
Application of Lipidomics in Psychiatry: Plasma-Based Potential Biomarkers in Schizophrenia and Bipolar Disorder

 , , , and
, , , and 
Abstract
1. Introduction
2. Material and Methods
2.1. Sample and Clinical Assessments
2.2. Chemicals
2.3. Sample Collection and Preparation
2.4. Lipidomics Analysis
2.5. Data Processing and Statistical Analysis
3. Results
3.1. Selection of Potential Lipid Biomarkers
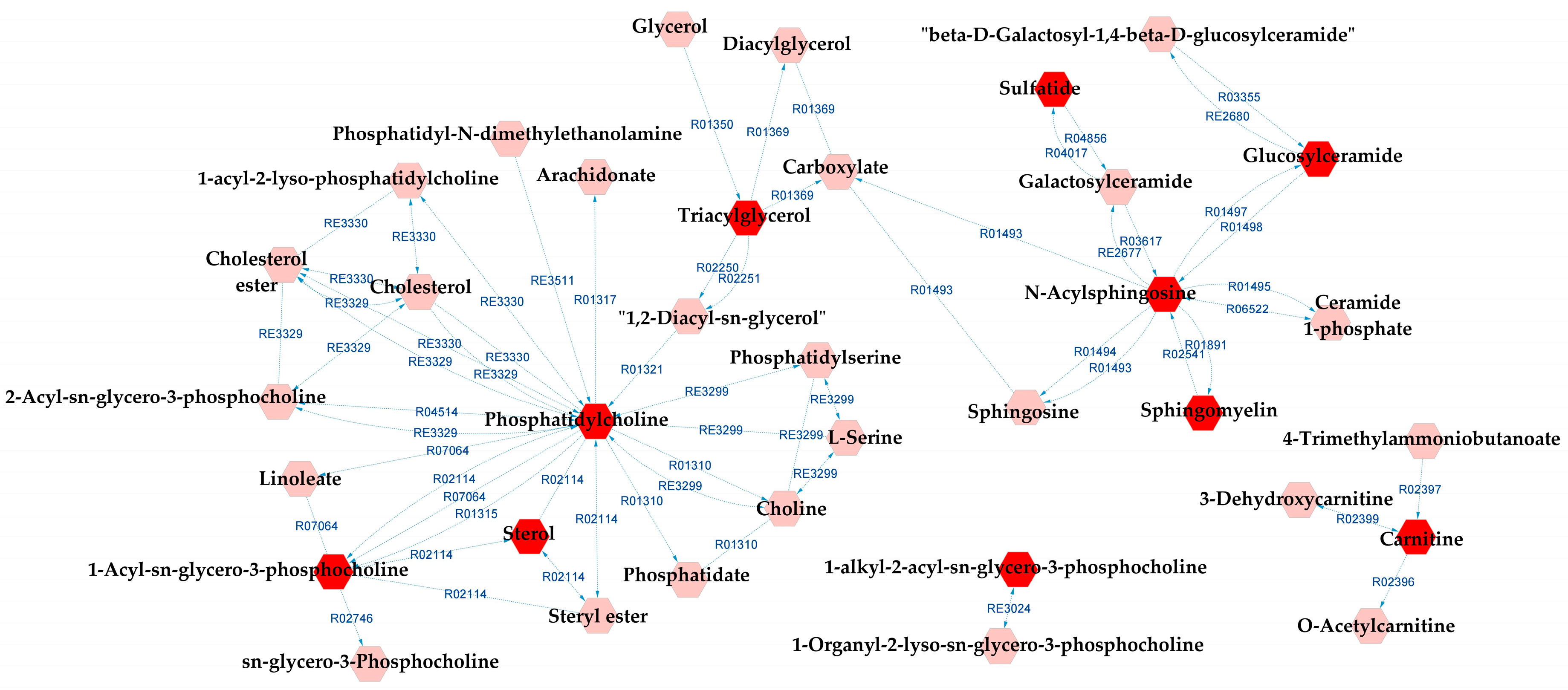
3.2. Differential Lipids and Potentially Altered Biochemical Pathways
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grande, I.; Berk, M.; Birmaher, B.; Vieta, E. Bipolar disorder. Lancet 2016, 387, 1561–1572. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Petukhova, M.; Vilagut, G.; Chatterji, S.; Heeringa, S.; Üstün, T.B.; Al-Hamzawi, A.; Viana, M.C.; Angermeyer, M.; Bromet, E.; et al. Days out of role due to common physical and mental conditions: Results from the WHO World Mental Health surveys. Mol. Psychiatry 2011, 16, 1234–1246. [Google Scholar] [CrossRef] [PubMed]
- Rowland, T.A.; Marwaha, S. Epidemiology and risk factors for bipolar disorder. Ther. Adv. Psychopharmacol. 2018, 8, 251–269. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). DSM-5: Manual Diagnóstico e Estatístico de Transtornos Mentais; Artmed Editora Ltda: Porto Alegre, Brazil, 2014. [Google Scholar]
- WHO. ICD-10 Classification of Mental and Behavioural Disorders (the): Diagnostic Criteria for Research; World Health Organization: Geneva, Switzerland, 1993.
