
Reproducibility of Baseline Tumour Metabolic Volume Measurements in Diffuse Large B-Cell Lymphoma: Is There a Superior Method?

 ,
,
Abstract
1. Introduction
2. Results
2.1. Patients Chracteristics
2.2. Descriptive Statistics for the MTV Values
2.3. Interobserver Variability
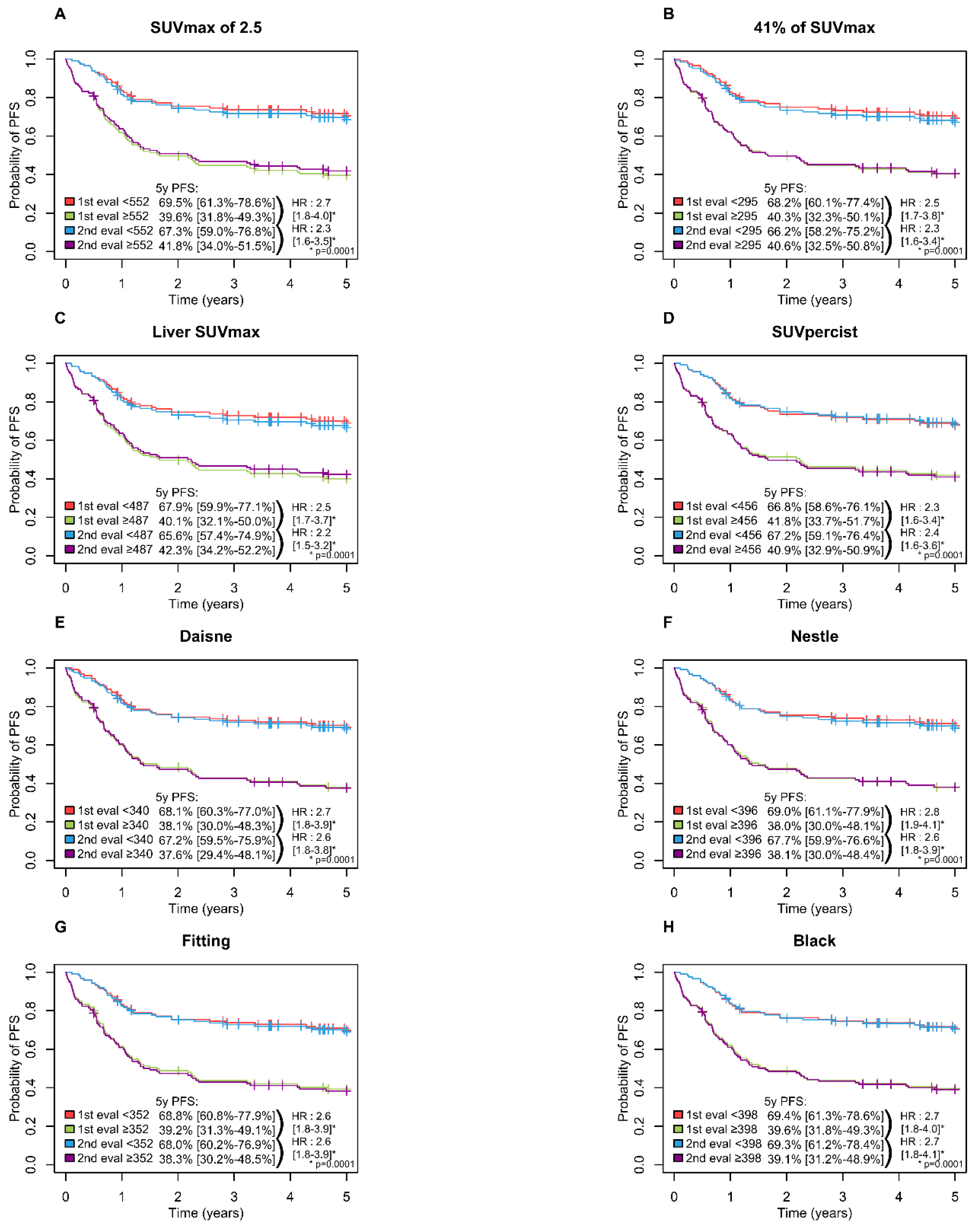
2.4. Prognostic Value and Survival Analysis
3. Discussion
4. Materials and Methods
4.1. Patients and Methods
4.2. FDG-PET/CT Acquisitions
