

The Evaluation of CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Phenoconversion in Post-Mortem Casework: The Challenge of Forensic Toxicogenetics

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population, Inclusion Criteria, and Sample Collection
2.2. Systematic Toxicological Analysis
2.3. CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Genotyping
2.4. Activity Score, Phenotype, and Phenoconversion Assessment
2.5. Data and Statistical Analyses
3. Results
3.1. CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Genotype and g-Phenotype
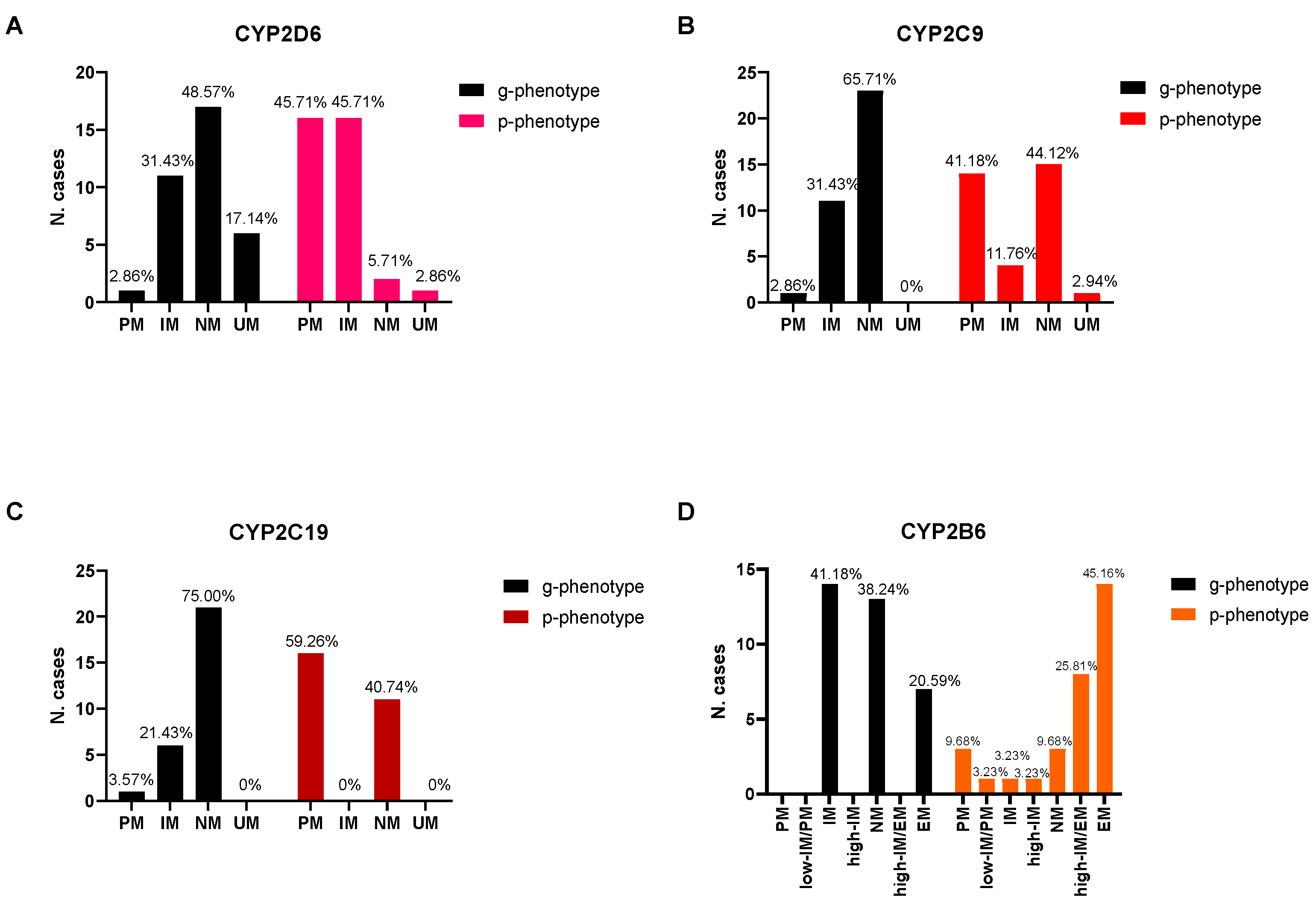
3.2. Phenoconversion, Activity Score (AS) Adjustment, and Statistical Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hicks, J.K.; Swen, J.J.; Gaedigk, A. Challenges in CYP2D6 Phenotype Assignment from Genotype Data: A Critical Assessment and Call for Standardization. Curr. Drug Metab. 2014, 15, 218–232. [Google Scholar] [CrossRef]
- Pirmohamed, M. Pharmacogenomics: Current status and future perspectives. Nat. Rev. Genet. 2023. ahead of print. [Google Scholar] [CrossRef]
- Wendt, F.R.; Novroski, N.M.; Rahikainen, A.-L.; Sajantila, A.; Budowle, B. Supervised Classification of CYP2D6 Genotype and Metabolizer Phenotype with Postmortem Tramadol-Exposed Finns. Am. J. Forensic Med. Pathol. 2019, 40, 8–18. [Google Scholar] [CrossRef]
- Musshoff, F.; Stamer, U.M.; Madea, B. Pharmacogenetics and forensic toxicology. Forensic Sci. Int. 2010, 203, 53–62. [Google Scholar] [CrossRef]
- Hahn, M.; Roll, S.C. The Influence of Pharmacogenetics on the Clinical Relevance of Pharmacokinetic Drug-Drug Interactions: Drug-Gene, Drug-Gene-Gene and Drug-Drug-Gene Interactions. Pharmaceuticals 2021, 14, 487. [Google Scholar] [CrossRef]
- Peters, F.T.; Steuer, A.E. Antemortem and Postmortem Influences on Drug Concentrations and Metabolite Patterns in Post-mortem Specimens. WIREs Forensic Sci. 2019, 1. [Google Scholar] [CrossRef]
- Shah, R.R.; Smith, R.L. Addressing phenoconversion: The Achilles’ heel of personalized medicine. Br. J. Clin. Pharmacol. 2015, 79, 222–240. [Google Scholar] [CrossRef]
