
Lipid Profile and Hepatic Fat Content Measured by 1H MR Spectroscopy in Patients before and after Liver Transplantation

 ,
,
Abstract
1. Introduction
2. Results
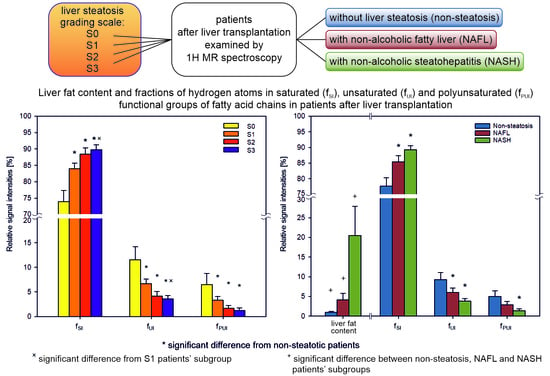
2.1. Steatosis Grade
2.2. Lipid Profile
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. Phantoms
4.3. MR Examination
4.4. Data Evaluation
4.5. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nassir, F.; Rector, R.S.; Hammoud, G.M.; Ibdah, J.A. Pathogenesis and Prevention of Hepatic Steatosis. Gastroenterol. Hepatol. 2015, 11, 167–175. [Google Scholar]
- Linares, I.; Hamar, M.; Selzner, N.; Selzner, M. Steatosis in Liver Transplantation: Current Limitations and Future Strategies. Transplantation 2019, 103, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Benedict, M.; Zhang, X. Non-alcoholic fatty liver disease: An expanded review. World J. Hepatol. 2017, 9, 715–732. [Google Scholar] [CrossRef]
- Kramer, H.; Pickhardt, P.J.; Kliewer, M.A.; Hernando, D.; Chen, G.H.; Zagzebski, J.A.; Reeder, S.B. Accuracy of Liver Fat Quantification with Advanced CT, MRI, and Ultrasound Techniques: Prospective Comparison with MR Spectroscopy. AJR Am. J. Roentgenol. 2017, 208, 92–100. [Google Scholar] [CrossRef]
- Schwenzer, N.F.; Springer, F.; Schraml, C.; Stefan, N.; Machann, J.; Schick, F. Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J. Hepatol. 2009, 51, 433–445. [Google Scholar] [CrossRef]
- Cheng, Y.; Zhang, K.; Chen, Y.; Chen, Y.; Li, Y.; Li, Y.; Fu, K.; Feng, R. Associations between Dietary Nutrient Intakes and Hepatic Lipid Contents in NAFLD Patients Quantified by 1H-MRS and Dual-Echo MRI. Nutrients 2016, 8, 527. [Google Scholar] [CrossRef] [PubMed]
- Kovar, J.; Dusilova, T.; Sedivy, P.; Bruha, R.; Gottfriedova, H.; Pavlikova, P.; Pitha, J.; Smid, V.; Drobny, M.; Dezortova, M.; et al. Acute responses of hepatic fat content to consuming fat, glucose and fructose alone and in combination in non-obese non-diabetic individuals with non-alcoholic fatty liver disease. J. Physiol. Pharmacol. 2021, 72, 1. [Google Scholar] [CrossRef]
- Golabi, P.; Locklear, C.T.; Austin, P.; Afdhal, S.; Byrns, M.; Gerber, L.; Younossi, Z.M. Effectiveness of exercise in hepatic fat mobilization in non-alcoholic fatty liver disease: Systematic review. World J. Gastroenterol. 2016, 22, 6318–6327. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.; Guo, Z.; Schroder, P.M.; Zheng, Z.; Lu, Y.; Gu, J.; He, X. Accuracy of MR Imaging and MR Spectroscopy for Detection and Quantification of Hepatic Steatosis in Living Liver Donors: A Meta-Analysis. Radiology 2017, 282, 92–102. [Google Scholar] [CrossRef]
- Chiang, H.J.; Chang, W.P.; Chiang, H.W.; Lazo, M.Z.; Chen, T.Y.; Ou, H.Y.; Tsanga, L.L.-C.; Huanga, T.-L.; Chenb, C.-L.; Cheng, Y.-F. Magnetic resonance spectroscopy in living-donor liver transplantation. Transplant. Proc. 2016, 48, 1003–1006. [Google Scholar] [CrossRef]
