
Dietary Inflammatory and Insulinemic Potentials, Plasma Metabolome and Risk of Colorectal Cancer
 , ,
, ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
1. Introduction
2. Methods
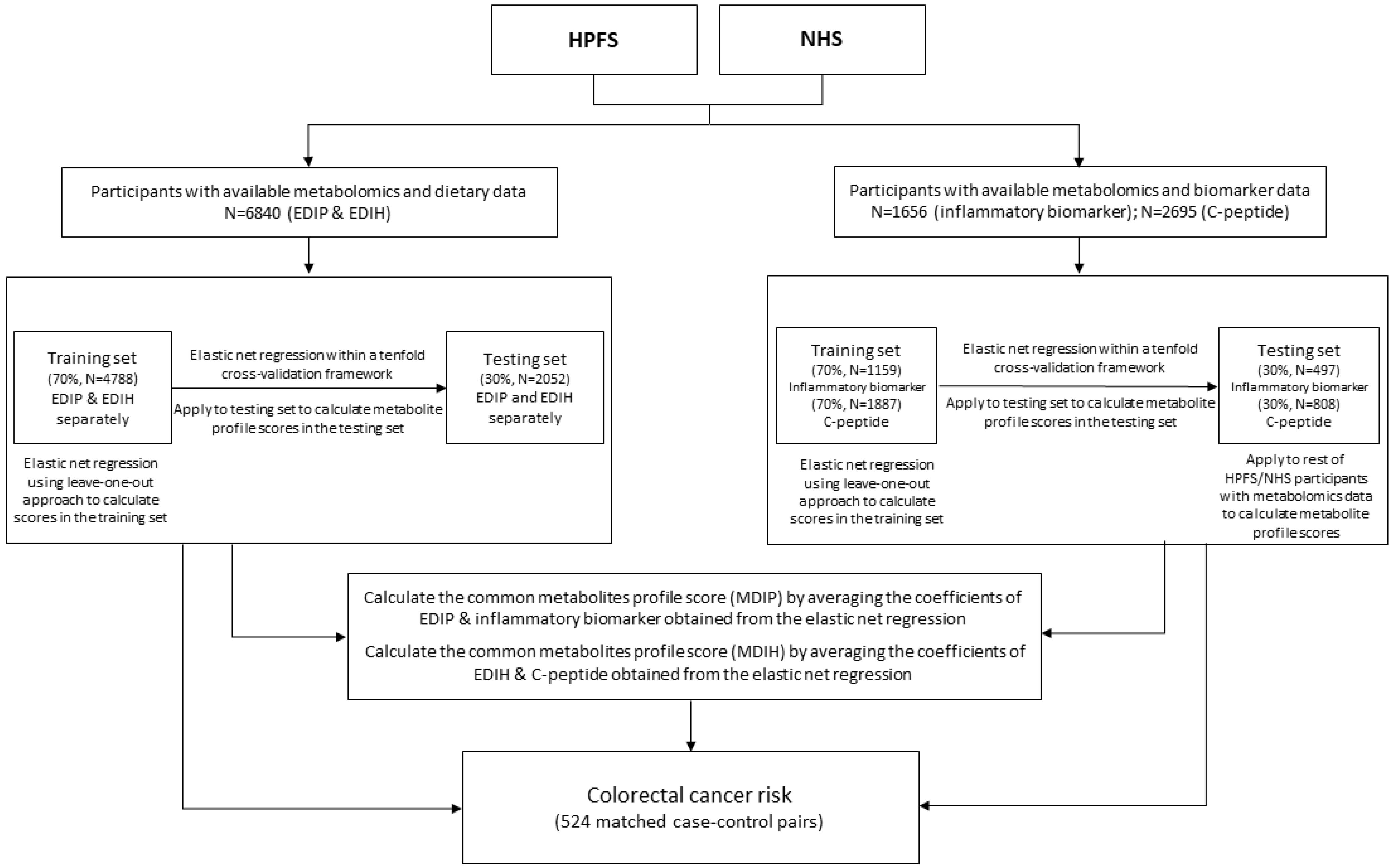
2.1. Study Design and Population
2.2. Dietary Assessment
2.3. Covariate Assessment
2.4. Plasma Inflammatory Biomarker Assessment and Metabolomics Profiling
2.5. Colorectal Cancer Assessment
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics and Identification of Metabolomic Signatures
3.2. Association between Metabolomic Profile Scores and Colorectal Cancer Risk
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA A Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Harmon, B.E.; Boushey, C.J.; Shvetsov, Y.B.; Ettienne, R.; Reedy, J.; Wilkens, L.R.; Le Marchand, L.; Henderson, B.E.; Kolonel, L.N. Associations of key diet-quality indexes with mortality in the Multiethnic Cohort: The Dietary Patterns Methods Project. Am. J. Clin. Nutr. 2015, 101, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Liese, A.D.; Krebs-Smith, S.M.; Subar, A.F.; George, S.M.; Harmon, B.E.; Neuhouser, M.L.; Boushey, C.J.; Schap, T.E.; Reedy, J. The Dietary Patterns Methods Project: Synthesis of findings across cohorts and relevance to dietary guidance. J. Nutr. 2015, 145, 393–402. [Google Scholar] [CrossRef]
- Wang, P.; Song, M.; Eliassen, A.H.; Wang, M.; Fung, T.T.; Clinton, S.K.; Rimm, E.B.; Hu, F.B.; Willett, W.C.; Tabung, F.K. Optimal dietary patterns for prevention of chronic disease. Nat. Med. 2023, 29, 719–728. [Google Scholar] [CrossRef]
- Fung, T.T.; Brown, L.S. Dietary patterns and the risk of colorectal cancer. Curr. Nutr. Rep. 2013, 2, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Brown, L.S.; Fung, T.T. Dietary Patterns and Colorectal Cancer Risk: A Review of 17 Years of Evidence (2000–2016). Curr. Color. Cancer Rep. 2017, 13, 440–454. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Giovannucci, E.L.; Giulianini, F.; Liang, L.; Chandler, P.D.; Balasubramanian, R.; Manson, J.E.; Cespedes Feliciano, E.M.; Hayden, K.M.; Van Horn, L. An empirical dietary inflammatory pattern score is associated with circulating inflammatory biomarkers in a multi-ethnic population of postmenopausal women in the United States. J. Nutr. 2018, 148, 771–780. [Google Scholar] [CrossRef]
- Tabung, F.K.; Smith-Warner, S.A.; Chavarro, J.E.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Giovannucci, E.L. An empirical dietary inflammatory pattern score enhances prediction of circulating inflammatory biomarkers in adults. J. Nutr. 2017, 147, 1567–1577. [Google Scholar] [CrossRef]
- Tabung, F.K.; Smith-Warner, S.A.; Chavarro, J.E.; Wu, K.; Fuchs, C.S.; Hu, F.B.; Chan, A.T.; Willett, W.C.; Giovannucci, E.L. Development and validation of an empirical Dietary Inflammatory Index. J. Nutr. 2016, 146, 1560–1570. [Google Scholar] [CrossRef]