4.3. MTV Measurement
- -
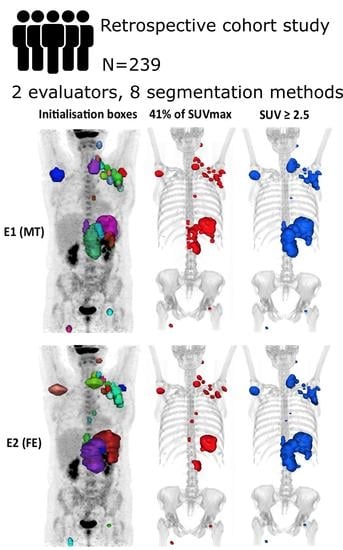
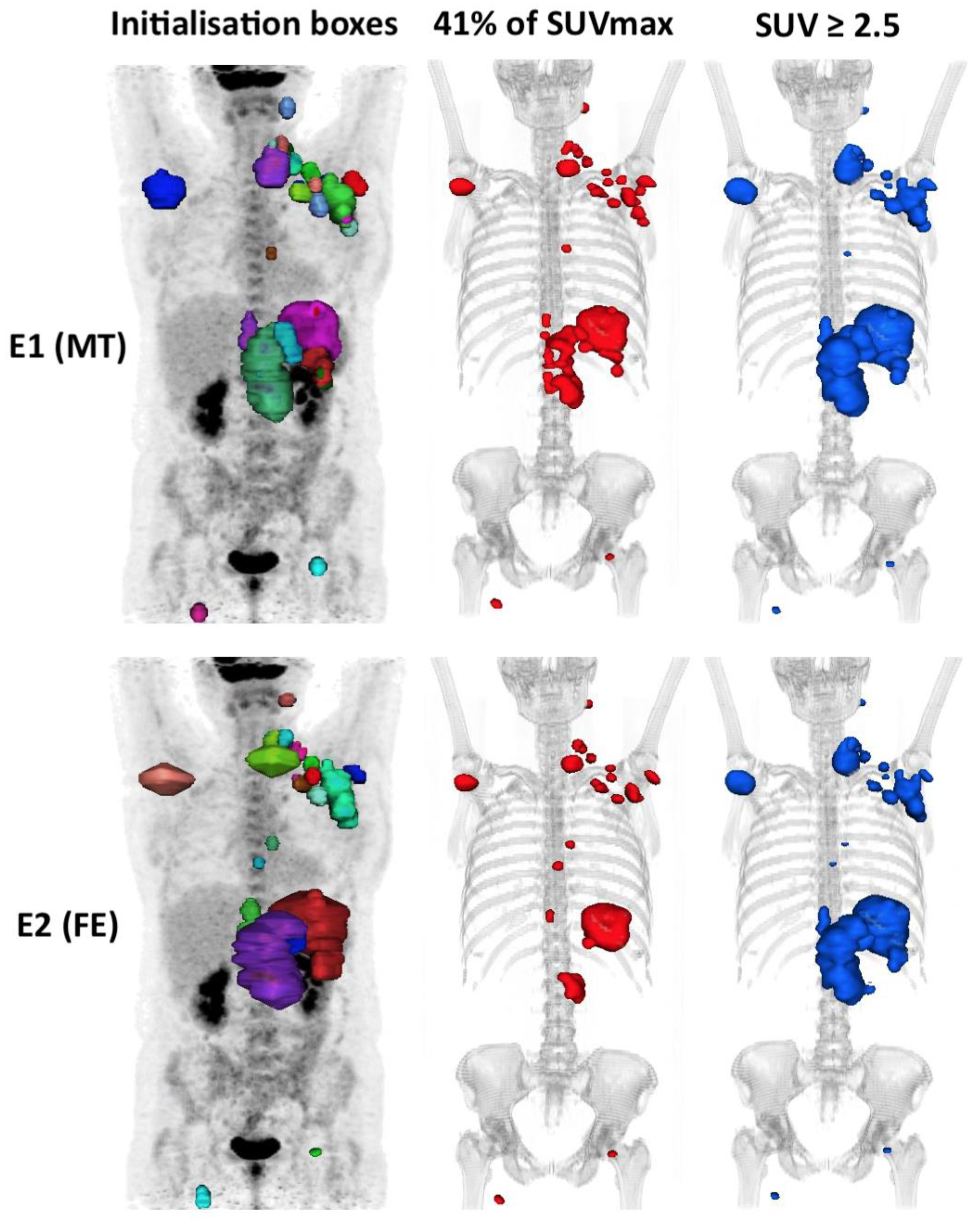
- A total of 4 percentage and absolute thresholds: 41% SUVmax (MTV41%) corresponding to volume with counts ≥ 41% of the maximum SUV within individual tumour regions, considered thereafter as the reference [23,30]; SUV ≥ 2.5 (MTV2.5) [11]; SUV ≥ liver SUVmax (MTVLiv); SUV ≥ PERCIST SUV (MTVPer) with PERCIST SUV = 1.5 × (liver mean SUV) + 2 standard deviations [24].
