
A Pilot Study on Biochemical Profile of Follicular Fluid in Breast Cancer Patients
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Sample Preparation and NMR Analysis
Multivariate Analysis of NMR Data
2.3. Western Blot Analysis
2.4. Measurement of Chemokine CXCL10
2.5. Statistical Analysis
2.6. Analysis of Discriminating Capability of Metabolites and Proteins
3. Results
3.1. Patient’s Characteristics
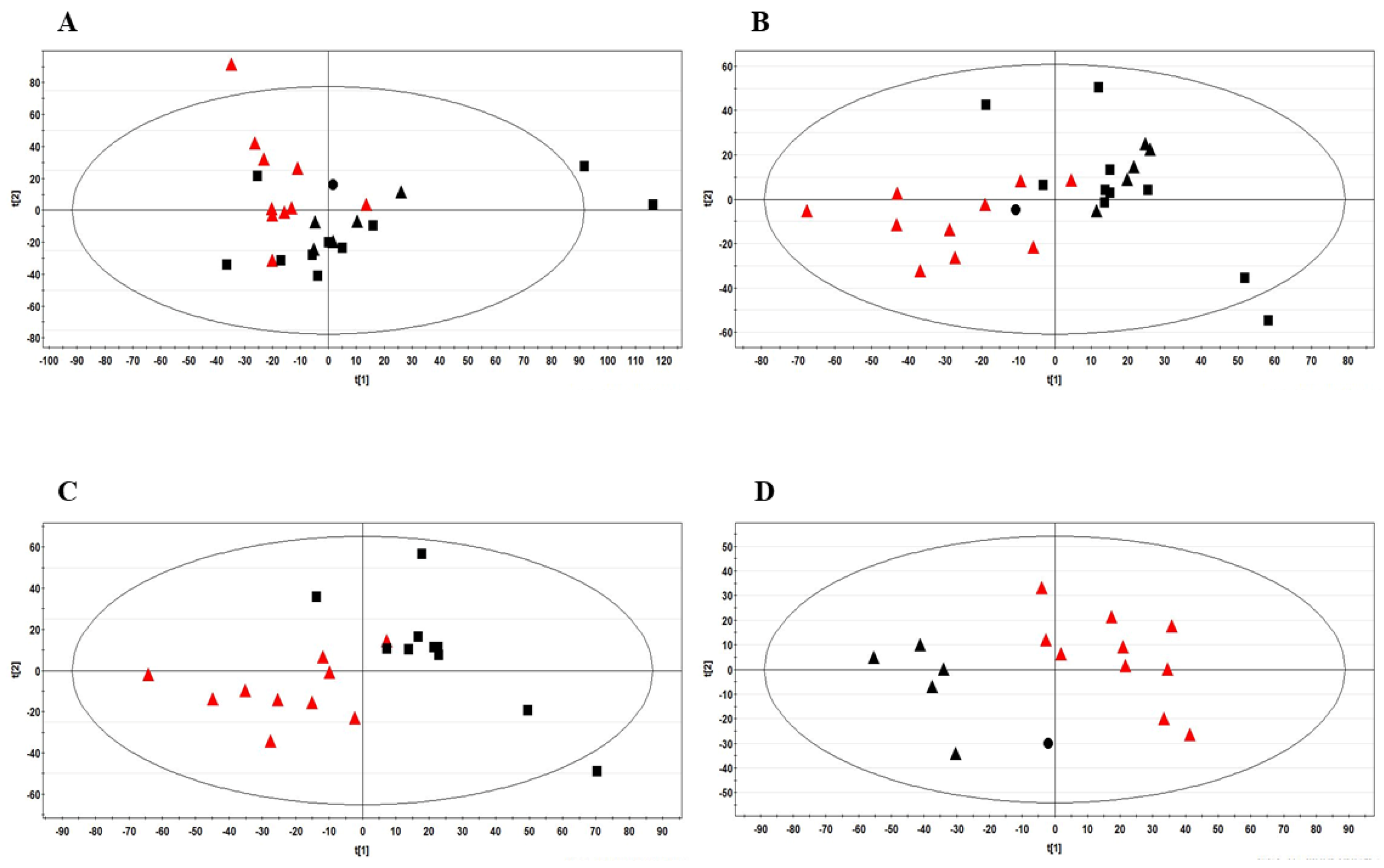
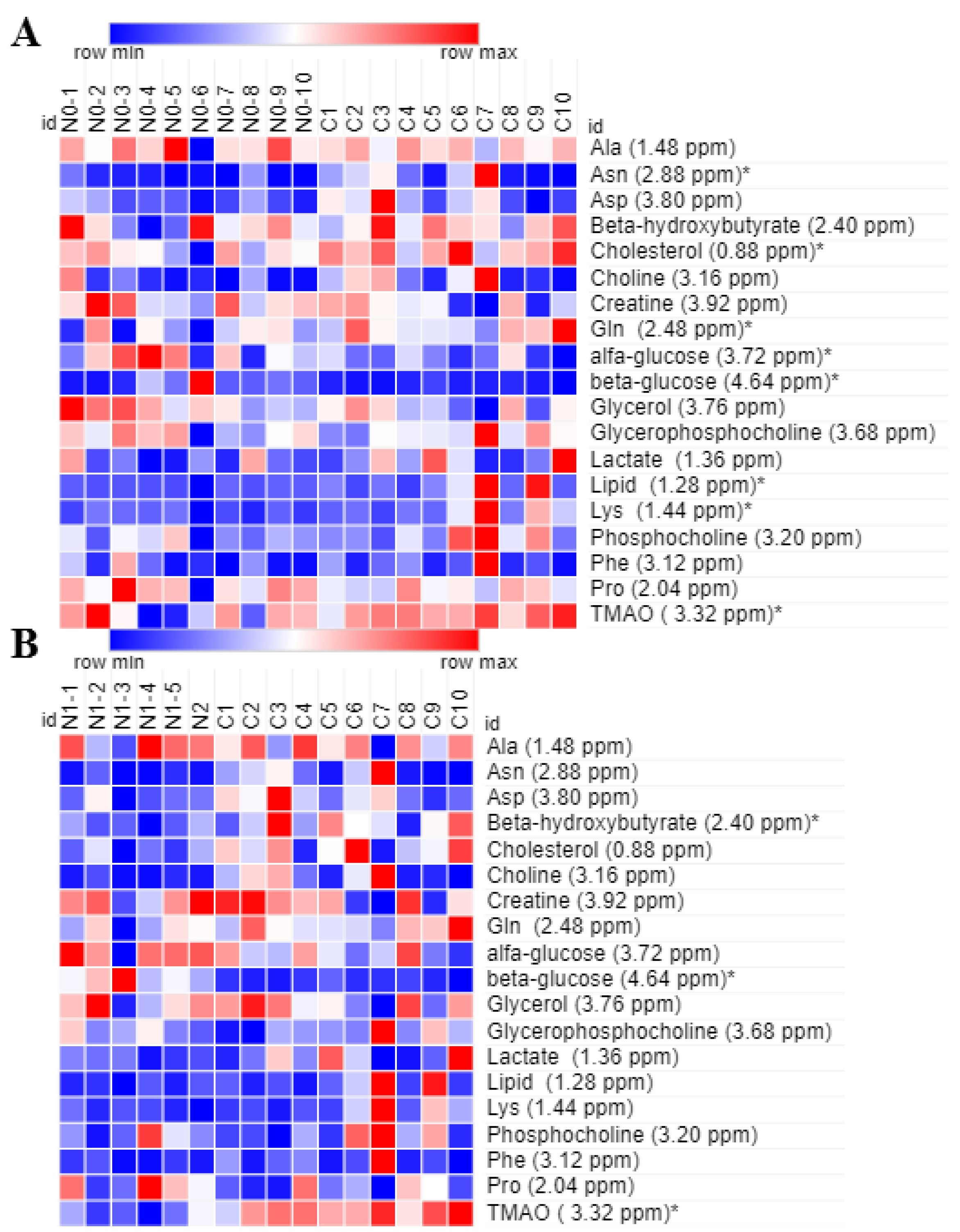
3.2. Identification of Biomarkers in BC Patients
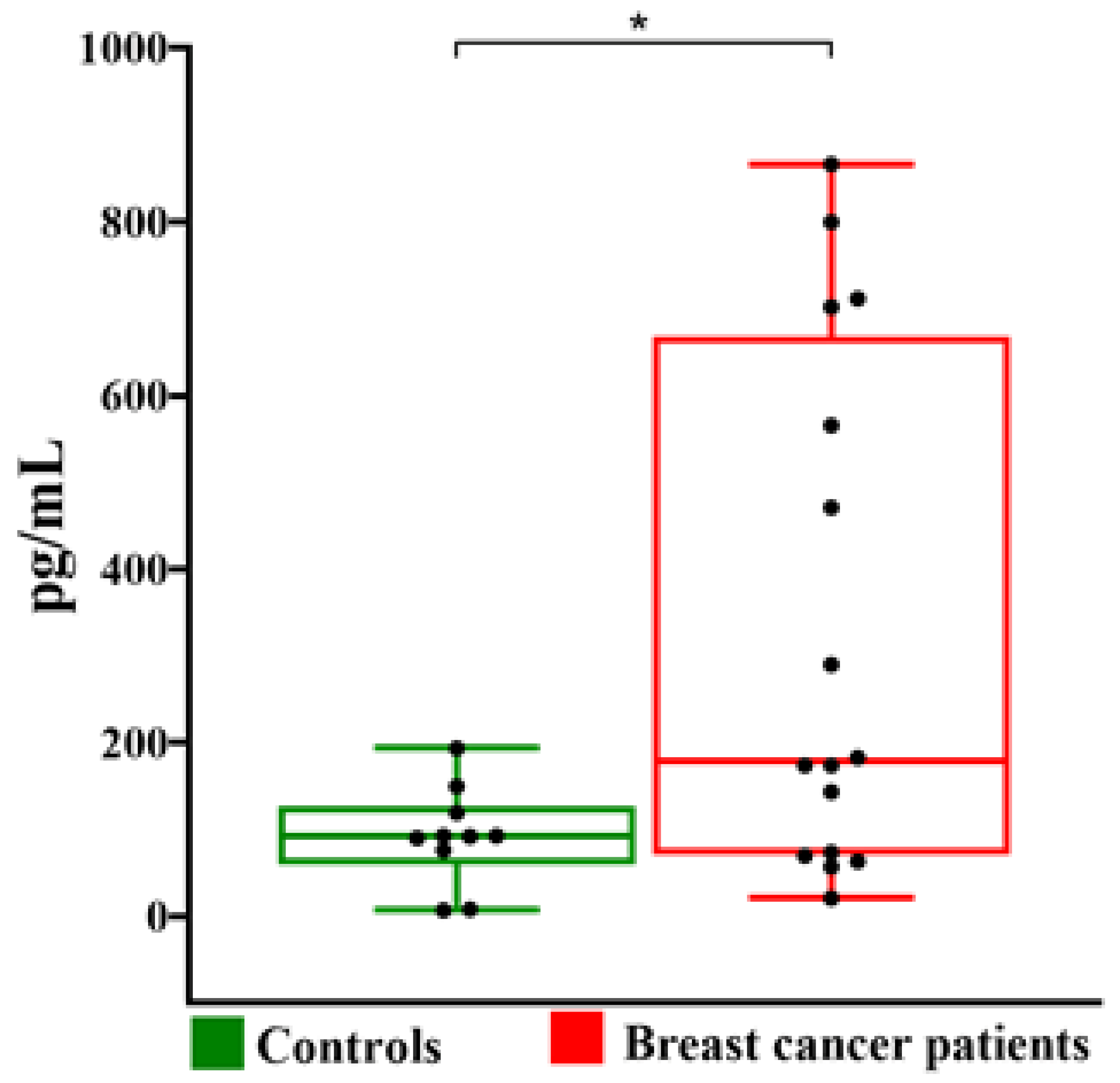
3.3. Follicular Fluid Antioxidant and Anti-Inflammation Biomarkers
3.4. Assessment of Diagnostic Potential and Predictive Ability of Some Identified Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Cancer Atlas. Available online: https://canceratlas.cancer.org/the-burden/breast-cancer/ (accessed on 13 March 2023).
- GLOBOCAN 2020: New Global Cancer Data. Available online: https://www.uicc.org/news/globocan-2020-new-global-cancer-data (accessed on 13 October 2022).
