
Changes in Intake and Major Food Sources of Carotenoids among U.S. Adults between 2009–2018




Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Dietary Intake of Carotenoids
2.3. Estimation of Carotenoid Intake and Major Food Sources
2.4. Statistical Analysis
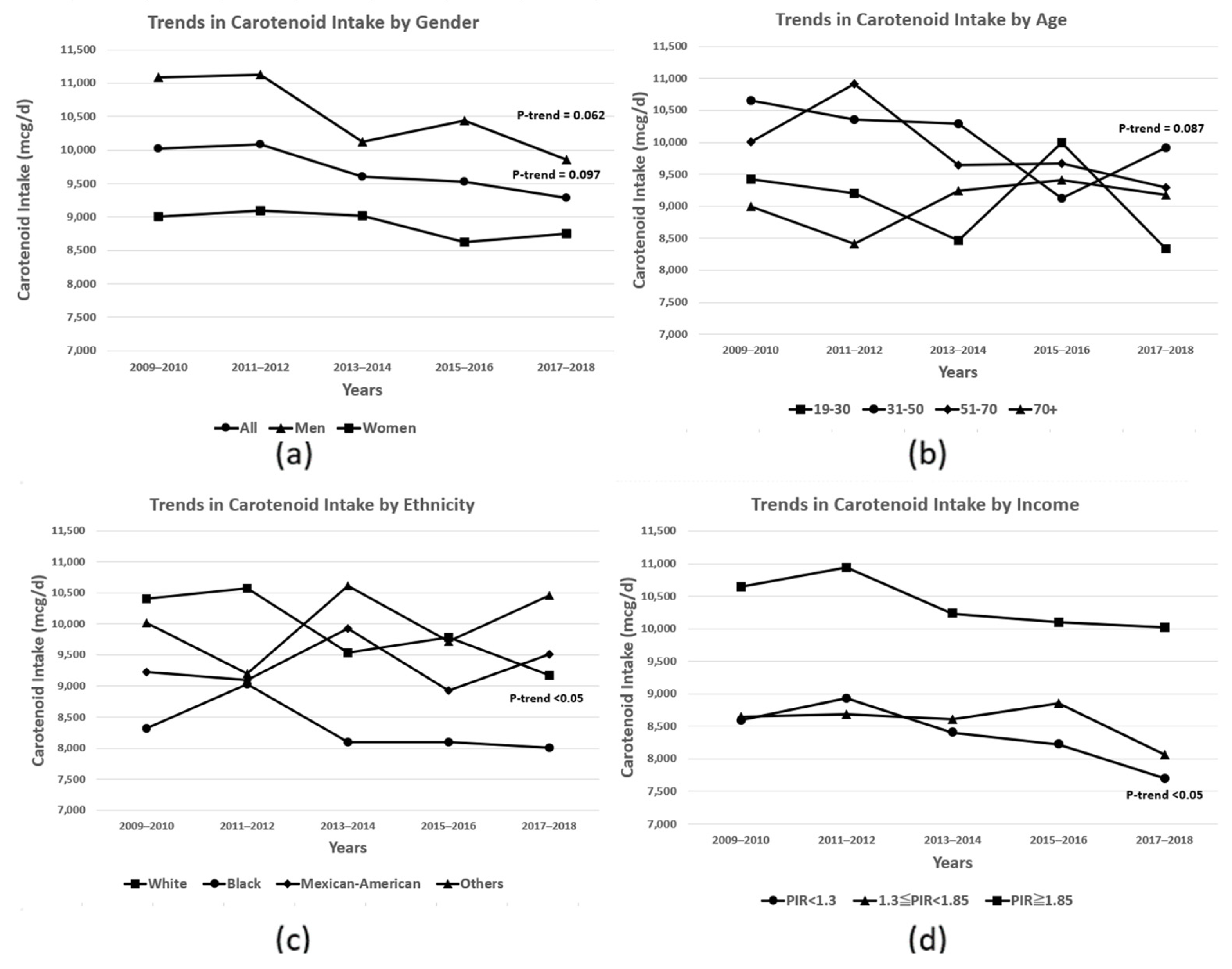
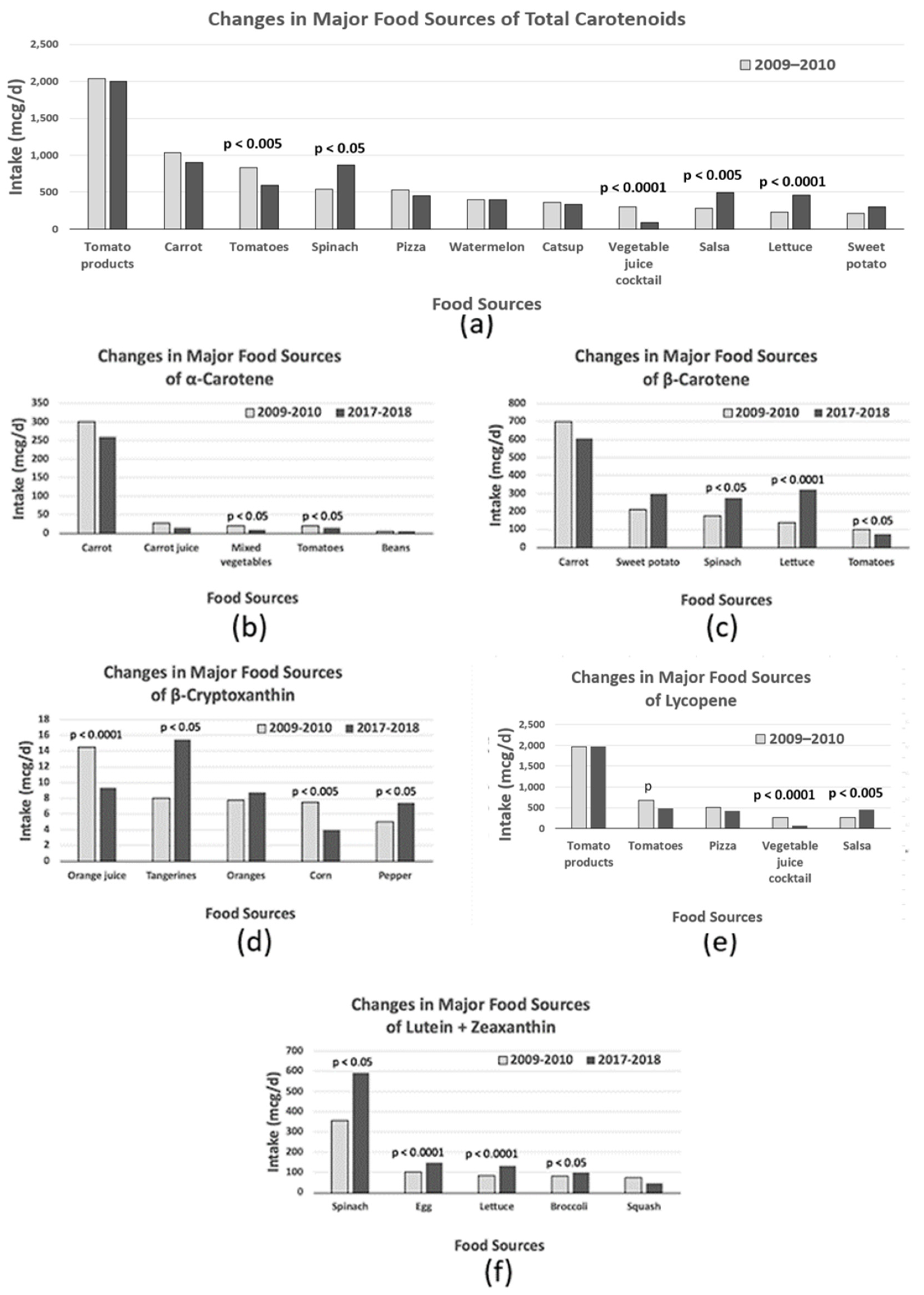
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stahl, W.; Sies, H. Antioxidant activity of carotenoids. Mol. Asp. Med. 2003, 24, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, J.; Zhang, D. Association between dietary carotenoid intakes and hypertension in adults: National Health and Nutrition Examination Survey 2007–2014. J. Hypertens. 2019, 37, 2371–2379. [Google Scholar] [CrossRef] [PubMed]
- Sluijs, I.; Cadier, E.; Beulens, J.W.; van der, A.D.; Spijkerman, A.M.; van der Schouw, Y.T. Dietary intake of carotenoids and risk of type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Arab, L.; Steck, S. Lycopene and cardiovascular disease. Am. J. Clin. Nutr. 2000, 71, 1691S–1695S. [Google Scholar] [CrossRef] [PubMed]
- Kritchevsky, S.B.; Tell, G.S.; Shimakawa, T.; Dennis, B.; Li, R.; Kohlmeier, L.; Steere, E.; Heiss, G. Provitamin A carotenoid intake and carotid artery plaques: The Atherosclerosis Risk in Communities Study. Am. J. Clin. Nutr. 1998, 68, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Leoncini, E.; Edefonti, V.; Hashibe, M.; Parpinel, M.; Cadoni, G.; Ferraroni, M.; Serraino, D.; Matsuo, K.; Olshan, A.F.; Zevallos, J.P.; et al. Carotenoid intake and head and neck cancer: A pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Eur. J. Epidemiol. 2016, 31, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Liu, Y.; Michalek, J.E.; Mesa, R.A.; Parma, D.L.; Rodriguez, R.; Mansour, A.M.; Svatek, R.; Tucker, T.C.; Ramirez, A.G. Carotenoid Intake and Circulating Carotenoids Are Inversely Associated with the Risk of Bladder Cancer: A Dose-Response Meta-analysis. Adv. Nutr. 2020, 11, 630–643. [Google Scholar] [CrossRef]
- Jung, S.; Wu, K.; Giovannucci, E.; Spiegelman, D.; Willett, W.C.; Smith-Warner, S.A. Carotenoid intake and risk of colorectal adenomas in a cohort of male health professionals. Cancer Causes Control 2013, 24, 705–717. [Google Scholar] [CrossRef]
- Van Hoang, D.; Pham, N.M.; Lee, A.H.; Tran, D.N.; Binns, C.W. Dietary Carotenoid Intakes and Prostate Cancer Risk: A Case-Control Study from Vietnam. Nutrients 2018, 10, 70. [Google Scholar] [CrossRef]
- Nkondjock, A.; Ghadirian, P.; Johnson, K.C.; Krewski, D.; Canadian Cancer Registries Epidemiology Research, G. Dietary intake of lycopene is associated with reduced pancreatic cancer risk. J. Nutr. 2005, 135, 592–597. [Google Scholar] [CrossRef]