- Tabung, F.K.; Wang, W.; Fung, T.T.; Hu, F.B.; Smith-Warner, S.A.; Chavarro, J.E.; Fuchs, C.S.; Willett, W.C.; Giovannucci, E.L. Development and validation of empirical indices to assess the insulinaemic potential of diet and lifestyle. Br. J. Nutr. 2016, 116, 1787–1798. [Google Scholar] [CrossRef]
- Tabung, F.K.; Liu, L.; Wang, W.; Fung, T.T.; Wu, K.; Smith-Warner, S.A.; Cao, Y.; Hu, F.B.; Ogino, S.; Fuchs, C.S.; et al. Association of dietary inflammatory potential with colorectal cancer risk in men and women. JAMA Oncol. 2018, 4, 366–373. [Google Scholar] [CrossRef]
- Liu, L.; Nishihara, R.; Qian, Z.R.; Tabung, F.K.; Nevo, D.; Zhang, X.; Song, M.; Cao, Y.; Mima, K.; Masugi, Y.; et al. Association Between Inflammatory Diet Pattern and Risk of Colorectal Carcinoma Subtypes Classified by Immune Responses to Tumor. Gastroenterology 2017, 156, 1517–1530.e1514. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Tabung, F.K.; Zhang, X.; Nowak, J.A.; Qian, Z.R.; Hamada, T.; Nevo, D.; Bullman, S.; Mima, K.; Kosumi, K.; et al. Diets That Promote Colon Inflammation Associate With Risk of Colorectal Carcinomas That Contain Fusobacterium nucleatum. Clin. Gastroenterol. Hepatol. 2018, 16, 1622–1631. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Wang, W.; Fung, T.T.; Smith-Warner, S.A.; Keum, N.; Wu, K.; Fuchs, C.S.; Hu, F.B.; Giovannucci, E.L. Association of dietary insulinemic potential and colorectal cancer risk in men and women. Am. J. Clin. Nutr. 2018, 108, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, L.; Wang, Y.; Li, P.; Luo, L.; Yang, B.; Wang, H.; Chen, M. Circulating C-peptide level is a predictive factor for colorectal neoplasia: Evidence from the meta-analysis of prospective studies. Cancer Causes Control. CCC 2013, 24, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.; Song, M.; Papadimitriou, N.; Carreras-Torres, R.; Langenberg, C.; Martin, R.M.; Tsilidis, K.K.; Barroso, I.; Chen, J.; Frayling, T.M.; et al. Associations Between Glycemic Traits and Colorectal Cancer: A Mendelian Randomization Analysis. J. Natl. Cancer Inst. 2022, 114, 740–752. [Google Scholar] [CrossRef]
- Kakourou, A.; Koutsioumpa, C.; Lopez, D.S.; Hoffman-Bolton, J.; Bradwin, G.; Rifai, N.; Helzlsouer, K.J.; Platz, E.A.; Tsilidis, K.K. Interleukin-6 and risk of colorectal cancer: Results from the CLUE II cohort and a meta-analysis of prospective studies. Cancer Causes Control. CCC 2015, 26, 1449–1460. [Google Scholar] [CrossRef]
- Tsilidis, K.K.; Branchini, C.; Guallar, E.; Helzlsouer, K.J.; Erlinger, T.P.; Platz, E.A. C-reactive protein and colorectal cancer risk: A systematic review of prospective studies. Int. J. Cancer 2008, 123, 1133–1140. [Google Scholar] [CrossRef]
