
Exhaled Metabolite Patterns to Identify Recent Asthma Exacerbations

 ,
,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Discriminant Analysis
2.3. Sensitivity Analysis
3. Discussion
4. Materials and Methods
4.1. Population
4.2. Outcomes
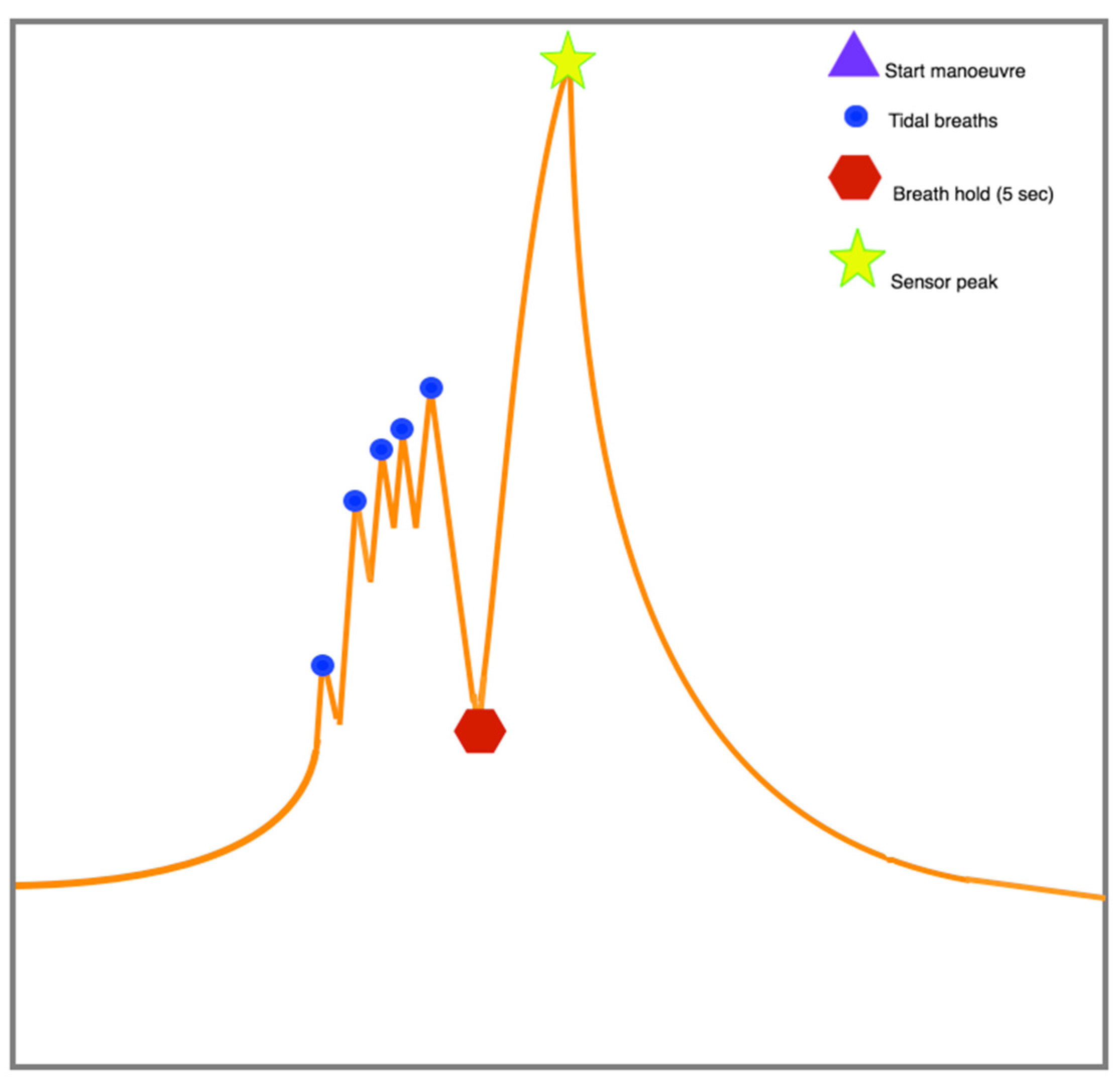
4.3. Exhaled Breath Analysis
4.4. Statistical Analysis
4.5. Sensitivity Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- To, T.; Stanojevic, S.; Moores, G.; Gershon, A.S.; Bateman, E.D.; Cruz, A.A.; Boulet, L.P. Global Asthma Prevalence in Adults: Findings from the Cross-Sectional World Health Survey. BMC Public Health 2012, 12, 204. [Google Scholar] [CrossRef] [Green Version]
- Masoli, M.; Fabian, D.; Holt, S.; Beasley, R.; Global Initiative for Asthma (GINA) Program. The Global Burden of Asthma: Executive Summary of the GINA Dissemination Committee Report. Allergy 2004, 59, 469–478. [Google Scholar] [CrossRef]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.-P.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations—Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef] [Green Version]
- Williams, L.K.; Peterson, E.L.; Wells, K.; Ahmedani, B.K.; Kumar, R.; Burchard, E.G.; Chowdhry, V.K.; Favro, D.; Lanfear, D.E.; Pladevall, M. Quantifying the Proportion of Severe Asthma Exacerbations Attributable to Inhaled Corticosteroid Nonadherence. J. Allergy Clin. Immunol. 2011, 128, 1185–1191.e2. [Google Scholar] [CrossRef] [Green Version]
- Global Initiative for Asthma—Global Initiative for Asthma—GINA. Available online: https://ginasthma.org/ (accessed on 7 July 2021).
- Castillo, J.R.; Peters, S.P.; Busse, W.W. Asthma Exacerbations: Pathogenesis, Prevention, and Treatment. J. Allergy Clin. Immunol. Pract. 2017, 5, 918–927. [Google Scholar] [CrossRef]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Age-Sex-Specific Mortality for 282 Causes of Death in 195 Countries and Territories, 1980–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Chung, K.F. Asthma Phenotyping: A Necessity for Improved Therapeutic Precision and New Targeted Therapies. J. Intern. Med. 2016, 279, 192–204. [Google Scholar] [CrossRef]
