
Modeling Intraperitoneal Insulin Absorption in Patients with Type 1 Diabetes




Abstract
:1. Introduction
2. Materials and Methods
2.1. Database and Protocol
2.2. Model Development
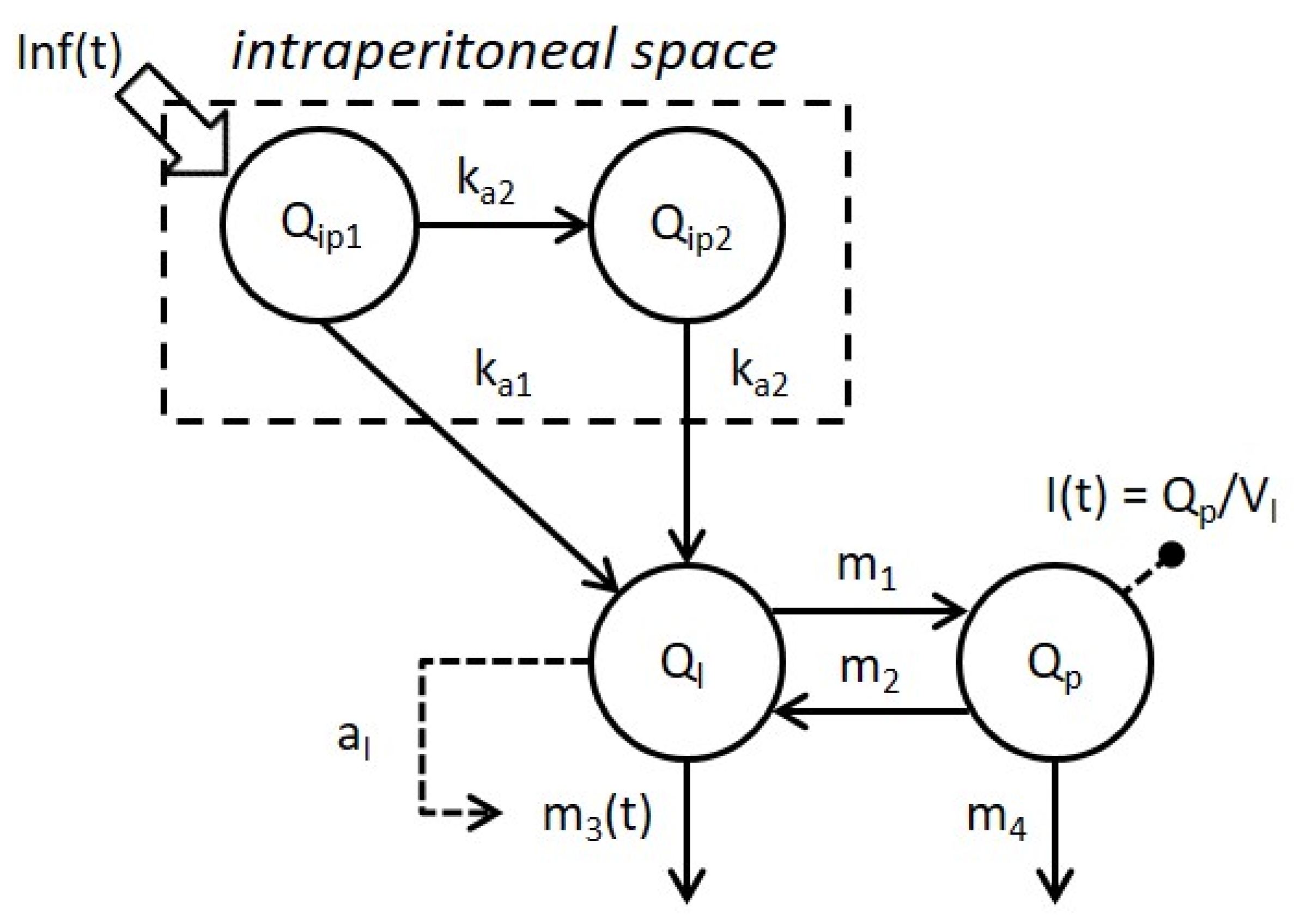
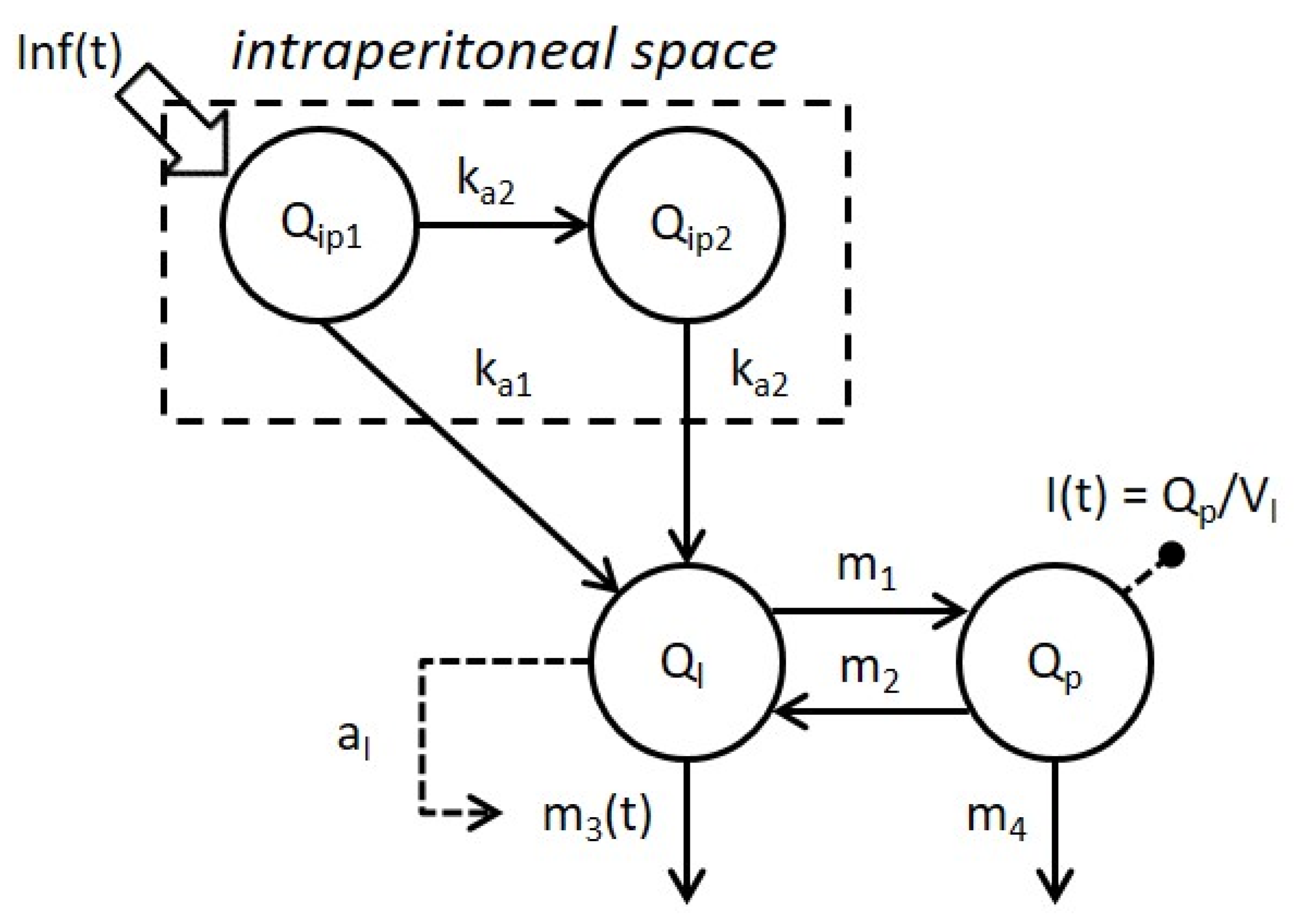
2.2.1. Model of IP Insulin Absorption