- Polyak, K. Heterogeneity in breast cancer. J. Clin. Investig. 2011, 121, 3786–3788. [Google Scholar] [CrossRef] [PubMed]
- Russnes, H.G.; Navin, N.; Hicks, J.; Borresen-Dale, A.L. Insight into the heterogeneity of breast cancer through next-generation sequencing. J. Clin. Investig. 2011, 121, 3810–3818. [Google Scholar] [CrossRef] [PubMed]
- Kenemans, P.; Verstraeten, R.A.; Verheijen, R.H. Oncogenic pathways in hereditary and sporadic breast cancer. Maturitas 2008, 61, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.J.; Thomassen, M.; Gerdes, A.M.; Kruse, T.A. Hereditary breast cancer: Clinical, pathological and molecular characteristics. Breast Cancer 2014, 8, 145–155. [Google Scholar] [CrossRef]
- ESHRE Guideline Group on Female Fertility Preservation; Anderson, R.A.; Amant, F.; Braat, D.; D’Angelo, A.; Chuva de Sousa Lopes, S.M.; Demeestere, I.; Dwek, S.; Frith, L.; Lambertini, M.; et al. ESHRE guideline: Female fertility preservation. Hum. Reprod. Open 2020, 2020, hoaa052. [Google Scholar]
- Mahajan, N. Fertility preservation in female cancer patients: An overview. J. Hum. Reprod. Sci. 2015, 8, 3–13. [Google Scholar] [CrossRef]
- Vuković, P.; Kasum, M.; Raguž, J.; Lonjak, N.; Bilić Knežević, S.; Orešković, I.; Beketić Orešković, L.; Čehić, E. Fertility preservation in young women with early-stage breast. Acta Clin. Croat. 2019, 58, 147–156. [Google Scholar] [CrossRef]
- Zhang, X.; Niu, J.; Che, T.; Zhu, Y.; Zhang, H.; Qu, J. Fertility preservation in BRCA mutation carriers-efficacy and safety issues: A review. Reprod. Biol. Endocrinol. 2020, 18, 11. [Google Scholar] [CrossRef]
- Dolmans, M.M.; Manavella, D.D. Recent advances in fertility preservation. J. Obstet. Gynaecol. Res. 2019, 45, 266–279. [Google Scholar] [CrossRef]
- McClam, M.; Xiao, S. Preserving oocytes in oncofertility. Biol. Reprod. 2022, 106, 328–337. [Google Scholar] [CrossRef]
- Fabiani, C.; Ferrante, M.G.; Meneghini, C.; Licata, E.; Paciotti, G.; Gallo, M.; Schiavi, M.; Spina, V.; Guarino, A.; Caserta, D.; et al. Female fertility preservation: Impact of cancer on ovarian function and oocyte quality. Int. J. Gynecol. Obstet. 2022, 156, 166–171. [Google Scholar] [CrossRef]
- Rodgers, R.J.; Reid, G.D.; Koch, J.; Deans, R.; Ledger, W.L.; Friedlander, M.; Gilchrist, R.B.; Walters, K.A.; Abbott, J.A. The safety and efficacy of controlled ovarian hyperstimulation for fertility preservation in women with early breast cancer: A systematic review. Hum. Reprod. 2017, 32, 1033–1045. [Google Scholar] [CrossRef]
- Turan, V.; Quinn, M.M.; Dayioglu, N.; Rosen, M.P.; Oktay, K. The impact of malignancy on response to ovarian stimulation for fertility preservation: A meta-analysis. Fertil. Steril. 2018, 110, 1347–1355. [Google Scholar] [CrossRef]
- Quinn, M.M.; Cakmak, H.; Letourneau, J.M.; Cedars, M.I.; Rosen, M.P. Response to ovarian stimulation is not impacted by a breast cancer diagnosis. Hum. Reprod. 2017, 32, 568–574. [Google Scholar] [CrossRef]
- Kaushik, A.K.; DeBerardinis, R.J. Applications of metabolomics to study cancer metabolism. Biochim. Biophys. Acta Rev. Cancer 2018, 1870, 2–14. [Google Scholar] [CrossRef]
- Vignoli, A.; Ghini, V.; Meoni, G.; Licari, C.; Takis, P.G.; Tenori, L.; Turano, P.; Luchinat, C. High-throughput metabolomics by 1D NMR. Angew. Chem. Int. Ed. Engl. 2019, 58, 968–994. [Google Scholar] [CrossRef]