- Bloom, C.I.; Palmer, T.; Feary, J.; Quint, J.K.; Cullinan, P. Exacerbation Patterns in Adults with Asthma in England. A Population-Based Study. Am. J. Respir. Crit. Care Med. 2019, 199, 446–453. [Google Scholar] [CrossRef]
- Besa, V.; Teschler, H.; Kurth, I.; Khan, A.M.; Zarogoulidis, P.; Baumbach, J.I.; Sommerwerck, U.; Freitag, L.; Darwiche, K. Exhaled Volatile Organic Compounds Discriminate Patients with Chronic Obstructive Pulmonary Disease from Healthy Subjects. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Finamore, P.; Scarlata, S.; Incalzi, R.A. Breath analysis in respiratory diseases: state-of-the-art and future perspectives. Expert Rev. Mol. Diagn. 2018, 19, 47–61. [Google Scholar] [CrossRef]
- van der Schee, M.P.; Paff, T.; Brinkman, P.; van Aalderen, W.M.C.; Haarman, E.G.; Sterk, P.J. Breathomics in Lung Disease. Chest 2015, 147, 224–231. [Google Scholar] [CrossRef]
- De Vries, R.; Brinkman, P.; Van Der Schee, M.P.; Fens, N.; Dijkers, E.; Bootsma, S.; De Jongh, F.H.C.; Sterk, P.J. Integration of electronic nose technology with spirometry: validation of a new approach for exhaled breath analysis. J. Breath Res. 2015, 9, 046001. [Google Scholar] [CrossRef]
- De Vries, R.; Dagelet, Y.W.; Spoor, P.; Snoey, E.; Jak, P.M.; Brinkman, P.; Dijkers, E.; Bootsma, S.K.; Elskamp, F.; De Jongh, F.H.; et al. Clinical and inflammatory phenotyping by breathomics in chronic airway diseases irrespective of the diagnostic label. Eur. Respir. J. 2018, 51, 1701817. [Google Scholar] [CrossRef] [Green Version]
- Van Vliet, D.; Smolinska, A.; Jöbsis, Q.; Rosias, P.; Muris, J.; Dallinga, J.; Dompeling, E.; Van Schooten, F.-J. Can exhaled volatile organic compounds predict asthma exacerbations in children? J. Breath Res. 2017, 11, 016016. [Google Scholar] [CrossRef]
