Open Innovation in Digital Healthcare: Users’ Discrimination between Certified and Non-Certified mHealth Applications



Abstract
1. Introduction
2. Theoretical Background and Related Work
2.1. Apps and Certified Quality
2.2. Online User Reviews
3. Materials and Methods
3.1. Sample
3.2. Data Analysis and Collection
- X → 1, 2, …, i
- Y → 1, 2, …, j
- Z → 1, 2, …, k
- = frequency determined for the ijk cell in the contingency table
- = Main impact of the X variable
- = Main impact of the Y variable
- = Main impact of the Z variable
- = Second degree interaction impact of variables X and Y
- = Second degree interaction impact of variables Y and Z
4. Results. Analysis and discussion
4.1. Sample Characteristics
4.2. Hypotheses Testing
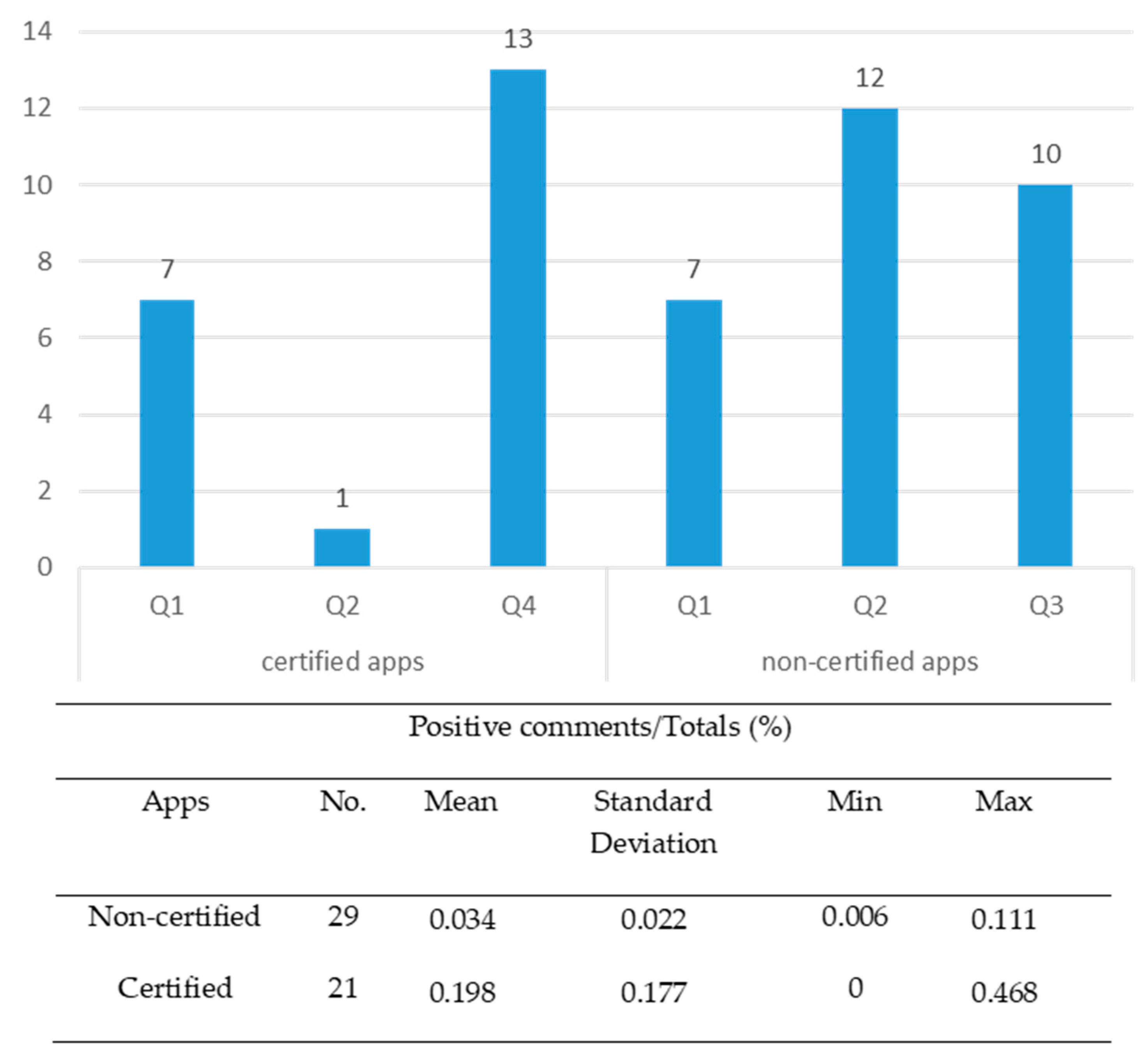
“It’s excellent. The design of the app makes it easy to use. The interface is very intuitive. I recommend it”.
