Preoperatory Anxiety in Patients Undergoing Cardiac Surgery



Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Study Participants
2.3. Data Collection
STAI
2.4. Ethical and Administrative Considerations
2.5. Statistical Data Analysis
3. Results
3.1. Features of Participants
3.2. Anxiety Levels Analysis
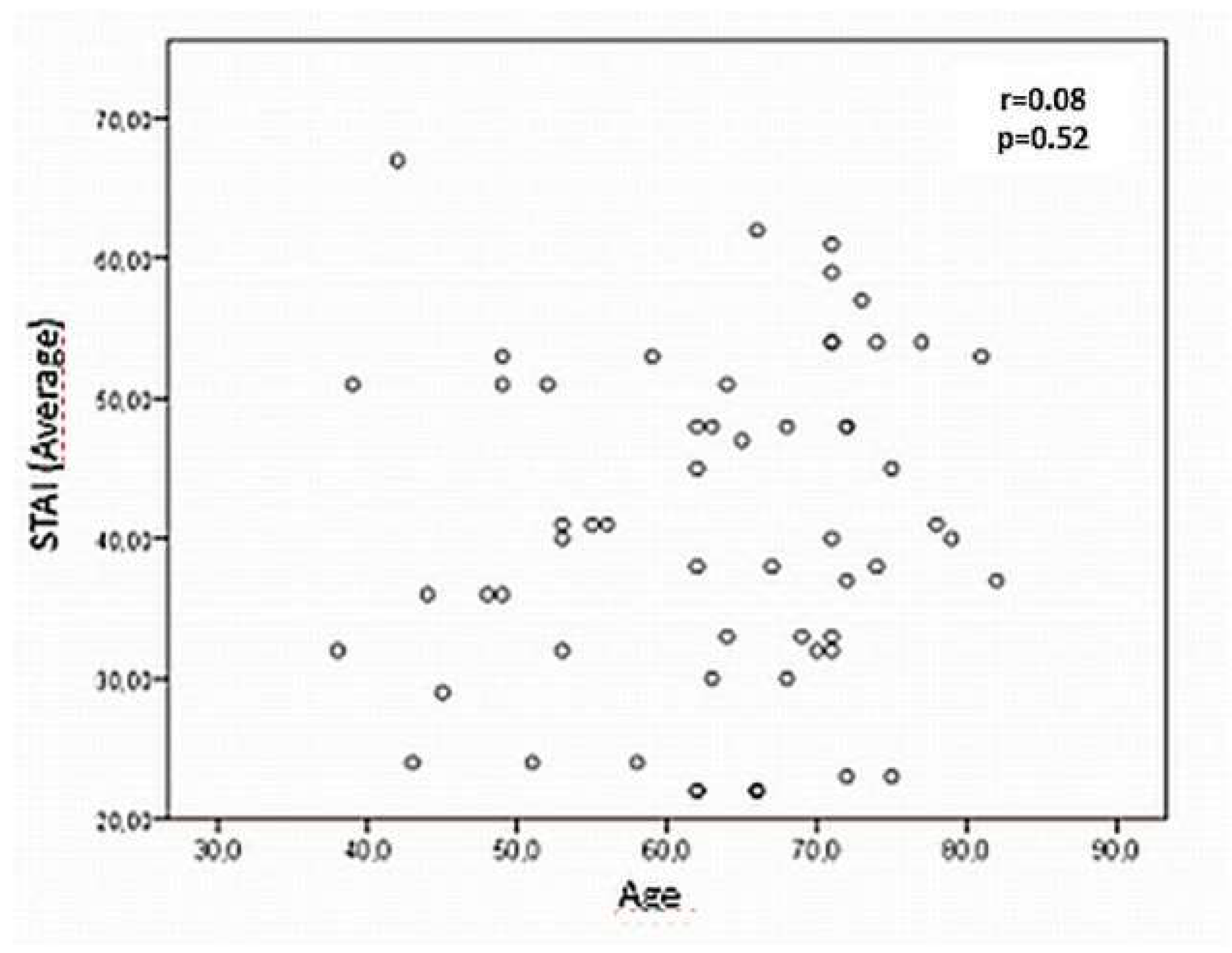
3.3. Relationships between Anxiety Levels and Features of the Studied Population
3.4. Bivariate Linear Model, Explanatory of the Factors which Influence the Preoperative Anxiety in the Studied Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barrilero Gómez, J.A.; Casero Mayorga, J.A.; Cebrián Picazo, F.; Córdoba Monedero, C.A.; García Alcaraz, F.; Gregorio González, E.; Hernández Martínez, A.; Pérez Morote, J.; Tébar Parreño, F.J. Ansiedad y cirugía: Repercusiones en el paciente sometido a cirugía programada. Rev. de enfermería 1998, 3–20. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Pr: Palo Alto, CA, USA, 1983. [Google Scholar]
- Teixeira Lima, F.E.; Leite de Araújo, T.; Gomes Serafim, E.C.; Lopes Custódio, I. Protocolo de consultas de enfermería al paciente después de la revascularización del miocardio: Influencia en la ansiedad y depresión. Rev. Latino-Am. Enfermagem 2010. [Google Scholar] [CrossRef]
- Fathi, M.; Alavi, S.M.; Joudi, M.; Joudi, M.; Mahdikhani, H.; Ferasatkish, R.; Bakhshandeh, H.; Jabbari Nooghabi, M. Preoperative anxiety in candidates for heart surgery. Iranian J. Psychiatry Behavior. Sci. 2014, 8, 90–96. [Google Scholar]
- Hernández-Palazón, J.; Fuentes-García, D.; Falcón-Araña, L.; Roca-Calvo, M.J.; Burguillos-López, S.; Doménech-Asensi, P.; Jara-Rubio, R. Assessment of Preoperative Anxiety in Cardiac Surgery Patients Lacking a History of Anxiety: Contributing Factors and Postoperative Morbidity. J. Cardiothoracic Vascular Anesthesia 2018, 32, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Oscco-Torres, O.; Bendezú-Sarcines, C.E.; Escajadillo-Lagos, N. Actitud que adopta la enfermera durante la atencion y nivel de ansiedad del paciente en el pre operatorio en un hospital público de pisco, perú. Rev. Méd. Panacea 2011, 1, 85–88. [Google Scholar]
- Carapia-Sadurni, A.; Mejía-Terrazas, G.E.; Nacif-Gobera, L.; Hernández-Ordóñez, N. Efecto de la intervención psicológica sobre la ansiedad preoperatoria. Rev. Mex. de Anestesiol. 2011, 34, 260–263. [Google Scholar]
- Moix Queraltó, J. EMOCIÓN Y CIRUGÍA. Anales de Psicología 1994, 10, 167. [Google Scholar]