- Bernstein, P.S.; Li, B.; Vachali, P.P.; Gorusupudi, A.; Shyam, R.; Henriksen, B.S.; Nolan, J.M. Lutein, zeaxanthin, and meso-zeaxanthin: The basic and clinical science underlying carotenoid-based nutritional interventions against ocular disease. Prog. Retin. Eye Res. 2016, 50, 34–66. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.A. Dietary carotenoids and human immune function. Nutrition 2001, 17, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Pattison, D.J.; Symmons, D.P.; Lunt, M.; Welch, A.; Bingham, S.A.; Day, N.E.; Silman, A.J. Dietary beta-cryptoxanthin and inflammatory polyarthritis: Results from a population-based prospective study. Am. J. Clin. Nutr. 2005, 82, 451–455. [Google Scholar] [CrossRef] [PubMed]
- Davinelli, S.; Ali, S.; Solfrizzi, V.; Scapagnini, G.; Corbi, G. Carotenoids and Cognitive Outcomes: A Meta-Analysis of Randomized Intervention Trials. Antioxidants 2021, 10, 223. [Google Scholar] [CrossRef] [PubMed]
- Carnauba, R.A.; Sarti, F.M.; Hassimotto, N.M.A.; Lajolo, F.M. Assessment of dietary intake of bioactive food compounds according to income level in the Brazilian population. Br. J. Nutr. 2022, 127, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Estevez-Santiago, R.; Beltran-de-Miguel, B.; Olmedilla-Alonso, B. Assessment of dietary lutein, zeaxanthin and lycopene intakes and sources in the Spanish survey of dietary intake (2009–2010). Int. J. Food Sci. Nutr. 2016, 67, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Manzi, F.; Flood, V.; Webb, K.; Mitchell, P. The intake of carotenoids in an older Australian population: The Blue Mountains Eye Study. Public. Health Nutr. 2002, 5, 347–352. [Google Scholar] [CrossRef]
- Amiot, M.J.; Latge, C.; Plumey, L.; Raynal, S. Intake Estimation of Phytochemicals in a French Well-Balanced Diet. Nutrients 2021, 13, 3628. [Google Scholar] [CrossRef]
- Han, S.; Wu, L.; Wang, W.; Li, N.; Wu, X. Trends in Dietary Nutrients by Demographic Characteristics and BMI among US Adults, 2003–2016. Nutrients 2019, 11, 2617. [Google Scholar] [CrossRef]
- Nebeling, L.C.; Forman, M.R.; Graubard, B.I.; Snyder, R.A. The impact of lifestyle characteristics on carotenoid intake in the United States: The 1987 National Health Interview Survey. Am J Public Health 1997, 87, 268–271. [Google Scholar] [CrossRef][Green Version]
- Bentley, J.U.S. Trends in Food Availability and a Dietary Assessment of Loss-Adjusted Food Availability, 1970–2014; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2017. [Google Scholar]