- Prvulovic Bunovic, N.; Sveljo, O.; Kozic, D.; Boban, J. Is elevated choline on magnetic resonance Sspectroscopy a reliable marker of breast lesion malignancy? Front. Oncol. 2021, 11, 610354. [Google Scholar] [CrossRef] [PubMed]
- Shahbazi-Gahrouei, D.; Aminolroayaei, F.; Nematollahi, H.; Ghaderian, M.; Gahrouei, S.S. Advanced magnetic resonance imaging modalities for breast cancer diagnosis: An overview of recent findings and perspectives. Diagnostics 2022, 12, 2741. [Google Scholar] [CrossRef] [PubMed]
- Giskeødegård, G.F.; Madssen, T.S.; Euceda, L.R.; Tessem, M.B.; Moestue, S.A.; Bathen, T.F. NMR-based metabolomics of biofluids in cancer. NMR Biomed. 2019, 32, e3927. [Google Scholar] [CrossRef]
- Claudino, W.M.; Quattrone, A.; Biganzoli, L.; Pestrin, M.; Bertini, I.; Di Leo, A. Metabolomics: Available results, current research projects in breast cancer, and future applications. J. Clin. Oncol. 2007, 25, 2840–2846. [Google Scholar] [CrossRef]
- Hart, C.D.; Tenori, L.; Luchinat, C.; Di Leo, A. Metabolomics in breast cancer: Current status and perspectives. Adv. Exp. Med. Biol. 2016, 882, 217–234. [Google Scholar] [PubMed]
- McCartney, A.; Vignoli, A.; Biganzoli, L.; Love, R.; Tenori, L.; Luchinat, C.; Di Leo, A. Metabolomics in breast cancer: A decade in review. Cancer Treat. Rev. 2018, 67, 88–96. [Google Scholar] [CrossRef]
- Silva, C.; Perestrelo, R.; Silva, P.; Tomás, H.; Câmara, J.S. Breast Cancer Metabolomics: From Analytical platforms to multivariate data analysis. A review. Metabolites 2019, 9, 102. [Google Scholar] [CrossRef]
- Vignoli, A.; Risi, E.; McCartney, A.; Migliaccio, I.; Moretti, E.; Malorni, L.; Luchinat, C.; Biganzoli, L.; Tenori, L. Precision oncology via NMR-based metabolomics: A review on breast cancer. Int. J. Mol. Sci. 2021, 22, 4687. [Google Scholar] [CrossRef]
- Yang, Y.; Zhu, Y.; Li, X.; Zhang, X.; Yu, B. Identification of potential biomarkers and metabolic pathways based on integration of metabolomic and transcriptomic data in the development of breast cancer. Arch. Gynecol. Obstet. 2021, 303, 1599–1606. [Google Scholar] [CrossRef]
- Morad, H.M.; Abou-Elzahab, M.M.; Aref, S.; El-Sokkary, A.M.A. Diagnostic value of 1H NMR-based metabolomics in acute lymphoblastic leukemia, acute myeloid leukemia, and breast cancer. ACS Omega 2022, 7, 8128–8140. [Google Scholar] [CrossRef]
- Vicente-Muñoz, S.; Hunt, B.G.; Lange, T.E.; Wells, S.I.; Waltz, S.E. NMR-based metabolomic analysis identifies RON-DEK-β-catenin dependent metabolic pathways and a gene signature that stratifies breast cancer patient survival. PLoS ONE 2022, 17, e0274128. [Google Scholar] [CrossRef]
- Revelli, A.; Delle Piane, L.; Casano, S.; Molinari, E.; Massobrio, M.; Rinaudo, P. Follicular fluid content and oocyte quality: From single biochemical markers to metabolomics. Reprod. Biol. Endocrinol. 2009, 7, 40. [Google Scholar] [CrossRef]
- Piñero-Sagredo, E.; Nunes, S.; de los Santos, M.J.; Celda, B.; Esteve, V. NMR metabolic profile of human follicular fluid. NMR Biomed. 2010, 23, 485–495. [Google Scholar] [CrossRef]
- Wallace, M.; Cottell, E.; Gibney, M.J.; McAuliffe, F.M.; Wingfield, M.; Brennan, L. An investigation into the relationship between the metabolic profile of follicular fluid, oocyte developmental potential, and implantation outcome. Fertil. Steril. 2012, 97, 1078–1084.e8. [Google Scholar] [CrossRef]