- -
- A total of 4 adaptives based on mathematic algorithms: Daisne modified by Vauclin et al. (MTVDai), which iteratively adapts the threshold according to the local signal-to-background ratio [27]; Fitting (MTVFit), which fits the sphere image using a 3-dimensional geometric model based on the spatial resolution in the reconstructed images and on a tumour shape derived from activity thresholding [31]; Nestle (MTVNes) according to the tumour and background intensities [32]; Black (MTVBla) according to the SUVmean [33].
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armitage, J.O.; Gascoyne, R.D.; Lunning, M.A.; Cavalli, F. Non-Hodgkin lymphoma. Lancet 2017, 390, 298–310. [Google Scholar] [CrossRef]
- Coiffier, B.B.; Thieblemont, C.; Neste, E.V.D.; Lepeu, G.; Plantier, I.; Castaigne, S.; Lefort, S.; Marit, G.; Macro, M.; Sebban, C.; et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: A study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood 2010, 116, 2040–2045. [Google Scholar] [CrossRef]
- Friedberg, J.W. Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Hematology 2011, 2011, 498–505. [Google Scholar] [CrossRef]
- Gisselbrecht, C.; Glass, B.; Mounier, N.; Singh Gill, D.; Linch, D.C.; Trneny, M.; Bosly, A.; Ketterer, N.; Shpilberg, O.; Hagberg, H.; et al. Salvage Regimens with Autologous Trans-plantation for Relapsed Large B-Cell Lymphoma in the Rituximab Era. J. Clin. Oncol. 2010, 28, 4184–4190. [Google Scholar] [CrossRef]
- Ceriani, L.; Gritti, G.; Cascione, L.; Pirosa, M.C.; Polino, A.; Ruberto, T.; Stathis, A.; Bruno, A.; Moccia, A.A.; Giovanella, L.; et al. SAKK38/07 study: Integration of baseline metabolic heterogeneity and metabolic tumor volume in DLBCL prognostic model. Blood Adv. 2020, 4, 1082–1092. [Google Scholar] [CrossRef]
- Thieblemont, C.; Bernard, S.; Meignan, M.; Molina, T.J. Optimizing initial therapy in DLBCL. Best Pr. Res. Clin. Haematol. 2018, 31, 199–208. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef] [PubMed]
- Lanic, H.; Mareschal, S.; Mechken, F.; Picquenot, J.-M.; Cornic, M.; Maingonnat, C.; Bertrand, P.; Clatot, F.; Bohers, E.; Stamatoullas, A.; et al. Interim positron emission tomography scan associated with international prognostic index and germinal center B cell-like signature as prognostic index in diffuse large B-cell lymphoma. Leuk. Lymphoma 2011, 53, 34–42. [Google Scholar] [CrossRef]
- Casasnovas, R.-O.; Meignan, M.; Berriolo-Riedinger, A.; Bardet, S.; Julian, A.; Thieblemont, C.; Vera, P.; Bologna, S.; Brière, J.; Jais, J.-P.; et al. SUVmax reduction improves early prognosis value of interim positron emission tomography scans in diffuse large B-cell lymphoma. Blood 2011, 118, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.N.; Vera, P.; Tilly, H.; Jardin, F.; Becker, S. Comparison of therapeutic evaluation criteria in FDG-PET/CT in patients with diffuse large-cell B-cell lymphoma: Prognostic impact of tumor/liver ratio. PLoS ONE 2019, 14, e0211649. [Google Scholar] [CrossRef] [PubMed]
- Mikhaeel, N.G.; Smith, D.; Dunn, J.T.; Phillips, M.; Møller, H.; Fields, P.A.; Wrench, D.; Barrington, S.F. Combination of baseline metabolic tumour volume and early response on PET/CT improves progression-free survival prediction in DLBCL. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1209–1219. [Google Scholar] [CrossRef]