5. Conclusions
5.1. Implications: Open Innovation and Certification in mHealth Application Industry
5.2. Limitations and Further Research
Author Contributions
Funding
Conflicts of Interest
Appendix A
References
- BinDhim, N.F.; Hawkey, A.; Trevena, L. A systematic review of quality assessment methods for smartphone health apps. Telemed. e-Health 2015, 21, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.N.K.; Brewer, A.C.; Karimkhani, C.; Buller, D.B.; Dellavalle, R.P. Mobile medical and health apps: State of the art, concerns, regulatory control and certification. Online J. Public Health Inform. 2014, 5, 229. [Google Scholar] [CrossRef]
- Huckvale, K.; Prieto, J.T.; Tilney, M.; Benghozi, P.-J.; Car, J. Unaddressed privacy risks in accredited health and wellness apps: A cross-sectional systematic assessment. BMC Med. 2015, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Llorens-Vernet, P.; Miró, J. Standards for Mobile Health–Related Apps: Systematic Review and Development of a Guide. JMIR mHealth uHealth 2020, 8, e13057. [Google Scholar] [CrossRef] [PubMed]
- Kanthawala, S.; Joo, E.; Kononova, A.; Peng, W.; Cotten, S. Folk theorizing the quality and credibility of health apps. Mob. Media Commun. 2018, 7, 175–194. [Google Scholar] [CrossRef]
- Krebs, P.; Duncan, D.T. Health app use among us mobile phone owners: A national survey. JMIR mHealth uHealth 2015, 3, e101. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile app rating scale: A new tool for assessing the quality of health mobile apps. JMIR mHealth uHealth 2015, 3, e27. [Google Scholar] [CrossRef]
- Payne, A.; Frow, P. Strategic Customer Management: Integrating Relationship Marketing and CRM; Cambridge University Press: Cambridge, UK, 2013. [Google Scholar]
- Oliver, R.L. Satisfaction: A Behavioral Perspective on the Consumer, 2nd ed.; M.E. Sharpe: New York, NY, USA, 2010. [Google Scholar]
- Larson, R.S. A path to better-quality mhealth Apps. JMIR mHealth uHealth 2018, 6, e10414. [Google Scholar] [CrossRef]
- Hughes, O. Safety Stamp for Health Apps to Bring More Trust to New Solutions. Digitalhealth. 2018. Available online: https://www.digitalhealth.net/2018/06/safety-stamp-health-apps/ (accessed on 17 January 2020).