- Gaedigk, A.; Simon, S.D.; Pearce, R.E.; Bradford, L.D.; Kennedy, M.J.; Leeder, J.S. The CYP2D6 Activity Score: Translating Genotype Information into a Qualitative Measure of Phenotype. Clin. Pharmacol. Ther. 2008, 83, 234–242. [Google Scholar] [CrossRef]
- Pratt, V.M.; Cavallari, L.H.; Del Tredici, A.L.; Gaedigk, A.; Hachad, H.; Ji, Y.; Kalman, L.V.; Ly, R.C.; Moyer, A.M.; Scott, S.A.; et al. Recommendations for Clinical CYP2D6 Genotyping Allele Selection: A Joint Consensus Recommendation of the Association for Molecular Pathology, College of American Pathologists, Dutch Pharmacogenetics Working Group of the Royal Dutch Pharmacists Association, and the European Society for Pharmacogenomics and Personalized Therapy. J. Mol. Diagn. 2021, 23, 1047–1064. [Google Scholar]
- Del Toro-Pagán, N.M.; Matos, A.; Thacker, D.; Turgeon, J.; Amin, N.S.; Michaud, V. Pharmacist-Led Medication Evaluation Considering Pharmacogenomics and Drug-Induced Phenoconversion in the Treatment of Multiple Comorbidities: A Case Report. Medicina 2021, 57, 955. [Google Scholar] [CrossRef]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.-J.; Swen, J.J. Phenoconversion of Cytochrome P450 Metabolism: A Systematic Review. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef]
- Mostafa, S.; Polasek, T.M.; Sheffield, L.J.; Huppert, D.; Kirkpatrick, C.M.J. Quantifying the Impact of Phenoconversion on Medications With Actionable Pharmacogenomic Guideline Recommendations in an Acute Aged Persons Mental Health Setting. Front Psychiatry 2021, 12, 724170. [Google Scholar] [CrossRef]
- Cicali, E.J.; Smith, D.M.; Duong, B.Q.; Kovar, L.G.; Cavallari, L.H.; Johnson, J.A. A Scoping Review of the Evidence Behind Cyto-chrome P450 2D6 Isoenzyme Inhibitor Classifications. Clin. Pharmacol. Ther. 2020, 108, 116–125. [Google Scholar] [CrossRef]
- Scordo, M.G.; Caputi, A.P.; D’arrigo, C.; Fava, G.; Spina, E. Allele and genotype frequencies of CYP2C9, CYP2C19 and CYP2D6 in an Italian population. Pharmacol. Res. 2004, 50, 195–200. [Google Scholar] [CrossRef]
