1. Introduction
According to Jones [
1], oxidative stress (OS) has been defined as an imbalance between reactive oxygen species, or ROS (including free radical and non-free radical species), and antioxidants in favor of the former, leading to a disruption of the redox signaling and/or molecular damage to lipids, proteins, and DNA. Such a concept takes into account that ROS comprise both physiological and pathological properties [
2,
3]. At the physiological level, ROS act as secondary messengers (redox signaling) able to induce over-expression of gene coding for antioxidant enzymes. When produced in excessive amount, ROS, as powerful oxidants, provoke irreversible damage to lipids, DNA, and proteins, which are potentially involved in the development of ageing and ageing-associated diseases (cardio-vascular and neuro-degenerative pathologies, cancer, diabetes, etc.). Increased OS may result from a poor diet in fruits and vegetables known for their richness in antioxidants but also from endogenous and exogenous sources (e.g., smoking habits, exposure to radiations, sun and nanoparticles, excessive alcohol intake, physical exercise, intake of drugs (e.g., contraceptive pills), mitochondrial and endothelial dysfunctions, iron overload, chronic inflammation, etc.) [
3].
Obtaining evidence in vivo pathological OS still remains a great challenge [
4,
5]. Five classical axes of investigation using biological samples (whole blood, plasma, serum, urine, saliva, expired air) have been developed: measurement of both enzymatic (e.g., superoxide dismutase, glutathione peroxidases, etc.) and low molecular weight (vitamins C and E, glutathione, ubiquinone, thiol proteins, carotenoids, polyphenols, etc.) antioxidants, determination of trace elements (selenium, copper, and zinc), indirect ROS production evidenced by evaluating oxidative damage to lipids (lipid peroxides, isoprostanes, 4-hydroxynonenal), DNA (8-OH deoxyguanosine), and proteins (carbonyl group), or by identifying endogenous sources of ROS production (hyperglycemia, inflammation, iron overload, etc.) and, finally, use of a dietary questionnaire for estimating antioxidant intake [
6]. In addition to being invasive (except the last one), all these approaches are time-consuming and require complex protocols, specific equipment (HPLC, ELISA, chemiluminescence, fluorescence and spectrophotometry, mass spectrometry, etc.). and qualified staff, thus making the majority of the analysis very expensive. Due to the great complexity of OS, none of them can claim to be a specific index of this biological process, except perhaps isoprostanes being considered as a “gold standard” of the lipid peroxidation process [
7]. In order to bypass this problem, some authors have proposed the determination of the total antioxidant capacity (TAC) of biological samples such as whole blood and plasma. The most popular test is the ORAC (oxygen radical antioxidant capacity) assay which evaluates how antioxidants present in biological samples can inhibit, or not, physiological free radical species produced in a test tube. A very strong limitation of such an approach is that the plasma antioxidant capacity is dependent on uric acid and total protein concentrations of more than 70% [
8,
9].
A promising, but always under-explored way, to show OS is to use the skin as a matrix [
10]. Having the largest surface area of the body, skin is the major organ target for oxidative stress, as it is continually exposed to external and internal “aggressions. As early as 1999, Kohen et al. [
11] were the first to develop a noninvasive in vivo method for measuring at the skin level both low molecular weight antioxidants (LMWA) and lipid hydroperoxides levels as an indicator of oxidation status. For that, they used an electrochemical methodology (potentiometer) able to evaluate potential changes of reference and working electrodes immersed in an electro-conductive solution (FeCl
3) applied to the skin. Later, Brainina’s group [
12] determined both antioxidant (AOA) and oxidant (OA) skin activities using a K
3[Fe(CN)
6/]/K
4[Fe(CN)
6] mixture as a reduced/oxidized mediator (M) system, platinum as the working electrode, and electro-cardio cardiogram (ECG) electrodes as the reference. Ermakov et al. [
13] developed resonance Raman spectroscopy (RRS) and reflection spectroscopy (RS) as optical methods applicable to the noninvasive detection of carotenoids in human skin. The authors showed that the skin carotenoid status can be a strong predictor of plasma carotenoid status and dietary intake of vegetables and fruits enriched in carotenoids [
14,
15]. Using electron spin resonance (ESR), a technology specifically dedicated to directly detect oxygenated free radicals, D’Errico et al. and Bourji et al. showed ROS production, respectively, on frog skin biopsies and fibrotic and non-fibrotic skin biopsies from patients with diffuse cutaneous systemic sclerosis [
16,
17]. Even if being specific for detection of free radical species, ESR technology has the great disadvantages to need biopsies, to be time consuming, being expensive, and requiring highly qualified staff.