- Santonastaso, M.; Pucciarelli, A.; Costantini, S.; Caprio, F.; Sorice, A.; Capone, F.; Natella, A.; Iardino, P.; Colacurci, N.; Chiosi, E. Metabolomic profiling and biochemical evaluation of the follicular fluid of endometriosis patients. Mol. Biosyst. 2017, 13, 1213–1222. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, L.; Yin, T.L.; Yang, J.; Xiong, C.L. Follicular metabolic changes and effects on oocyte quality in polycystic ovary syndrome patients. Oncotarget 2017, 8, 80472–80480. [Google Scholar] [CrossRef] [PubMed]
- Karaer, A.; Tuncay, G.; Mumcu, A.; Dogan, B. Metabolomics analysis of follicular fluid in women with ovarian endometriosis undergoing in vitro fertilization. Syst. Biol. Reprod. Med. 2019, 65, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Castiglione Morelli, M.A.; Iuliano, A.; Schettini, S.C.A.; Petruzzi, D.; Ferri, A.; Colucci, P.; Viggiani, L.; Cuviello, F.; Ostuni, A. NMR metabolic profiling of follicular fluid for investigating the different causes of female infertility: A pilot study. Metabolomics 2019, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Castiglione Morelli, M.A.; Iuliano, A.; Schettini, S.C.A.; Petruzzi, D.; Ferri, A.; Colucci, P.; Viggiani, L.; Cuviello, F.; Ostuni, A. NMR metabolomics study of follicular fluid in women with cancer resorting to fertility preservation. J. Assist. Reprod. Genet. 2018, 35, 2063–2070. [Google Scholar] [CrossRef]
- Oktay, K.; Türkçüoğlu, I.; Rodriguez-Walberg, K.A. GnRH agonist trigger for women with breast cancer undergoing fertility preservation by aromatase inhibitor/FSH stimulation. Reprod. Biomed. Online 2010, 20, 783–788. [Google Scholar] [CrossRef]
- La Marca, A.; Grisendi, V.; Giulini, S.; Argento, C.; Tirelli, A.; Dondi, G.; Papaleo, E.; Volpe, A. Individualization of the FSH starting dose in IVF/ICSI cycles using the antral follicle count. J. Ovarian Res. 2013, 6, 11. [Google Scholar] [CrossRef]
- Baird, L.; Yamamoto, M. The molecular mechanisms regulating the KEAP1-NRF2 pathway. Mol. Cell. Biol. 2020, 40, e00099-20. [Google Scholar] [CrossRef]
- Saha, S.; Buttari, B.; Panieri, E.; Profumo, E.; Saso, L. An overview of Nrf2 signaling pathway and its role in inflammation. Molecules 2020, 25, 5474. [Google Scholar] [CrossRef]
- Da Broi, M.G.; Giorgi, V.S.I.; Wang, F.; Keefe, D.L.; Albertini, D.; Navarro, P.A. Influence of follicular fluid and cumulus cells on oocyte quality: Clinical implications. J. Assist. Reprod. Genet. 2018, 35, 735–751. [Google Scholar] [CrossRef]
- Bianchi, L.; Gagliardi, A.; Landi, C.; Focarelli, R.; De Leo, V.; Luddi, A.; Bini, L.; Piomboni, P. Protein pathways working in human follicular fluid: The future for tailored IVF? Expert Rev. Mol. Med. 2016, 18, e9. [Google Scholar] [CrossRef]
- von Wolff, M.; Kollmann, Z.; Flück, C.E.; Stute, P.; Marti, U.; Weiss, B.; Bersinger, N.A. Gonadotrophin stimulation for in vitro fertilization significantly alters the hormone milieu in follicular fluid: A comparative study between natural cycle IVF and conventional IVF. Hum. Reprod. 2014, 29, 1049–1057. [Google Scholar] [CrossRef]