- Cacabelos, R.; Naidoo, V.; Corzo, L.; Cacabelos, N.; Carril, J.C. Genophenotypic Factors and Pharmacogenomics in Adverse Drug Reactions. Int. J. Mol. Sci. 2021, 22, 13302. [Google Scholar] [CrossRef]
- Di Nunno, N.; Esposito, M.; Argo, A.; Salerno, M.; Sessa, F. Pharmacogenetics and Forensic Toxicology: A New Step towards a Multidisciplinary Approach. Toxics 2021, 9, 292. [Google Scholar] [CrossRef]
- Sajantila, A.; Palo, J.U.; Ojanperä, I.; Davis, C.; Budowle, B. Pharmacogenetics in Medico-Legal Context. Forensic Sci. Int. 2010, 203, 44–52. [Google Scholar] [CrossRef]
- Wendt, F.R.; Budowle, B. Pharmacogenetics and the postmortem molecular autopsy. WIREs Forensic Sci. 2020, 2, e1361. [Google Scholar] [CrossRef]
- Pelletti, G.; Rossi, F.; Garagnani, M.; Barone, R.; Roffi, R.; Fais, P.; Pelotti, S. Optimization of cloned enzyme donor immunoassay cut-offs for drugs of abuse in post-mortem whole blood. Forensic Sci. Int. 2020, 312, 110291. [Google Scholar] [CrossRef]
- Pelletti, G.; Barone, R.; Giorgetti, A.; Garagnani, M.; Rossi, F.; Fais, P.; Pelotti, S. “Light cannabis” consumption in a sample of young adults: Preliminary pharmacokinetic data and psychomotor impairment evaluation. Forensic Sci. Int. 2021, 323, 110822. [Google Scholar] [CrossRef]
- Barone, R.; Giorgetti, A.; Cardella, R.; Rossi, F.; Garagnani, M.; Pascali, J.P.; Mohamed, S.; Fais, P.; Pelletti, G. Development and validation of a fast UPLC-MS/MS screening method for the detection of 68 psychoactive drugs and metabolites in whole blood and application to post-mortem cases. J. Pharm. Biomed Anal. 2023, 10, 115315. [Google Scholar] [CrossRef]
- Pelletti, G.; Verstraete, A.G.; Reyns, T.; Barone, R.; Rossi, F.; Garagnani, M.; Pelotti, S. Prevalence of Therapeutic Drugs in Blood of Drivers Involved in Traffic Crashes in the Area Segoe UI of Bologna, Italy. Forensic Sci. Int. 2019, 302, 109914. [Google Scholar] [CrossRef]
- Thermo Fisher Cloud Genotyping Application. Available online: https://apps.thermofisher.com/apps/spa/#/apps (accessed on 24 March 2023).