Due to its easy method of application, we decided to develop an improved electrochemical method for evaluating SOSS by increasing sensibilities of both mediator M and microelectrodes. In addition to the examination of both method robustness and validation, we also investigated, for the first time, the possible existence of relationships between SOSS and blood concentration of classical OS biomarkers.
2. Materials and Methods
2.1. Reagents and Chemicals
Butylhydroxyanisol, 3,5-Di-tert-butylhydroxytoluene, sinapic, benzoic, salicylic, ferulic, and uric acids, catechol, cysteine, β-caroten, α-tocopherol, resveratrol, curcumin, glutathione, and bilirubin as antioxidants were all purchased from Sigma, Lezennes, France. Hydrogen peroxide, tert-butyl hydroperoxide, 2,2-diphenyl-1-picrylhydrazyl, 2,2′-zinobis(3-ethylbenzothiazoline-6-sulfonic acid, 2,2′-azobis(2-amidinopropane) dihydrochloride, potassium permanganate, and sodium hypochlorite as sources of oxidants production were also supplied by Sigma, Lezennes, France. Electrocardiogram (ECG) conductive gel was provided by Dermedics, Veauche, France.
The topical cream containing reduced coenzyme
10 or CoQ
10 (Sigma-Aldrich, Munich, Germany) as a bioactive antioxidant compound was prepared according to Kaci et al. [
18]. Encapsulation of the antioxidant was performed thanks to nano–emulsions consisting of rapeseed oil (vegetable oil, Lesieur, Asnières-sur-Seine, France), rapeseed lecithin (Lecresoyaf F60 IP, Verdun, France) deionized water, and two polysaccharide polymers used as thickeners, xanthan gum (XG) from
Xanthomonas campestris (Sigma-Aldrich, Munich, Germany), and carboxymethylcellulose sodium salt (CMC) (Alfa Aesar, Karlsruhe, Germany).
Food supplements fortified with vitamin C as synthetic (synthetic vitamin C supplement) or natural (Arkovital® Pure’Energie containing natural vitamin C) composed of acerola berry (Malpighia punicifolia L. or Malpighia glabra L.), amla fruit (Phyllanthus emblica L.), goyave (Psidium guajava L.), holy basil leaf (Ocimum tenuiflorum L.), curry tree leaf (Murraya koenigii L.), and lemon (Citrus limon L) forms were supplied by Arkopharma, Carros, France. Each capsule of both forms contains 72 mg of vitamin C.
In Group III, vitamins C and E, reduced and oxidized glutathione, thiol proteins, selenium, copper, zinc, copper zinc/ratio, superoxide dismutase (SOD) and glutathione peroxidase (GPx), and lipid peroxides were assessed in plasma or whole blood according to analytical protocols as described earlier in detail by us [
19,
20,
21]. Plasma isoprostanes were measured by Liquid chromatography-mass spectrometry (LC-MS) according to a homemade method [
22]. Oxidative damage to DNA was evaluated by the measurement of urinary 8-hydroxydesoxyguanosine (8OH-dG) thanks to the kit developed by the Japan Institute for Control of Aging (Shizuoka, Japan). Total urinary polyphenols were measured according to Hoge et al. [
6]. Both 8OH-dG and polyphenols were standardized to urinary creatinine. The participants also completed a self-administered food frequency questionnaire (FFQ) in order to estimate their dietary polyphenols intake [
6].