- Boudreaux, E.D.; Waring, M.; Hayes, R.B.; Sadasivam, R.S.; Mullen, S.; Pagoto, S. Evaluating and selecting mobile health apps: Strategies for healthcare providers and healthcare organizations. Transl. Behav. Med. 2014, 4, 363–371. [Google Scholar] [CrossRef]
- Wicks, P.; Chiauzzi, E. ‘Trust but verify’—Five approaches to ensure safe medical apps. BMC Med. 2015, 13, 205. [Google Scholar] [CrossRef]
- McMillan, B.; Hickey, E.; Patel, M.; Mitchell, C.; Information, P.E.K.F.C. Quality assessment of a sample of mobile app-based health behavior change interventions using a tool based on the National Institute of Health and Care Excellence behavior change guidance. Patient Educ. Couns. 2016, 99, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.-K.; Liebovitz, D.M. Consumer mobile health Apps: Current state, barriers, and future directions. PM&R 2017, 9, S106–S115. [Google Scholar] [CrossRef]
- Powell, A.C.; Landman, A.B.; Bates, D.W. In search of a few good apps. JAMA 2014, 311, 1851–1852. [Google Scholar] [CrossRef] [PubMed]
- Zanni, G.R. Medical apps worth having. Consult. Pharm. 2013, 28, 322–324. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; Rigby, M.; Blair, M. The limited extent of accreditation mechanisms for websites and mobile applications in Europe. Stud. Health Technol. Inform. 2019, 262, 158–161. [Google Scholar] [PubMed]
- Castro, M.L.; Huerta, F.L.; May, A.L.H. Aplicaciones médicas en dispositivos móviles. Interconectando Saberes 2018, 6, 101–109. [Google Scholar] [CrossRef]
- Grau, I.; Kostov, B.; Gallego, J.; Iii, F.G.; Fernández-Luque, L.; Sisó-Almirall, A. Método de valoración de aplicaciones móviles de salud en español: El índice iSYScore. SEMERGEN Med. Fam. 2016, 42, 575–583. [Google Scholar] [CrossRef]
- Moreno, J.M.; Moreno, O.A.M.; Castelló, S.M.; Castelló, F.M.; Rodriguez, L.M.; Garví, O.M. Análisis de la calidad y seguridad de la información de aplicaciones móviles en prevención terciaria. Farm. Comunitarios 2015, 7, 23–26. [Google Scholar] [CrossRef]
- Pérez-Alcántara, P.; Herrera-Usagre, M. Improving health empowerment and evidence-based decision-making using collective intelligence and self-management health system: Em-Phasys project. In Proceedings of the 5th International Conference on Technological Ecosystems for Enhancing Multiculturality, Cádiz, Spain, 18–20 October 2017; pp. 1–4. [Google Scholar]
- Mira, J.J.; Carrillo, I.; Fernández, C.; Vicente, M.A.; Guilabert, M.; Elliott, P.; Lorenzo, S. Design and testing of the safety agenda mobile app for managing health care managers’ patient safety responsibilities. JMIR mHealth uHealth 2016, 4, e131. [Google Scholar] [CrossRef]
- Scott, K.M.; Richards, D.; Londos, G. Assessment criteria for parents to determine the trustworthiness of maternal and child health apps: A pilot study. Health Technol. 2018, 8, 63–70. [Google Scholar] [CrossRef]
- De La Vega, R.; Miró, J. mHealth: A strategic field without a solid scientific soul. A systematic review of pain-related Apps. PLoS ONE 2014, 9, e101312. [Google Scholar] [CrossRef] [PubMed]
- Car, J. Accreditation of Health and Wellness Apps. Harvard Global Health Institute. 2016. Available online: https://www.oecd.org/sti/ieconomy/4%20-%20Josip%20Car.pdf (accessed on 26 June 2020).