- Goodwin, G.M.; Anderson, I.; Arango, C.; Bowden, C.L.; Henry, C.; Mitchell, P.B.; Nolen, W.A.; Vieta, E.; Wittchen, H.-U. ECNP consensus meeting. Bipolar depression. Nice, March 2007. Eur. Neuropsychopharmacol. 2008, 18, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.L.; Kupfer, D.J. Bipolar Disorder Diagnosis: Challenges and Future Directions. Lancet 2013, 381, 1663–1671. [Google Scholar] [CrossRef]
- Janoutová, J.; Janácková, P.; Serý, O.; Zeman, T.; Ambroz, P.; Kovalová, M.; Varechova, K.; Hosák, L.; Jirik, V.; Janout, V. Epidemiology and risk factors of schizophrenia. Neuro Endocrinol. Lett. 2016, 37, 1–8. [Google Scholar]
- Charlson, F.J.; Ferrari, A.J.; Santomauro, D.F.; Diminic, S.; Stockings, E.; Scott, J.G.; McGrath, J.; Whiteford, A.H. Global epidemiology and burden of schizophrenia: Findings from the global burden of disease study 2016. Schizophr. Bull. 2018, 44, 1195–1203. [Google Scholar] [CrossRef]
- Ayano, G. Bipolar disorder: A concise overview of etiology, epidemiology diagnosis and management: Review of literatures. SOJ Psychol. 2016, 3, 1–8. [Google Scholar] [CrossRef]
- Ayano, G. Schizophrenia: A concise overview of etiology, epidemiology diagnosis and management: Review of Literatures. J. Schizophr. Res. 2016, 3, 2–7. [Google Scholar]
- Brunkhorst-Kanaan, N.; Klatt-Schreiner, K.; Hackel, J.; Schröter, K.; Trautmann, S.; Hahnefeld, L.; Wicker, S.; Reif, A.; Thomas, D.; Geisslinger, G.; et al. Targeted lipidomics reveal derangement of ceramides in major depression and bipolar disorder. Metabolism 2019, 95, 65–76. [Google Scholar] [CrossRef]
- Ghosh, S.; Dyer, R.A.; Beasley, C.L. Evidence for altered cell membrane lipid composition in postmortem prefrontal white matter in bipolar disorder and schizophrenia. J. Psychiatr. Res. 2017, 95, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Tasic, L.; Pontes, J.G.M.; Carvalho, M.S.; Cruz, G.; Dal Mas, C.; Sethi, S.; Pedrini, M.; Rizzo, L.B.; Zeni-Graiff, M.; Asevedo, E.; et al. Metabolomics and lipidomics analyses by 1H nuclear magnetic resonance of schizophrenia patient serum reveal potential peripheral biomarkers for diagnosis. Schizophr. Res. 2017, 185, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Tessier, C.; Sweers, K.; Frajerman, A.; Bergaoui, H.; Ferreri, F.; Delva, C.; Lapidus, N.; Lamaziere, A.; Roiser, J.P.; De Hert, M.; et al. Membrane lipidomics in schizophrenia patients: A correlational study with clinical and cognitive manifestations. Transl. Psychiatry 2016, 6, e906. [Google Scholar] [CrossRef]
- Wang, F.; Guo, L.; Zhang, T.; Cui, Z.; Wang, J.; Zhang, C.; Xue, F.; Zhou, C.; Li, B.; Tan, Q.; et al. Alterations in plasma lipidomic profiles in adult patients with schizophrenia and major depressive disorder. Medicina 2022, 58, 1509. [Google Scholar] [CrossRef]
- Guo, L.; Zhang, T.; Li, R.; Cui, Z.-Q.; Du, J.; Yang, J.-B.; Xue, F.; Chen, Y.H.; Tan, Q.R.; Peng, Z.W. Alterations in the plasma lipidome of adult women with bipolar disorder: A mass spectrometry-based lipidomics research. Front. Psychiatry 2022, 13, 802710. [Google Scholar] [CrossRef] [PubMed]
- Adibhatla, R.M.; Hatcher, J.F. Role of lipids in brain injury and diseases. Future Lipidol. 2007, 2, 403–422. [Google Scholar] [CrossRef] [PubMed]
