
Myoinositol vs. Metformin in Women with Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial



Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcomes
2.2. Blood Samples and Assays
2.3. Menstrual Cycle, Ovarian Ultrasound
2.4. FG Score
2.5. Adverse Effects and Pregnancies
2.6. Questionnaires
2.7. Statistics
2.8. Ethical Approval
3. Results
3.1. Metabolic Changes
3.2. Anthropometric Values
3.3. Cycle Length
3.4. FG Score
3.5. Gonadotrophins, Sex Hormones, and AMH
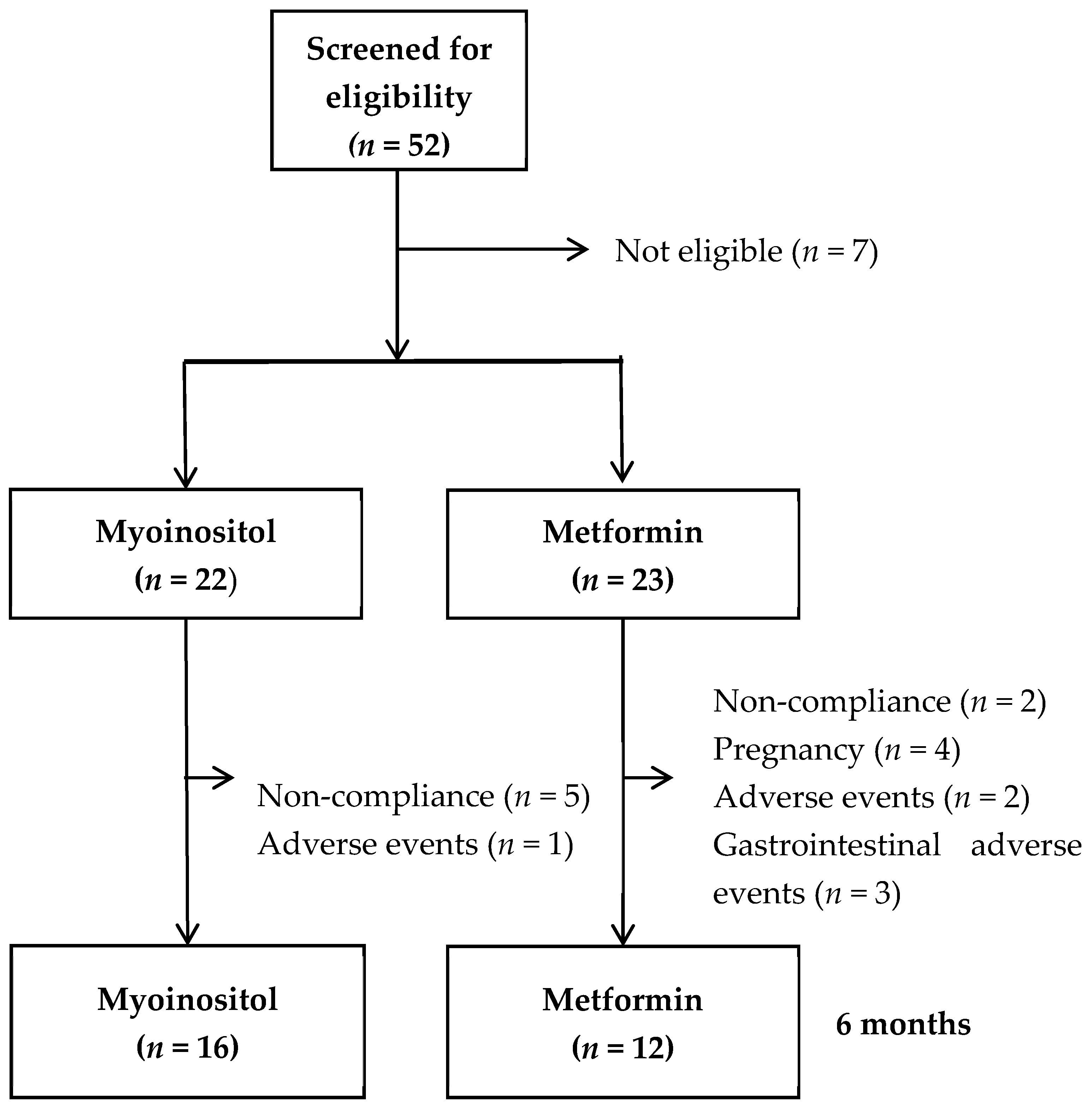
3.6. Adverse Effects, Non-Completion, and Pregnancy
3.7. Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bozdag, G.; Mumusoglu, S.; Zengin, D.; Karabulut, E.; Yildiz, B.O. The prevalence and phenotypic features of polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. (Oxf. Engl.) 2016, 31, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moghetti, P. Insulin Resistance and Polycystic Ovary Syndrome. Curr. Pharm. Des. 2016, 22, 5526–5534. [Google Scholar] [CrossRef] [PubMed]
- Glintborg, D.; Andersen, M. An update on the pathogenesis, inflammation, and metabolism in hirsutism and polycystic ovary syndrome. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2010, 26, 281–296. [Google Scholar] [CrossRef] [PubMed]
- Rubin, K.H.; Glintborg, D.; Nybo, M.; Abrahamsen, B.; Andersen, M. Development and Risk Factors of Type 2 Diabetes in a Nationwide Population of Women With Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2017, 102, 3848–3857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, X.; Ji, Y.; Chan, C.L.W.; Chan, C.H.Y. The mental health of women with polycystic ovary syndrome: A systematic review and meta-analysis. Arch. Women Ment. Health 2021, 24, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Altinok, M.L.; Glintborg, D.; Depont Christensen, R.; Hallas, J.; Andersen, M. Prescription of antidepressants is increased in Danish patients with polycystic ovary syndrome and is associated with hyperandrogenism. A population-based cohort study. Clin. Endocrinol. (Oxf.) 2014, 80, 884–889. [Google Scholar] [CrossRef]
- Clements, R.S., Jr.; Darnell, B. Myo-inositol content of common foods: Development of a high-myo-inositol diet. Am. J. Clin. Nutr. 1980, 33, 1954–1967. [Google Scholar] [CrossRef] [Green Version]
- Facchinetti, F.; Unfer, V.; Dewailly, D.; Kamenov, Z.A.; Diamanti-Kandarakis, E.; Laganà, A.S.; Nestler, J.E.; Soulage, C.O.; For the Group of Inositol in PCOS and Reproduction. Inositols in Polycystic Ovary Syndrome: An Overview on the Advances. Trends Endocrinol. Metab. 2020, 31, 435–447. [Google Scholar] [CrossRef]