2.2. Patients’s Consent
For each study presented in this paper, the trial objectives, study design, risks, and benefits were explained and written informed consent was obtained from all participants. As blood samples were needed for analysis of OS biomarkers, the full study protocol was approved by the institutional ethics committee of the Liège University Hospitals (reference 2017/342) and conducted in accordance with the 1964 Declaration of Helsinki and the European guidelines for good clinical practice.
2.3. Principle of SOSS Evaluation
SOSS (expressed as PAOT (Pouvoir AntiOxydant Total)-Skin Score
®) reflecting the redox equilibrium between skin antioxidants and oxidants was measured using the equipment described in
Figure 1 (Oxystress Analyzer). On subjects placed in a controlled temperature (20 °C) and humidity room (70%) during all experimentation, 12 cm
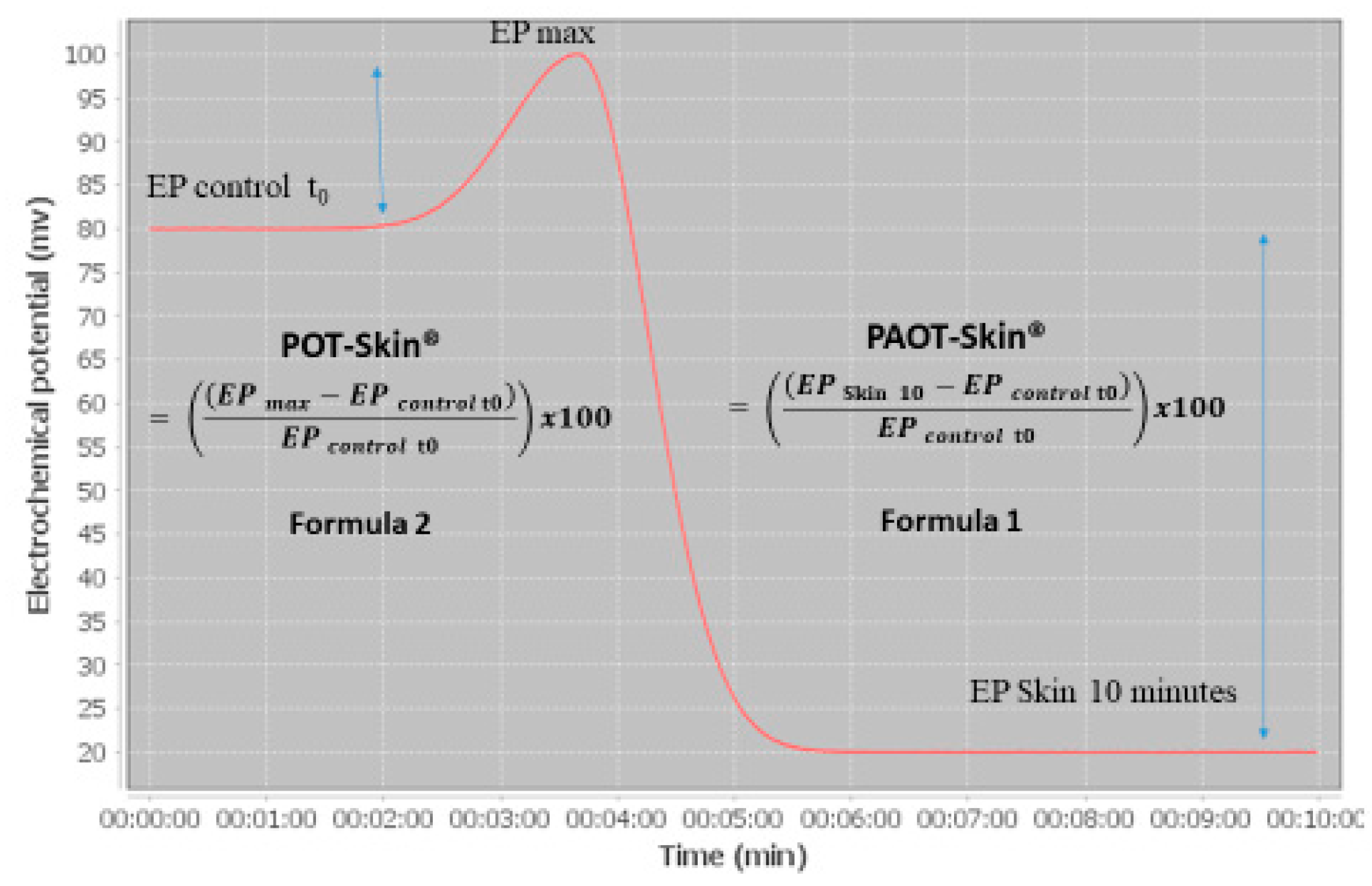
2 skin areas, free of hair, were marked on the left forearm or back. Before analysis, the skin was cleaned with distilled water and dried with absorbent paper. The SOSS evaluation was performed by applying to the tested skin areas a patch constituting 1 mL ECG conductive gel containing both oxidized and reduced iron complex forms (mediator M) and being connected to both working and reference microelectrodes securely attached to the arms. Microelectrodes were recovered by four noble metal alloys, which is actually under patent FR1871986; 11.28.2018. Under these conditions, the initial potential of oxidized/reduced mediator M was around 80 nV, see