- O’Neill, M.E.; Carroll, Y.; Corridan, B.; Olmedilla, B.; Granado, F.; Blanco, I.; Van den Berg, H.; Hininger, I.; Rousell, A.M.; Chopra, M.; et al. A European carotenoid database to assess carotenoid intakes and its use in a five-country comparative study. Br. J. Nutr. 2001, 85, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Toh, D.W.K.; Loh, W.W.; Sutanto, C.N.; Yao, Y.; Kim, J.E. Skin carotenoid status and plasma carotenoids: Biomarkers of dietary carotenoids, fruits and vegetables for middle-aged and older Singaporean adults. Br. J. Nutr. 2021, 126, 1398–1407. [Google Scholar] [CrossRef] [PubMed]
- Kiani, A.K.; Dhuli, K.; Donato, K.; Aquilanti, B.; Velluti, V.; Matera, G.; Iaconelli, A.; Connelly, S.T.; Bellinato, F.; Gisondi, P.; et al. Main nutritional deficiencies. J. Prev. Med. Hyg. 2022, 63, E93–E101. [Google Scholar] [PubMed]
- Stephensen, C.B. Vitamin A, infection, and immune function. Annu. Rev. Nutr. 2001, 21, 167–192. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D. Vitamin A, immunity, and infection. Clin. Infect. Dis. 1994, 19, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Correia, L.L.; Rocha, H.A.L.; Campos, J.S.; Silva, A.C.E.; Silveira, D.; Machado, M.M.T.; Leite, A.J.M.; Cunha, A. Interaction between vitamin A supplementation and chronic malnutrition on child development. Cien. Saude. Colet. 2019, 24, 3037–3046. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, C. The eye signs of vitamin A deficiency. Community Eye Health 2013, 26, 66–67. [Google Scholar]
- West, K.P., Jr. Vitamin A deficiency disorders in children and women. Food Nutr. Bull. 2003, 24, S78–S90. [Google Scholar] [CrossRef]
- Latham, M.C. Human Nutrition in the Developing World; Food and Agriculture Organization of the United Nations: Rome, Italy, 1997. [Google Scholar]
- Division, N. Human Vitamin and Mineral Requirements; Report of a Joint FAO/WHO Expert Consultation: Bangkok, Thailand, 2002. [Google Scholar]
- National Institutes of Health (NIH) Office of Dietary Supplements (ODS). Vitamin A and Carotenoids. Available online: https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/ (accessed on 19 October 2023).
- U.S. Department of Agriculture, A.R.S. USDA Food and Nutrient Database for Dietary Studies, 5.0; Food Surveys Research Group Home Page: Beltsville, MD, USA, 2012.
- U.S. Department of Agriculture, A.R.S. USDA Food and Nutrient Database for Dietary Studies 2011–2012; Food Surveys Research Group Home Page: Beltsville, MD, USA, 2014.
- U.S. Department of Agriculture, A.R.S. USDA Food and Nutrient Database for Dietary Studies 2013–2014; Food Surveys Research Group Home Page: Beltsville, MD, USA, 2016.
- U.S. Department of Agriculture, A.R.S. USDA Food and Nutrient Database for Dietary Studies 2015–2016; Food Surveys Research Group Home Page: Beltsville, MD, USA, 2018.
- U.S. Department of Agriculture, A.R.S. USDA Food and Nutrient Database for Dietary Studies 2017–2018; Food Surveys Research Group Home Page: Beltsville, MD, USA, 2020.