- Díez-Álvarez, E.; Arrospide, A.; Mar, J.; Alvarez, U.; Belaustegi, A.; Lizaur, B.; Larrañaga, A.; Arana, J.M. Efectividad de una intervención preoperatoria de enfermería sobre el control de la ansiedad de los pacientes quirúrgicos. Enfermería Clín. 2012, 22, 18–26. [Google Scholar] [CrossRef]
- Castillero Amador, Y. Intervención psicológica en cirugía cardíaca. Avances en Psicología Latinoamericana 2010, 25, 52–63. [Google Scholar]
- Guo, P. Preoperative education interventions to reduce anxiety and improve recovery among cardiac surgery patients: A review of randomised controlled trials. J. Clin. Nursing 2015, 24, 34–46. [Google Scholar] [CrossRef]
- León Castro, A.; Salazar Vargas, C. Valoración psicológica perioperatoria en pacientes sometidos a cirugía cardiovascular. Rev. Costarricense de Cardiol. 2007, 9, 11–15. [Google Scholar]
- Negromonte-Gonçalves, K.K.; da Silva, J.I.; Tavares-Gomes, E.; Lopes de Souza-Pinheiro, L.; Remigio-Figueiredo, T.; Muniz da Silva-Bezerra, S.M. Anxiety in the preoperative period of heart surgery. Rev. Brasileira de Enfermagem 2016, 69, 397. [Google Scholar] [CrossRef]
- Choinière, M.; Watt-Watson, J.; Victor, J.C.; Baskett, R.J.F.; Bussières, J.S.; Carrier, M.; Cogan, J.; Cosello, J.; Feindel, C.; Guerton, M.C.; et al. Prevalence of and risk factors for persistent postoperative nonanginal pain after cardiac surgery: a 2-year prospective multicentre study. CMAJ Canadian Med. Assoc. J. 2014, 186, E223. [Google Scholar] [CrossRef] [PubMed]
- Tavares-Gomes, E.; Muniz da Silva-Bezerra, S.M. Anxiety and depression in the preoperative period of cardiac surgery. Rev. da Rede de Enfermagem do Nordeste 2017, 18, 420. [Google Scholar] [CrossRef]
- Matthias, A.T.; Samarasekera, D.N. Preoperative anxiety in surgical patients-experience of a single unit. Acta Anaesthesiol. Taiwanica 2012, 50, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Julian, L.J. Measures of Anxiety. Arthritis Care Res. 2011, 63. [Google Scholar] [CrossRef] [PubMed]
- Spielberg, C.D.; Gorsuch, R.L.; Lushene, R.E.; Buela-Casal, G.; Guillen-Riquelme, A.; Seisdedos Cubero, N. Cuestionario de Ansiedad Estado Rasgo. Adaptación Española; TEA Ediciones: Madrid, Spain, 2015. [Google Scholar]
- Martin, M. Instrumentos para el estudio de la ansiedad y depresión. In Instrumentos de Evaluación Psicológica; González Llaneza, F.M., Ed.; Editorial Ciencias Médicas: Ciudad de la Habana, Cuba, 2007. [Google Scholar]
- Valenzuela-Millán, J.; Barrera-Serrano, J.R.; Ornelas-Aguirre, J.M. Ansiedad preoperatoria en procedimientos anestésicos. Cirugía y Cirujanos 2010, 78, 151–156. [Google Scholar]