Figure 2). SOSS was then estimated by registering for ten minutes the electrochemical potential shift in the gel mixture according to reactions between oxidized/reduced forms of mediator M with, respectively, skin antioxidants or AO (= PAOT-Skin
®) and oxidants or O (= POT-Skin
®).
Results were calculated according to the two following formulas:
where EP
0 is the electrochemical potential at time 0, EP
max is the maximum electrochemical potential and EP
10 is the electrochemical potential registered 10 min after the contact of the patch with the skin. Finally, the PAOT-Skin Score
® was calculated as the ratio PAOT-Skin
®/POT-Skin
®.
2.4. Determination of Antioxidant and Pro-Oxidant Activities Using Electrochemical Detection
For the determination of antioxidant and pro-oxidant activities, the same patch containing ECG conductive gel, mediator M, and microelectrodes as described in
Section 2.3 was directly put in contact with pure antioxidants or oxidant system production in liquid form deposited on a tape strip. PAOT (Pouvoir AntiOxydant Total)-Score
® of antioxidants was calculated according to Equation (1), expressed as ascorbic acid equivalent (AAE)/L gel). When using oxidant sources, POT (Pouvoir Oxidant Total)-Score
® was calculated according to Equation (2), expressed as superoxide anion equivalent (SAE)/L gel × 1000.