- Krishan, S.; Jain, D.; Bathina, Y.; Kale, A.; Saraf, N.; Saigal, S.; Choudhary, N.; Baijal, S.; Soin, A. Non-invasive quantification of hepatic steatosis in living. related liver donors using dual-echo Dixon imaging and single-voxel proton spectroscopy. Clin. Radiol. 2016, 71, 58–63. [Google Scholar] [CrossRef]
- Satkunasingham, J.; Nik, H.H.; Fischer, S.; Menezes, R.; Selzner, N.; Cattral, M.; Grant, D.; Jhaveri, K. Can negligible hepatic steatosis determined by magnetic resonance imaging-proton density fat fraction obviate the need for liver biopsy in potential liver donors? Liver Transpl. 2018, 24, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, R.; Gupta, S.; Garg, B.; Vohra, S.; Wadhawan, M.; Rastogi, H. Comparative accuracy of CT. dual-echo MRI and MR spectroscopy for preoperative liver fat quantification in living related liver donors. Indian J. Radiol. Imaging 2016, 26, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Hajek, M.; Dezortova, M.; Wagnerova, D.; Skoch, A.; Voska, L.; Hejlova, I.; Trunecka, P. MR spectroscopy as a tool for in vivo determination of steatosis in liver transplant recipients. Magn. Reson. Mater. Phys. Biol. Med. 2011, 24, 297–304. [Google Scholar] [CrossRef]
- Provencher, S.W. Automatic quantitation of localized in vivo 1H spectra with LCModel. NMR Biomed. 2001, 14, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Walton, D.W.; Sachinwalla, T.; Thompson, C.H.; Smith, K.; Ruell, P.A.; Stannard, S.R.; George, J. Noninvasive assessment of hepatic lipid composition: Advancing understanding and management of fatty liver disorders. Hepatology 2008, 47, 1513–1523. [Google Scholar] [CrossRef]
- Strobel, K.; van den Hoff, J.; Pietzsch, J. Localized proton magnetic resonance spectroscopy of lipids in adipose tissue at high spatial resolution in mice in vivo. J. Lipid Res. 2008, 49, 473–480. [Google Scholar] [CrossRef]
- Ren, J.; Dimitrov, I.; Sherry, A.D.; Malloy, C.R. Composition of adipose tissue and marrow fat in humans by 1H NMR at 7 Tesla. J. Lipid Res. 2008, 49, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Erickson, M.L.; Haus, J.M.; Malin, S.K.; Flask, C.A.; McCullough, A.J.; Kirwan, J.P. Non-invasive assessment of hepatic lipid subspecies matched with non-alcoholic fatty liver disease phenotype. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1197–1204. [Google Scholar] [CrossRef]
- Traussnigg, S.; Kienbacher, C.; Gajdošík, M.; Valkovič, L.; Halilbasic, E.; Stift, J.; Rechling, C.; Hofer, H.; Steindl-Munda, P.; Ferenci, P.; et al. Ultra-high-field magnetic resonance spectroscopy in non-alcoholic fatty liver disease: Novel mechanistic and diagnostic insights of energy metabolism in non-alcoholic steatohepatitis and advanced fibrosis. Liver Int. 2017, 37, 1544–1553. [Google Scholar] [CrossRef]
- Gajdošík, M.; Chadzynski, G.L.; Hangel, G.; Mlynárik, V.; Chmelík, M.; Valkovič, L.; Bogner, W.; Pohmann, R.; Scheffler, K.; Trattnig, S.; et al. Ultrashort-TE stimulated echo acquisition mode (STEAM) improves the quantification of lipids and fatty acid chain unsaturation in the human liver at 7 T. NMR Biomed. 2015, 28, 1283–1293. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Hejlova, I.; Honsova, E.; Sticova, E.; Lanska, V.; Hucl, T.; Spicak, J.; Jirsa, M.; Trunecka, P. Prevalence and risk factors of steatosis after liver transplantation and patient outcomes. Liver Transpl. 2016, 22, 644–655. [Google Scholar] [CrossRef]