- Castiglione Morelli, M.A.; Iuliano, A.; Schettini, S.C.A.; Petruzzi, D.; Ferri, A.; Colucci, P.; Viggiani, L.; Cuviello, F.; Ostuni, A. Metabolic changes in follicular fluids of patients treated with recombinant versus urinary human chorionic gonadotropin for triggering ovulation in assisted reproductive technologies: A metabolomics pilot study. Arch. Gynecol. Obstet. 2020, 302, 741–751. [Google Scholar] [CrossRef]
- Palini, S.; Benedetti, S.; Tagliamonte, M.C.; De Stefani, S.; Primiterra, M.; Polli, V.; Rocchi, P.; Catalani, S.; Battistelli, S.; Canestrari, F.; et al. Influence of ovarian stimulation for IVF/ICSI on the antioxidant defence system and relationship to outcome. Reprod. Biomed. Online 2014, 29, 65–71. [Google Scholar] [CrossRef]
- Brinca, A.T.; Ramalhinho, A.C.; Sousa, Â.; Oliani, A.H.; Breitenfeld, L.; Passarinha, L.A.; Gallardo, E. Follicular Fluid: A powerful tool for the understanding and diagnosis of polycystic ovary syndrome. Biomedicines 2022, 10, 1254. [Google Scholar] [CrossRef]
- Castiglione Morelli, M.A.; Iuliano, A.; Schettini, S.C.A.; Ferri, A.; Colucci, P.; Viggiani, L.; Matera, I.; Ostuni, A. Are the follicular fluid characteristics of recovered coronavirus disease 2019 patients different from those of vaccinated women approaching in vitro fertilization? Front. Physiol. 2022, 13, 840109. [Google Scholar] [CrossRef]
- Smith, B.; Schafer, X.L.; Ambeskovic, A.; Spencer, C.M.; Land, H.; Munger, J. Addiction to coupling of the Warburg effect with glutamine catabolism in cancer cells. Cell Rep. 2016, 17, 821–836. [Google Scholar] [CrossRef]
- Men, Y.L.L.; Zhang, F.; Kong, X.; Zhang, W.; Hao, C.; Wang, G. Evaluation of heavy metals and metabolites in the urine of patients with breast cancer. Oncol. Lett. 2020, 19, 1331–1337. [Google Scholar] [CrossRef]
- El Ansari, R.; McIntyre, A.; Craze, M.L.; Ellis, I.O.; Rakha, E.A.; Green., A.R. Altered glutamine metabolism in breast cancer; subtype dependencies and alternative adaptations. Histopathology 2018, 72, 183–190. [Google Scholar] [CrossRef]
- Hong, J.; Lee, E. Intrafollicular amino acid concentration and the effect of amino acids in a defined maturation medium on porcine oocyte maturation, fertilization, and preimplantation development. Theriogenology 2007, 68, 728–773. [Google Scholar] [CrossRef]
- Bahrami, M.; Cottee, P.A. Culture conditions for in vitro maturation of oocytes–A review. Reprod. Breed. 2022, 2, 31–36. [Google Scholar] [CrossRef]
- DeBerardinis, R.; Cheng, T. Q’s next: The diverse functions of glutamine in metabolism, cell biology and cancer. Oncogene 2010, 29, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhou, C.; Sun, J.; Zhang, Q.; Lai, D. Glutamine and norepinephrine in follicular fluid synergistically enhance the antioxidant capacity of human granulosa cells and the outcome of IVF-ET. Sci. Rep. 2022, 12, 9936. [Google Scholar] [CrossRef] [PubMed]
- Miao, S.B.; Feng, Y.R.; Wang, X.D.; Lian, K.Q.; Meng, F.Y.; Song, G.; Yuan, J.C.; Geng, C.P.; Wu, X.H. Glutamine as a potential noninvasive biomarker for human embryo selection. Reprod. Sci. 2022, 29, 1721–1729. [Google Scholar] [CrossRef]
- Greten, F.R.; Grivennikov, S.I. Inflammation and cancer: Triggers, mechanisms, and consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef]
- Xing, F.; Hu, Q.; Qin, Y.; Xu, J.; Zhang, B.; Yu, X.; Wang, W. The relationship of redox with hallmarks of cancer: The importance of homeostasis and context. Front. Oncol. 2022, 12, 862743. [Google Scholar] [CrossRef]