- Itti, E.; Meignan, M.; Berriolo-Riedinger, A.; Biggi, A.; Cashen, A.F.; Véra, P.; Tilly, H.; Siegel, B.A.; Gallamini, A.; Casasnovas, R.-O.; et al. An international confirmatory study of the prognostic value of early PET/CT in diffuse large B-cell lymphoma: Comparison between Deauville criteria and ΔSUVmax. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1312–1320. [Google Scholar] [CrossRef]
- Barrington, S.F.; Kluge, R. FDG PET for therapy monitoring in Hodgkin and non-Hodgkin lymphomas. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 97–110. [Google Scholar] [CrossRef]
- Sasanelli, M.; Meignan, M.; Haioun, C.; Berriolo-Riedinger, A.; Casasnovas, R.-O.; Biggi, A.; Gallamini, A.; Siegel, B.A.; Cashen, A.F.; Véra, P.; et al. Pretherapy metabolic tumour volume is an independent predictor of outcome in patients with diffuse large B-cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2017–2022. [Google Scholar] [CrossRef]
- Song, M.-K.; Chung, J.-S.; Shin, H.-J.; Lee, S.-M.; Lee, S.-E.; Lee, H.-S.; Lee, G.-W.; Kim, S.-J.; Lee, S.-M.; Chung, D.-S. Clinical significance of metabolic tumor volume by PET/CT in stages II and III of diffuse large B cell lymphoma without extranodal site involvement. Ann. Hematol. 2011, 91, 697–703. [Google Scholar] [CrossRef]
- Kim, J.; Hong, J.; Kim, S.G.; Hwang, K.H.; Kim, M.; Ahn, H.K.; Sym, S.J.; Park, J.; Cho, E.K.; Shin, D.B.; et al. Prognostic Value of Metabolic Tumor Volume Estimated by 18 F-FDG Positron Emission Tomography/Computed Tomography in Patients with Diffuse Large B-Cell Lymphoma of Stage II or III Disease. Nucl. Med. Mol. Imaging 2014, 48, 187–195. [Google Scholar] [CrossRef]
- Toledano, M.N.; Desbordes, P.; Banjar, A.; Gardin, I.; Vera, P.; Ruminy, P.; Jardin, F.; Tilly, H.; Becker, S. Combination of baseline FDG PET/CT total metabolic tumour volume and gene expression profile have a robust predictive value in patients with diffuse large B-cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 680–688. [Google Scholar] [CrossRef]
- Barrington, S.F.; Meignan, M.A. Time to Prepare for Risk Adaptation in Lymphoma by Standardizing Measurement of Metabolic Tumor Burden. J. Nucl. Med. 2019, 60, 1096–1102. [Google Scholar] [CrossRef]
- Comelli, A.; Stefano, A.; Russo, G.; Bignardi, S.; Sabini, M.G.; Petrucci, G.; Ippolito, M.; Yezzi, A. K-nearest neighbor driving active contours to delineate biological tumor volumes. Eng. Appl. Artif. Intell. 2019, 81, 133–144. [Google Scholar] [CrossRef]
- Stefano, A.; Comelli, A.; Bravata, V.; Barone, S.; Daskalovski, I.; Savoca, G.; Sabini, M.G.; Ippolito, M.; Russo, G. A preliminary PET radiomics study of brain me-tastases using a fully automatic segmentation method. BMC Bioinform. 2020, 21, 325. [Google Scholar] [CrossRef]
- Capobianco, N.; Meignan, M.A.; Cottereau, A.-S.; Vercellino, L.; Sibille, L.; Spottiswoode, B.; Zuehlsdorff, S.; Casasnovas, O.; Thieblemont, C.; Buvat, I. Deep-Learning 18F-FDG Uptake Classification Enables Total Metabolic Tumor Volume Estimation in Diffuse Large B-Cell Lymphoma. J. Nucl. Med. 2021, 62, 30–36. [Google Scholar] [CrossRef]