- Singer, P.; Gnauck, G.; Honigmann, G.; Stolz, P.; Schliack, V.; Kettler, L.-H.; Buntrock, P.; Thoelke, H. The fatty acid pattern of adipose tissue and liver triglycerides according to fat droplet size in liver parenchymal cells of diabetic subjects. Diabetologia 1974, 10, 455–458. [Google Scholar] [CrossRef][Green Version]
- Araya, J.; Rodrigo, R.; Videla, L.A.; Thielemann, L.; Orellana, M.; Pettinelli, P.; Poniachik, J. Increase in long-chain polyunsaturated fatty acid n-6/n-3 ratio in relation to hepatic steatosis in patients with non-alcoholic fatty liver disease. Clin. Sci. 2004, 106, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Puri, P.; Baillie, R.A.; Wiest, M.M.; Mirshahi, F.; Choudhury, J.; Cheung, O.; Díaz, J.C.; Signorini, C.; Sgherri, C.; Comporti, M.; et al. A lipidomic analysis of nonalcoholic fatty liver disease. Hepatology 2007, 46, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Elizondo, A.; Araya, J.; Rodrigo, R.; Poniachik, J.; Csendes, A.; Maluenda, F.; Díaz, J.C.; Signorini, C.; Sgherri, C.; Comporti, M.; et al. Polyunsaturated fatty acid pattern in liver and erythrocyte phospholipids from obese patients. Obesity 2007, 15, 24–31. [Google Scholar] [CrossRef]
- Yamada, K.; Mizukoshi, E.; Sunagozaka, H.; Arai, K.; Yamashita, T.; Takeshita, Y.; Misu, H.; Takamura, T.; Kitamura, S.; Zen, Y.; et al. Characteristics of hepatic fatty acid compositions in patients with nonalcoholic steatohepatitis. Liver Int. 2015, 35, 582–590. [Google Scholar] [CrossRef]
- Roumans, K.H.M.; Lindeboom, L.; Veeraiah, P.; Remie, C.M.E.; Phielix, E.; Havekes, B.; Bruls, Y.; Brouwers, M.C.G.J.; Ståhlman, M.; Alssema, M.; et al. Hepatic saturated fatty acid fraction is associated with de novo lipogenesis and hepatic insulin resistance. Nat. Commun. 2020, 11, 1891. [Google Scholar] [CrossRef] [PubMed]
- Biological Magnetic Resonance Data Bank. Available online: https://bmrb.io/metabolomics/ (accessed on 30 June 2021).
- Šedivý, P.; Dezortová, M.; Burian, M.; Dusilová, T.; Kovář, J.; Hájek, M. Comparison of Accuracy of Magnetic Resonance Spectroscopic and Imaging Techniques for the Liver Steatosis Assessment. Chem. Listy 2021, 115, 46–53. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signal Label | Ppm | Expected Signals | LCModel Starting Parameters | |||
|---|---|---|---|---|---|---|
| Position [ppm] | Position SD [ppm] | Width Min [ppm] | Width Max [ppm] | |||
| Lip09 | 0.9 | –(CH2)n–CH3 | 0.87 | 0.04 | 0.25 | 0.45 |
| Lip13 | 1.3 | –(CH2)n | 1.28 | 0.04 | 0.02 | 0.55 |
| Lip16 | 1.6 | –O–CO–CH2–CH2– | 1.60 | 0.02 | 0.02 | 0.25 |
| Lip21 | 2.0–2.1 | –CH2–CH=CH–CH2– (allylic) | 2.02 | 0.03 | 0.05 | 0.25 |
| Lip24 | 2.4 | –CO–CH2–CH2– | 2.23 | 0.03 | 0.05 | 0.25 |
| Lip28 | 2.8 | –CH=CH–CH2–CH=CH– (diallylic) | 2.76 | 0.03 | 0.05 | 0.25 |