- Carano, F.; Sarno, S.; Fanti, D.; Serventi, P.; Bini, C.; Luiselli, D.; Pelotti, S. Genetic Variability of CYP2D6, CYP2B6, CYP2C9 and CYP2C19 Genes across the Italian Peninsula. Ann Hum. Biol. 2018, 45, 66–71. [Google Scholar] [CrossRef]
- Botton, M.R.; Lu, X.; Zhao, G.; Repnikova, E.; Seki, Y.; Gaedigk, A.; Schadt, E.E.; Edelmann, L.; Scott, S.A. Structural variation at the CYP2C locus: Characterization of deletion and duplication alleles. Hum. Mutat. 2019, 40. [Google Scholar] [CrossRef]
- Martis, S.; Mei, H.; Vijzelaar, R.; Edelmann, L.; Desnick, R.J.; Scott, S.A. Multi-ethnic cytochrome-P450 copy number profiling: Novel pharmacogenetic alleles and mechanism of copy number variation formation. Pharm. J. 2013, 13, 558–566. [Google Scholar] [CrossRef]
- Stephens, M.; Donnelly, P. A comparison of bayesian methods for haplotype reconstruction from population genotype data. Am. J. Hum. Genet. 2003, 73, 1162–1169. [Google Scholar] [CrossRef]
- PharmVar. Available online: https://www.pharmvar.org/ (accessed on 24 March 2023).
- Borges, S.; Desta, Z.; Jin, Y.; Faouzi, A.; Robarge, J.D.; Philips, S.; Nguyen, A.; Stearns, V.; Hayes, D.; Rae, J.M.; et al. Composite Functional Genetic and Comedication CYP2D6 Activity Score in Predicting Tamoxifen Drug Exposure among Breast Cancer Patients. J. Clin. Pharmacol. 2010, 50, 450–458. [Google Scholar] [CrossRef]
- PharmGKB. PGx Gene-Specific Information Tables. Available online: https://www.pharmgkb.org/page/pgxGeneRef (accessed on 24 March 2023).
- Caudle, K.E.; Sangkuhl, K.; Whirl-Carrillo, M.; Swen, J.J.; Haidar, C.E.; Klein, T.E.; Gammal, R.S.; Relling, M.V.; Scott, S.A.; Hertz, D.L.; et al. Standardizing CYP2D6 Genotype to Phenotype Translation: Consensus Recommendations from the Clin-ical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin. Transl. Sci. 2020, 13, 116–124. [Google Scholar] [CrossRef]
- Koopmans, A.B.; Braakman, M.H.; Vinkers, D.J.; Hoek, H.W.; van Harten, P.N. Meta-analysis of probability estimates of worldwide variation of CYP2D6 and CYP2C19. Transl. Psychiatry 2021, 11, 141. [Google Scholar] [CrossRef]
- Theken, K.N.; Lee, C.R.; Gong, L.; Caudle, K.E.; Formea, C.M.; Gaedigk, A.; Klein, T.E.; Agúndez, J.A.; Grosser, T. Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clin. Pharmacol. Ther. 2020, 108, 191–200. [Google Scholar] [CrossRef]
- DPWG: Dutch Pharmacogenetics Working Group. Available online: https://www.pharmgkb.org/page/dpwg (accessed on 24 March 2023).
- Whirl-Carrillo, M.; Huddart, R.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Whaley, R.; Klein, T.E. An Evidence-Based Framework for Evaluating Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2021, 110, 563–572. [Google Scholar] [CrossRef]
- Mostafa, S.; Kirkpatrick, C.M.J.; Byron, K.; Sheffield, L. An analysis of allele, genotype and phenotype frequencies, actionable pharmacogenomic (PGx) variants and phenoconversion in 5408 Australian patients genotyped for CYP2D6, CYP2C19, CYP2C9 and VKORC1 genes. J. Neural Transm. 2018, 126, 5–18. [Google Scholar] [CrossRef]
- Flockhart, D.A.; Thacker, D.; McDonald, C.; Desta, Z.; The Flockhart Cytochrome P450 Drug-Drug Interaction Table. Division of Clinical Pharmacology, Indiana University School of Medicine (Updated 2021). Available online: https://drug-interactions.medicine.iu.edu (accessed on 24 March 2023).