- Im, H.-J.; Bradshaw, T.; Solaiyappan, M.; Cho, S.Y. Current Methods to Define Metabolic Tumor Volume in Positron Emission Tomography: Which One is Better? Nucl. Med. Mol. Imaging. Févr. 2018, 52, 5–15. [Google Scholar] [CrossRef]
- Meignan, M.; Sasanelli, M.; Casasnovas, R.O.; Luminari, S.; Fioroni, F.; Coriani, C.; Masset, H.; Itti, E.; Gobbi, P.G.; Merli, F.; et al. Metabolic tumour volumes measured at staging in lymphoma: Methodological evaluation on phantom experiments and patients. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1113–1122. [Google Scholar] [CrossRef]
- Ilyas, H.; Mikhaeel, N.G.; Dunn, J.T.; Rahman, F.; Møller, H.; Smith, D.; Barrington, S.F. Defining the optimal method for measuring baseline metabolic tumour volume in diffuse large B cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1142–1154. [Google Scholar] [CrossRef]
- Cottereau, A.-S.; Lanic, H.; Mareschal, S.; Meignan, M.; Vera, P.; Tilly, H.; Jardin, F.; Becker, S. Molecular Profile and FDG-PET/CT Total Metabolic Tumor Volume Improve Risk Classification at Diagnosis for Patients with Diffuse Large B-Cell Lymphoma. Clin. Cancer Res. 2016, 22, 3801–3809. [Google Scholar] [CrossRef]
- Song, M.-K.; Yang, D.-H.; Lee, G.-W.; Lim, S.-N.; Shin, S.; Pak, K.J.; Kwon, S.Y.; Shim, H.K.; Choi, B.-H.; Kim, I.-S.; et al. High total metabolic tumor volume in PET/CT predicts worse prognosis in diffuse large B cell lymphoma patients with bone marrow involvement in rituximab era. Leuk. Res. 2016, 42, 1–6. [Google Scholar] [CrossRef]
- Vauclin, S.; Doyeux, K.; Hapdey, S.; Edet-Sanson, A.; Vera, P.; Gardin, I. Development of a generic thresholding algorithm for the delineation of18FDG-PET-positive tissue: Application to the comparison of three thresholding models. Phys. Med. Biol. 2009, 54, 6901–6916. [Google Scholar] [CrossRef]
- Tout, M.; Casasnovas, O.; Meignan, M.; Lamy, T.; Morschhauser, F.; Salles, G.; Gyan, E.; Haioun, C.; Mercier, M.; Feugier, P.; et al. Rituximab exposure is influenced by baseline metabolic tumor volume and predicts outcome of DLBCL patients: A Lymphoma Study Association report. Blood 2017, 129, 2616–2623. [Google Scholar] [CrossRef]
- Comelli, A.; Bignardi, S.; Stefano, A.; Russo, G.; Sabini, M.G.; Ippolito, M.; Yezzi, A. Development of a new fully three-dimensional methodology for tumours delineation in functional images. Comput. Biol. Med. 2020, 120, 103701. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Tylski, P.; Stute, S.; Grotus, N.; Doyeux, K.; Hapdey, S.; Gardin, I.; Vanderlinden, B.; Buvat, I. Comparative Assessment of Methods for Estimating Tumor Volume and Standardized Uptake Value in 18F-FDG PET. J. Nucl. Med. 2010, 51, 268–276. [Google Scholar] [CrossRef]
- Nestle, U.; Kremp, S.; Schaefer-Schuler, A.; Sebastian-Welsch, C.; Hellwig, D.; Rübe, C.; Kirsch, C.-M. Comparison of different methods for delineation of 18F-FDG PET-positive tissue for target volume definition in radiotherapy of patients with non-Small cell lung cancer. J. Nucl. Med. 2005, 46, 1342–1348. [Google Scholar]
- Black, Q.C.; Grills, I.S.; Kestin, L.L.; Wong, C.-Y.O.; Wong, J.W.; Martinez, A.A.; Yan, D. Defining a radiotherapy target with positron emission tomography. Int. J. Radiat. Oncol. 2004, 60, 1272–1282. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 10 November 2020).