| Lip41 | 4.1 | –CH2–O–CO–R (glycerol) | 4.10 | 0.03 | 0.20 | 0.30 |
| Lip43 | 4.3 | –CH2–O–CO–R (glycerol) | 4.30 | 0.03 | 0.20 | 0.30 |
| Lip53 | 5.2–5.3 | >CH–O–CO–R (glycerol) –CH=CH– (olefinic) | 5.20 5.33 | 0.03 0.02 | 0.02 0.20 | 0.15 0.40 |
| Water | 4.7 | H2O | 4.65 | 0.05 | 0.01 | 0.55 |
| Histological Grading [22] | S0 | S1 | S2 | S3 | |
|---|---|---|---|---|---|
| Tx group 84biopsies | N | 34 | 34 | 9 | 7 |
| Mean FF | 0.98 | 2.71 | 14.50 | 23.32 | |
| (0.71–1.25) | (1.82–3.61) | (7.00–21.99) | (13.65–33.00) | ||
| MRS grading | S0mr | S1mr | S2mr | S3mr | |
| (FF ≤ 0.81) | (0.81 < FF ≤ 6.07) | (6.07 < FF ≤ 15.9) | (FF > 15.9) | ||
| Tx group 101MRS | N | 22 | 62 | 9 | 8 |
| Mean FF | 0.55 | 2.22 | 11.41 | 26.57 | |
| (0.48–0.62) | (1.83–2.57) | (8.95–13.88) | (19.53–33.60) | ||
| WL group 47 MRS | N | 16 | 29 | 1 | 1 |
| Mean FF | 0.60 | 2.01 | 15.23 + | 20.74 + | |
| (0.50–0.69) | (1.30–2.73) |
| Non-Steatosis | NAFL | NASH | Unknown | |
|---|---|---|---|---|
| N | 34 | 39 | 11 | 17 |
| fSI [%] | 77.62 | 85.36 a | 89.31 a | 82.00 |
| (74.87–80.37) | (83.29–87.42) | (88.05–90.57) | (77.36–86.65) | |
| fUI [%] | 9.24 | 6.00 a | 3.80 a | 8.47 |
| (7.37–11.11) | (4.88–7.12) | (3.15–4.44) | (5.69–11.25) | |
| fPUI [%] | 4.97 | 2.86 | 1.40 a | 4.60 |
| (3.46–6.47) | (2.01–3.71) | (0.92–1.87) | (2.28–6.92) | |
| FF [%] | 0.98 b | 4.11 b | 20.50 b | 2.62 |
| (0.71–1.26) | (2.39–5.84) | (13.07–27.93) | (1.45–3.80) |
| Tx | S0mr-Tx | S1mr-Tx | S2mr-Tx | S3mr-Tx | WL | S0mr-WL | S1mr-WL | |
|---|---|---|---|---|---|---|---|---|
| N | 101 | 22 | 62 | 9 | 8 | 47 | 16 | 29 |
| Age (yrs) | 56.4 | 52.1 | 57.4 | 56.6 | 59.4 | 58 | 58.8 | 57.5 |
| (11.4) | (12.9) | (11.1) | (10.8) | (6.5) | (9.9) | (10.0) | (10.0) | |
| BMI (kg/m2) | 26.4 | 21.7 | 26.8 | 28.6 | 27.6 | 26.8 | 25.1 | 27.6 |
| (4.4) | (2.1) | (4.0) | (3.8) | (3.3) | (4.7) | (4.3) | (4.7) | |
| Waist circumference (cm) | 98.2 | 83.6 | 98.3 | 109.6 | 108.4 | 101.7 | 97.3 | 104.1 |
| (13.2) | (8.5) | (11.2) | (8.8) | (12.9) | (13.6) | (11.9) | (13.9) | |
| Total bilirubin (umol/L) | 15.2 | 14.8 | 15.0 | 14.0 | 14.4 | 60.7 | 78.1 | 51.7 |
| (7.8) | (9.4) | (7.2) | (8.8) | (3.9) | (49.3) | (55.6) | (43.9) | |
| AST (ukat/L) | 0.43 | 0.45 | 0.42 | 0.56 | 0.54 | 1.21 | 1.29 | 1.17 |
| (0.22) | (0.27) | (0.16) | (0.52) | (0.1) | (0.78) | (0.91) | (0.72) | |
| ALT (ukat/L) | 0.56 | 0.56 | 0.54 | 0.69 | 0.85 | 0.81 | 0.77 | 0.83 |
| (0.33) | (0.47) | (0.33) | (0.28) | (0.45) | (0.54) | (0.56) | (0.54) | |
| ALP (ukat/L) | 1.66 | 1.47 | 1.69 | 1.72 | 1.62 | 2.82 | 2.94 | 2.76 |
| (0.99) | (0.57) | (1.07) | (1.10) | (0.73) | (2.48) | (1.32) | (2.92) | |
| GGT (ukat/L) | 0.91 | 0.67 | 0.78 | 1.78 | 1.75 | 2.25 | 2.04 | 2.37 |
| (1.58) | (0.95) | (1.25) | (3.55) | (1.06) | (2.70) | (1.94) | (3.04) | |
| Triglycerides (mmol/L) | 1.55 | 1.16 | 1.36 | 2.25 | 3.44 | 1.11 | 0.92 | 1.19 |
| (1.09) | (0.43) | (0.68) | (1.02) | (3.13) | (0.68) | (0.30) | (0.77) | |
| Cholesterol (mmol/L) | 4.67 | 4.59 | 4.60 | 5.10 | 4.74 | 3.96 | 3.85 | 4.01 |