- Petsky, H.L.; Li, A.M.; Au, C.T.; Kynaston, J.A.; Turner, C.; Chang, A.B. Management Based on Exhaled Nitric Oxide Levels Adjusted for Atopy Reduces Asthma Exacerbations in Children: A Dual Centre Randomized Controlled Trial. Pediatr. Pulmonol. 2015, 50, 535–543. [Google Scholar] [CrossRef]
- Robroeks, C.M.; van Berkel, J.J.; Jöbsis, Q.; van Schooten, F.-J.; Dallinga, J.W.; Wouters, E.F.; Dompeling, E. Exhaled Volatile Organic Compounds Predict Exacerbations of Childhood Asthma in a 1-Year Prospective Study. Eur. Respir. J. 2013, 42, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Van Bragt, J.J.M.H.; Brinkman, P.; de Vries, R.; Vijverberg, S.J.H.; Weersink, E.J.M.; Haarman, E.G.; de Jongh, F.H.C.; Kester, S.; Lucas, A.; in ‘t Veen, J.C.C.M.; et al. Identification of Recent Exacerbations in COPD patients by Electronic Nose. ERJ Open Res. 2020, 6, 00307–02020. [Google Scholar] [CrossRef]
- Lammers, A.; Brinkman, P.; Nijenhuis, L.H.T.; de Vries, R.; Dagelet, Y.W.F.; Duijvelaar, E.; Xu, B.; Abdel-Aziz, M.I.; Vijverberg, S.J.; Neerincx, A.H.; et al. Increased day-to-day fluctuations in exhaled breath profiles after a rhinovirus challenge in asthma. Allergy 2021, 76, 2488–2499. [Google Scholar] [CrossRef]
- Pauwels, R.A. Similarities and Differences in Asthma and Chronic Obstructive Pulmonary Disease Exacerbations. Proc. Am. Thorac. Soc. 2004, 1, 73–76. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Couillard, S. Antibiotics for asthma attacks: masking uncertainty. Eur. Respir. J. 2021, 58, 2100183. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Updated 2021; GINA: Fontana, WI, USA, 2021. [Google Scholar]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Report 2021. 2021. Available online: https://goldcopd.org/2021-gold-reports/ (accessed on 7 July 2021).