2.2.2. Model of Whole-Body Insulin Kinetics
2.3. Model Identification
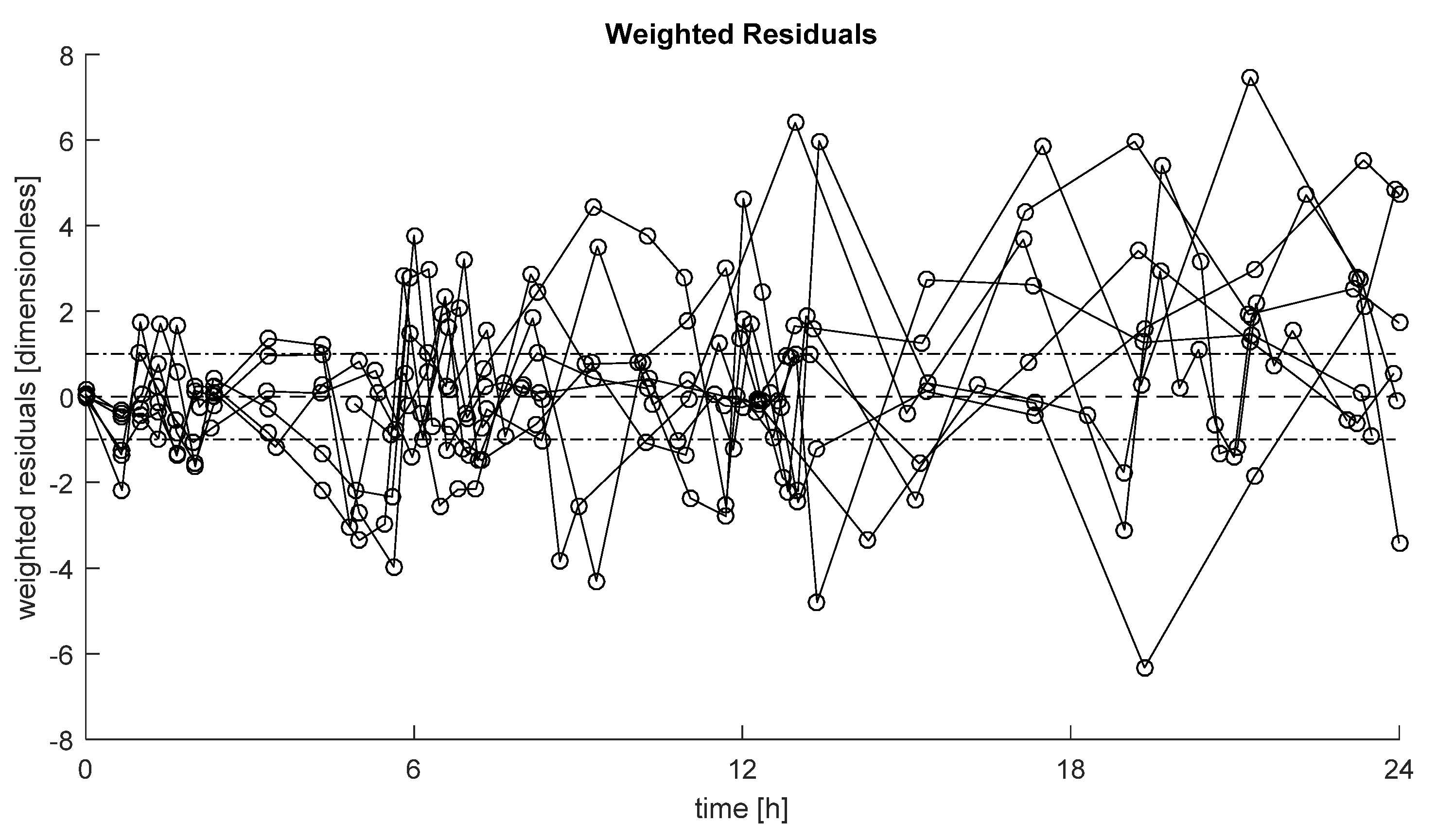
2.4. Model Assessment and Comparison
2.5. Statistical Analysis