- Haytowitz, D.B.; Ahuja, J.K.C.; Wu, X.; Somanchi, M.; Nickle, M.; Nguyen, Q.A.; Roseland, J.M.; Williams, J.R.; Patterson, K.Y.; Li, Y.; et al. USDA National Nutrient Database for Standard Reference, Legacy Release; Nutrient Data Laboratory, Beltsville Human Nutrition Research Center, ARS, USDA: Beltsville, MD, USA, 2019. [Google Scholar]
- Krauss, R.M.; Eckel, R.H.; Howard, B.; Appel, L.J.; Daniels, S.R.; Deckelbaum, R.J.; Erdman, J.W., Jr.; Kris-Etherton, P.; Goldberg, I.J.; Kotchen, T.A.; et al. Revision 2000: A statement for healthcare professionals from the Nutrition Committee of the American Heart Association. J. Nutr. 2001, 131, 132–146. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Cook, A.; Subar, A.F.; Cleveland, L.; Friday, J. US adults’ fruit and vegetable intakes, 1989 to 1991: A revised baseline for the Healthy People 2000 objective. Am. J. Public. Health 1995, 85, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Hoy, M.K.; Goldman, J.D.; Moshfegh, A.J. Differences in fruit and vegetable intake of U.S. adults by sociodemographic characteristics evaluated by two methods. J. Food Compos. Anal. 2017, 64, 97–103. [Google Scholar] [CrossRef]
- Subar, A.F.; Heimendinger, J.; Patterson, B.H.; Krebs-Smith, S.M.; Pivonka, E.; Kessler, R. Fruit and vegetable intake in the United States: The baseline survey of the Five A Day for Better Health Program. Am. J. Health Promot. 1995, 9, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Diet quality in Canada. Health Rep. 2009, 20, 41–52. [Google Scholar]
- Beydoun, M.A.; Wang, Y. How do socio-economic status, perceived economic barriers and nutritional benefits affect quality of dietary intake among US adults? Eur. J. Clin. Nutr. 2008, 62, 303–313. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press (US): Washington, DC, USA, 2000. [Google Scholar]
- Bohm, V.; Lietz, G.; Olmedilla-Alonso, B.; Phelan, D.; Reboul, E.; Banati, D.; Borel, P.; Corte-Real, J.; de Lera, A.R.; Desmarchelier, C.; et al. From carotenoid intake to carotenoid blood and tissue concentrations—Implications for dietary intake recommendations. Nutr. Rev. 2021, 79, 544–573. [Google Scholar] [CrossRef]
- Economic Research Service (ERS), U.S.D.o.A.U. Food Availability (Per Capita) Data System; Economic Research Service (ERS), U.S. Department of Agriculture (USDA): Washington, DC, USA, 2001. [Google Scholar]



{kind=link}
{kind=link}
| Subgroups | α-Carotene (mcg/Day) | β-Carotene (mcg/Day) | β-Cryptoxanthin (mcg/Day) | Lycopene (mcg/Day) | Lutein + Zeaxanthin (mcg/Day) | Total (mcg/Day) | |
|---|---|---|---|---|---|---|---|
| n | Mean (Median) | Mean (Median) | Mean (Median) | Mean (Median) | Mean (Median) | Mean (Median) | |
| All | 22,339 | 422.0 (83.6) | 2335.9 (1163.3) | 85.7 (40.5) | 5206.5 (2684.6) | 1636.9 (872.2) | 9687.1 (6821.4) |
| Gender | |||||||
| Men | 10,837 | 435.5 (74.7) | 2288.2 (1098.3) | 87.3 (41.9) | 6101.2 (3240.6) | 1599.4 (902.7) | 10,512.0 (7371.4) |
| Women | 11,502 | 409.0 (95.7) | 2381.9 (1258.8) | 84.2 (39.1) | 4344.5 (2249.8) | 1673.0 (850.1) | 8892.6 (6426.2) |
| p-value 1 | 0.1734 | 0.1927 | 0.2835 | <0.0001 | 0.1080 | <0.0001 | |
| Age, y | |||||||
| 19–30 | 4263 | 348.2 (47.9) | 1824.8 (763.6) | 68.6 (31.8) | 5456.8 (3031.0) | 1374.8 (714.2) | 9073.1 (6266.5) |
| 31–50 | 7221 | 420.1 (71.6) | 2342.8 (1070.0) | 83.0 (39.3) | 5520.7 (3020.3) | 1705.1 (860.9) | 10,072.0 (6915.7) |
| 51–70 | 7518 | 460.9 (116.0) | 2564.7 (1403.3) | 95.2 (44.5) | 5021.3 (2492.7) | 1744.9 (964.7) | 9887.1 (7205.9) |
| 70+ | 3337 | 451.5 (154.3) | 2596.6 (1510.9) | 98.4 (49.3) | 4325.0 (1859.6) | 1600.7 (955.7) | 9072.2 (6491.5) |
| p-value 1 | <0.001 | <0.0001 | <0.0001 | <0.0001 | <0.01 | 0.5283 | |
| Men, y | |||||||
| 19–30 | 2136 | 360.7 (43.9) | 1788.6 (735.6) | 72.6 (33.0) | 6396.4 (3617.0) | 1327.1 (710.9) | 9945.3 (6514.8) |
| 31–50 | 3430 | 453.4 (68.6) | 2362.4 (1079.6) | 86.7 (41.7) | 6534.2 (3637.5) | 1689.5 (900.0) | 11,126.0 (7681.9) |