- DrugBank Online|Database for Drug and Drug Target Info. Available online: https://go.drugbank.com/ (accessed on 24 March 2023).
- Obach, R.S.; Walker, G.S.; Brodney, M.A. Biosynthesis of Fluorinated Analogs of Drugs Using Human Cytochrome P450 Enzymes Followed by Deoxyfluorination and Quantitative Nuclear Magnetic Resonance Spectroscopy to Improve Metabolic Stability. Drug Metab. Dispos. 2016, 44, 634–646. [Google Scholar] [CrossRef]
- Hakkola, J.; Hukkanen, J.; Turpeinen, M.; Pelkonen, O. Inhibition and induction of CYP enzymes in humans: An update. Arch. Toxicol. 2020, 94, 3671–3722. [Google Scholar] [CrossRef]
- Luong, T.-L.T.; Powers, C.N.; Reinhardt, B.J.; Weina, P.J. Pre-clinical drug-drug interactions (DDIs) of gefitinib with/without losartan and selective serotonin reuptake inhibitors (SSRIs): Citalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, and venlafaxine. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100112. [Google Scholar] [CrossRef]
- Mangó, K.; Kiss, F.; Fekete, F.; Erdős, R.; Monostory, K. CYP2B6 allelic variants and non-genetic factors influence CYP2B6 enzyme function. Sci. Rep. 2022, 12, 2984. [Google Scholar] [CrossRef]
- Bousman, C.A.; Wu, P.; Aitchison, K.J.; Cheng, T. Sequence2Script: A Web-Based Tool for Translation of Pharmacogenetic Data Into Evidence-Based Prescribing Recommendations. Front. Pharmacol. 2021, 12, 636650. [Google Scholar] [CrossRef]
- Huddart, R.; Fohner, A.E.; Whirl-Carrillo, M.; Wojcik, G.L.; Gignoux, C.R.; Popejoy, A.B.; Bustamante, C.D.; Altman, R.B.; Klein, T.E. Standardized Biogeographic Grouping System for Annotating Populations in Pharmacogenetic Research. Clin. Pharmacol. Ther. 2019, 105, 1256–1262. [Google Scholar] [CrossRef]
- Taylor, C.; Crosby, I.; Yip, V.; Maguire, P.; Pirmohamed, M.; Turner, R.M. A Review of the Important Role of CYP2D6 in Pharmacogenomics. Genes 2020, 11, 1295. [Google Scholar] [CrossRef]
- Volpe, D.A.; Xu, Y.; Sahajwalla, C.G.; Younis, I.R.; Patel, V. Methadone Metabolism and Drug-Drug Interactions: In Vitro and In Vivo Literature Review. J. Pharm. Sci. 2018, 107, 2983–2991. [Google Scholar] [CrossRef]
- Packiasabapathy, S.; Aruldhas, B.W.; Horn, N.; Overholser, B.R.; Quinney, S.K.; Renschler, J.S.; Sadhasivam, S. Phar-macogenomics of Methadone: A Narrative Review of the Literature. Pharmacogenomics 2020, 21, 871–887. [Google Scholar] [CrossRef] [PubMed]
- Skoda, J.; Dusek, J.; Drastik, M.; Stefela, A.; Dohnalova, K.; Chalupsky, K.; Smutny, T.; Micuda, S.; Gerbal-Chaloin, S.; Pavek, P. Diazepam Promotes Translocation of Human Constitutive Androstane Receptor (CAR) via Direct Interaction with the Ligand-Binding Domain. Cells 2020, 9, 2532. [Google Scholar] [CrossRef] [PubMed]