3. Results
3.1. Model Comparison
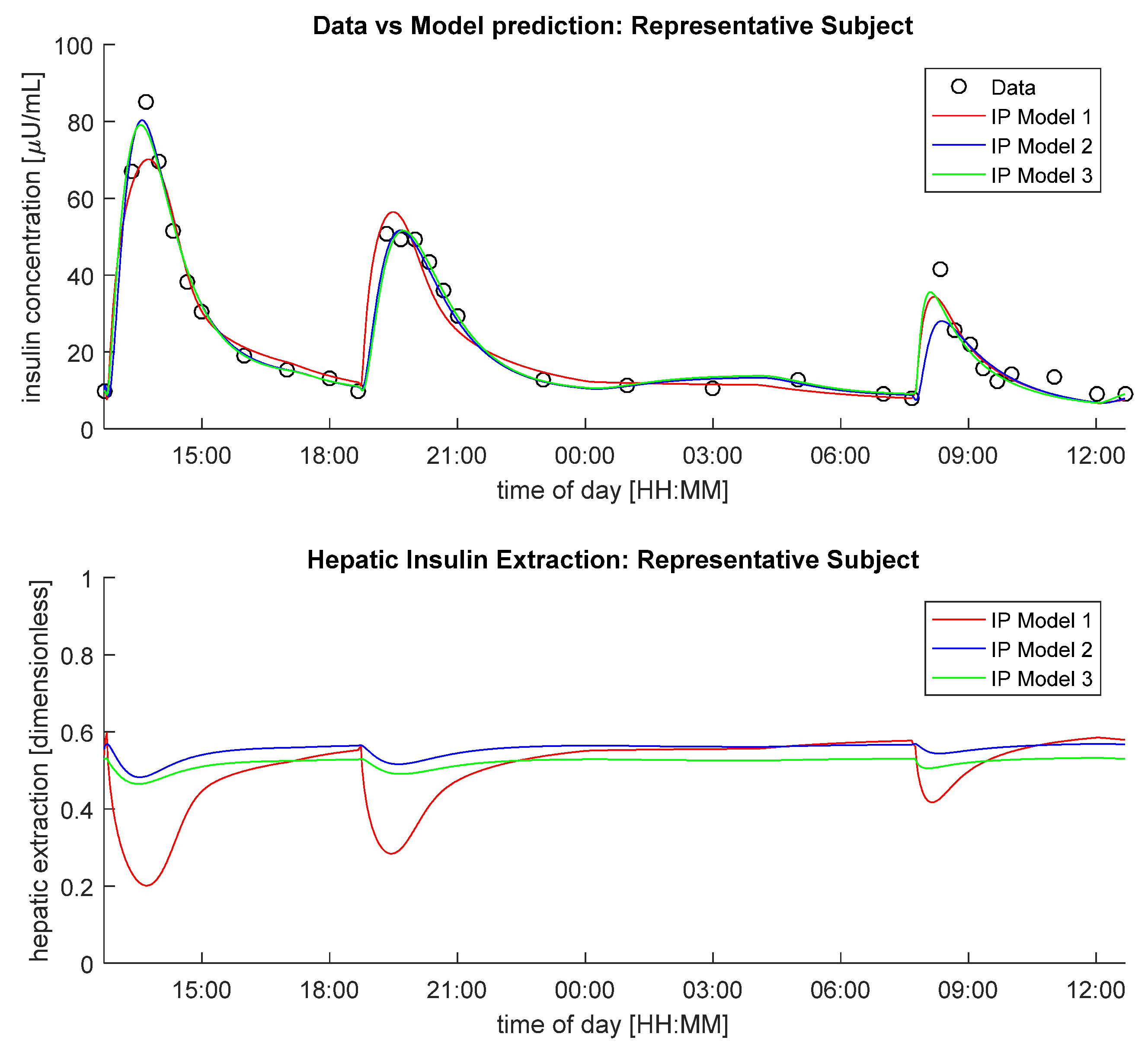
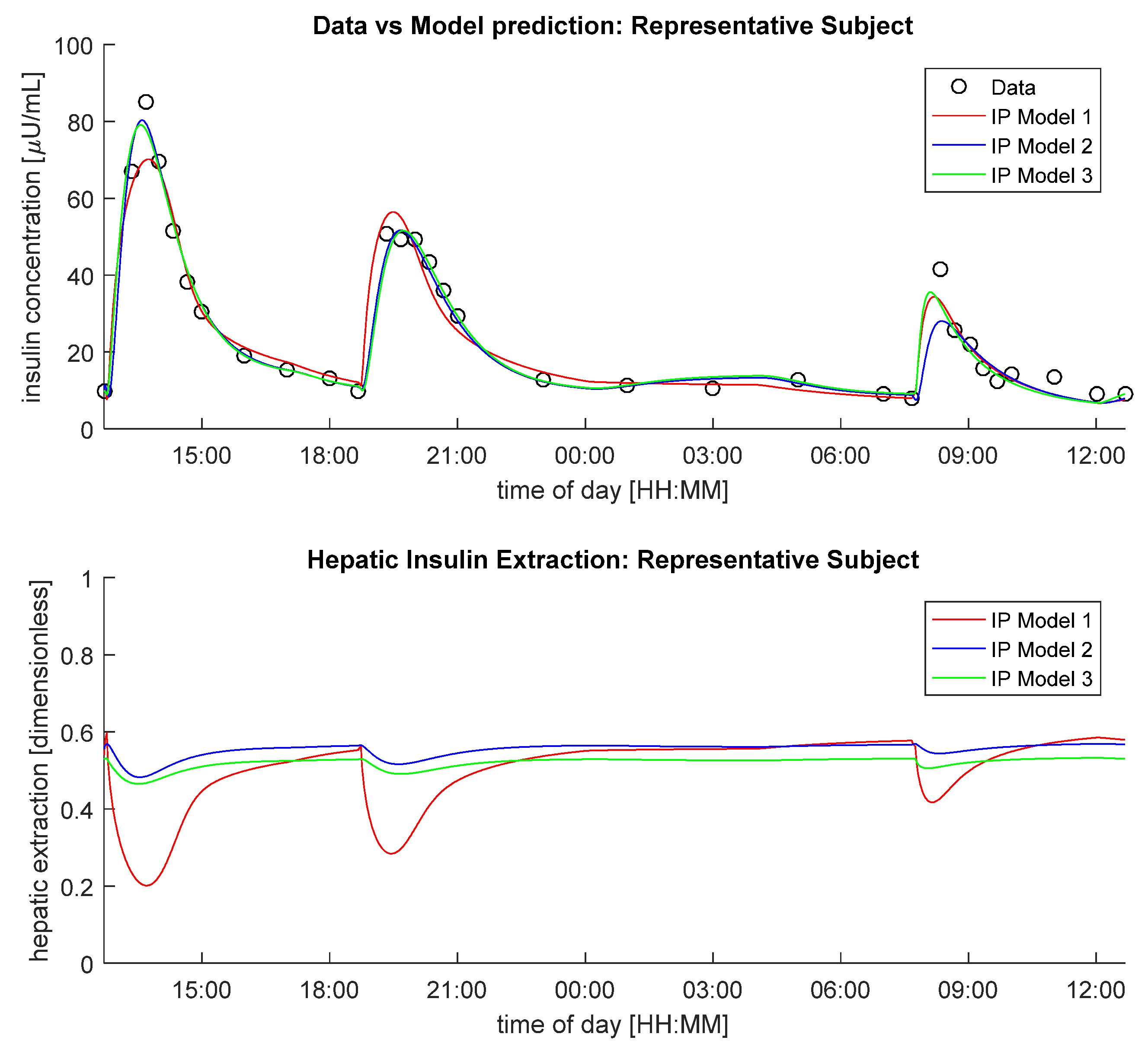
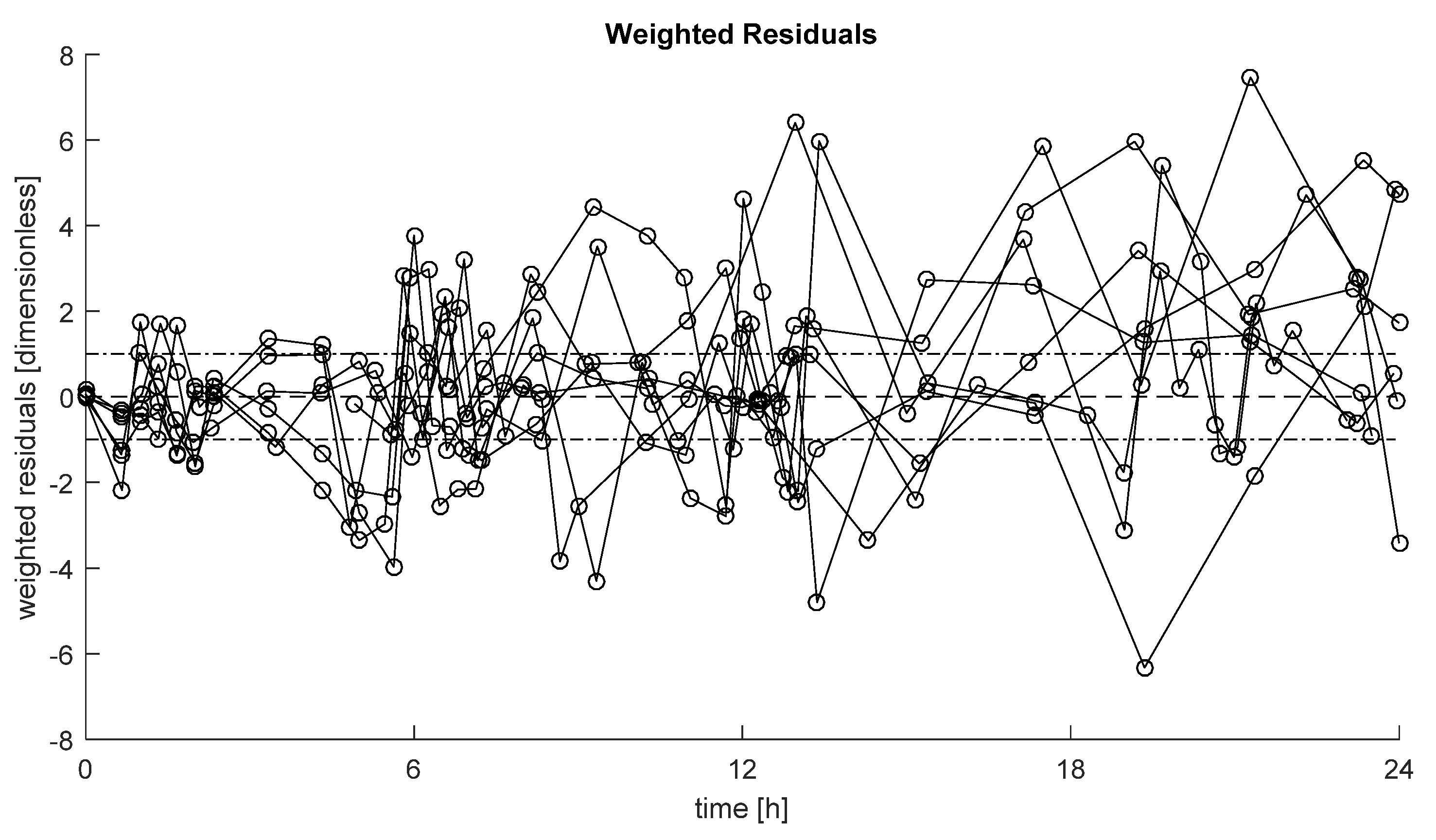