- Skinner, E.R. (Ed.) Brain Lipids and Disorders in Biological Psychiatry; Elsevier Science: London, UK, 2002; Volume 35. [Google Scholar]
- Balanzá-Martínez, V.; Fries, G.R.; Colpo, G.D.; Silveira, P.P.; Portella, A.K.; Tabarés-Seisdedos, R.; Kapczinski, F. Therapeutic Use of Omega-3 Fatty Acids in Bipolar Disorder. Expert Rev. Neurother. 2011, 11, 1029–1047. [Google Scholar] [CrossRef]
- McEvoy, J.; Baillie, R.A.; Zhu, H.; Buckley, P.; Keshavan, M.S.; Nasrallah, H.A.; Dougherty, G.G.; Yao, J.K.; Kaddurah-Daouk, R. Lipidomics reveals early metabolic changes in subjects with schizophrenia: Effects of atypical antipsychotics. PLoS ONE 2013, 8, e68717. [Google Scholar] [CrossRef]
- Teixeira, A.L.; Colpo, G.D.; Fries, G.R.; Bauer, I.E.; Selvaraj, S. Biomarkers for bipolar disorder: Current status and challenges ahead. Expert Rev. Neurother. 2019, 19, 67–81. [Google Scholar] [CrossRef]
- Yuan, N.; Chen, Y.; Xia, Y.; Dai, J.; Liu, C. Inflammation-related biomarkers in major psychiatric disorders: A cross-disorder assessment of reproducibility and specificity in 43 meta-analyses. Transl. Psychiatry 2019, 9, 233. [Google Scholar] [CrossRef]
- Quintero, M.; Stanisic, D.; Cruz, G.; Pontes, J.G.M.; Costa, T.B.B.C.; Tasic, L. Metabolomic biomarkers in mental disorders: Bipolar disorder and schizophrenia. Adv. Exp. Med. Biol. 2019, 1118, 271–293. [Google Scholar] [PubMed]
- Brand, S.J.; Moller, M.; Harvey, B.H. A review of biomarkers in mood and psychotic disorders: A dissection of clinical vs. Preclinical correlates. Curr. Neuropharmacol. 2015, 13, 324–368. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Brietzke, E. Omics-Based Biomarkers: Application of Metabolomics in Neuropsychiatric Disorders. Int. J. Neuropsychopharmacol. 2015, 19, yv096. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.C. DSM-IV: Diagnostic and statistical manual of mental disorders. JAMA 1994, 272, 828. [Google Scholar] [CrossRef]
- Gorgens, K.A. Structured clinical interview for DSM-IV (SCID-I/SCID-II). In Encyclopedia of Clinical Neuropsychology; Springer: New York, NY, USA, 2011; pp. 2410–2417. [Google Scholar]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A rating scale for mania: Reliability, validity and sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef]
- Coman, C.; Solari, F.A.; Hentschel, A.; Sickmann, A.; Zahedi, R.P.; Ahrends, R. Simultaneous metabolite, protein, lipid extraction (SIMPLEX): A combinatorial multimolecular omics approach for systems biology. Mol. Cell Proteom. 2016, 15, 1453–1466. [Google Scholar] [CrossRef]
- Smith, C.A.; Want, E.J.; O’Maille, G.; Abagyan, R.; Siuzdak, G. XCMS: Processing mass spectrometry data for metabolite profiling using nonlinear peak alignment, matching, and identification. Anal. Chem. 2006, 78, 779–787. [Google Scholar] [CrossRef]
- Libiseller, G.; Dvorzak, M.; Kleb, U.; Gander, E.; Eisenberg, T.; Madeo, F.; Neumann, S.; Trausinger, G.; Sinner, F.; Pieber, T.; et al. IPO: A tool for automated optimization of XCMS parameters. BMC Bioinform. 2015, 16, 118. [Google Scholar] [CrossRef]