- Chau, M.; Xu, J. Business intelligence in blogs: Understanding consumer interactions and communities. MIS Q. 2012, 36, 1189. [Google Scholar] [CrossRef]
- Flanagin, A.J.; Metzger, M.J. Trusting expert- versus user-generated ratings online: The role of information volume, valence, and consumer characteristics. Comput. Hum. Behav. 2013, 29, 1626–1634. [Google Scholar] [CrossRef]
- Jin, J.; Ji, P.; Gu, R. Identifying comparative customer requirements from product online reviews for competitor analysis. Eng. Appl. Artif. Intell. 2016, 49, 61–73. [Google Scholar] [CrossRef]
- Sparks, B.A.; So, K.K.F.; Bradley, G.L. Responding to negative online reviews: The effects of hotel responses on customer inferences of trust and concern. Tour. Manag. 2016, 53, 74–85. [Google Scholar] [CrossRef]
- Genc-Nayebi, N.; Abran, A. A systematic literature review: Opinion mining studies from mobile app store user reviews. J. Syst. Softw. 2017, 125, 207–219. [Google Scholar] [CrossRef]
- Palomba, F.; Linares-Vásquez, M.; Bavota, G.; Oliveto, R.; Di Penta, M.; Poshyvanyk, D.; De Lucia, A. Crowdsourcing user reviews to support the evolution of mobile apps. J. Syst. Softw. 2018, 137, 143–162. [Google Scholar] [CrossRef]
- Picazo-Vela, S. The Effect of Online Reviews on Customer Satisfaction: An Expectation Disconfirmation Approach; Southern Illinois University: Carbondale, IL, USA, 2010. [Google Scholar]
- Ahmed, I.; Ahmad, N.S.; Ali, S.; Ali, S.; George, A.; Danish, H.S.; Uppal, E.; Soo, J.; Mobasheri, M.H.; King, D.; et al. Medication adherence apps: Review and content analysis. JMIR mHealth uHealth 2018, 6, e62. [Google Scholar] [CrossRef] [PubMed]
- Frie, K.; Hartmann-Boyce, J.; Jebb, S.; Albury, C.; Nourse, R.; Aveyard, P.; Bardus, M.; Brinker, T.; Lin, P.-H. Insights from google play store user reviews for the development of weight loss Apps: Mixed-method analysis. JMIR mHealth uHealth 2017, 5, e203. [Google Scholar] [CrossRef]
- Mendiola, M.F.; Kalnicki, M.; Lindenauer, S. Valuable features in mobile health apps for patients and consumers: Content analysis of apps and user ratings. JMIR mHealth uHealth 2015, 3, e40. [Google Scholar] [CrossRef]
- Switsers, L.; Dauwe, A.; Vanhoudt, A.; Van Dyck, H.; Lombaerts, K.; Oldenburg, J. Users’ perspectives on mhealth self-management of bipolar disorder: Qualitative focus group study. JMIR mHealth uHealth 2018, 6, e108. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, J.; Fogarty, A.S.; Boydell, K.; Christensen, H. The reviews are in: A qualitative content analysis of consumer perspectives on apps for bipolar disorder. J. Med. Internet Res. 2017, 19, e105. [Google Scholar] [CrossRef] [PubMed]
- Stawarz, K.; Preist, C.; Tallon, D.; Wiles, N.J.; Coyle, D. User experience of cognitive behavioral therapy apps for depression: An analysis of app functionality and user reviews. J. Med. Internet Res. 2018, 20, e10120. [Google Scholar] [CrossRef] [PubMed]
- Thornton, L.; Quinn, C.; Birrell, L.; Guillaumier, A.; Shaw, B.; Forbes, E.; Deady, M.; Kay-Lambkin, F. Free smoking cessation mobile apps available in Australia: A quality review and content analysis. Aust. N. Z. J. Public Health 2017, 41, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile health apps to facilitate self-care: A qualitative study of user experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [PubMed]
- Nicolai, M.; Pascarella, L.; Palomba, F.; Bacchelli, A. Healthcare android apps: A tale of the customers’ perspective. In Proceedings of the 3rd ACM SIGSOFT International Workshop on App Market Analytics, Tallinn, Estonia, 27 August 2019; pp. 33–39. [Google Scholar]
- Peng, W.; Kanthawala, S.; Yuan, S.; Hussain, S.A. A qualitative study of user perceptions of mobile health apps. BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef]
- Bullinger, A.C.; Rass, M.; Adamczyk, S.; Möslein, K.; Sohn, S. Open innovation in health care: Analysis of an open health platform. Health Policy 2012, 105, 165–175. [Google Scholar] [CrossRef]