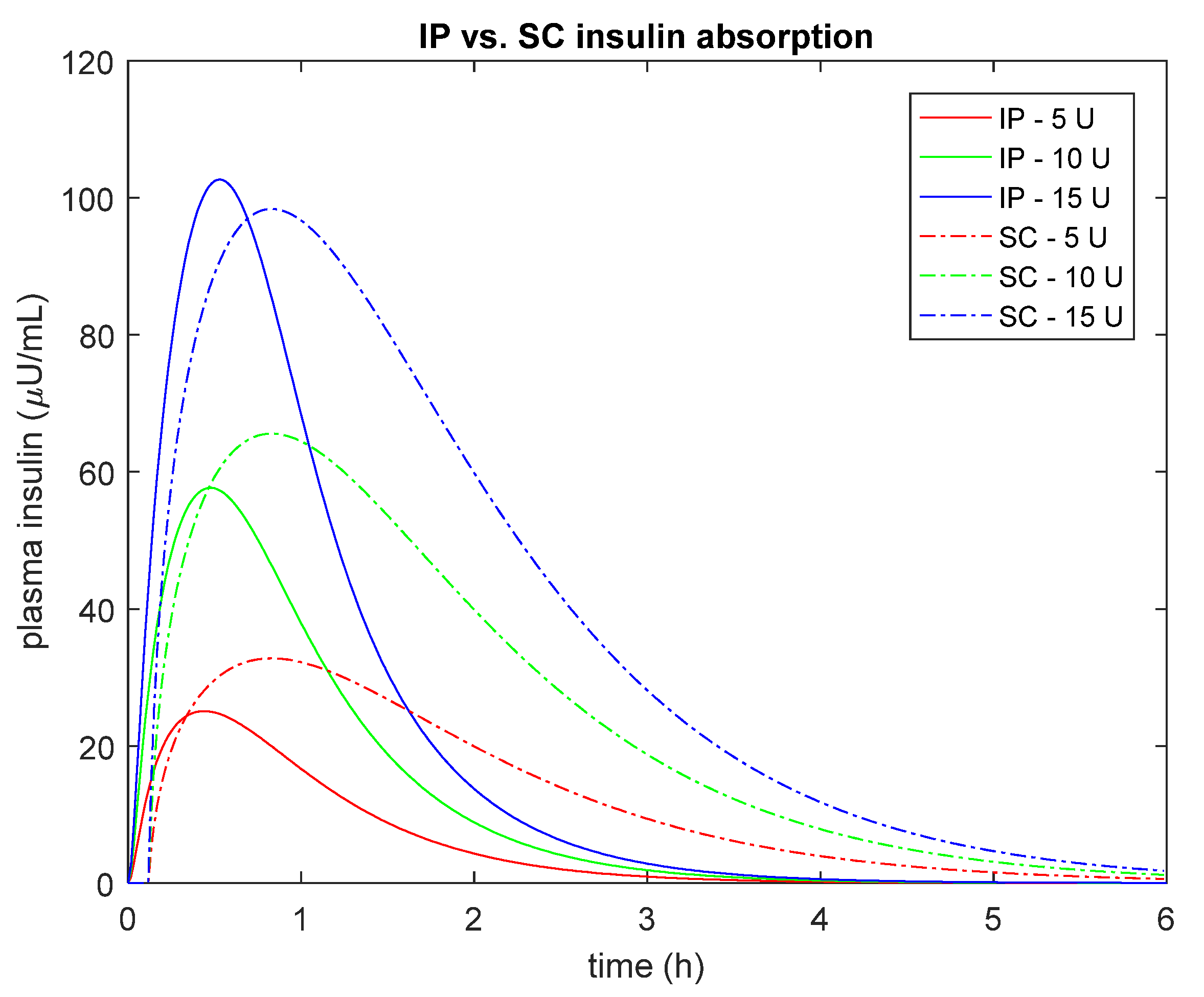
3.2. Performance of the Selected Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications: Report of a WHO Consultation. Part 1, Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 1999; Available online: https://apps.who.int/iris/handle/10665/66040 (accessed on 17 February 2021).