- Ruiz-López, E.; Muñoz-Cuevas, J.H.; Olivero-Vásquez, Y.I.; Islas-Saucillo, M. Ansiedad preoperatoria en el Hospital General de México. Rev. Méd. del Hospital General de México 2010, 63, 231–236. [Google Scholar]
- Kiyohara, L.Y.; Kayano, L.K.; Oliveira, L.M.; Yamamoto, M.U.; Inagaki, M.M.; Ogawa, N.Y.; Gonzales, P.E.S.M.; Mandelbaum, R.; Okubo, S.T.; Watanuki, T.; et al. Surgery information reduces anxiety in the pre-operative period. Rev. do Hospital das Clin. 2004, 59, 51–56. [Google Scholar] [CrossRef]
- Doñate Marín, M.; Litago Cortés, A.; Monge Sanz, Y.; Martínez Serrano, R. Aspectos de la información preoperatoria relacionada con la ansiedad del paciente programado para cirugía. Enfermería Global 2015, 14, 170–180. [Google Scholar] [CrossRef][Green Version]
- Galego Vázquez, H.; Pena Valiño, H. Ansiedade do paciente na área de espera cirurxica valoración e intervención de enfermería. Rev. do Colexio Oficial de Enfermería de Lugo 2006, 35–48. [Google Scholar]
- Gordillo León, F.; Arana Martínez, J.M.; Mestas Hernández, L. Tratamiento de la ansiedad en pacientes prequirúrgicos. Rev. Clín. de Med. de Familia 2011, 4, 228–233. [Google Scholar] [CrossRef]
- Quintero, A.; Yasnó, D.A.; Riveros, O.L.; Castillo, J.; Borráez, B.A. Ansiedad en el paciente prequirúrgico: Un problema que nos afecta a todos. Rev. Colombiana de Cirugía 2017, 32, 115–120. [Google Scholar] [CrossRef]
- Rodrigues, H.F.; Furuya, R.K.; Spadoti-Dantas, R.A.; Marosti-Dessotte, C.A. Ansiedade e depressão em cirurgia cardíaca: Diferenças entre sexo e faixa etária. Escola Anna Nery 2016, 20. [Google Scholar] [CrossRef]
- Orihuela-Pérez, I.; Pérez-Espinosa, J.A.; Aranda-Salcedo, T.; Zafra-Norte, J.; Jiménez-Ruiz, R.M.; Martínez-García, Á.; González-Ramírez, A.R.; Escobar-Julián, F.M. Visita preoperatoria de enfermería: Evaluación de la efectividad de la intervención enfermera y percepción del paciente. Enfermería Clín. 2010, 20, 349–354. [Google Scholar] [CrossRef]
- Sjöling, M.; Nordahl, G.; Olofsson, N.; Asplund, K. The impact of preoperative information on state anxiety, postoperative pain and satisfaction with pain management. Patient Edu. Counsel. 2003, 51, 169–176. [Google Scholar] [CrossRef]
- Carrascosa López, M.T.; Aguilar Martínez, R.; Carrascosa López, M.C. Disminución de ansiedad en paciente quirúrgico mediante una intervención de enseñanza individual. Enfuro 2011, 13–17. [Google Scholar]