- Desta, Z.; El-Boraie, A.; Gong, L.; Somogyi, A.A.; Lauschke, V.M.; Dandara, C.; Klein, K.; Miller, N.; Klein, T.E.; Tyndale, R.F.; et al. PharmVar GeneFocus: CYP2B6. Clin. Pharmacol. Ther. 2021, 110, 82–97. [Google Scholar] [CrossRef]
- Drevin, G.; Picard, N.; Jousset, N.; Briet, M.; Abbara, C. Pitfalls and Challenges Associated with Phenoconversion in Forensic Toxcicology. Forensic Sci. Int. Genet 2021, 51, 102433. [Google Scholar] [CrossRef]
- Cicali, E.J.; Elchynski, A.L.; Cook, K.J.; Houder, J.T.; Thomas, C.D.; Smith, D.M.; Elsey, A.; Johnson, J.A.; Cavallari, L.H.; Wiisanen, K. How to Integrate CYP2D6 Phenoconversion into Clinical Pharmacogenetics: A Tutorial. Clin. Pharmacol. Ther. 2021, 110, 677–687. [Google Scholar] [CrossRef]
- Veronin, M.A.; Schumaker, R.P.; Dixit, R.R.; Elath, H. Opioids and frequency counts in the US Food and Drug Administration Adverse Event Reporting System (FAERS) database: A quantitative view of the epidemic. Drug Health Patient Saf. 2019, 11, 65–70. [Google Scholar] [CrossRef]
- Gadel, S.; Friedel, C.; Kharasch, E.D. Differences in Methadone Metabolism by CYP2B6 Variants. Drug Metab. Dispos. 2015, 43, 994–1001. [Google Scholar] [CrossRef]
- Ahmad, T.; Sabet, S.; Primerano, D.A.; Richards-Waugh, L.L.; Rankin, G.O. Tell-Tale SNPs: The Role of CYP2B6 in Methadone Fatalities. J. Anal. Toxicol. 2017, 41, 325–333. [Google Scholar] [CrossRef]
- Langmia, I.M.; Just, K.S.; Yamoune, S.; Brockmöller, J.; Masimirembwa, C.; Stingl, J.C. CYP2B6 Functional Variability in Drug Metabolism and Exposure Across Populations-Implication for Drug Safety, Dosing, and Individualized Therapy. Front Genet 2021, 12, 692234. [Google Scholar] [CrossRef] [PubMed]
- Turpeinen, M.; Zanger, U.M. Cytochrome P450 2B6: Function, Genetics, and Clinical Relevance. Drug Metabol. Drug Interact 2012, 27, 185–197. [Google Scholar] [CrossRef]
- Parkinson, A.; Mudra, D.R.; Johnson, C.; Dwyer, A.; Carroll, K.M. The effects of gender, age, ethnicity, and liver cirrhosis on cytochrome P450 enzyme activity in human liver microsomes and inducibility in cultured human hepatocytes. Toxicol. Appl. Pharmacol. 2004, 199, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Koski, A.; Sistonen, J.; Ojanperä, I.; Gergov, M.; Vuori, E.; Sajantila, A. CYP2D6 and CYP2C19 genotypes and amitriptyline metabolite ratios in a series of medicolegal autopsies. Forensic Sci. Int. 2006, 158, 177–183. [Google Scholar] [CrossRef]
- Zhou, Y.; Lauschke, V.M. Population pharmacogenomics: An update on ethnogeographic differences and opportunities for precision public health. Hum Genet. 2022, 141, 1113–1136. [Google Scholar] [CrossRef] [PubMed]