- Zheng, X.; Lin, D.; Zhang, Y.; Lin, Y.; Song, J.; Li, S.; Sun, Y. Inositol supplement improves clinical pregnancy rate in infertile women undergoing ovulation induction for ICSI or IVF-ET. Medicine (Baltimore) 2017, 96, e8842. [Google Scholar] [CrossRef]
- Kamenov, Z.; Kolarov, G.; Gateva, A.; Carlomagno, G.; Genazzani, A.D. Ovulation induction with myo-inositol alone and in combination with clomiphene citrate in polycystic ovarian syndrome patients with insulin resistance. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2015, 31, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Unfer, V.; Nestler, J.E.; Kamenov, Z.A.; Prapas, N.; Facchinetti, F. Effects of Inositol(s) in Women with PCOS: A Systematic Review of Randomized Controlled Trials. Int. J. Endocrinol. 2016, 2016, 1849162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, D.; Minozzi, G.; Minozzi, E.; Guaraldi, C. Metabolic and hormonal effects of myo-inositol in women with polycystic ovary syndrome: A double-blind trial. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 105–110. [Google Scholar]
- Fraison, E.; Kostova, E.; Moran, L.J.; Bilal, S.; Ee, C.C.; Venetis, C.; Costello, M.F. Metformin versus the combined oral contraceptive pill for hirsutism, acne, and menstrual pattern in polycystic ovary syndrome. Cochrane Database Syst. Rev. 2020, 8, Cd005552. [Google Scholar] [PubMed]
- Morley, L.C.; Tang, T.; Yasmin, E.; Norman, R.J.; Balen, A.H. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst. Rev. 2017, 11, Cd003053. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. (Oxf. Engl.) 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [Green Version]
- Guan, Y.; Wang, D.; Bu, H.; Zhao, T.; Wang, H. The Effect of Metformin on Polycystic Ovary Syndrome in Overweight Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Endocrinol. 2020, 2020, 5150684. [Google Scholar] [CrossRef]
- Garcia-Hernandez, S.C.; Porchia, L.M.; Pacheco-Soto, B.T.; López-Bayghen, E.; Gonzalez-Mejia, M.E. Metformin does not improve insulin sensitivity over hypocaloric diets in women with polycystic ovary syndrome: A systematic review of 12 studies. Gynecol. Endocrinol. 2021, 37, 968–976. [Google Scholar] [CrossRef]
- Romualdi, D.; Giuliani, M.; Cristello, F.; Fulghesu, A.M.; Selvaggi, L.; Lanzone, A.; Guido, M. Metformin effects on ovarian ultrasound appearance and steroidogenic function in normal-weight normoinsulinemic women with polycystic ovary syndrome: A randomized double-blind placebo-controlled clinical trial. Fertil. Steril. 2010, 93, 2303–2310. [Google Scholar] [CrossRef]