| 51–70 | 3636 | 468.8 (106.5) | 2512.3 (1295.0) | 94.7 (47.2) | 5711.2 (2845.9) | 1686.8 (1011.3) | 10,474.0 (7736.5) |
| 70+ | 1635 | 433.8 (148.8) | 2431.5 (1412.0) | 98.9 (48.8) | 5179.2 (2242.9) | 1615.8 (984.7) | 9759.3 (6787.9) |
| p-value 1 | 0.0684 | <0.0001 | <0.001 | <0.001 | <0.01 | 0.8164 | |
| Women, y | |||||||
| 19–30 | 2127 | 334.3 (52.0) | 1865.1 (791.5) | 64.2 (29.9) | 4411.2 (2483.5) | 1427.8 (714.4) | 8102.6 (6015.0) |
| 31–50 | 3791 | 387.0 (76.8) | 2323.4 (1069.1) | 79.3 (36.7) | 4516.8 (2448.2) | 1720.6 (826.5) | 9027.0 (6451.9) |
| 51–70 | 3882 | 453.7 (129.6) | 2613.3 (1494.6) | 95.6 (43.1) | 4381.7 (2145.5) | 1798.8 (918.0) | 9343.1 (6656.4) |
| 70+ | 1702 | 464.9 (158.4) | 2721.7 (1607.9) | 98.1 (50.2) | 3677.9 (1694.5) | 1589.2 (923.2) | 8551.8 (6095.1) |
| p-value 1 | <0.0001 | <0.0001 | <0.0001 | <0.05 | <0.05 | <0.05 | |
| Ethnicity | |||||||
| White | 9234 | 434.7 (86.9) | 2385.0 (1235.6) | 78.5 (38.7) | 5358.9 (2811.2) | 1640.4 (890.7) | 9897.5 (7147.6) |
| Black | 4914 | 290.3 (47.9) | 2053.6 (761.7) | 73.4 (35.6) | 4211.1 (1784.5) | 1682.6 (763.1) | 8310.9 (5078.6) |
| Mexican-American | 3161 | 379.0 (79.8) | 1905.5 (968.0) | 108.6 (57.8) | 5688.5 (3460.8) | 1271.2 (819.3) | 9352.9 (6681.3) |
| Others | 5030 | 495.6 (134.5) | 2599.9 (1401.2) | 115.2 (44.2) | 5006.5 (2409.0) | 1808.3 (942.0) | 10,026.0 (7017.9) |
| p-value 1 | 0.3835 | 0.8971 | <0.0001 | 0.1626 | 0.6419 | 0.5060 | |
| BMI 2 | |||||||
| BMI <18.5 | 587 | 528.0 (84.8) | 2421.6 (1034.3) | 70.8 (31.3) | 4645.4 (2345.1) | 1533.4 (751.6) | 9199.2 (6479.3) |
| 18.5 ≤ BMI < 25 | 5873 | 463.3 (96.4) | 2618.8 (1303.7) | 91.0 (40.2) | 5542.5 (2664.0) | 1873.1 (942.8) | 10,589.0 (7419.3) |
| 25 ≤ BMI < 30 | 7106 | 439.4 (95.2) | 2446.3 (1275.0) | 88.6 (42.6) | 5152.5 (2769.0) | 1719.6 (912.6) | 9846.4 (7174.6) |
| 30 ≤ BMI | 8773 | 371.5 (70.3) | 2035.9 (1016.3) | 80.4 (39.4) | 5043.9 (2605.1) | 1404.7 (818.0) | 8936.5 (6305.8) |
| p-value 1 | <0.001 | <0.0001 | <0.05 | 0.1554 | <0.0001 | <0.0001 | |
| PIR 3 | |||||||
| <1.3 | 6542 | 331.0 (51.9) | 1786.7 (737.8) | 78.1 (33.8) | 4895.5 (2491.6) | 1307.7 (681.7) | 8399.0 (5561.2) |
| 1.3–1.85 | 2712 | 360.7 (66.0) | 2064.8 (947.5) | 84.6 (39.8) | 4665.8 (2415.1) | 1402.5 (791.5) | 8578.4 (6010.2) |
| ≥1.85 | 11,158 | 458.7 (104.6) | 2560.9 (1387.7) | 87.0 (42.4) | 5468.3 (2844.8) | 1799.8 (978.7) | 10,375.0 (7556.7) |
| p-value 1 | <0.0001 | <0.0001 | <0.05 | <0.01 | <0.0001 | <0.0001 | |
| Alcohol consumption 4 | |||||||
| No | 7958 | 442.0 (88.1) | 2236.8 (1061.5) | 90.3 (40.0) | 4514.5 (2336.7) | 1398.6 (810.5) | 8682.1 (6052.6) |
| Moderate | 7266 | 469.4 (107.6) | 2678.5 (1465.2) | 94.0 (44.6) | 5589.5 (2761.4) | 1887.6 (1029.2) | 10,719.0 (7655.1) |
| Heavy | 7115 | 358.9 (63.2) | 2078.0 (973.6) | 73.9 (36.5) | 5391.6 (2932.0) | 1583.2 (812.3) | 9485.6 (6748.4) |
| p-value 1 | <0.001 | <0.05 | <0.0001 | <0.001 | <0.05 | <0.05 | |
| Smoking 5 | |||||||
| Never | 12,474 | 456.8 (97.7) | 2539.2 (1309.8) | 92.1 (42.8) | 5360.5 (2771.3) | 1734.6 (914.5) | 10,183.0 (7200.4) |
| Former | 5353 | 462.9 (111.0) | 2523.4 (1403.6) | 89.7 (45.7) | 5119.1 (2709.9) | 1750.2 (987.3) | 9945.3 (7397.7) |
| Current | 3391 | 256.2 (38.4) | 1399.9 (607.7) | 58.3 (27.1) | 4590.4 (2208.4) | 1085.6 (602.4) | 7390.4 (4907.9) |
| p-value 1 | <0.0001 | <0.0001 | <0.0001 | <0.01 | <0.0001 | <0.0001 | |
| Physical activity 6 | |||||||
| Light activity | 8966 | 353.7 (67.0) | 1897.6 (918.7) | 76.1 (35.5) | 4814.1 (2417.0) | 1291.6 (741.4) | 8433.0 (5854.8) |
| Moderate activity | 3467 | 386.5 (83.9) | 2185.4 (1154.4) | 87.0 (38.1) | 5244.1 (2757.9) | 1470.6 (855.3) | 9373.6 (6950.4) |
| Vigorous activity | 9883 | 485.7 (99.5) | 2717.9 (1377.3) | 92.7 (45.1) | 5493.8 (2888.1) | 1952.3 (1005.5) | 10,742.0 (7610.7) |
| p-value 1 | <0.0001 | <0.0001 | <0.0001 | <0.001 | <0.0001 | <0.0001 | |
| Supplement use | |||||||