- Khalid, M.; Shehzaib, U.; Asif, M. A case of mobile App reviews as a crowdsource. Int. J. Inf. Eng. Electron. Bus. 2015, 7, 39–47. [Google Scholar] [CrossRef]
- Yoo, Y.; Henfridsson, O.; Lyytinen, K. Research commentary—the new organizing logic of digital innovation: An agenda for information systems research. Inf. Syst. Res. 2010, 21, 724–735. [Google Scholar] [CrossRef]
- Chatterji, A.K. Spawned with a silver spoon? Entrepreneurial performance and innovation in the medical device industry. Strat. Manag. J. 2009, 30, 185–206. [Google Scholar] [CrossRef]
- Davey, S.M.; Brennan, M.; Meenan, B.J.; McAdam, R. Innovation in the medical device sector: An open business model approach for high-tech small firms. Technol. Anal. Strat. Manag. 2011, 23, 807–824. [Google Scholar] [CrossRef]
- Chesbrough, H.W.; Garman, A.R. How open innovation can help you cope in lean times. Harv. Bus. Rev. 2009, 87. Available online: https://hbr.org/2009/12/how-open-innovation-can-help-you-cope-in-lean-times (accessed on 6 June 2020). [CrossRef]
- Yun, J.J.; Liu, Z. Micro- and macro-dynamics of open innovation with a quadruple-helix model. Sustainability 2019, 11, 3301. [Google Scholar] [CrossRef]
- Peter, L.; Hajek, L.; Maresova, P.; Augustynek, M.; Penhaker, M. Medical devices: Regulation, risk classification, and open innovation. J. Open Innov. Technol. Mark. Complex. 2020, 6, 42. [Google Scholar] [CrossRef]
- Van Der Kleij, R.M.; Kasteleyn, M.J.; Meijer, E.; Bonten, T.N.; Houwink, E.J.; Teichert, M.; Van Luenen, S.; Vedanthan, R.; Evers, A.; Car, J.; et al. SERIES: eHealth in primary care. Part 1: Concepts, conditions and challenges. Eur. J. Gen. Pract. 2019, 25, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Lin, J.; Hoi, S.C.; Xiao, X.; Zhang, B. AR-miner: Mining informative reviews for developers from mobile app marketplace. In Proceedings of the 36th International Conference on Software Engineering, Hyderabad, India, 31 May–7 June 2014; pp. 767–778. [Google Scholar] [CrossRef]
- Duan, W.; Gu, B.; Whinston, A.B. The dynamics of online word-of-mouth and product sales—An empirical investigation of the movie industry. J. Retail. 2008, 84, 233–242. [Google Scholar] [CrossRef]
- Liu, Y. Word of mouth for movies: Its dynamics and impact on box office revenue. J. Mark. 2006, 70, 74–89. [Google Scholar] [CrossRef]
- Chen, M.; Liu, X. Predicting popularity of online distributed applications: ITunes app store case analysis. In Proceedings of the 2011 iConference, Seattle, WA, USA, 8–11 February 2011; Association for Computing Machinery (ACM): New York, NY, USA, 2011; pp. 661–663. [Google Scholar]
- Harman, M.; Jia, Y.; Zhang, Y. App store mining and analysis: MSR for app stores. In Proceedings of the 2012 9th IEEE Working Conference on Mining Software Repositories (MSR), Zurich, Switzerland, 2–3 June 2012; pp. 108–111. [Google Scholar]
- Chevalier, J.A.; Mayzlin, D. The effect of word of mouth on sales: Online book reviews. J. Mark. Res. 2006, 43, 345–354. [Google Scholar] [CrossRef]
- Zhou, W.; Duan, W. Online user reviews, product variety, and the long tail: An empirical investigation on online software downloads. Electron. Commer. Res. Appl. 2012, 11, 275–289. [Google Scholar] [CrossRef]
- Sharma, T.; Bashir, M. Privacy apps for smartphones: An assessment of users’ preferences and limitations. In International Conference on Human-Computer Interaction; Springer: Cham, Switzerland, 2020; pp. 533–546. [Google Scholar] [CrossRef]
- Mahalanobis, P.C. On tests and measures of groups divergence. J. Asiat. Sociol. Bengal 1930, 26, 541–588. [Google Scholar]
- Andalusian Agency for Healthcare Quality. Complete List of Recommendations on Design, Use and Assessment of Health Apps. 2012. Available online: http://www.calidadappsalud.com/en/listado-completo-recomendaciones-app-salud/ (accessed on 12 January 2020).