- Harris-Glocker, M.; Davidson, K.; Kochman, L.; Guzick, D.; Hoeger, K. Improvement in quality-of-life questionnaire measures in obese adolescent females with polycystic ovary syndrome treated with lifestyle changes and oral contraceptives, with or without metformin. Fertil. Steril. 2010, 93, 1016–1019. [Google Scholar] [CrossRef] [Green Version]
- Altinok, M.L.; Ravn, P.; Andersen, M.; Glintborg, D. Effect of 12-month treatment with metformin and/or oral contraceptives on health-related quality of life in polycystic ovary syndrome. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2018, 34, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Domecq, J.P.; Prutsky, G.; Mullan, R.J.; Sundaresh, V.; Wang, A.T.; Erwin, P.J.; Welt, C.; Ehrmann, D.; Montori, V.M.; Murad, M.H. Adverse effects of the common treatments for polycystic ovary syndrome: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2013, 98, 4646–4654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fruzzetti, F.; Perini, D.; Russo, M.; Bucci, F.; Gadducci, A. Comparison of two insulin sensitizers, metformin and myo-inositol, in women with polycystic ovary syndrome (PCOS). Gynecol. Endocrinol. 2017, 33, 39–42. [Google Scholar] [CrossRef]
- Tagliaferri, V.; Romualdi, D.; Immediata, V.; De Cicco, S.; Di Florio, C.; Lanzone, A.; Guido, M. Metformin vs myoinositol: Which is better in obese polycystic ovary syndrome patients? A randomized controlled crossover study. Clin. Endocrinol. (Oxf.) 2017, 86, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Shokrpour, M.; Foroozanfard, F.; Afshar Ebrahimi, F.; Vahedpoor, Z.; Aghadavod, E.; Ghaderi, A.; Asemi, Z. Comparison of myo-inositol and metformin on glycemic control, lipid profiles, and gene expression related to insulin and lipid metabolism in women with polycystic ovary syndrome: A randomized controlled clinical trial. Gynecol. Endocrinol. 2019, 35, 406–411. [Google Scholar] [CrossRef]
- Jamilian, M.; Farhat, P.; Foroozanfard, F.; Afshar Ebrahimi, F.; Aghadavod, E.; Bahmani, F.; Badehnoosh, B.; Jamilian, H.; Asemi, Z. Comparison of myo-inositol and metformin on clinical, metabolic and genetic parameters in polycystic ovary syndrome: A randomized controlled clinical trial. Clin. Endocrinol. (Oxf.) 2017, 87, 194–200. [Google Scholar] [CrossRef]
- Nehra, J.K.J.; Singhal, S.R.; Ghalaut, V.S. A comparative study of myo inositol versus metformin on biochemical profile in polycystic ovarian syndrome in women. Int. J. Pharm. Sci. Res. 2017, 8, 1664–1670. [Google Scholar]
- Jamilian, H.; Jamilian, M.; Foroozanfard, F.; Afshar Ebrahimi, F.; Bahmani, F.; Asemi, Z. Comparison of myo-inositol and metformin on mental health parameters and biomarkers of oxidative stress in women with polycystic ovary syndrome: A randomized, double-blind, placebo-controlled trial. J. Psychosom. Obstet. Gynaecol. 2018, 39, 307–314. [Google Scholar] [CrossRef]