- Kuhl, C.; Tautenhahn, R.; Böttcher, C.; Larson, T.R.; Neumann, S. CAMERA: An integrated strategy for compound spectra extraction and annotation of liquid chromatography/mass spectrometry data sets. Anal. Chem. 2012, 84, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Veselkov, K.A.; Vingara, L.K.; Masson, P.; Robinette, S.L.; Want, E.; Li, J.V.; Barton, R.H.; Boursier-Neyret, C.; Walther, B.; Ebbels, T.M.; et al. Optimized preprocessing of ultra-performance liquid chromatography/mass spectrometry urinary metabolic profiles for improved information recovery. Anal. Chem. 2011, 83, 5864–5872. [Google Scholar] [CrossRef]
- Pang, Z.; Zhou, G.; Ewald, J.; Chang, L.; Hacariz, O.; Basu, N.; Xia, J. Using MetaboAnalyst 5.0 for LC-HRMS spectra processing, multi-omics integration and covariate adjustment of global metabolomics data. Nat. Protoc. 2022, 17, 1735–1761. [Google Scholar] [CrossRef]
- Gil de la Fuente, A.; Godzien, J.; Fernández López, M.; Rupérez, F.J.; Barbas, C.; Otero, A. Knowledge-based metabolite annotation tool: CEU Mass Mediator. J. Pharm. Biomed. Anal. 2018, 154, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Gil-de-la-Fuente, A.; Godzien, J.; Saugar, S.; Garcia-Carmona, R.; Badran, H.; Wishart, D.S.; Barbas, C.; Otero, A. CEU mass mediator 3.0: A metabolite annotation tool. J. Proteome Res. 2019, 18, 797–802. [Google Scholar] [CrossRef]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Gao, J.; Tarcea, V.G.; Karnovsky, A.; Mirel, B.R.; Weymouth, T.E.; Beecher, C.W.; Cavalcoli, J.D.; Athey, B.D.; Omenn, G.S.; Burant, C.F.; et al. Metscape: A Cytoscape plug-in for visualizing and interpreting metabolomic data in the context of human metabolic networks. Bioinformatics 2010, 26, 971–973. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Duren, W.; Evans, C.R.; Burant, C.F.; Michailidis, G.; Karnovsky, A. Sparse network modeling and metscape-based visualization methods for the analysis of large-scale metabolomics data. Bioinformatics 2017, 33, 1545–1553. [Google Scholar] [CrossRef]
- Sud, M.; Fahy, E.; Cotter, D.; Azam, K.; Vadivelu, I.; Burant, C.; Edison, A.; Fiehn, O.; Higashi, R.; Nair, K.S. Metabolomics Workbench: An International Repository for Metabolomics Data and Metadata, Metabolite Standards, Protocols, Tutorials and Training, and Analysis Tools. Nucleic Acids Res. 2016, 44, D463–D470. [Google Scholar] [CrossRef]
- Liu, J.-C.; Yu, H.; Li, R.; Zhou, C.-H.; Shi, Q.-Q.; Guo, L.; He, H. A preliminary comparison of plasma tryptophan metabolites and medium- and long-chain fatty acids in adult patients with major depressive disorder and schizophrenia. Medicina 2023, 59, 413. [Google Scholar] [CrossRef]
- Burton, T.C.; Lv, N.; Tsai, P.; Peñalver Bernabé, B.; Tussing-Humphreys, L.; Xiao, L.; Pandey, G.N.; Wu, Y.; Ajilore, O.A.; Ma, J. Associations between fecal short-chain fatty acids, plasma inflammatory cytokines, and dietary markers with depression and anxiety: Post hoc analysis of the ENGAGE-2 pilot trial. Am. J. Clin. Nutr. 2023, 117, 717–730. [Google Scholar] [CrossRef]