- Velthove, K.J.; Bracke, M.; Souverein, P.C.; Schweizer, R.C.; Berg, M.J.T.; Leufkens, H.G.M.; van Solinge, W.W. Identification of Exacerbations in Obstructive Lung Disease Through Biomarkers. Biomarkers 2009, 14, 523–528. [Google Scholar] [CrossRef]
- Brinkman, P.; Wagener, A.H.; Hekking, P.-P.; Bansal, A.T.; Maitland-van der Zee, A.-H.; Wang, Y.; Weda, H.; Knobel, H.H.; Vink, T.J.; Rattray, N.J.; et al. Identification and Prospective Stability of Electronic Nose (Enose)–Derived Inflammatory Phenotypes in Patients with Severe Asthma. J. Allergy Clin. Immunol. 2019, 143, 1811–1820.e7. [Google Scholar] [CrossRef] [Green Version]
- Kirkham, P.A.; Barnes, P.J. Oxidative Stress in COPD. Chest 2013, 144, 266–273. [Google Scholar] [CrossRef]
- Principe, S.; van Bragt, J.J.M.H.; Longo, C.; de Vries, R.; Sterk, P.J.; Scichilone, N.; Vijverberg, S.J.H.; Maitland-van der Zee, A.H. The Influence of Smoking Status on Exhaled Breath Profiles in Asthma and COPD Patients. Molecules 2021, 26, 1357. [Google Scholar] [CrossRef]
- Van der Schee, M.P.; Palmay, R.; Cowan, J.O.; Taylor, D.R. Predicting Steroid Responsiveness in Patients with Asthma Using Exhaled Breath Profiling. Clin. Exp. Allergy 2013, 43, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Berchtold, C.; Bosilkovska, M.; Daali, Y.; Walder, B.; Zenobi, R. Real-Time Monitoring of Exhaled Drugs by Mass Spectrometry. Mass Spectrom. Rev. 2014, 33, 394–413. [Google Scholar] [CrossRef]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. Benralizumab, an Anti-Interleukin-5 Receptor α Monoclonal Antibody, as Add-on Treatment for Patients with Severe, Uncontrolled, Eosinophilic Asthma (CALIMA): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef]
- Postma, D.S.; Brightling, C.; Baldi, S.; van den Berge, M.; Fabbri, L.M.; Gagnatelli, A.; Papi, A.; van der Molen, T.; Rabe, K.F.; Siddiqui, S.; et al. Exploring the Relevance and Extent of Small Airways Dysfunction in Asthma (ATLANTIS): Baseline Data from a Prospective Cohort Study. Lancet Respir. Med. 2019, 7, 402–416. [Google Scholar] [CrossRef] [Green Version]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; Fitzgerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab Treatment in Patients with Severe Eosinophilic Asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrao, G.; Arfè, A.; Nicotra, F.; Ghirardi, A.; Vaghi, A.; de Marco, R.; Pesci, A.; Merlino, L.; Zambon, A. Persistence with Inhaled Corticosteroids Reduces the Risk of Exacerbation Among Adults with Asthma: A Real-World Investigation. Respirology 2016, 21, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Pont, L.G.; van der Werf, G.T.; Denig, P.; Haaijer-Ruskamp, F.M. Identifying General Practice Patients Diagnosed with Asthma and Their Exacerbation Episodes from Prescribing Data. Eur. J. Clin. Pharmacol. 2002, 57, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, P.W.; Ghushchyan, V.H.; Campbell, J.D.; Globe, G.; Bender, B.; Magid, D.J. Measuring the Cost of Poor Asthma Control and Exacerbations. J. Asthma 2016, 54, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Murphy, V.E.; Gibson, P.; Talbot, P.I.; Clifton, V.L. Severe Asthma Exacerbations during Pregnancy. Obstet. Gynecol. 2005, 106, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- De Vries, R.; Sterk, P.J. eNose Breathprints as Composite Biomarker for Real-Time Phenotyping of Complex Respiratory Diseases. J. Allergy Clin. Immunol. 2020, 146, 995–996. [Google Scholar] [CrossRef]