- Zhou, B.; Shu, B.; Yang, J.; Liu, J.; Xi, T.; Xing, Y. C-reactive protein, interleukin-6 and the risk of colorectal cancer: A meta-analysis. Cancer Causes Control. CCC 2014, 25, 1397–1405. [Google Scholar] [CrossRef]
- Tian, G.; Mi, J.; Wei, X.; Zhao, D.; Qiao, L.; Yang, C.; Li, X.; Zhang, S.; Li, X.; Wang, B. Circulating interleukin-6 and cancer: A meta-analysis using Mendelian randomization. Sci. Rep. 2015, 5, 11394. [Google Scholar] [CrossRef]
- Wang, X.; Dai, J.Y.; Albanes, D.; Arndt, V.; Berndt, S.I.; Bézieau, S.; Brenner, H.; Buchanan, D.D.; Butterbach, K.; Caan, B.; et al. Mendelian randomization analysis of C-reactive protein on colorectal cancer risk. Int. J. Epidemiol. 2019, 48, 767–780. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferre, M.; Bhupathiraju, S.N.; Hu, F.B. Use of metabolomics in improving assessment of dietary intake. Clin. Chem. 2018, 64, 82–98. [Google Scholar] [CrossRef] [PubMed]
- Brennan, L.; Hu, F.B. Metabolomics-Based Dietary Biomarkers in Nutritional Epidemiology—Current Status and Future Opportunities. Mol. Nutr. Food Res. 2019, 63, 1701064. [Google Scholar] [CrossRef]
- Johnson, C.H.; Ivanisevic, J.; Siuzdak, G. Metabolomics: Beyond biomarkers and towards mechanisms. Nat. Rev. Mol. Cell Biol. 2016, 17, 451. [Google Scholar] [CrossRef]
- Colditz, G.A.; Manson, J.E.; Hankinson, S.E. The Nurses’ Health Study: 20-year contribution to the understanding of health among women. J. Women’s Health 1997, 6, 49–62. [Google Scholar] [CrossRef]
- Rimm, E.B.; Giovannucci, E.L.; Willett, W.C.; Colditz, G.A.; Ascherio, A.; Rosner, B.; Stampfer, M.J. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet 1991, 338, 464–468. [Google Scholar] [CrossRef]
- Hankinson, S.E.; Willett, W.C.; Manson, J.E.; Hunter, D.J.; Colditz, G.A.; Stampfer, M.J.; Longcope, C.; Speizer, F.E. Alcohol, height, and adiposity in relation to estrogen and prolactin levels in postmenopausal women. JNCI J. Natl. Cancer Inst. 1995, 87, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Feskanich, D.; Rimm, E.B.; Giovannucci, E.L.; Colditz, G.A.; Stampfer, M.J.; Litin, L.B.; Willett, W.C. Reproducibility and validity of food intake measurements from a semiquantitative food frequency questionnaire. J. Am. Diet. Assoc. 1993, 93, 790–796. [Google Scholar] [CrossRef]
- Rimm, E.B.; Giovannucci, E.L.; Stampfer, M.J.; Colditz, G.A.; Litin, L.B.; Willett, W.C. Reproducibility and validity of an expanded self-administered semiquantitative food frequency questionnaire among male health professionals. Am. J. Epidemiol. 1992, 135, 1114–1126. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Rood, J.C.; Harnack, L.J.; Sampson, L.K.; et al. Relative Validity of Nutrient Intakes Assessed by Questionnaire, 24-Hour Recalls, and Diet Records as Compared With Urinary Recovery and Plasma Concentration Biomarkers: Findings for Women. Am. J. Epidemiol. 