- Angik, R.; Jajoo, S.S.; Hariharan, C.; Chimote, A. A comparative study of metabolic and hormonal effects of myoinositol vs. metformin in women with polycystic ovary syndrome: A randomised controlled trial. J. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Leo, V. A Combined Treatment with Myo-Inositol and Monacolin K Improve the Androgen and Lipid Profiles of Insulin-Resistant PCOS Patients. J. Metab. Syndr. 2013, 2, 1000127. [Google Scholar]
- Zhao, H.; Xing, C.; Zhang, J.; He, B. Comparative efficacy of oral insulin sensitizers metformin, thiazolidinediones, inositol, and berberine in improving endocrine and metabolic profiles in women with PCOS: A network meta-analysis. Reprod. Health 2021, 18, 171. [Google Scholar] [CrossRef]
- Facchinetti, F.; Orrù, B.; Grandi, G.; Unfer, V. Short-term effects of metformin and myo-inositol in women with polycystic ovarian syndrome (PCOS): A meta-analysis of randomized clinical trials. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2019, 35, 198–206. [Google Scholar] [CrossRef]
- Free and bioavailable testosterone calculator. Available online: http://www.issam.ch/freetesto.htm (accessed on 30 August 2021).
- Rosenfield, R.L. Clinical practice. Hirsutism. N. Engl. J. Med. 2005, 353, 2578–2588. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Mahey, R.; Kachhawa, G.; Khadgawat, R.; Vanamail, P.; Kriplani, A.; Kriplani, A. Comparison of metformin plus myoinositol vs metformin alone in PCOS women undergoing ovulation induction cycles: Randomized controlled trial. Gynecol. Endocrinol. 2019, 35, 511–514. [Google Scholar] [CrossRef]
- Glueck, C.J.; Goldenberg, N. Characteristics of obesity in polycystic ovary syndrome: Etiology, treatment, and genetics. Metabolism 2019, 92, 108–120. [Google Scholar] [CrossRef]
- Moran, L.J.; Pasquali, R.; Teede, H.J.; Hoeger, K.M.; Norman, R.J. Treatment of obesity in polycystic ovary syndrome: A position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil. Steril. 2009, 92, 1966–1982. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; Falbo, A.; Russo, T.; Orio, F.; Tolino, A.; Zullo, F. Systemic and local effects of metformin administration in patients with polycystic ovary syndrome (PCOS): Relationship to the ovulatory response. Hum. Reprod. 2010, 25, 1005–1013. [Google Scholar] [CrossRef] [Green Version]