- Sistonen, J.; Fuselli, S.; Palo, J.U.; Chauhan, N.; Padh, H.; Sajantila, A. Pharmacogenetic variation at CYP2C9, CYP2C19, and CYP2D6 at global and microgeographic scales. Pharmacogenet Genomics. 2009, 19, 170–179. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Genotype | n. | % | g-Phenotype |
|---|---|---|---|
| CYP2D6 | |||
| *1/*1 | 7 | 20.00 | gNM |
| *1/*1 ×3 | 2 | 5.71 | gUM |
| *1/*2 | 4 | 11.43 | gNM |
| *1/*2 ×4 | 1 | 2.86 | gUM |
| *1/*4 | 5 | 14.29 | gIM |
| *1/*41 ×3 | 1 | 2.86 | gUM |
| *2/*2 ×3 | 1 | 2.86 | gUM |
| *2/*2 ×4 | 1 | 2.86 | gUM |
| *2/*2 | 4 | 11.43 | gNM |
| *2/*4 | 2 | 5.71 | gIM |
| *2/*41 | 2 | 5.71 | gNM |
| *4/*41 | 1 | 2.86 | gIM |
| *10/*10 | 1 | 2.86 | gIM |
| *41/*41 | 1 | 2.86 | gIM |
| *4/*10 | 1 | 2.86 | gIM |
| *4/*5 | 1 | 2.86 | gPM |
| Total | 35 | 100% | - |
| CYP2C9 | |||
| *1/*1 | 23 | 65.71 | gNM |
| *1/*2 | 9 | 25.71 | gIM |
| *1/*3 | 1 | 2.86 | gIM |
| *2/*2 | 1 | 2.86 | gIM |
| *2/*3 | 1 | 2.86 | gPM |
| 35 | 100% | - | |
| CYP2C19 | |||
| *1/*1 | 21 | 75 | gNM |
| *1/*2 | 6 | 21.43 | gIM |
| *2/*2 | 1 | 3.57 | gPM |
| Total | 28 | 100% | - |
| CYP2B6 | |||
| *1/*1 | 7 | 20.59 | gNM |
| *1/*4 | 6 | 17.65 | gEM |
| *1/*5 | 5 | 14.71 | gNM |
| *1/*6 | 10 | 29.41 | gIM |
| *1/*7 | 3 | 8.82 | gIM |
| *1/*9 | 1 | 2.94 | gIM |
| *1/*22 | 1 | 2.94 | gEM |
| *2/*5 | 1 | 2.94 | gNM |
| Total | 34 | 100% | - |
| Starting AS | g-Phenotype (n) | Inhibitors in Blood | Inducers in Blood | Adjusted AS | p-Phenotype | |
|---|---|---|---|---|---|---|
| CYP2D6 (n = 35) | ||||||
| Effect (n) | Drug(s) Detected | Drug(s) Detected | ||||
| 0 | gPM (1) | Strong (0) | - | - | - | - |
| Weak (1) | Citalopram | - | 0 | PM | ||
| None (0) | - | - | - | - | ||
| 0 < x < 1.25 | gIM (11) | Strong (4) | Chlorpromazine * Cocaine * Haloperidol * Paroxetine | - | 0 | PM |
| Moderate/Weak (7) | Amiodarone Clozapine Levomepromazine Methadone Sertraline Trazodone 11-OH-THC | - | 0.25 < x < 0.5 | IM | ||
| None (0) | - | - | - | - | ||
| 1.25 ≤ x ≤2.25 | gNM (17) | Strong (7) | Cocaine * Fluoxetine Paroxetine | - | 0 | PM |
| Moderate/Weak (8) | Citalopram Levomepromazine Lidocaine ** Methadone Olanzapine ** Trazodone Venlafaxine 11-OH -THC | - | 0.75 < x < 1 | IM | ||
| None (2) | - | - | - | NM | ||
| >2.25 | gUM (6) | Strong (4) | Chlorpromazine * Citalopram Cocaine * Paroxetine | - | 0 | PM |
| Moderate/Weak (1) | Methadone Trazodone | - | 1.5 | NM | ||
| None (1) | - | - | - | UM | ||
| CYP2C9 (n = 35) | ||||||
| Effect (n) | Drug(s) Detected | Drug(s) Detected | ||||
| 0–0.5 | gPM (1) | Strong/Moderate/Weak (1) | Paroxetine | - | - | PM |
| 1–1.5 | gIM (11) | Strong/Moderate/Weak (6) | Paroxetine Δ9-THC | - | - | PM |
| Strong/Moderate/Weak (1) | Valproic acid | Phenobarbital | - | n.d. | ||
| None (4) | - | - | - | IM | ||
| 2 | gNM (23) | Strong/Moderate/Weak (7) | Amiodarone Olanzapine Paroxetine Sertraline Δ9-THC Valproic acid | - | - | PM |