2018, 187, 1051–1063. [Google Scholar] [CrossRef]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Subar, A.F.; Sampson, L.K.; Willett, W.C. Validity of a Dietary Questionnaire Assessed by Comparison With Multiple Weighed Dietary Records or 24-Hour Recalls. Am. J. Epidemiol. 2017, 185, 570–584. [Google Scholar] [CrossRef] [PubMed]
- Al-Shaar, L.; Yuan, C.; Rosner, B.; Dean, S.B.; Ivey, K.L.; Clowry, C.M.; Sampson, L.A.; Barnett, J.B.; Rood, J.; Harnack, L.J. Reproducibility and Validity of a Semiquantitative Food Frequency Questionnaire in Men Assessed by Multiple Methods. Am. J. Epidemiol. 2021, 190, 1122–1132. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef]
- Hu, F.B.; Stampfer, M.J.; Rimm, E.; Ascherio, A.; Rosner, B.A.; Spiegelman, D.; Willett, W.C. Dietary fat and coronary heart disease: A comparison of approaches for adjusting for total energy intake and modeling repeated dietary measurements. Am. J. Epidemiol. 1999, 149, 531–540. [Google Scholar] [CrossRef]
- Pai, J.K.; Pischon, T.; Ma, J.; Manson, J.E.; Hankinson, S.E.; Joshipura, K.; Curhan, G.C.; Rifai, N.; Cannuscio, C.C.; Stampfer, M.J. Inflammatory markers and the risk of coronary heart disease in men and women. N. Engl. J. Med. 2004, 351, 2599–2610. [Google Scholar] [CrossRef] [PubMed]
- Hankinson, S.; London, S.; Chute, C.; Barbieri, R.L.; Jones, L.; Kaplan, L.; Sacks, F.; Stampfer, M. Effect of transport conditions on the stability of biochemical markers in blood. Clin. Chem. 1989, 35, 2313–2316. [Google Scholar] [CrossRef]
- Cheng, S.; Larson, M.G.; McCabe, E.L.; Murabito, J.M.; Rhee, E.P.; Ho, J.E.; Jacques, P.F.; Ghorbani, A.; Magnusson, M.; Souza, A.L. Distinct metabolomic signatures are associated with longevity in humans. Nat. Commun. 2015, 6, 6791. [Google Scholar] [CrossRef]
- Mascanfroni, I.D.; Takenaka, M.C.; Yeste, A.; Patel, B.; Wu, Y.; Kenison, J.E.; Siddiqui, S.; Basso, A.S.; Otterbein, L.E.; Pardoll, D.M. Metabolic control of type 1 regulatory T cell differentiation by AHR and HIF1-α. Nat. Med. 2015, 21, 638–646. [Google Scholar] [CrossRef]
- O’Sullivan, J.F.; Morningstar, J.E.; Yang, Q.; Zheng, B.; Gao, Y.; Jeanfavre, S.; Scott, J.; Fernandez, C.; Zheng, H.; O’Connor, S. Dimethylguanidino valeric acid is a marker of liver fat and predicts diabetes. J. Clin. Investig. 2017, 127, 4394–4402. [Google Scholar] [CrossRef]
- Paynter, N.P.; Balasubramanian, R.; Giulianini, F.; Wang, D.D.; Tinker, L.F.; Gopal, S.; Deik, A.A.; Bullock, K.; Pierce, K.A.; Scott, J. Metabolic predictors of incident coronary heart disease in women. Circulation 2018, 137, 841–853. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Baden, M.Y.; Guasch-Ferré, M.; Wittenbecher, C.; Li, J.; Li, Y.; Wan, Y.; Bhupathiraju, S.N.; Tobias, D.K.; Clish, C.B. Plasma metabolite profiles related to plant-based diets and the risk of type 2 diabetes. Diabetologia 2022, 65, 1119–1132. [Google Scholar] [CrossRef]