- Jackman, S. Data from Web into R. Political Methodol. 2006, 14, 11–16. [Google Scholar]
- Zhao, Y.; Xu, X.; Wang, M. Predicting overall customer satisfaction: Big data evidence from hotel online textual reviews. Int. J. Hosp. Manag. 2019, 76, 111–121. [Google Scholar] [CrossRef]
- Van Der Meer, T.G. Automated content analysis and crisis communication research. Public Relat. Rev. 2016, 42, 952–961. [Google Scholar] [CrossRef]
- Grimmer, J.; Stewart, B.M. Text as data: The promise and pitfalls of automatic content analysis methods for political texts. Political Anal. 2013, 21, 267–297. [Google Scholar] [CrossRef]
- Erlingsson, C.; Brysiewicz, P. A hands-on guide to doing content analysis. Afr. J. Emerg. Med. 2017, 7, 93–99. [Google Scholar] [CrossRef]
- Yurt-Öncel, S.; Erdugan, F. Kontenjans Tablolarının Analizinde Log-Lineer Modellerin Kullanımı Ve Sigara Bağımlılığı Üzerine Bir Uygulama. SAÜ Fen Bil. Der. 2015, 19, 221–235. [Google Scholar] [CrossRef]
- Ye, B.H.; Luo, J.M.; Vu, H.Q. Spatial and temporal analysis of accommodation preference based on online reviews. J. Destin. Mark. Manag. 2018, 9, 288–299. [Google Scholar] [CrossRef]
- Haberman, S.J. The analysis of residuals in cross-classified tables. Biometrics 1973, 29, 205. [Google Scholar] [CrossRef]
- Yun, J.J.; Zhao, X.; Jung, K.; Yigitcanlar, T. The culture for open innovation dynamics. Sustainability 2020, 12, 5076. [Google Scholar] [CrossRef]
- Malik, A.; Suresh, S.; Sharma, S. Factors influencing consumers’ attitude towards adoption and continuous use of mobile applications: A conceptual model. Procedia Comput. Sci. 2017, 122, 106–113. [Google Scholar] [CrossRef]
- Freier, A. 55% of Consumers Download an App from a Paid Advert. Businessofapps. 2019. Available online: https://www.businessofapps.com/news/55-of-consumers-download-an-app-from-a-paid-advert/ (accessed on 5 October 2020).
- Strzelecki, A. Application of developers’ and users’ dependent factors in app store optimization. Int. J. Interact. Mob. Technol. (iJIM) 2020, 14, 91–106. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Initiative | Origin | Year | Features/Requirements |
|---|---|---|---|
| FDA (US Food and Drug Administration) | United State (US) | 2013 | Oversight of device software functions. Three-tier classification system: - Class I: lowest risk. Exempt from FDA review - Class II: intermediate level of risk. Developers are required to submit a premarket notification. - Class III: highest risk level. More complex, time-consuming, and expensive premarket approval process |
| https://apps.healthskouts.com/ | |||
| NHS Health Apps Library | United Kingdom (UK) | 2013 | Technical assessment tries to check the following items: available evidence on outcomes, clinical safety, data protection, security, usability and accessibility, interoperability and technical stability. |
| https://www.nhs.uk/apps-library/ | |||
| European Directory of Health Apps | European Union (EU) | 2012 | Health apps it lists have all been recommended by patient groups and empowered consumers, then categorised and indexed in several ways (including by local language), to make the details easy for readers to find. |
| https://g3ict.org/publication/european-directory-of-health-apps-2012-2013 | |||