- Kovatchev, B.P. The year of transition from research to clinical practice. Nat. Rev. Endocrinol. 2018, 14, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, M.; Dalla Man, C.; Cobelli, C. Modeling subcutaneous absorption of fast-acting insulin in type 1 diabetes. IEEE Trans. Biomed. Eng. 2018, 65, 2019–2086. [Google Scholar] [CrossRef]
- Van Dijk, P.R.; Logtenberg, S.J.; Gans, R.O.; Bilo, H.J.; Kleefstra, N. Intraperitoneal insulin infusion: Treatment option for type 1 diabetes resulting in beneficial endocrine effects beyond glycaemia. Clin. Endocrinol. 2014, 81, 488–497. [Google Scholar] [CrossRef]
- Selam, J.L.; Bergman, R.N.; Raccah, D.; Jean-Didier, N.; Lonzano, J.; Charles, M.A. Determination of portal insulin absorption from peritoneum via novel nonisotopic method. Diabetes 1990, 39, 1361–1365. [Google Scholar] [CrossRef]
- Nathan, D.M.; Dunn, F.L.; Bruch, J.; McKitrick, C.; Larkin, M.; Haggan, C.; Lavin-Tompkins, J.; Norman, D.; Rogers, D.; Simon, D. Postprandial insulin profiles with implantable pump therapy may explain decreased frequency of severe hypoglycemia, compared with intensive subcutaneous regimens, in insulin-dependent diabetes mellitus patients. Am. J. Med. 1996, 100, 412–417. [Google Scholar] [CrossRef]
- Haardt, M.J.; Selam, J.L.; Slama, G.; Bethoux, J.P.; Dorange, C.; Mace, B.; Ramaniche, M.L.; Bruzzo, F. A cost–benefit comparison of intensive diabetes management with implantable pumps versus multiple subcutaneous injections in patients with type I diabetes. Diabetes Care 1994, 17, 847–851. [Google Scholar] [CrossRef]
- Selam, J.L.; Raccah, D.; Jean–Didier, N.; Lozano, J.L.; Waxman, K.; Charles, M.A. Randomized comparison of metabolic control achieved by intraperitoneal insulin infusion with implantable pumps versus intensive subcutaneous insulin therapy in type I diabetic patients. Diabetes Care 1992, 15, 53–58. [Google Scholar] [CrossRef]
- Van Dijk, P.R.; Logtenberg, S.J.; Groenier, K.H.; Gans, R.O.; Kleefstra, N.; Bilo, H.J. Continuous intraperitoneal insulin infusion in type 1 diabetes: A 6–year post-trial follow–up. BMC Endocr. Disord. 2014, 14, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dijk, P.R.; Groenier, K.H.; DeVries, J.H.; Gans, R.O.; Kleefstra, N.; Bilo, H.J.; Logtenberg, S.J.J. Continuous intraperitoneal insulin infusion versus subcutaneous insulin therapy in the treatment of type 1 diabetes: Effects on glycemic variability. Diabetes Technol. Ther. 2015, 17, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Dassau, E.; Renard, E.; Place, J.; Farret, A.; Pelletier, M.J.; Lee, J.; Huyett, L.M.; Chakrabarty, A.; Doyle, F.J., III. Intraperitoneal insulin delivery provides superior glycaemic regulation to subcutaneous insulin delivery in model predictive control-based fully-automated artificial pancreas in patients with type 1 diabetes: A pilot study. Diabetes Obes. Metab. 2017, 19, 1698–1705. [Google Scholar] [CrossRef] [PubMed]
- Toffanin, C.; Lalo, M.; Cobelli, C. Artificial Pancreas: In silico study shows no need of meal announcement and improved time in range of glucose with intraperitoneal vs subcutaneous delivery. IEEE Trans. Med. Robot. Bionics 2021, 3, 306–314. [Google Scholar] [CrossRef]
- Renard, E.; Place, J.; Cantwell, M.; Chevassus, H.; Palerm, C. Closed–Loop insulin delivery using a subcutaneous glucose sensor and intraperitoneal insulin delivery. Diabetes Care 2010, 33, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovatchev, B.P.; Breton, M.; Dalla Man, C.; Cobelli, C. In silico precilinical trials: A proof of concept in closed-loop control of type 1 diabetes. J. Diabetes Sci. Technol. 2009, 3, 44–55. [Google Scholar] [CrossRef] [Green Version]