- Duffy, D.M.; Ko, C.; Jo, M.; Brannstrom, M.; Curry, T.E. Ovulation: Parallels with inflammatory processes. Endocr. Rev. 2019, 40, 369–416. [Google Scholar] [CrossRef]
- Adamczak, R.; Ukleja-Sokołowska, N.; Lis, K.; Dubiel, M. Function of follicular cytokines: Roles played during maturation, development and implantation of embryo. Medicina 2021, 57, 1251. [Google Scholar] [CrossRef]
- Zavatta, A.; Parisi, F.; Mandò, C.; Scaccabarozzi, C.; Savasi, V.M.; Cetin, I. Role of inflammaging on the reproductive function and pregnancy. Clin. Rev. Allergy Immunol. 2022, 64, 145–160. [Google Scholar] [CrossRef]
- Liu, P.; Zhang, X.; Hu, J.; Cui, L.; Zhao, S.; Jiao, X.; Qin, Y. Dysregulated cytokine profile associated with biochemical premature ovarian insufficiency. Am. J. Reprod. Immunol. 2020, 84, e13292. [Google Scholar] [CrossRef]
- Velez, L.M.; Seldin, M.; Motta, A.B. Inflammation and reproductive function in women with polycystic ovary syndrome. Biol. Reprod. 2021, 104, 1205–1217. [Google Scholar] [CrossRef]
- Nagarsheth, N.; Wicha, M.S.; Zou, W. Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat. Rev. Immunol. 2017, 17, 559–572. [Google Scholar] [CrossRef]
- Masih, M.; Agarwal, S.; Kaur, R.; Gautam, P.K. Role of chemokines in breast cancer. Cytokine 2022, 155, 155909. [Google Scholar] [CrossRef]
- Kim, M.; Choi, H.Y.; Woo, J.W.; Chung, Y.R.; Park, S.Y. Role of CXCL10 in the progression of in situ to invasive carcinoma of the breast. Sci. Rep. 2021, 11, 18007. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breast Cancer | Healthy Control | |
|---|---|---|
| Number of patients | 16 | 10 |
| Age (years) | 33.5 (5.0) | 36.0 (4.0) |
| FSH (UI/mL) | 6.8 (1.2) | 6.9 (2.0) |
| AMH (ng/mL) | 2.8 (1.5) | 4.1 (4.4) |
| AFC | 12.2 (7.0) | 13.2 (4.0) |
| Estradiol (pg/mL) * | 599.2 (410.4) | 1721.7 (1229.0) |
| Progesterone (ng/mL) | 1.9 (1.1) | 1.3 (0.9) |
| BMI (kg/m2) | 22.3 (2.8) | 22.2 (3.4) |
| Follicles monitored | 13.2 (9.0) | 11.8 (4.4) |
| Total oocytes collected | 9.3 (7.3) | 8.8 (5.9) |
| MII oocytes | 6.3 (6.3) | 6.6 (5.2) |
| Breast cancer stadiation | ||
| T1N0M0 | 4 | |
| T1N1M0 | 1 | |
| T1aN1M0 | 1 | |
| T2N0M0 | 4 | |
| T2N1M0 | 1 | |
| T2N2M0 | 1 | |
| T3N0M0 | 2 | |
| T3N1M0 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castiglione Morelli, M.A.; Iuliano, A.; Matera, I.; Viggiani, L.; Schettini, S.C.A.; Colucci, P.; Ostuni, A. A Pilot Study on Biochemical Profile of Follicular Fluid in Breast Cancer Patients. Metabolites 2023, 13, 441. https://doi.org/10.3390/metabo13030441
Castiglione Morelli MA, Iuliano A, Matera I, Viggiani L, Schettini SCA, Colucci P, Ostuni A. A Pilot Study on Biochemical Profile of Follicular Fluid in Breast Cancer Patients. Metabolites. 2023; 13(3):441. https://doi.org/10.3390/metabo13030441
Chicago/Turabian StyleCastiglione Morelli, Maria A., Assunta Iuliano, Ilenia Matera, Licia Viggiani, Sergio C. A. Schettini, Paola Colucci, and Angela Ostuni. 2023. "A Pilot Study on Biochemical Profile of Follicular Fluid in Breast Cancer Patients" Metabolites 13, no. 3: 441. https://doi.org/10.3390/metabo13030441
APA StyleCastiglione Morelli, M. A., Iuliano, A., Matera, I., Viggiani, L., Schettini, S. C. A., Colucci, P., & Ostuni, A. (2023). A Pilot Study on Biochemical Profile of Follicular Fluid in Breast Cancer Patients. Metabolites, 13(3), 441. https://doi.org/10.3390/metabo13030441