- Hahn, S.; Janssen, O.E.; Tan, S.; Pleger, K.; Mann, K.; Schedlowski, M.; Kimmig, R.; Benson, S.; Balamitsa, E.; Elsenbruch, S. Clinical and psychological correlates of quality-of-life in polycystic ovary syndrome. Eur. J. Endocrinol. 2005, 153, 853–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coffey, S.; Bano, G.; Mason, H.D. Health-related quality of life in women with polycystic ovary syndrome: A comparison with the general population using the Polycystic Ovary Syndrome Questionnaire (PCOSQ) and the Short Form-36 (SF-36). Gynecol. Endocrinol. 2006, 22, 80–86. [Google Scholar] [CrossRef]
- Kolotkin, R.L.; Meter, K.; Williams, G.R. Quality of life and obesity. Obes. Rev. 2001, 2, 219–229. [Google Scholar] [CrossRef]
- Stewart, P.M.; Shackleton, C.H.; Beastall, G.H.; Edwards, C.R. 5 alpha-reductase activity in polycystic ovary syndrome. Lancet (Lond. Engl.) 1990, 335, 431–433. [Google Scholar] [CrossRef]
- Kolhe, J.V.; Chhipa, A.S.; Butani, S.; Chavda, V.; Patel, S.S. PCOS and Depression: Common Links and Potential Targets. Reprod. Sci. (Thousand Oaks Calif) 2021, 29, 3106–3123. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Intervention | Myoinositol (n = 16) | Metformin (n = 12) | |||||
|---|---|---|---|---|---|---|---|
| Time | Baseline | 6 Months | Δ p | Baseline | 6 Months | Δ p | Δ vs. Δ p |
| HOMA-IR (pmol mmol L−2) | 28.5 (19.6;45.6) | 33.7 (27.1;49.6) | 0.31 | 30.9 (24.9;32.4) | 18.8 (14.3;29.6) | 0.11 | 0.09 |
| Insulin (pmol/L) | 126 (85;190) | 119 (78;219) | 0.38 | 117 (112;143) | 80 (65;121) | 0.21 | 0.13 |
| Glucose (mmol/L) | 5.2 (5.0;5.4) | 5.4 (5.3;5.7) | 0.00 | 5.3 (5.1;5.7) | 5.2 (4.8;5.3) | 0.04 | 0.00 |
| HbA1c (mmol/mol) | 32.0 (30.0;36.0) | 33.0 (31.0;34.0) | 0.18 | 33.5 (32.0;35) | 32.0 (31.5;33.5) | 0.47 | 0.12 |
| Triglycerides (mmol/L) | 1.2 (1.0;1.4) | 1.3 (1.0;1.6) | 0.09 | 1.0 (0.9;1.2) | 1.0 (0.8;1.5) | 0.81 | 0.25 |
| HDL (mmol/L) | 1.2 (1.0;1.3) | 1.2 (1.1;1.3) | 0.92 | 1.3 (1.2;1.4) | 1.4 (1.2;1.6) | 0.04 | 0.07 |
| LDL (mmol/L) | 2.9 (2.4;3.2) | 2.9 (2.5;3.1) | 0.44 | 3.1 (2.6;3.3) | 2.9 (2.6;3.3) | 0.93 | 0.64 |
| Cholesterol (mmol/L) | 4.6 (4.1;4.9) | 4.7 (4.1;5.1) | 0.46 | 4.8 (4.3;5.2) | 4.8 (4.2;5.3) | 0.69 | 0.42 |
| Age (years) | 25 (22;34) | - | 27 (24;33) | - | - | ||
| Weight (kg) | 96.7 (84.5;107.6) | 94.4 (84.9;107.0) | 0.98 | 99.8 (86.4;108.9) | 93.7(81.7;106.8) | 0.00 | 0.02 |
| BMI (kg/m2) | 34.2 (30.9;37.2) | 34.5 (29.9;36.8) | 0.96 | 35.2 (31.0;39.8) | 32.8 (29.8;38.5) | 0.00 | 0.02 |
| Waist (cm) | 103 (93;108) | 100 (93;104) | 0.31 | 99 (92;106) | 100 (90;105) | 0.41 | 0.62 |
| Hip (cm) | 122 (108;125) | 119 (110;125) | 0.84 | 123 (114;129) | 119 (110;128) | 0.06 | 0.11 |
| Cycle length (days) | 45 (35;175) | 36 (32;60) | 0.03 | 47 (35;82) | 34 (28;37) | 0.03 | 0.92 |
| FG score | 6 (0;17) | 8 (3;12) | 0.79 | 6 (2;12) | 6 (2;12) | 0.40 | 0.49 |
| SHBG (nmol/L) | 30 (18;46) | 30 (14;37) | 0.78 | 35 (27;57) | 38 (29;44) | 0.88 | 0.92 |