- Wang, F.; Chandler, P.D.; Zeleznik, O.A.; Wu, K.; Wu, Y.; Yin, K.; Song, R.; Avila-Pacheco, J.; Clish, C.B.; Meyerhardt, J.A.; et al. Plasma Metabolite Profiles of Red Meat, Poultry, and Fish Consumption, and Their Associations with Colorectal Cancer Risk. Nutrients 2022, 14, 978. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. J. Stat. Softw. 2010, 33, 1. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Giovannucci, E.L. Sex differences in the association of obesity and colorectal cancer risk. Cancer Causes Control CCC 2017, 28, 1–4. [Google Scholar] [CrossRef]
- Yue, Y.; Hur, J.; Cao, Y.; Tabung, F.K.; Wang, M.; Wu, K.; Song, M.; Zhang, X.; Liu, Y.; Meyerhardt, J.A.; et al. Prospective evaluation of dietary and lifestyle pattern indices with risk of colorectal cancer in a cohort of younger women. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Seidel, A.; Brunner, S.; Seidel, P.; Fritz, G.I.; Herbarth, O. Modified nucleosides: An accurate tumour marker for clinical diagnosis of cancer, early detection and therapy control. Br. J. Cancer 2006, 94, 1726–1733. [Google Scholar] [CrossRef]
- Feng, B.; Zheng, M.H.; Zheng, Y.F.; Lu, A.G.; Li, J.W.; Wang, M.L.; Ma, J.J.; Xu, G.W.; Liu, B.Y.; Zhu, Z.G. Normal and modified urinary nucleosides represent novel biomarkers for colorectal cancer diagnosis and surgery monitoring. J. Gastroenterol. Hepatol. 2005, 20, 1913–1919. [Google Scholar] [CrossRef]
- Rubin, J.B.; Lagas, J.S.; Broestl, L.; Sponagel, J.; Rockwell, N.; Rhee, G.; Rosen, S.F.; Chen, S.; Klein, R.S.; Imoukhuede, P.; et al. Sex differences in cancer mechanisms. Biol. Sex Differ. 2020, 11, 17. [Google Scholar] [CrossRef]
- Zeleznik, O.A.; Eliassen, A.H.; Kraft, P.; Poole, E.M.; Rosner, B.A.; Jeanfavre, S.; Deik, A.A.; Bullock, K.; Hitchcock, D.S.; Avila-Pacheco, J.; et al. A Prospective Analysis of Circulating Plasma Metabolites Associated with Ovarian Cancer Risk. Cancer Res. 2020, 80, 1357–1367. [Google Scholar] [CrossRef]
- Dossus, L.; Kouloura, E.; Biessy, C.; Viallon, V.; Siskos, A.P.; Dimou, N.; Rinaldi, S.; Merritt, M.A.; Allen, N.; Fortner, R.; et al. Prospective analysis of circulating metabolites and endometrial cancer risk. Gynecol. Oncol. 2021, 162, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; He, X.; Ugai, T.; Haruki, K.; Lo, C.H.; Hang, D.; Akimoto, N.; Fujiyoshi, K.; Wang, M.; Fuchs, C.S.; et al. Risk Factors and Incidence of Colorectal Cancer According to Major Molecular Subtypes. JNCI Cancer Spectr. 2021, 5, pkaa089. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Giovannucci, E.L. Are exposure-disease relationships assessed in cohorts of health professionals generalizable?: A comparative analysis based on WCRF/AICR systematic literature reviews. Cancer Causes Control. CCC 2022, 34, 39–45. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Metabolomic Studies | CRC Nested Case-Control Study | |||