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Kendall, M.G. A new measure of rank correlation. Biometrika 1938, 30, 81–93. [Google Scholar] [CrossRef]
- Davison, A.C.; Hinkley, D.V. Bootstrap Methods and Their Application (Cambridge Series in Statistical and Probabilistic Mathematics); Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Heagerty, P.J.; Lumley, T.; Pepe, M.S. Time-Dependent ROC Curves for Censored Survival Data and a Diagnostic Marker. Biometrics 2000, 56, 337–344. [Google Scholar] [CrossRef]
- Hochberg, Y. A Sharper Bonferroni Procedure for Multiple Tests of Significance. Biometrika 1988, 75, 800–802. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | Total (n = 239) (%) |
|---|---|
| Diagnosis age (years), median (min; max) | 65.9 (18; 92) |
| Age ≥ 60 years | 152 (63.6) |
| Female | 124 (51.9) |
| Male | 115 (48.1) |
| ECOG Performance Status (%) | |
| 0 | 106 (44.4) |
| 1 | 72 (30.1) |
| 2 | 35 (14.6) |
| 3 | 24 (10.0) |
| 4 | 2 (0.8) |
| LDH (%) | |
| Normal | 79 (33.1) |
| Elevated (>480) | 160 (66.9) |
| Ann Arbor stage (%) | |
| I–II | 53 (22.2) |
| III–IV | 186 (77.8) |
| Extra-nodal sites ≥ 2 | 155 (64.9) |
| IPI score (%) | |
| Low (0–1) | 48 (20.0) |
| Low-intermediate (2) | 52 (21.8) |
| High-intermediate (3) | 67 (28.0) |
| High (4–5) | 72 (30.2) |
| Chemotherapy (%) | |
| R-ACVBP | 67 (28.0) |
| R-CHOP and others * | 172 (72.0) |
| Method | E | Mean | SD | Min. | Q1 = 25% | Median | Q3 = 75% | Max. |
|---|---|---|---|---|---|---|---|---|
| SUVmax 2.5 | E1 | 1017.02 | 1405.12 | 1.9 | 156.61 | 609.38 | 1381.71 | 12117.25 |
| E2 | 1023.15 | 1319.56 | 4.16 | 167.92 | 618.46 | 1340.28 | 10065.02 | |
| 41% SUVmax | E1 | 512.37 | 645.57 | 3.77 | 80.54 | 304.57 | 706.21 | 4549.41 |
| E2 | 440.65 | 500.27 | 3.47 | 74.61 | 263.73 | 588.83 | 2843.38 | |
| Liver SUVmax | E1 | 907.61 | 1406.49 | 0.07 | 105.52 | 494.39 | 1317.90 | 13662.33 |
| E2 | 905.03 | 1302.67 | 0.08 | 106.28 | 478.78 | 1303.99 | 11662.33 | |
| PERCIST | E1 | 905.84 | 1510.22 | 0.00 | 87.71 | 487.00 | 1208.41 | 14276.43 |
| E2 | 899.24 | 1457.80 | 0.00 | 86.26 | 445.04 | 1228.28 | 12332.37 | |
| Daisne | E1 | 474.19 | 544.20 | 2.57 | 77.42 | 309.55 | 678.68 | 3573.04 |
| E2 | 432.00 | 476.33 | 2.87 | 79.28 | 252.98 | 594.22 | 2621.32 | |
| Nestle | E1 | 569.24 | 666.84 | 1.99 | 95.73 | 359.19 | 806.33 | 4383.07 |
| E2 | 551.95 | 624.80 | 2.61 | 90.61 | 324.54 | 746.83 | 3753.35 | |
| Fitting | E1 | 623.27 | 797.44 | 2.90 | 104.70 | 356.58 | 844.97 | 5588.33 |
| E2 | 546.74 | 659.45 | 3.20 | 93.72 | 311.25 | 719.15 | 4227.48 | |
| Black | E1 | 813.05 | 1212.58 | 5.62 | 118.97 | 454.26 | 1085.04 | 10328.49 |