| Free testosterone (nmol/L) | 0.032 (0.025;0.038) | 0.028 (0.025;0.045) | 0.89 | 0.027 (0.019;0.035) | 0.021 (0.017;0.028) | 0.06 | 0.70 |
| Total testosterone (nmol/L) | 1.5 (1.1;1.7) | 1.2 (1.0;1.8) | 0.39 | 1.5 (1.3;1.8) | 1.2 (0.9;1.7) | 0.10 | 0.28 |
| AMH (pmol/L) | 37.7 (25.1;51.8) | 36.0 (31.6;44.4) | 0.96 | 38.9 (33.9;78.4) | 38.3 (25.8;57.0) | 0.46 | 0.74 |
| FSH (IU/L) | 5.8 (4.6;7.0) | 5.4 (4.9;7.0) | 0.67 | 5.4 (3.3;6.0) | 5.7 (4.3;6.6) | 0.26 | 0.26 |
| LH (IU/L) | 8.9 (6.2;11.8) | 12.0 (9.4;16.0) | 0.15 | 12.5 (8.2;16.0) | 10.4 (5.0;13.5) | 0.16 | 0.04 |
| Estradiol (nmol/L) | 0.19 (0.14;0.41) | 0.18 (0.15;0.25) | 0.16 | 0.26 (0.17;0.70) | 0.19 (0.13;0.29) | 0.08 | 0.34 |
| Intervention | Myoinositol (n = 14) | Metformin (n = 12) | |||||
|---|---|---|---|---|---|---|---|
| Time | Baseline | 6 Months | Δ p | Baseline | 6 Months | Δ p | Δ vs. Δ p |
| SF-36 | |||||||
| Physical functioning | 90 (75;95) | 90 (80;95) | 0.14 | 90 (85;95) | 95 (85;100) | 0.16 | 0.78 |
| RPH | 88 (50;100) | 100 (50;100) | 0.57 | 100 (75;100) | 100 (50;100) | 0.29 | 0.25 |
| REP | 100 (0;100) | 100 (33;100) | 0.58 | 100 (50;100) | 100 (17;100) | 0.28 | 0.29 |
| Energy/fatigue | 50 (35;60) | 53 (30:65) | 0.59 | 40 (25;65) | 48 (30;73) | 0.61 | 0.22 |
| Emotional well-being | 74 (60;84) | 80 (52;84) | 0.57 | 72 (58;84) | 70 (52:84) | 0.32 | 0.31 |
| Social functioning | 59 (45;80) | 69 (38;80) | 0.92 | 53 (36;73) | 64 (40;79) | 0.43 | 0.55 |
| Pain | 58 (45;90) | 68 (55;90) | 0.61 | 74 (68;95) | 69 (68;90) | 0.52 | 0.50 |
| General health | 65 (50;80) | 63 (35;75) | 0.25 | 58 (38;80) | 68 (38;78) | 0.42 | 0.17 |
| MDI | |||||||
| Score | 11 (9;20) | 10 (7;22) | 0.92 | 13 (5;29) | 15 (6;27) | 0.87 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ravn, P.; Gram, F.; Andersen, M.S.; Glintborg, D. Myoinositol vs. Metformin in Women with Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial. Metabolites 2022, 12, 1183. https://doi.org/10.3390/metabo12121183
Ravn P, Gram F, Andersen MS, Glintborg D. Myoinositol vs. Metformin in Women with Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial. Metabolites. 2022; 12(12):1183. https://doi.org/10.3390/metabo12121183
Chicago/Turabian StyleRavn, Pernille, Freja Gram, Marianne S. Andersen, and Dorte Glintborg. 2022. "Myoinositol vs. Metformin in Women with Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial" Metabolites 12, no. 12: 1183. https://doi.org/10.3390/metabo12121183
APA StyleRavn, P., Gram, F., Andersen, M. S., & Glintborg, D. (2022). Myoinositol vs. Metformin in Women with Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial. Metabolites, 12(12), 1183. https://doi.org/10.3390/metabo12121183