|---|---|---|---|---|
| HPFS (n = 697) | NHS (n = 6143) | Control (n = 524) | Case (n = 524) | |
| Age, year | 63.3 (8.1) | 57.4 (6.8) | 60.2 (7.6) | 60.2 (7.6) |
| BMI, kg/m2 | ||||
| Lean | 58 | 56 | 54 | 49 |
| Overweight | 37 | 30 | 32 | 37 |
| Obese | 5 | 14 | 14 | 15 |
| Physical activity, MET-h/week | 35.6 (32.4) | 15.2 (10.1) | 19.5 (20.7) | 20.0 (22.3) |
| Total calorie, kcal/day | 2016 (567) | 1775 (465) | 1853 (511) | 1854 (523) |
| Women, % | 0 | 100 | 75.2 | 75.2 |
| White, % | 96 | 96 | 99 | 97 |
| NSAIDs use, % | 46 | 25 | 33 | 29 |
| Smoking, % | ||||
| Never | 48 | 46 | 43 | 43 |
| Past | 47 | 41 | 45 | 43 |
| Current | 5 | 13 | 12 | 14 |
| Menopausal status, % | ||||
| Missing/dubious | NA | 10 | 8 | 8 |
| Premenopausal | NA | 17 | 14 | 15 |
| Post on PMH | NA | 33 | 31 | 28 |
| Post but not on PMH | NA | 40 | 47 | 49 |
| Family history of CRC, % | 15 | 13 | 14 | 17 |
| Endoscopy, % | 33 | 38 | 37 | 33 |
| OR (95% CI) | Men | Women | ||
|---|---|---|---|---|
| Per 1 SD Increase in Score | p-Value | Per 1 SD Increase in Score | p-Value | |
| MDIP signature | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 1.58 (1.15–2.17) | 0.005 | 1.02 (0.89–1.18) | 0.78 |
| MV model 1 | 1.89 (1.30–2.74) | <0.001 | 0.99 (0.84–1.17) | 0.87 |
| MV model 2 | 1.91 (1.31–2.78) | <0.001 | 1.00 (0.85–1.19) | 0.97 |
| EDIP-only signature | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 0.97 (0.75–1.26) | 0.83 | 1.06 (0.92–1.23) | 0.40 |
| MV model 1 | 1.00 (0.74–1.36) | 0.99 | 1.05 (0.89–1.24) | 0.56 |
| MV model 2 | 1.12 (0.78–1.60) | 0.55 | 1.13 (0.94–1.36) | 0.18 |
| BIOM-only signature | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 1.37 (1.02–1.84) | 0.04 | 1.06 (0.92–1.22) | 0.65 |
| MV model 1 | 1.60 (1.13–2.27) | 0.008 | 1.04 (0.88–1.23) | 0.69 |
| MV model 2 | 1.65 (1.16–2.36) | 0.006 | 1.05 (0.89–1.24) | 0.57 |
| EDIP score (diet) | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 0.99 (0.80–1.24) | 0.95 | 1.08 (0.93–1.24) | 0.31 |
| MV model 1 | 1.20 (0.90–1.61) | 0.21 | 1.04 (0.89–1.22) | 0.63 |
| MV model 2 | 1.47 (1.03–2.09) | 0.03 | 1.12 (0.94–1.34) | 0.21 |
| EDIP score (diet)—full cohort a | ||||
| Case/person-year | 1189/968,564 | 1486/1,685,241 | ||
| Basic model | 1.10 (1.03–1.17) | 0.003 | 1.05 (0.99–1.11) | 0.08 |
| MV model 1 | 1.15 (1.08–1.23) | <0.001 | 1.06 (1.01–1.13) | 0.03 |
| MV model 2 | 1.17 (1.09–1.26) | <0.001 | 1.08 (1.02–1.16) | 0.02 |
| OR (95% CI) | Men | Women | ||