| Clinical Laboratory Improvement Amendment (CLIA) | US | 1988 | Certifies and ensures the quality of testing in US laboratories. Over time a similar approach is applied to m-Health apps. They must comply with basic standards in three areas: accessibility, privacy and content. |
| https://www.cms.gov/Regulations-and-Guidance/Legislation/CLIA | |||
| Happtique | US | 2010 | Requirements assess: operability, privacy, security and content. |
| Suspended since December 2013 | |||
| mHONcode | Switzerland | 1996 | Reflect the accountability, trustworthiness, and transparency of health application. The Honcode app certification has 8 principles: authority, complementarity, confidentiality, validity, justifiability and objectivity, user‘s practice, financial disclosure and advertisement policy. |
| https://www.hon.ch/imgs/2020/ENGuidelinesApp_compressed.pdf | |||
| AppSaludable | Spain | 2012 | This seal is based on the 31 recommendations published in the Guide of Recommendations on Design, Use and Assessment of Health Apps (see Appendix A). |
| http://www.calidadappsalud.com/distintivo/catalogue | |||
| Appsalut | Spain | 2015 | It is based on criteria published in the criteria guide of the accreditation process. The criteria are structured in 4 groups: usability and design, functionality, technology, and security. At the end of the accreditation process, the mHealth.cat office grants those applications that have successfully passed the mandatory minimum criteria to publish on the AppSalut portal, a numerical note resulting from the evaluation of the criteria. |
| https://appsalut.gencat.cat/ | |||
| Characteristics | Certified | Top (Non-Certified) | ||
|---|---|---|---|---|
| No. | % | No. | % | |
| Users | ||||
| Patients | 7 | 33.33 | 15 | 51.72 |
| Professionals | 8 | 38.10 | 1 | 3.45 |
| General public | 6 | 28.57 | 13 | 44.83 |
| Category | ||||
| Monofunction | 13 | 61.90 | 14 | 48.27 |
| Multifunction | 8 | 38.10 | 15 | 51.73 |
| Developer | ||||
| Health sector company | 4 | 19.05 | 11 | 37.93 |
| Technological company | 8 | 38.10 | 16 | 55.17 |
| Sanitary professional | 6 | 28.57 | 1 | 3.45 |
| Particular | 1 | 4.76 | 0 | 0.00 |
| Public administration | 2 | 9.52 | 1 | 3.45 |
| Communication (bidirectional) | ||||
| Yes | 4 | 19.05 | 5 | 17.24 |
| No | 17 | 80.95 | 24 | 82.76 |
| Variables | Chi-Squared | p |
|---|---|---|
| User | 11.738 | 0.047 * |
| Developer | 19.516 | 0.04 * |
| Stars | 122.832 | 0.045 * |
| Categories (mono-multi function) | 2.579 | 0.453 |
| Health and general well-being | 9.179 | 0.027 * |
| Medical information | 3.792 | 0.285 |
| Healthcare administration | 12.940 | 0.044 * |
| Remote and sensor-based monitoring | 8.289 | 0.040 * |
| Other | 11.167 | 0.011 * |
| Health Apps | Online User Reviews 1 | Total | ||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |||
| Non-certified | Observed count | 7 | 12 | 10 | 0 | 29 |
| Expected count | 8.1 | 7.5 | 5.8 | 7.5 | 29.0 | |
| Standardized residual | −0.4 | 1.6 | 1.7 | −2.7 | ||
| Adjusted residual | −0.7 | 2.9 | 3.0 | −4.9 | ||
| Certified | Observed count | 7 | 1 | 0 | 13 | 21 |
| Expected count | 5.9 | 5.5 | 4.2 | 5.5 | 21.0 | |
| Standardized residual | 0.5 | −1.9 | −2.0 | 3.2 | ||
| Adjusted residual | 0.7 | −2.9 | −3.0 | 4.9 | 0.7 | |