| None (1) | - | Warfarin | UM | |||
| None (15) | - | - | - | NM | ||
| CYP2C19 (n = 28) | ||||||
| Effect (n) | Drug(s) Detected | Drug(s) Detected | ||||
| gPM (1) | None (1) | - | - | |||
| - | gIM (6) | Strong/Moderate/Weak (3) | Amitriptyline Diazepam Sertraline | - | - | PM |
| None (3) | - | - | - | IM | ||
| - | gNM (21) | Strong/Moderate/Weak (13) | Amiodarone Citalopram Diazepam Fluoxetine Nordazepam Olanzapine Δ9-THC Valproic acid Warfarin | - | - | PM |
| - | Strong/Moderate/Weak (1) | Diazepam Valproic acid | Phenobarbital | - | n.d. | |
| - | None (7) | - | - | - | NM | |
| CYP2B6 (n = 34) | ||||||
| Effect (n) | Drug(s) Detected | Drug(s) Detected | ||||
| - | gIM (14) | Strong/Moderate/Weak (3) | Paroxetine | - | - | PM |
| - | None (8) | - | Diazepam * Methadone | - | high-IM\EM | |
| - | Strong/Moderate/Weak (2) | 11-OH-THC Paroxetine | Diazepam * Methadone | - | n.d. | |
| - | None (1) | - | - | - | IM | |
| - | gNM (13) | None (8) | - | Diazepam * Methadone | - | EM |
| - | Strong/Moderate/Weak (1) | Paroxetine | Diazepam * Methadone | - | n.d. | |
| - | Strong/Moderate/Weak (1) | Paroxetine | - | - | Low-IM/PM | |
| - | None (3) | - | - | - | NM | |
| - | gEM (7) | Strong/Moderate/Weak (1) | Paroxetine | - | - | High-IM |
| - | None (3) | - | Diazepam * Methadone | - | EM | |
| - | None (3) | - | - | - | EM | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giorgetti, A.; Amurri, S.; Fazio, G.; Bini, C.; Anniballi, L.; Pirani, F.; Pelletti, G.; Pelotti, S. The Evaluation of CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Phenoconversion in Post-Mortem Casework: The Challenge of Forensic Toxicogenetics. Metabolites 2023, 13, 661. https://doi.org/10.3390/metabo13050661
Giorgetti A, Amurri S, Fazio G, Bini C, Anniballi L, Pirani F, Pelletti G, Pelotti S. The Evaluation of CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Phenoconversion in Post-Mortem Casework: The Challenge of Forensic Toxicogenetics. Metabolites. 2023; 13(5):661. https://doi.org/10.3390/metabo13050661
Chicago/Turabian StyleGiorgetti, Arianna, Sara Amurri, Giulia Fazio, Carla Bini, Laura Anniballi, Filippo Pirani, Guido Pelletti, and Susi Pelotti. 2023. "The Evaluation of CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Phenoconversion in Post-Mortem Casework: The Challenge of Forensic Toxicogenetics" Metabolites 13, no. 5: 661. https://doi.org/10.3390/metabo13050661
APA StyleGiorgetti, A., Amurri, S., Fazio, G., Bini, C., Anniballi, L., Pirani, F., Pelletti, G., & Pelotti, S. (2023). The Evaluation of CYP2D6, CYP2C9, CYP2C19, and CYP2B6 Phenoconversion in Post-Mortem Casework: The Challenge of Forensic Toxicogenetics. Metabolites, 13(5), 661. https://doi.org/10.3390/metabo13050661