| E2 | 794.46 | 1099.18 | 7.17 | 123.88 | 414.65 | 1094.36 | 8067.13 |
| Segmentation Method | ICC (n = 239) (95% CI) | Kendall’s Tau (n = 239) (95% CI) |
|---|---|---|
| SUV ≥ liver SUVmax | 0.96 (0.89–0.98) | 0.93 (0.87–0.95) |
| PERCIST SUV | 0.95 (0.87–0.98) | 0.93 (0.88–0.96) |
| SUV ≥ 2.5 | 0.94 (0.85–0.98) | 0.92 (0.87–0.94) |
| Black | 0.94 (0.83–0.98) | 0.89 (0.84–0.92) |
| Nestle | 0.91 (0.76–0.97) | 0.89 (0.83–0.92) |
| Fitting | 0.88 (0.68–0.96) | 0.88 (0.83–0.92) |
| Daisne | 0.88 (0.73–0.95) | 0.86 (0.80–0.90) |
| 41% of SUVmax | 0.82 (0.66–0.92) | 0.85 (0.80–0.89) |
| Methods | SUVmax ≥ 2.5 | 41% of SUVmax | Liver SUVmax | PERCIST | Daisne | Nestle | Fitting | Black |
|---|---|---|---|---|---|---|---|---|
| SUVmax ≥ 2.5 | - | 0.12 (0.03 to 0.27) p = 0.038 | −0.01 (−0.09 to 0.01) p = 0.82 | −0.01 (−0.02 to 0.01) p = 0.82 | 0.06 (−0.01 to 0.21) p = 0.72 | 0.03 (0.01 to 0.1) p = 0.038 | 0.06 (0.02 to 0.17) p = 0.023 | 0.01 (−0.01 to 0.02) p = 0.82 |
| 41% of SUVmax | −0.07 (−0.1 to −0.04) p = 0.01 | - | −0.13 (−0.28 to −0.05) p = 0.023 | −0.12 (−0.27 to −0.03) p = 0.038 | −0.06 (−0.10 to −0.03) p = 0.023 | −0.09 (−0.21 to 0.01) p = 0.77 | −0.06 (−0.19 to 0.06) p = 0.82 | −0.11 (−0.27 to −0.02) p = 0.102 |
| Liver SUVmax | 0.01 (−0.01 to 0.02) p = 0.74 | 0.07 (0.05 to 0.12) p = 0.01 | - | 0.01 (−0.01 to 0.06) p = 0.82 | 0.08 (0.01 to 0.23) p = 0.072 | 0.05 (0.01 to 0.17) p = 0.144 | 0.08 (0.02 to 0.25) p = 0.023 | 0.02 (−0.01 to 0.11) p = 0.82 |
| PERCIST | 0.01 (0.01 to 0.03) p = 0.07 | 0.08 (0.05 to 0.13) p = 0.01 | 0.01 (−0.01 to 0.02) p = 0.7 | - | 0.07 (0.01 to 0.22) p = 0.42 | 0.04 (0.01 to 0.12) p = 0.038 | 0.07 (0.02 to 0.2) p = 0.023 | 0.01 (−0.01 to 0.04) p = 0.82 |
| Daisne | −0.06 (−0.10 to −0.03) p = 0.01 | 0.01 (−0.01 to 0.03) p = 0.7 | −0.06 (−0.11 to −0.03) p = 0.01 | −0.07 (−0.11 to −0.04) p = 0.01 | - | −0.03 (−0.15 to 0.04) p = 0.82 | −0.01 (−0.11 to 0.11) p = 0.99 | −0.05 (−0.21 to 0.01) p = 0.82 |
| Nestle | −0.03 (−0.07 to −0.01) p = 0.01 | 0.03 (0.02 to 0.05) p = 0.01 | −0.04 (−0.08 to −0.02) p = 0.01 | −0.05 (−0.09 to −0.03) p = 0.01 | 0.02 (0.01 to 0.04) p = 0.01 | - | 0.03 (0.01 to 0.08) p = 0.42 | −0.03 (−0.09 to −0.01) p = 0.52 |
| Fitting | −0.03 (−0.07 to −0.02) p = 0.01 | 0.03 (0.02 to 0.06) p = 0.01 | −0.04 (−0.08 to −0.02) p = 0.01 | −0.05 (−0.09 to −0.03) p = 0.01 | 0.02 (0.01 to 0.04) p = 0.07 | −0.01 (−0.01 to 0.01) p = 0.86 | - | −0.06 (−0.16 to −0.02) p = 0.023 |
| Black | −0.02 (−0.06 to −0.01) p = 0.01 | 0.04 (0.02 to 0.08) p = 0.01 | −0.03 (−0.07 to −0.01) p = 0.01 | −0.04 (−0.08 to −0.02) p = 0.01 | 0.03 (0.01 to 0.07) p = 0.03 | 0.01 (−0.01 to 0.05) p = 0.74 | 0.01 (−0.01 to 0.04) p = 0.74 | - |
