 g/day | 0.84 (0.48–1.46) | 0.67 (0.32–1.42) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Jeong, K.; Lim, S.; Lee, S.; Baek, Y. Association of Dietary Protein Sources and Their Adequacy, Body Composition and Risk of Sarcopenic Obesity in South Korean Populations: A Cross-Sectional Study. Metabolites 2024, 14, 130. https://doi.org/10.3390/metabo14020130
Kim J, Jeong K, Lim S, Lee S, Baek Y. Association of Dietary Protein Sources and Their Adequacy, Body Composition and Risk of Sarcopenic Obesity in South Korean Populations: A Cross-Sectional Study. Metabolites. 2024; 14(2):130. https://doi.org/10.3390/metabo14020130
Chicago/Turabian StyleKim, Jieun, Kyoungsik Jeong, Sueun Lim, Siwoo Lee, and Younghwa Baek. 2024. "Association of Dietary Protein Sources and Their Adequacy, Body Composition and Risk of Sarcopenic Obesity in South Korean Populations: A Cross-Sectional Study" Metabolites 14, no. 2: 130. https://doi.org/10.3390/metabo14020130
APA StyleKim, J., Jeong, K., Lim, S., Lee, S., & Baek, Y. (2024). Association of Dietary Protein Sources and Their Adequacy, Body Composition and Risk of Sarcopenic Obesity in South Korean Populations: A Cross-Sectional Study. Metabolites, 14(2), 130. https://doi.org/10.3390/metabo14020130