- Wheelock, C.E.; Goss, V.M.; Balgoma, D.; Nicholas, B.; Brandsma, J.; Skipp, P.J.; Snowden, S.; Burg, D.; D’Amico, A.; Horvath, I.; et al. Application of ’omics Technologies to Biomarker Discovery in Inflammatory Lung Diseases. Eur. Respir. J. 2013, 42, 802–825. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aziz, M.I.; Brinkman, P.; Vijverberg, S.J.H.; Neerincx, A.H.; de Vries, R.; Dagelet, Y.W.F.; Riley, J.H.; Hashimoto, S.; Montuschi, P.; Chung, K.F.; et al. eNose Breath Prints as a Surrogate Biomarker for Classifying Patients with Asthma by Atopy. J. Allergy Clin. Immunol. 2020, 146, 1045–1055. [Google Scholar] [CrossRef] [PubMed]
- Wu, W. Predicting Atopic Asthma by Using eNose Breath Profiles with Machine Learning. J. Allergy Clin. Immunol. 2020, 146, 1010–1012. [Google Scholar] [CrossRef]
- Romain, A.C.; Nicolas, J. Long Term Stability of Metal Oxide-Based Gas Sensors for e-Nose Environmental Applications: An Overview. Sensors Actuators B Chem. 2010, 146, 502–506. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Training Dataset | Exacerbation | No Exacerbation | |
|---|---|---|---|
| n | 252 | 41 | 211 |
| Age (years), mean (SD) | 48.3 (18.1) | 51.3 (16.1) | 47.7 (18.5) |
| Gender, male (n, %), | 89 (35.3) | 9 (22.0) | 80 (38.0) |
| BMI (kg/m2), mean (SD) | 27.4 (6.5) | 26.7 (5.0) | 27.5 (6.8) |
| Smoking (never/ex/current), n | 173/65/13 | 26/15/0 | 147/50/13 |
| Pack-years, median (IQR) | 5.0 (2.0–8.0) | 4.8 (2.0–8.8) | 5.0 (2.0–8.0) |
| Exacerbations *, n (%) | 41 (16.3) | 41 (100) | 0 (0) |
| Previous AB use #, n (%) | 23 (9.1) | 17 (41.5) | 6 (2.8) |
| FEV1 as % of predicted, mean (SD) | 88.4 (22.0) | 88.4 (25.0) | 87.2 (20.9) |
| Post-bronchodilator FEV1 as % of predicted, mean (SD) | 90.1 (20.0) | 88.0 (19.7) | 92.7 (20.0) |
| FEV1/FVC as % of predicted, mean (SD) | 86.7 (15.4) | 87.8 (14.1) | 86.7 (15.6) |
| Post-bronchodilator FEV1/FVC as % of predicted, mean (SD) | 89.1 (14.6) | 86.9 (14.5) | 90.9 (14.4) |
| Blood eosinophils (cells·µL−1), median (IQR) | 0.21 (0.09–0.42) | 0.24 (0.11–0.47) | 0.21 (0.09–0.42) |
| Blood neutrophils (cells·µL−1), median (IQR) | 4.8 (3.5–6.0) | 5.5 (4.3–7.5) | 4.5 (3.4–6.2) |
| FeNO (ppb), median (IQR) | 25.5 (15.0–41.0) | 28.0 (17.5–39.5) | 22.0 (13.0–47.5) |
| ACQ score, mean (SD) | 1.8 (1.4) | 1.8 (1.4) | 1.7 (1.4) |
| ACQ-score > 1.5 (n, %) | 130 (51.6) | 23 (56.1) | 98 (46.4) |
| Allergy †, yes, n (%) | 183 (72.6) | 29 (70.1) | 151 (71.6) |
| Use of ICS, yes, n (%) | 213 (84.5) | 37 (90.2) | 176 (70.1) |
| Total Validation Dataset | Exacerbation | No Exacerbation | |
|---|---|---|---|
| n | 109 | 11 | 98 |
| Age (years), mean (SD) | 48.2 (16.2) | 55.7 (17.1) | 47.3 (15.9) |