- Ortiz, J.; Wang, S.; Elayda, M.A.; Tolpin, D.A. Información preoperatoria al paciente: ¿podemos mejorar la satisfacción y reducir la ansiedad? Braz. J. Anesthesiol. 2015, 65, 7–13. [Google Scholar] [CrossRef]
- Miguel Romeo, M.C.; Sagardoy Muniesa, L. Efectos del uso de un tríptico informativo en la reducción de la ansiedad y el dolor perioperatorios en pacientes intervenidos de patología urológica. Enfermería Clín. 2013, 24, 233–240. [Google Scholar] [CrossRef]


{kind=link}
| N | (%) | |
|---|---|---|
| Gender | ||
| Female | 35 | 58.3% |
| Male | 25 | 41.7% |
| Marital status | ||
| Single | 4 | 6.7% |
| In union | 4 | 6.7% |
| Married | 35 | 58.3% |
| Separated | 3 | 5.0% |
| Divorced | 2 | 3.3% |
| Widow/er | 12 | 20.0% |
| Level of education | ||
| No studies | 7 | 11.7% |
| Primary studies | 30 | 50.0% |
| Secondary studies | 15 | 25.0% |
| University studies | 8 | 13.3% |
| STAI-S Score (Mean ± SD) | p-Value | |
|---|---|---|
| Gender | p = 0.13 | |
| Men | 38.92 ± 13.94 | |
| Women | 43.29 ± 9.59 | |
| Level of education | * p < 0.05 | |
| No studies | 52.57 ± 8.66 | |
| Primary studies | 40.9 0± 11.46 | |
| Secondary studies | 36.26 ± 10.68 | |
| University studies | 36.13 ± 10.68 | |
| Surgery type | p = 0.86 | |
| CABG | 42.60 ± 13.86 | |
| Valvular | 40.8 1± 10.94 | |
| Both | 40.53 ± 9.45 | |
| Previous surgery | ** p < 0.01 | |
| Yes (n = 43) | 48.50 ± 9.06 | |
| No (n = 17) | 37.44 ± 11.56 | |
| Previous surgery’s assessment | * p < 0.05 | |
| Very good (n = 13) | 32.07 ± 7.94 | |
| Good (n = 18) | 33.83 ± 11.20 | |
| Bad (n = 11) | 47.73 ± 6.98 | |
| Very bad (n = 1) | 59.00 |
| β | p-Value | OR | OR CI (95%) | |
|---|---|---|---|---|
| Age | −0.14 | <0.05 | 0.87 | 0.76–0.99 |
| Previous surgery’s assessment | −2.29 | <0.05 | 0.10 | 0.02–0.57 |
| Level of education | −3.11 | <0.01 | 0.04 | 0.01–0.38 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prado-Olivares, J.; Chover-Sierra, E. Preoperatory Anxiety in Patients Undergoing Cardiac Surgery. Diseases 2019, 7, 46. https://doi.org/10.3390/diseases7020046
Prado-Olivares J, Chover-Sierra E. Preoperatory Anxiety in Patients Undergoing Cardiac Surgery. Diseases. 2019; 7(2):46. https://doi.org/10.3390/diseases7020046
Chicago/Turabian StylePrado-Olivares, José, and Elena Chover-Sierra. 2019. "Preoperatory Anxiety in Patients Undergoing Cardiac Surgery" Diseases 7, no. 2: 46. https://doi.org/10.3390/diseases7020046
APA StylePrado-Olivares, J., & Chover-Sierra, E. (2019). Preoperatory Anxiety in Patients Undergoing Cardiac Surgery. Diseases, 7(2), 46. https://doi.org/10.3390/diseases7020046