- Brum, M.; Nieberler, M.; Kehrwald, C.; Knopf, K.; Brunkhorst-Kanaan, N.; Etyemez, S.; Allers, K.A.; Bittner, R.A.; Slattery, D.A.; McNeill, R.V.; et al. Phase-and disorder-specific differences in peripheral metabolites of the kynurenine pathway in major depression, bipolar affective disorder and schizophrenia. World J. Biol. Psychiatry, 2023; 1–14, ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.C.; Joaquim, H.P.G.; Talib, L.L.; Serpa, M.H.; Zanetti, M.V.; Gattaz, W.F. Plasma metabolites in first episode psychoses. Schizophr. Res. 2019, 206, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Talib, L.L.; Costa, A.C.; Joaquim, H.P.G.; Pereira, C.A.C.; Van de Bilt, M.T.; Loch, A.A.; Gattaz, W.F. Increased PLA2 activity in individuals at ultra-high risk for psychosis. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 1593–1599. [Google Scholar] [CrossRef]
- Gattaz, W.F.; Köllisch, M.; Thuren, T.; Virtanen, J.A.; Kinnunen, P.K. Increased plasma phospholipase-A2 activity in schizophrenic patients: Reduction after neuroleptic therapy. Biol. Psychiatry 1987, 22, 421–426. [Google Scholar] [CrossRef]
- Gattaz, W.F.; Schmitt, A.; Maras, A. Increased platelet phospholipase A2 activity in schizophrenia. Schizophr. Res. 1995, 16, 1–6. [Google Scholar] [CrossRef]
- Gattaz, W.F.; Brunner, J.; Schmitt, A.; Maras, A. Accelerated breakdown of membrane phospholipids in schizophrenia-implications for the hypofrontality hypothesis. Fortschr. Neurol. Psychiatr. 1994, 62, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Gattaz, W.F.; Valente, K.D.; Raposo, N.R.B.; Vincentiis, S.; Talib, L.L. Increased PLA2 activity in the hippocampus of patients with temporal lobe epilepsy and psychosis. J. Psychiatr. Res. 2011, 45, 1617–1620. [Google Scholar] [CrossRef]
- Smesny, S.; Milleit, B.; Hipler, U.-C.; Milleit, C.; Schäfer, M.R.; Klier, C.M.; Holub, M.; Holzer, I.; E Berger, G.; Otto, M.; et al. Omega-3 fatty acid supplementation changes intracellular phospholipase A2 activity and membrane fatty acid profiles in individuals at ultra-high risk for psychosis. Mol. Psychiatry 2014, 19, 317–324. [Google Scholar] [CrossRef]
- Yao, J.K.; Leonard, S.; Reddy, R.D. Membrane phospholipid abnormalities in postmortem brains from schizophrenic patients. Schizophr. Res. 2000, 42, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Ross, B.M.; Seguin, J.; Sieswerda, L.E. Omega-3 fatty acids as treatments for mental illness: Which disorder and which fatty acid? Lipids Health Dis. 2007, 6, 21. [Google Scholar] [CrossRef] [PubMed]
- Arvindakshan, M.; Sitasawad, S.; Debsikdar, V.; Ghate, M.; Evans, D.; Horrobin, D.F.; Bennett, C.; Ranjekar, P.K.; Mahadik, S.P. Essential polyunsaturated fatty acid and lipid peroxide levels in never-medicated and medicated schizophrenia patients. Biol. Psychiatry 2003, 53, 56–64. [Google Scholar] [CrossRef]
- Harper, K.N.; Hibbeln, J.R.; Deckelbaum, R.; Quesenberry, C.P., Jr.; Schaefer, C.A.; Brown, A.S. Maternal serum docosahexaenoic acid and schizophrenia spectrum disorders in adult offspring. Schizophr. Res. 2011, 128, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Chiappelli, J.; Pocivavsek, A.; Nugent, K.L.; Notarangelo, F.M.; Kochunov, P.; Rowland, L.M.; Schwarcz, R.; Hong, L.E. Stress-induced increase in kynurenic acid as a potential biomarker for patients with schizophrenia and distress intolerance. JAMA Psychiatry 2014, 71, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Schwarcz, R.; Rassoulpour, A.; Wu, H.-Q.; Medoff, D.; Tamminga, C.A.; Roberts, R.C. Increased cortical kynurenate content in schizophrenia. Biol. Psychiatry 2001, 50, 521–530. [Google Scholar] [CrossRef]