| Gender, male (n, %), | 40 (36.7) | 5 (45.5) | 35 (35.7) |
| BMI (kg/m2), mean (SD) | 28.3 (6.0) | 29.5 (7.1) | 28.1 (5.9) |
| Smoking (never/ex/current), n | 85/14/10 | 10/1/0 | 75/13/10 |
| Pack-years, median (IQR) | 4.4 (2.5–8.5) | 5.0 (5.0–5.0) | 4.3 (2.3–8.8) |
| Exacerbations *, n (%) | 11 (10.1) | 11 (100) | 0 (0) |
| Previous AB use #, n (%) | 5 (4.6) | 3 (27.3) | 2 (2.0) |
| FEV1 as % of predicted, mean (SD) | 86.4 (21.0) | 78.4 (25.7) | 87.4 (20.3) |
| Post-bronchodilator FEV1 as % of predicted, mean (SD) | 89.8 (17.6) | 81.4 (19.7) | 91.2 (17.0) |
| FEV1/FVC as % of predicted, mean (SD) | 85.1 (14.9) | 74.5 (24.0) | 86.5 (13.0) |
| Post-bronchodilator FEV1/FVC as % of predicted, mean (SD) | 87.0 (14.5) | 75.5 (20.2) | 88.9 (12.6) |
| Blood eosinophils (cells·µL−1), median (IQR) | 0.22 (0.10–0.40) | 0.28 (0.12–0.47) | 0.21 (0.10–0.40) |
| Blood neutrophils (cells·µL−1), median (IQR) | 4.6 (3.6–6.1) | 5.6 (4.5–7.4) | 4.5 (3.6–5.8) |
| FeNO (ppb), median (IQR) | 25.0 (15.3–39.0) | 34.5 (24.0–39.0) | 24.5 (14.8–39.0) |
| ACQ score, mean (SD) | 1.8 (1.2) | 2.3 (1.2) | 1.8 (1.2) |
| ACQ-score > 1.5 (n, %) | 65 (59.6) | 9 (81.8) | 56 (57.1) |
| Allergy †, yes, n (%) | 76 (69.7) | 9 (81.8) | 67 (68.4) |
| Use of ICS, yes, n (%) | 95 (87.2) | 10 (90.9) | 85 (86.7) |
| Training AUC | Cross-Validated AUC | Validation AUC | |
|---|---|---|---|
| All asthma patients (n = 361) | 0.78 (0.72–0.84) | 0.76 (0.70–0.83) | 0.76 (0.64–0.87) |
| Without antibiotics users (n = 333) * | 0.81 (0.75–0.87) | 0.79 (0.72–0.85) | 0.81 (0.70–0.92) |
| Without current smokers (n = 338) | 0.77 (0.71–0.84) | 0.75 (0.68–0.82) | 0.74 (0.60–0.87) |
| Only with patients who use maintenance ICS (n = 308) | 0.83 (0.78–0.89) | 0.81 (0.76–0.87) | 0.84 (0.75–0.93) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Bragt, J.J.M.H.; Principe, S.; Hashimoto, S.; Versteeg, D.N.; Brinkman, P.; Vijverberg, S.J.H.; Weersink, E.J.M.; Scichilone, N.; Maitland-van der Zee, A.H. Exhaled Metabolite Patterns to Identify Recent Asthma Exacerbations. Metabolites 2021, 11, 872. https://doi.org/10.3390/metabo11120872
van Bragt JJMH, Principe S, Hashimoto S, Versteeg DN, Brinkman P, Vijverberg SJH, Weersink EJM, Scichilone N, Maitland-van der Zee AH. Exhaled Metabolite Patterns to Identify Recent Asthma Exacerbations. Metabolites. 2021; 11(12):872. https://doi.org/10.3390/metabo11120872
Chicago/Turabian Stylevan Bragt, Job J. M. H., Stefania Principe, Simone Hashimoto, D. Naomi Versteeg, Paul Brinkman, Susanne J. H. Vijverberg, Els J. M. Weersink, Nicola Scichilone, and Anke H. Maitland-van der Zee. 2021. "Exhaled Metabolite Patterns to Identify Recent Asthma Exacerbations" Metabolites 11, no. 12: 872. https://doi.org/10.3390/metabo11120872
APA Stylevan Bragt, J. J. M. H., Principe, S., Hashimoto, S., Versteeg, D. N., Brinkman, P., Vijverberg, S. J. H., Weersink, E. J. M., Scichilone, N., & Maitland-van der Zee, A. H. (2021). Exhaled Metabolite Patterns to Identify Recent Asthma Exacerbations. Metabolites, 11(12), 872. https://doi.org/10.3390/metabo11120872