| No | 11,692 | 350.8 (58.6) | 1920.7 (880.5) | 75.0 (34.0) | 5255.6 (2757.4) | 1381.7 (754.5) | 8984.0 (6232.9) |
| Yes | 10,647 | 492.3 (121.1) | 2745.4 (1507.1) | 96.3 (47.5) | 5158.1 (2605.6) | 1888.5 (1016.0) | 10,381.0 (7486.0) |
| p-value 1 | <0.0001 | <0.0001 | <0.0001 | 0.5813 | <0.0001 | <0.0001 |
| Subgroups | Vitamin A Adequacy Rate | |||||
|---|---|---|---|---|---|---|
| 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 | ||
| n, % | n, % | n, % | n, % | n, % | p-Trend 1 | |
| All | 1243, 27.8% | 1049, 27.1% | 1123, 27.7% | 935, 25.3% | 988, 25.5% | <0.0001 |
| Gender | ||||||
| Men | 521, 24.0% | 444, 25.7% | 463, 24.5% | 407, 22.8% | 422, 21.9% | <0.0001 |
| Women | 722, 31.4% | 605, 28.6% | 660, 30.8% | 528, 27.8% | 566, 29.0% | <0.0001 |
| p-value | <0.001 | 0.2042 | <0.001 | <0.01 | <0.01 | |
| Age, y | ||||||
| 19–30 | 208, 23.5% | 197, 24.0% | 198, 24.3% | 154, 23.0% | 151, 21.1% | <0.0001 |
| 31–50 | 402, 26.4% | 319, 24.3% | 367, 25.1% | 303, 26.3% | 295, 26.2% | <0.0001 |
| 51–70 | 394, 30.7% | 368, 31.3% | 379, 30.4% | 300, 24.0% | 354, 23.9% | <0.0001 |
| 70+ | 239, 32.2% | 165, 30.1% | 179, 34.4% | 178, 29.9% | 188, 35.9% | <0.0001 |
| p-value | <0.01 | <0.05 | <0.01 | 0.1154 | <0.01 | |
| Ethnicity | ||||||
| White | 768, 31.7% | 495, 30.9% | 575, 30.7% | 391, 28.3% | 426, 27.5% | <0.0001 |
| Black | 181, 20.9% | 238, 20.3% | 179, 19.1% | 175, 17.6% | 210, 19.6% | <0.0001 |
| Mexican-American | 151, 16.0% | 75, 18.1% | 131, 21.7% | 124, 20.9% | 102, 21.7% | <0.0001 |
| Others | 143, 20.0% | 241, 19.8% | 238, 24.7% | 245, 21.0% | 250, 24.3% | <0.0001 |
| p-value | <0.0001 | <0.0001 | <0.0001 | <0.05 | <0.0001 | |
| PIR 2 | ||||||
| <1.3 | 314, 22.1% | 304, 22.9% | 289, 22.2% | 220, 20.8% | 213, 17.7% | <0.0001 |
| 1.3–1.85 | 127, 21.3% | 113, 23.5% | 115, 26.3% | 127, 27.7% | 127, 22.8% | <0.0001 |
| ≥1.85 | 705, 30.9% | 556, 30.0% | 633, 29.7% | 505, 26.2% | 541, 28.4% | <0.0001 |
| p-value | <0.01 | <0.001 | <0.01 | <0.05 | <0.0001 | |
| Subgroups | Provitamin A (mcg RAE/Day) | Retinol (mcg RAE/Day) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | 2017–2018 | |||
| Mean (SE) | Mean (SE) | Mean (SE) | Mean (SE) | Mean (SE) | p-Trend | Mean (SE) | Mean (SE) | Mean (SE) | Mean (SE) | Mean (SE) | p-Trend | |
| All | 213.8 (4.9) | 227.5 (14.0) | 220.0 (7.8) | 202.4 (9.2) | 215.7 (11.3) | 0.3991 | 451.1 (10.4) | 436.7 (13.9) | 430.2 (9.8) | 434.1 (12.5) | 418.7 (8.5) | 0.0304 |
| Gender | ||||||||||||
| Men | 216.2 (10.7) | 232.7 (20.3) | 210.1 (6.4) | 204.4 (13.4) | 200.0 (13.1) | 0.1404 | 495.0 (12.5) | 502.0 (23.4) | 482.1 (13.4) | 476.4 (18.8) | 454.6 (9.5) | 0.012 |
| Women | 211.5 (7.3) | 222.5 (14.7) | 229.4 (12.5) | 200.5 (6.4) | 230.5 (11.7) | 0.7579 | 409.0 (11.6) | 373.9 (11.5) | 380.5 (12.2) | 392.2 (11.1) | 384.5 (14.0) | 0.4077 |
| p-value | 0.7635 | 0.6368 | 0.1240 | 0.6971 | <0.01 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.001 | ||
| Age, y | ||||||||||||
| 19–30 | 159.0 (8.8) | 169.0 (13.2) | 172.6 (12.0) | 176.9 (19.5) | 169.1 (17.9) | 0.5552 | 452.8 (19.8) | 420.8 (19.2) | 436.1 (16.4) | 431.0 (22.0) | 426.5 (16.3) | 0.4088 |
| 31–50 | 212.5 (11.6) | 212.9 (13.2) | 229.4 (15.0) | 194.8 (12.2) | 232.4 (20.7) | 0.676 | 442.1 (20.1) | 416.7 (14.3) | 402.0 (13.7) | 434.3 (21.0) | 413.6 (14.8) | 0.4867 |
| 51–70 | 242.9 (6.8) | 283.9 (31.5) | 234.4 (8.2) | 213.2 (11.8) | 214.5 (15.8) | 0.0119 | 457.0 (10.6) | 455.1 (39.9) | 429.5 (14.0) | 402.2 (12.8) | 392.8 (16.4) | 0.0032 |
| 70+ | 242.4 (17.1) | 222.3 (12.9) | 240.8 (29.0) | 236.1 (12.7) | 252.5 (22.9) | 0.5351 | 462.2 (17.5) | 480.5 (26.1) | 509.1 (16.7) | 521.0 (60.7) | 492.8 (22.2) | 0.3228 |
| p-value | <0.0001 | <0.001 | <0.01 | <0.01 | <0.05 | 0.6101 | 0.0963 | <0.05 | 0.4044 | 0.3315 | ||
| Ethnicity | ||||||||||||
| White | 224.8 (8.5) | 242.2 (18.4) | 220.1 (10.1) | 200.1 (11.0) | 213.5 (13.0) | 0.0754 | 480.1 (8.4) | 475.2 (17.5) | 460.4 (11.8) | 471.7 (16.1) | 443.5 (9.6) | 0.0243 |