- Lin, S.; Li, P.; Qin, J.; Liu, Q.; Zhang, J.; Meng, N.; Jia, C.; Zhu, K.; Lv, D.; Sun, L.; et al. Exploring the key factors of schizophrenia relapse by integrating LC-MS/1H NMR metabolomics and weighted correlation network analysis. Clin. Chim. Acta 2023, 541, 117252. [Google Scholar] [CrossRef]
- Ribeiro, H.C.; Sen, P.; Dickens, A.; Santa Cruz, E.C.; Orešič, M.; Sussulini, A. Metabolomic and proteomic profiling in bipolar disorder patients revealed potential molecular signatures related to hemostasis. Metabolomics 2022, 18, 65. [Google Scholar] [CrossRef]
- Ribeiro, H.C.; Klassen, A.; Pedrini, M.; Carvalho, M.S.; Rizzo, L.B.; Noto, M.N.; Zeni-Graiff, M.; Sethi, S.; Fonseca, F.A.; Tasic, L.; et al. A preliminary study of bipolar disorder type I by mass spectrometry-based serum lipidomics. Psychiatry Res. 2017, 258, 268–273. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | SZ (n = 30) | BD (n = 30) | CT (n = 30) | p † |
|---|---|---|---|---|
| Gender (M/F) | 16/14 | 11/19 | 15/15 | - |
| Age (mean ± SD) | 26.5 ± 6.8 | 26.6 ± 4.4 | 26.5 ± 2.2 | 0.999 |
| Education (mean ± SD) | 11.8 ± 3.0 | 12.6 ± 2.1 | 14.3 ± 2.8 | 0.002 |
| PANSS (mean ± SD) | 78 ± 22 | - | - | - |
| PANSS—Positive symptoms (mean ± SD) | 19 ± 5 | - | - | - |
| PANSS—Negative symptoms (mean ± SD) | 18 ± 8 | - | - | - |
| HAM-D (mean ± SD) | - | 15 ± 8 | - | - |
| YMRS (mean ± SD) | - | 9 ± 8 | - | - |
| Group Comparison | R2X | R2Y | Q2 | |
|---|---|---|---|---|
| BD×CT | p1 | 0.061 | 0.259 | 0.020 |
| o1 | 0.176 | 0.310 | 0.045 | |
| SZ×CT | p1 | 0.064 | 0.415 | 0.292 |
| o1 | 0.127 | 0.299 | 0.169 | |
| BD×SZ | p1 | 0.106 | 0.253 | 0.052 |
| o1 | 0.148 | 0.183 | −0.054 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, A.C.; Riça, L.B.; van de Bilt, M.; Zandonadi, F.S.; Gattaz, W.F.; Talib, L.L.; Sussulini, A. Application of Lipidomics in Psychiatry: Plasma-Based Potential Biomarkers in Schizophrenia and Bipolar Disorder. Metabolites 2023, 13, 600. https://doi.org/10.3390/metabo13050600
Costa AC, Riça LB, van de Bilt M, Zandonadi FS, Gattaz WF, Talib LL, Sussulini A. Application of Lipidomics in Psychiatry: Plasma-Based Potential Biomarkers in Schizophrenia and Bipolar Disorder. Metabolites. 2023; 13(5):600. https://doi.org/10.3390/metabo13050600
Chicago/Turabian StyleCosta, Alana C., Larissa B. Riça, Martinus van de Bilt, Flávia S. Zandonadi, Wagner F. Gattaz, Leda L. Talib, and Alessandra Sussulini. 2023. "Application of Lipidomics in Psychiatry: Plasma-Based Potential Biomarkers in Schizophrenia and Bipolar Disorder" Metabolites 13, no. 5: 600. https://doi.org/10.3390/metabo13050600
APA StyleCosta, A. C., Riça, L. B., van de Bilt, M., Zandonadi, F. S., Gattaz, W. F., Talib, L. L., & Sussulini, A. (2023). Application of Lipidomics in Psychiatry: Plasma-Based Potential Biomarkers in Schizophrenia and Bipolar Disorder. Metabolites, 13(5), 600. https://doi.org/10.3390/metabo13050600