|---|---|---|---|---|
| Per 1 SD Increase in Score | p-value | Per 1 SD Increase in Score | p-value | |
| MDIH signature | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 1.12 (0.86–1.45) | 0.40 | 0.97 (0.84–1.13) | 0.72 |
| MV model 1 | 1.11 (0.82–1.51) | 0.48 | 0.95 (0.80–1.11) | 0.50 |
| MV model 2 | 1.12 (0.82–1.52) | 0.48 | 0.95 (0.81–1.12) | 0.55 |
| EDIH-only signature | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 0.95 (0.73–1.23) | 0.69 | 1.14 (0.99–1.32) | 0.06 |
| MV model 1 | 0.92 (0.68–1.25) | 0.61 | 1.15 (0.98–1.36) | 0.09 |
| MV model 2 | 0.97 (0.70–1.34) | 0.85 | 1.20 (1.01–1.42) | 0.04 |
| CPEP-only signature | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 1.20 (0.90–1.59) | 0.21 | 0.98 (0.85–1.13) | 0.80 |
| MV model 1 | 1.25 (0.89–1.75) | 0.19 | 0.95 (0.81–1.12) | 0.55 |
| MV model 2 | 1.26 (0.90–1.77) | 0.19 | 0.97 (0.82–1.14) | 0.66 |
| EDIH score (diet) | ||||
| Case/control | 130/130 | 394/394 | ||
| Basic model | 1.04 (0.82–1.32) | 0.76 | 1.21 (1.05–1.40) | 0.01 |
| MV model 1 | 1.13 (0.85–1.51) | 0.40 | 1.22 (1.03–1.43) | 0.02 |
| MV model 2 | 1.20 (0.89–1.63) | 0.24 | 1.27 (1.07–1.50) | 0.006 |
| EDIH score (diet)—full cohort a | ||||
| Case/person-year | 1189/968,564 | 1486/1,685,241 | ||
| Basic model | 1.10 (1.03–1.17) | 0.007 | 1.08 (1.01–1.15) | 0.02 |
| MV model 1 | 1.13 (1.06–1.22) | <0.001 | 1.07 (1.00–1.14) | 0.04 |
| MV model 2 | 1.13 (1.06–1.22) | <0.001 | 1.08 (1.01–1.15) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.H.; Jin, Q.; Shi, N.; Wang, F.; Bever, A.M.; Li, J.; Liang, L.; Hu, F.B.; Song, M.; Zeleznik, O.A.; et al. Dietary Inflammatory and Insulinemic Potentials, Plasma Metabolome and Risk of Colorectal Cancer. Metabolites 2023, 13, 744. https://doi.org/10.3390/metabo13060744
Lee DH, Jin Q, Shi N, Wang F, Bever AM, Li J, Liang L, Hu FB, Song M, Zeleznik OA, et al. Dietary Inflammatory and Insulinemic Potentials, Plasma Metabolome and Risk of Colorectal Cancer. Metabolites. 2023; 13(6):744. https://doi.org/10.3390/metabo13060744
Chicago/Turabian StyleLee, Dong Hoon, Qi Jin, Ni Shi, Fenglei Wang, Alaina M. Bever, Jun Li, Liming Liang, Frank B. Hu, Mingyang Song, Oana A. Zeleznik, and et al. 2023. "Dietary Inflammatory and Insulinemic Potentials, Plasma Metabolome and Risk of Colorectal Cancer" Metabolites 13, no. 6: 744. https://doi.org/10.3390/metabo13060744
APA StyleLee, D. H., Jin, Q., Shi, N., Wang, F., Bever, A. M., Li, J., Liang, L., Hu, F. B., Song, M., Zeleznik, O. A., Zhang, X., Joshi, A., Wu, K., Jeon, J. Y., Meyerhardt, J. A., Chan, A. T., Eliassen, A. H., Clish, C. B., Clinton, S. K., ... Tabung, F. K. (2023). Dietary Inflammatory and Insulinemic Potentials, Plasma Metabolome and Risk of Colorectal Cancer. Metabolites, 13(6), 744. https://doi.org/10.3390/metabo13060744