| Black | 173.1 (11.9) | 190.2 (22.7) | 178.4 (11.2) | 187.9 (12.9) | 200.5 (19.1) | 0.3179 | 426.5 (51.0) | 357.0 (15.6) | 359.8 (14.1) | 312.7 (10.2) | 353.4 (13.3) | 0.0717 |
| Mexican-American | 170.7 (10.4) | 152.3 (16.4) | 188.4 (12.4) | 176.3 (16.6) | 203.9 (28.0) | 0.2083 | 366.2 (21.4) | 407.0 (20.3) | 406.8 (20.2) | 424.4 (23.2) | 434.0 (39.3) | 0.0889 |
| Others | 220.9 (19.8) | 232.9 (17.8) | 275.8 (23.5) | 237.9 (16.8) | 239.8 (12.1) | 0.7807 | 365.5 (11.9) | 332.3 (6.2) | 361.2 (17.9) | 365.9 (15.0) | 363.9 (11.3) | 0.2771 |
| p-value | 0.2398 | 0.1300 | 0.2205 | 0.1874 | 0.1493 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||
| PIR 1 | ||||||||||||
| <1.3 | 162.5 (5.9) | 160.4 (13.3) | 165.8 (12.6) | 185.6 (13.1) | 156.9 (12.5) | 0.8119 | 426.1 (25.1) | 400.5 (17.4) | 399.3 (15.5) | 387.1 (24.3) | 402.0 (19.2) | 0.4528 |
| 1.3–1.85 | 187.8 (12.6) | 174.3 (13.5) | 231.6 (23.3) | 179.0 (19.7) | 180.1 (16.6) | 0.7502 | 428.7 (27.9) | 451.0 (29.5) | 448.4 (40.9) | 418.1 (21.3) | 445.2 (36.5) | 0.9143 |
| ≥1.85 | 230.9 (6.5) | 266.5 (18.8) | 236.5 (9.9) | 208.9 (10.8) | 239.5 (12.6) | 0.2744 | 463.6 (10.7) | 454.5 (18.8) | 439.3 (12.1) | 439.2 (15.4) | 426.2 (10.5) | 0.018 |
| p-value | <0.0001 | <0.0001 | <0.0001 | <0.05 | <0.0001 | 0.1764 | 0.0570 | <0.05 | <0.05 | 0.2362 | ||
| Carotenoids | 2009–2010 (n = 5084) | 2017–2018 (n = 4160) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | Food Group | Average Intake (mcg/Day) | Contribution | Cumulative Contribution | Food Group | Average Intake (mcg/Day) | Contribution | Cumulative Contribution | |
| α-carotene | 1 | Carrot | 301.7 | 71.5% | 71.5% | Carrot | 261.1 | 61.9% | 61.9% |
| 2 | Carrot juice | 27.6 | 6.5% | 78.0% | Tomatoes | 15.1 | 3.6% | 65.5% | |
| 3 | Mixed vegetables 1 | 20.3 | 4.8% | 82.9% | Carrot juice | 14.7 | 3.5% | 68.9% | |
| 4 | Tomatoes | 20.1 | 4.8% | 87.6% | Mixed vegetables 1 | 9.1 | 2.1% | 71.1% | |
| 5 | Pumpkin | 7.0 | 1.7% | 89.3% | Pumpkin | 6.6 | 1.6% | 72.7% | |
| 6 | Bananas | 5.9 | 1.4% | 90.7% | Bananas | 5.8 | 1.4% | 74.0% | |
| 7 | Squash | 5.1 | 1.2% | 91.9% | Beans 2 | 5.7 | 1.3% | 75.4% | |
| 8 | Beans 2 | 4.6 | 1.1% | 93.0% | Squash | 4.3 | 1.0% | 76.4% | |
| 9 | Vegetable/meat (or seafood) soup | 3.8 | 0.9% | 93.9% | Plantains | 4.1 | 1.0% | 77.4% | |
| 10 | Vegetable juice cocktail | 3.5 | 0.8% | 94.7% | Tangerines | 3.9 | 0.9% | 78.3% | |
| β-carotene | 1 | Carrot | 699.9 | 30.0% | 30.0% | Carrot | 607.9 | 26.0% | 26.0% |
| 2 | Sweet potato | 213.3 | 9.1% | 39.1% | Lettuce | 322.4 | 13.8% | 39.8% | |
| 3 | Spinach | 177.4 | 7.6% | 46.7% | Sweet potato | 298.7 | 12.8% | 52.6% | |
| 4 | Lettuce | 140.8 | 6.0% | 52.7% | Spinach | 275.2 | 11.8% | 64.4% | |
| 5 | Tomatoes | 102.8 | 4.4% | 57.1% | Tomatoes | 75.8 | 3.2% | 67.6% | |
| 6 | Melons | 82.5 | 3.5% | 60.7% | Melons | 63.4 | 2.7% | 70.4% | |
| 7 | Carrot juice | 59.2 | 2.5% | 63.2% | Tomato products 3 | 48.3 | 2.1% | 72.4% | |
| 8 | Broccoli | 56.6 | 2.4% | 65.6% | Broccoli | 35.3 | 1.5% | 73.9% | |
| 9 | Tomato products 3 | 49.2 | 2.1% | 67.7% | Pepper 4 | 32.7 | 1.4% | 75.3% | |
| 10 | Mixed vegetables | 43.7 | 1.9% | 69.6% | Kale | 32.1 | 1.4% | 76.7% | |
| β-cryptoxanthin | 1 | Orange juice | 14.5 | 17.0% | 17.0% | Tangerines | 15.5 | 18.1% | 18.1% |
| 2 | Tangerines | 8.1 | 9.4% | 26.4% | Orange juice | 9.4 | 10.9% | 29.0% | |
| 3 | Oranges | 7.8 | 9.1% | 35.4% | Oranges | 8.8 | 10.2% | 39.2% | |
| 4 | Corn | 7.5 | 8.8% | 44.2% | Pepper 3 | 7.5 | 8.7% | 47.9% | |
| 5 | Watermelon | 6.3 | 7.4% | 51.6% | Watermelon | 6.3 | 7.4% | 55.3% | |
| 6 | Persimmons | 5.7 | 6.7% | 58.3% | Chili | 5.0 | 5.8% | 61.1% | |
| 7 | Pepper 4 | 5.0 | 5.8% | 64.1% | Corn | 4.0 | 4.7% | 65.8% | |
| 8 | Peaches | 4.6 | 5.3% | 69.4% | Carrot | 3.2 | 3.8% | 69.5% | |
| 9 | Pickles 5 | 3.5 | 4.0% | 73.5% | Papaya | 2.8 | 3.3% | 72.8% | |
| 10 | Chili | 3.4 | 3.9% | 77.4% | Egg | 2.7 | 3.2% | 76.0% | |