| Total | Observed count | 14 | 13 | 10 | 13 | 50 |
| Expected count | 14.0 | 13.0 | 10.0 | 13.0 | 50.0 | |
| Health Apps | Downloads 1 | Total | ||||
|---|---|---|---|---|---|---|
| D1 | D2 | D3 | D4 | |||
| Non-certified | Observed count | 5 | 5 | 8 | 11 | 29 |
| Expected count | 6.2 | 2.8 | 3.8 | 4.5 | 29.0 | |
| Standardized residual | −0.5 | 1.3 | 2.2 | 3.1 | ||
| Adjusted residual | −0.7 | 1.7 | 2.9 | 4.1 | ||
| Certified | Observed count | 13 | 3 | 3 | 2 | 21 |
| Expected count | 4.5 | 2.0 | 2.8 | 3.3 | 21.0 | |
| Standardized residual | 4.0 | 0.7 | 0.2 | −0.7 | ||
| Adjusted residual | 5.2 | 0.9 | 0.2 | −0.9 | ||
| Total | Observed count | 18 | 8 | 11 | 13 | 50 |
| Expected count | 18.0 | 8.0 | 11.0 | 13.0 | 50.0 | |
| Test Statistics | df | Sig. | |
|---|---|---|---|
| Likelihood ratio | 0.980 | 4 | 0.913 |
| Pearson chi-square | 0.749 | 4 | 0.945 |
| Parameter | Estimate | Std. Error | Z | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Constant | 4.002 × 10−17 | 1.000 | 0.000 | 1.000 | −1.960 | 1.960 |
| [certification = 0] × [Qi = 1] | 0.405 | 1.185 | 0.342 | 0.732 | −1.918 | 2.728 |
| [certification = 0] × [Qi = 2] | 1.019 | 1.157 | 0.880 | 0.379 | −1.250 | 3.287 |
| [certification = 0] × [Qi = 3] | 1.792 | 1.080 | 2.174 | 0.042 | −0.325 | 3.909 |
| [certification = 0] × [Qi = 4] | −20.378 | 4475.634 | −0.005 | 0.996 | −8792.460 | 8751.705 |
| [certification = 1] × [Qi = 1] | 0.405 | 1.185 | 0.342 | 0.732 | −1.918 | 2.728 |
| [certification = 1] × [Qi = 2] | −1.466 | 1.502 | −0.976 | 0.329 | −4.410 | 1.478 |
| [certification = 1] × [Qi = 3] | −18.665 | 5308.578 | −0.004 | 0.997 | −10,423.281 | 10,385.957 |
| [certification = 1] × [Qi = 4] | 0 | |||||
| [Qi = 1] × [Di = 0] | 1.299 | 0.651 | 1.995 | 0.046 | 0.023 | 2.576 |
| [Qi = 1] × [Di = 1] | 0 | |||||
| [Qi = 2] × [Di = 0] | 1.204 | 0.658 | 1.829 | 0.067 | −0.086 | 2.494 |
| [Qi = 2] × [Di = 1] | 0 | |||||
| [Qi = 3] × [Di = 0] | −0.405 | 0.645 | −0.628 | 0.530 | −1.671 | 0.860 |
| [Qi = 3] × [Di = 1] | 0 | |||||
| [Qi = 4] × [Di = 0] | 2.485 | 1.041 | 2.387 | 0.017 | 0.445 | 4.525 |
| [Qi = 4] × [Di = 1] | 0 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gessa, A.; Jiménez, A.; Sancha, P. Open Innovation in Digital Healthcare: Users’ Discrimination between Certified and Non-Certified mHealth Applications. J. Open Innov. Technol. Mark. Complex. 2020, 6, 130. https://doi.org/10.3390/joitmc6040130
Gessa A, Jiménez A, Sancha P. Open Innovation in Digital Healthcare: Users’ Discrimination between Certified and Non-Certified mHealth Applications. Journal of Open Innovation: Technology, Market, and Complexity. 2020; 6(4):130. https://doi.org/10.3390/joitmc6040130
Chicago/Turabian StyleGessa, Ana, Amor Jiménez, and Pilar Sancha. 2020. "Open Innovation in Digital Healthcare: Users’ Discrimination between Certified and Non-Certified mHealth Applications" Journal of Open Innovation: Technology, Market, and Complexity 6, no. 4: 130. https://doi.org/10.3390/joitmc6040130
APA StyleGessa, A., Jiménez, A., & Sancha, P. (2020). Open Innovation in Digital Healthcare: Users’ Discrimination between Certified and Non-Certified mHealth Applications. Journal of Open Innovation: Technology, Market, and Complexity, 6(4), 130. https://doi.org/10.3390/joitmc6040130