| (0.96) | (0.74) | (0.96) | (0.87) | (0.95) | (1.56) | (1.32) | (1.67) | |
| LDL chol (mmol/L) | 2.72 | 2.67 | 2.69 | 2.91 | 2.65 | 2.61 | 2.61 | 2.61 |
| (0.78) | (0.55) | (0.76) | (0.79) | (1.08) | (1.14) | (1.25) | (1.12) | |
| HDL chol (mmol/L) | 1.26 | 1.41 | 1.26 | 1.18 | 1.09 | 0.80 | 0.82 | 0.79 |
| (0.39) | (0.38) | (0.35) | (0.47) | (0.59) | (0.41) | (0.41) | (0.41) | |
| Glycaemia (mmol/L) | 6.12 | 5.37 | 6.03 | 8.02 | 6.29 | 5.49 | 5.35 | 5.57 |
| (1.87) | (0.67) | (1.62) | (3.03) | (0.78) | (1.33) | (1.43) | (1.29) | |
| HbA1c (mmol/mol) | 38.04 | 33.47 | 37.00 | 43.44 | 40.8 | 32.28 | 27.50 | 34.74 |
| (10.02) | (6.46) | (7.21) | (11.91) | (8.32) | (10.62) | (6.03) | (11.67) | |
| C-peptide (nmol/L) | 0.90 | 0.90 | 0.89 | 1.25 | 1.46 | 1.34 | 1.39 | 1.32 |
| (0.42) | (0.38) | (0.40) | (0.53) | (0.87) | (0.64) | (0.84) | (0.52) | |
| Fast insulinaemia (uIU/mL) | 7.92 | 6.76 | 7.73 | 12.24 | 14.59 | 20.60 | 15.52 | 23.31 |
| (5.32) | (3.15) | (4.16) | (8.31) | (11.73) | (22.16) | (16.99) | (24.31) | |
| HOMA-insulin resistance | 2.16 | 1.63 | 2.07 | 4.38 | 4.23 | 5.50 | 4.26 | 6.16 |
| (1.66) | (0.84) | (1.2) | (2.71) | (3.53) | (6.76) | (6.46) | (6.93) | |
| QUICKI | 0.357 | 0.364 | 0.355 | 0.325 | 0.338 | 0.327 | 0.338 | 0.321 |
| (0.039) | (0.030) | (0.036) | (0.044) | (0.070) | (0.049) | (0.041) | (0.053) | |
| Elastography (kPa) | 7.1 | 6.4 | 7.2 | 7.5 | 8.5 | 35.9 | 35.1 | 36.4 |
| (1.9) | (1.4) | (1.8) | (2.0) | (1.3) | (13.8) | (13.0) | (14.5) | |
| NAS score (84 subjects) | 1.81 | 0.16 | 1.54 | 4.43 | 5.13 | n/a | n/a | n/a |
| (1.87) | (0.36) | (1.17) | (1.68) | (1.17) |
| Fat Concentration in Phantom [%] | (a) fLip53 | (b) fLip21/2 + Lip28 | (c) fLip21 + Lip28 [19] |
|---|---|---|---|
| 5 | 4.1% | 4.6% | 8.6% |
| 10 | 4.4% | 3.8% | 7.3% |
| 15 | 4.0% | 3.3% | 6.3% |
| 20 | 6.9% | 4.4% | 8.4% |
| 30 | 5.6% | 5.2% | 9.8% |
| Theoretical values + | 4.5 | 4.5 | 8.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burian, M.; Hajek, M.; Sedivy, P.; Mikova, I.; Trunecka, P.; Dezortova, M. Lipid Profile and Hepatic Fat Content Measured by 1H MR Spectroscopy in Patients before and after Liver Transplantation. Metabolites 2021, 11, 625. https://doi.org/10.3390/metabo11090625
Burian M, Hajek M, Sedivy P, Mikova I, Trunecka P, Dezortova M. Lipid Profile and Hepatic Fat Content Measured by 1H MR Spectroscopy in Patients before and after Liver Transplantation. Metabolites. 2021; 11(9):625. https://doi.org/10.3390/metabo11090625
Chicago/Turabian StyleBurian, Martin, Milan Hajek, Petr Sedivy, Irena Mikova, Pavel Trunecka, and Monika Dezortova. 2021. "Lipid Profile and Hepatic Fat Content Measured by 1H MR Spectroscopy in Patients before and after Liver Transplantation" Metabolites 11, no. 9: 625. https://doi.org/10.3390/metabo11090625
APA StyleBurian, M., Hajek, M., Sedivy, P., Mikova, I., Trunecka, P., & Dezortova, M. (2021). Lipid Profile and Hepatic Fat Content Measured by 1H MR Spectroscopy in Patients before and after Liver Transplantation. Metabolites, 11(9), 625. https://doi.org/10.3390/metabo11090625