| Lycopene | 1 | Tomato products 3 | 1971.8 | 37.9% | 37.9% | Tomato products 3 | 1971.8 | 37.9% | 37.9% |
| 2 | Tomatoes | 677.9 | 13.0% | 50.9% | Tomatoes | 482.7 | 9.3% | 47.1% | |
| 3 | Pizza | 501.2 | 9.6% | 60.5% | Salsa | 456.6 | 8.8% | 55.9% | |
| 4 | Watermelon | 367.3 | 7.1% | 67.6% | Pizza | 424.8 | 8.2% | 64.1% | |
| 5 | Catsup | 348.2 | 6.7% | 74.3% | Watermelon | 366.4 | 7.0% | 71.1% | |
| 6 | Vegetable juice cocktail | 269.5 | 5.2% | 79.4% | Catsup | 320.5 | 6.2% | 77.3% | |
| 7 | Salsa | 257.0 | 4.9% | 84.4% | Tomato Soup | 166.8 | 3.2% | 80.5% | |
| 8 | Tomato Soup | 140.7 | 2.7% | 87.1% | Other sauce 6 | 161.3 | 3.1% | 83.6% | |
| 9 | Other sauce 6 | 127.0 | 2.4% | 89.5% | Tomato juice | 100.4 | 1.9% | 85.5% | |
| 10 | Tomato juice | 120.9 | 2.3% | 91.8% | Pasta 7 | 86.6 | 1.7% | 87.2% | |
| Lutein + zeaxanthin | 1 | Spinach | 358.4 | 21.9% | 21.9% | Spinach | 592.4 | 36.2% | 36.2% |
| 2 | Egg | 102.1 | 6.2% | 28.1% | Egg | 148.9 | 9.1% | 45.3% | |
| 3 | Lettuce | 84.3 | 5.1% | 33.3% | Lettuce | 134.6 | 8.2% | 53.5% | |
| 4 | Broccoli | 83.2 | 5.1% | 38.4% | Broccoli | 100.4 | 6.1% | 59.6% | |
| 5 | Squash | 74.4 | 4.5% | 42.9% | Squash | 46.8 | 2.9% | 62.5% | |
| 6 | Chicory greens | 62.7 | 3.8% | 46.7% | Kale | 44.5 | 2.7% | 65.2% | |
| 7 | Corn | 60.4 | 3.7% | 50.4% | Corn | 40.5 | 2.5% | 67.7% | |
| 8 | Collards | 52.4 | 3.2% | 53.6% | Beans 2 | 33.2 | 2.0% | 69.7% | |
| 9 | Kale | 41.1 | 2.5% | 56.1% | Carrot | 27.3 | 1.7% | 71.4% | |
| 10 | Beans 2 | 38.7 | 2.4% | 58.5% | Cereals 8 | 27.1 | 1.7% | 73.0% | |
| Total | 1 | Tomato products 3 | 2039.0 | 21.0% | 21.0% | Tomato products 3 | 2003.9 | 20.7% | 20.7% |
| 2 | Carrot | 1035.7 | 10.7% | 31.7% | Carrot | 899.6 | 9.3% | 30.0% | |
| 3 | Tomatoes | 830.4 | 8.6% | 40.3% | Spinach | 867.6 | 9.0% | 38.9% | |
| 4 | Spinach | 535.9 | 5.5% | 45.8% | Tomatoes | 595.0 | 6.1% | 45.1% | |
| 5 | Pizza | 534.1 | 5.5% | 51.4% | Salsa | 497.0 | 5.1% | 50.2% | |
| 6 | Watermelon | 398.8 | 4.1% | 55.5% | Lettuce | 457.2 | 4.7% | 54.9% | |
| 7 | Catsup | 361.9 | 3.7% | 59.2% | Pizza | 452.7 | 4.7% | 59.6% | |
| 8 | Vegetable juice cocktail | 297.8 | 3.1% | 62.3% | Watermelon | 397.8 | 4.1% | 63.7% | |
| 9 | Salsa | 279.6 | 2.9% | 65.2% | Catsup | 333.2 | 3.4% | 67.1% | |
| 10 | Lettuce | 225.7 | 2.3% | 67.5% | Sweet potato | 299.4 | 3.1% | 70.2% | |
| 11 | Sweet potato | 213.8 | 2.2% | 69.7% | Tomato Soup | 171.8 | 1.8% | 72.0% | |
| 12 | Tomato Soup | 144.7 | 1.5% | 71.2% | Other sauce 6 | 171.1 | 1.8% | 73.8% | |
| 13 | Broccoli | 140.5 | 1.4% | 72.7% | Egg | 151.8 | 1.6% | 75.3% | |
| 14 | Other sauce 6 | 134.6 | 1.4% | 74.0% | Broccoli | 137.6 | 1.4% | 76.8% | |
| 15 | Tomato juice | 125.3 | 1.3% | 75.3% | Pasta 7 | 104.2 | 1.1% | 77.8% | |
| 16 | Squash | 105.8 | 1.1% | 76.4% | Tomato juice | 104.0 | 1.1% | 78.9% | |
| 17 | Egg | 104.8 | 1.1% | 77.5% | Vegetable juice cocktail | 84.2 | 0.9% | 79.8% | |
| 18 | Collards | 89.9 | 0.9% | 78.4% | Chili | 79.3 | 0.8% | 80.6% | |
| 19 | Carrot juice | 88.9 | 0.9% | 79.4% | Kale | 77.3 | 0.8% | 81.4% | |
| 20 | Melons | 84.5 | 0.9% | 80.2% | Squash | 72.0 | 0.7% | 82.1% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Madore, M.P.; Chun, O.K. Changes in Intake and Major Food Sources of Carotenoids among U.S. Adults between 2009–2018. Metabolites 2024, 14, 13. https://doi.org/10.3390/metabo14010013
Kim K, Madore MP, Chun OK. Changes in Intake and Major Food Sources of Carotenoids among U.S. Adults between 2009–2018. Metabolites. 2024; 14(1):13. https://doi.org/10.3390/metabo14010013
Chicago/Turabian StyleKim, Kijoon, Matthew P. Madore, and Ock K. Chun. 2024. "Changes in Intake and Major Food Sources of Carotenoids among U.S. Adults between 2009–2018" Metabolites 14, no. 1: 13. https://doi.org/10.3390/metabo14010013
APA StyleKim, K., Madore, M. P., & Chun, O. K. (2024). Changes in Intake and Major Food Sources of Carotenoids among U.S. Adults between 2009–2018. Metabolites, 14(1), 13. https://doi.org/10.3390/metabo14010013