| Method | Se (%) | Sp (%) | Mean AUC | Cut-off (cm3) | Cut-off 1 (cm3) | Cut-off 2 (cm3) | ∣ΔCut-off∣(cm3) | Low MTV 1 (n=) | Low MTV 2 (n=) | ∣Δlow MTV∣ (n=) |
|---|---|---|---|---|---|---|---|---|---|---|
| SUVmax ≥ 2.5 | 67.1 | 61.1 | 0.655 | 552 | 548 | 555 | 7 | 115 | 114 | 1 |
| 41% of SUVmax | 64.8 | 63.8 | 0.672 | 295 | 324 | 252 | 72 | 117 | 125 | 8 |
| Liver SUVmax | 63.4 | 61.9 | 0.644 | 487 | 483 | 500 | 17 | 119 | 120 | 1 |
| PERCIST | 63.1 | 62.6 | 0.638 | 486 | 426 | 465 | 39 | 119 | 125 | 6 |
| Daisne | 61.7 | 67.3 | 0.671 | 340 | 334 | 345 | 11 | 126 | 132 | 6 |
| Nestle | 63.5 | 67.3 | 0.671 | 396 | 398 | 386 | 12 | 123 | 128 | 5 |
| Fitting | 64.3 | 64.9 | 0.667 | 352 | 360 | 335 | 25 | 119 | 126 | 7 |
| Black | 64.8 | 65.3 | 0.662 | 460 | 379 | 427 | 48 | 121 | 124 | 3 |
| Disease-Free Survival | Overall Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient (SE) | HR (95% CI) | p-Value | p Value (Hochberg Correction) | Coefficient (SE) | HR (95% CI) | p Value | p Value (Hochberg Correction) | ||
| IPI score | 0–2 | 1 | 0.02 | 0.02 | 1 | ||||
| 3–5 | 0.59 (0.24) | 1.8 | 0.66 (0.27) | 1.93 | 0.02 | 0.02 | |||
| (1.12–2.89) | (1.13–3.31) | ||||||||
| CT | ACVBP | 1 | 0.0001 | 0.0002 | 1 | ||||
| CHOP * | 1.11 (0.29) | 3.04 | 1.14 (0.32) | 3.12 | 0.0003 | 0.0006 | |||
| (1.73–5.33) | (1.68–5.83) | ||||||||
| MTV 41% | <295 cm3 | 0.84 (0.22) | 1 | 0.0001 | 0.0002 | 1 | |||
| ≥295 cm3 | 2.31 | 1.00 (0.25) | 2.72 | <0.0001 | 0.0003 | ||||
| (1.50–3.55) | (1.68–4.41) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eude, F.; Toledano, M.N.; Vera, P.; Tilly, H.; Mihailescu, S.-D.; Becker, S. Reproducibility of Baseline Tumour Metabolic Volume Measurements in Diffuse Large B-Cell Lymphoma: Is There a Superior Method? Metabolites 2021, 11, 72. https://doi.org/10.3390/metabo11020072
Eude F, Toledano MN, Vera P, Tilly H, Mihailescu S-D, Becker S. Reproducibility of Baseline Tumour Metabolic Volume Measurements in Diffuse Large B-Cell Lymphoma: Is There a Superior Method? Metabolites. 2021; 11(2):72. https://doi.org/10.3390/metabo11020072
Chicago/Turabian StyleEude, Florian, Mathieu Nessim Toledano, Pierre Vera, Hervé Tilly, Sorina-Dana Mihailescu, and Stéphanie Becker. 2021. "Reproducibility of Baseline Tumour Metabolic Volume Measurements in Diffuse Large B-Cell Lymphoma: Is There a Superior Method?" Metabolites 11, no. 2: 72. https://doi.org/10.3390/metabo11020072
APA StyleEude, F., Toledano, M. N., Vera, P., Tilly, H., Mihailescu, S.-D., & Becker, S. (2021). Reproducibility of Baseline Tumour Metabolic Volume Measurements in Diffuse Large B-Cell Lymphoma: Is There a Superior Method? Metabolites, 11(2), 72. https://doi.org/10.3390/metabo11020072