- Visentin, R.; Campos-Náñez, E.; Schiavon, M.; Lv, D.; Vettoretti, M.; Breton, M.; Kovatchev, B.P.; Dalla Man, C.; Cobelli, C. The UVA/PADOVA type 1 diabetes simulator goes from single meal to single day. J. Diabetes Sci. Technol. 2018, 12, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Wilinska, M.E.; Chassin, L.J.; Acerini, C.L.; Allen, J.M.; Dunger, D.B.; Hovorka, R. Simulation environment to evaluate closed-loop insulin delivery systems in type 1 diabetes. J. Diabetes Sci. Technol. 2010, 4, 132–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehmann, E.D.; Tarin, C.; Bondia, J.; Teufel, E.; Deutsch, T. Development of AIDA v4.3b Diabetes Simulator: Technical upgrade to support incorporation of insulin lispro, aspart, and glargine insulin analogues. J. Electr. Comput. Eng. 2011, 2011, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Piccinini, F.; Dalla Man, C.; Vella, A.; Cobelli, C. A model for the estimation of hepatic insulin extraction after a meal. IEEE Tran. Biomed. Eng. 2016, 63, 1925–1932. [Google Scholar] [CrossRef] [Green Version]
- Bellu, G.; Saccomani, M.P.; Audoly, S.; D’Angiò, L. DAISY: A new software tool to test global identifiability of biological and physiological systems. Comput. Methods Programs Biomed. 2007, 88, 52–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwin, R.S.; Kramer, K.J.; Tobin, J.D.; Insel, P.A.; Liljenquist, J.E.; Berman, E.; Andres, R. A model of the kinetics of insulin in man. JCI 1974, 53, 1481–1492. [Google Scholar] [CrossRef] [Green Version]
- Cobelli, C.; Carson, E.R. Introduction to Modeling of Metabolic in Physiology and Medicine; Academic Press: San Diego, CA, USA, 2008. [Google Scholar]
- Toffolo, G.; Campioni, M.; Basu, R.; Rizza, R.A.; Cobelli, C. A minimal model of insulin secretion and kinetics to assess hepatic insulin extraction. Am. J. Physiol. Endocrinol. Metab. 2006, 290, 169–176. [Google Scholar] [CrossRef]
- Matlab, version 9.0.0.341360 (R2016a); The MathWorks Inc.: Natick, MA, USA, 2016.
- Kass, R.E.; Raftery, A.E. Bayes Factors. J. Am. Statist. Assoc. 1995, 90, 773–795. [Google Scholar] [CrossRef]
- Ferrannini, E.; Cobelli, C. The kinetics of insulin in man. II. Role of the liver. Diabetes Metab. Rev. 1987, 3, 365–397. [Google Scholar] [CrossRef] [PubMed]
- Visentin, R.; Schiavon, M.; Giegerich, C.; Klabunde, T.; Dalla Man, C.; Cobelli, C. Incorporating long-acting insulin glargine into the UVa/Padova Type 1 Diabetes Simulator for in silico testing of MDI therapies. IEEE Trans. Biomed. Eng. 2019, 66, 2889–2896. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, M.; Visentin, R.; Giegerich, C.; Sieber, J.; Dalla Man, C.; Cobelli, C.; Klabunde, T. In silico head-to-head comparison of insulin glargine 300 U/mL and insulin degludec 100 U/mL in type 1 diabetes. Diabetes Technol. Ther. 2020, 22, 553–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iacovacci, V.; Ricotti, L.; Dario, P.; Menciassi, A. Design and development of a mechatronic system for noninvasive refilling of implantable artificial pancreas. IEEE/ASME Trans. Mechatron. 2014, 20, 1160–1169. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intraperitoneal Absorption Model | Whole-Body Kinetic Model | Residual Independence (*) | Parameters Estimated with Coefficient of Variation (CV) < 100% | BIC (**) |
|---|---|---|---|---|
| 1 | A | 7/8 | 100% | 183 |
| 2 | 7/8 | 86% | 178 | |
| 3 | 6/8 | 97% | 177 | |
| 1 | B | 8/8 | 92% | 168 |
| 2 | 8/8 | 80% | 176 | |
| 3 | 8/8 | 89% | 177 | |
| 1 | C | 8/8 | 97% | 171 |
| 2 | 7/8 | 91% | 176 | |
| 3 | 8/8 | 96% | 170 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiavon, M.; Cobelli, C.; Dalla Man, C. Modeling Intraperitoneal Insulin Absorption in Patients with Type 1 Diabetes. Metabolites 2021, 11, 600. https://doi.org/10.3390/metabo11090600
Schiavon M, Cobelli C, Dalla Man C. Modeling Intraperitoneal Insulin Absorption in Patients with Type 1 Diabetes. Metabolites. 2021; 11(9):600. https://doi.org/10.3390/metabo11090600
Chicago/Turabian StyleSchiavon, Michele, Claudio Cobelli, and Chiara Dalla Man. 2021. "Modeling Intraperitoneal Insulin Absorption in Patients with Type 1 Diabetes" Metabolites 11, no. 9: 600. https://doi.org/10.3390/metabo11090600
APA StyleSchiavon, M., Cobelli, C., & Dalla Man, C. (2021). Modeling Intraperitoneal Insulin Absorption in Patients with Type 1 Diabetes. Metabolites, 11(9), 600. https://doi.org/10.3390/metabo11090600