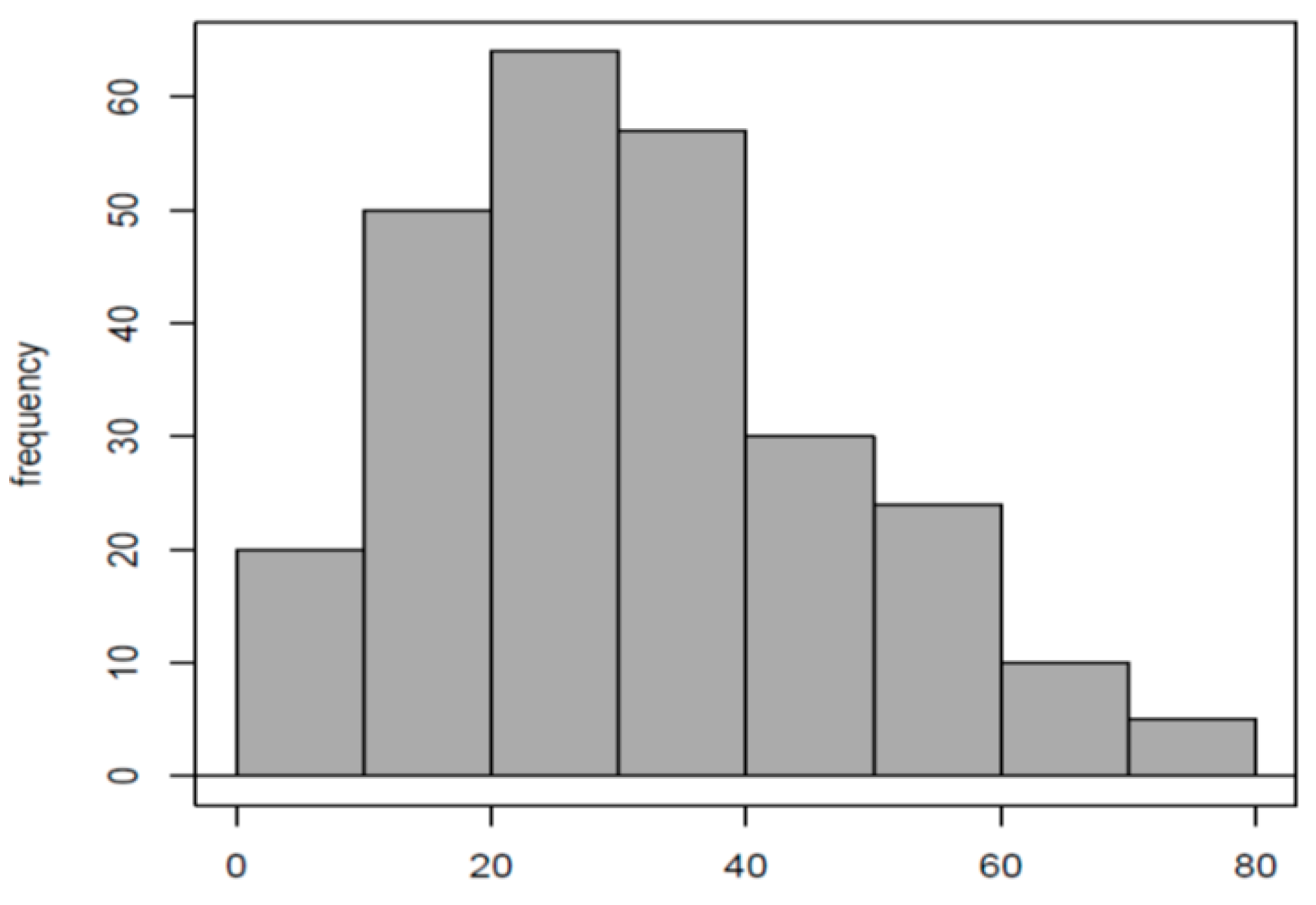
2.5. Normal Reference PAOT-Skin Score® Values and Stability Test
A first group (Group I) consisted of two hundred sixty-three healthily and fasted volunteers aged 20 to 65 years (116 females, 146 males, mean age and standard deviation (SD): 25.49 ± 6.22 years) was recruited for determining normal PAOT-Skin Score® reference values. All subjects were not exposed to sun exposition before experimentation and did not apply products with an anti-wrinkle/anti-ageing/antioxidant action on the forearms during two weeks before the study started. They were also not allowed to consume fruits or fruit juices, or alcohol, or to practice sport during the 48 h preceding the experimentation. For intra-assay CV determination, we selected from this group nine volunteers (Group IIa) on whom the PAOT-Skin Score® was evaluated on the same day 30, 60, 90, 120, and 150 min after the determination of the basal PAOT-Skin Score® (T0). The same volunteers were also solicited to repeat during three straight weeks the measurement of the basal PAOT-Skin Score® in order to determine the inter-assay CV (Group IIb).
2.6. Antioxidant Cream and PAOT-Skin Score®
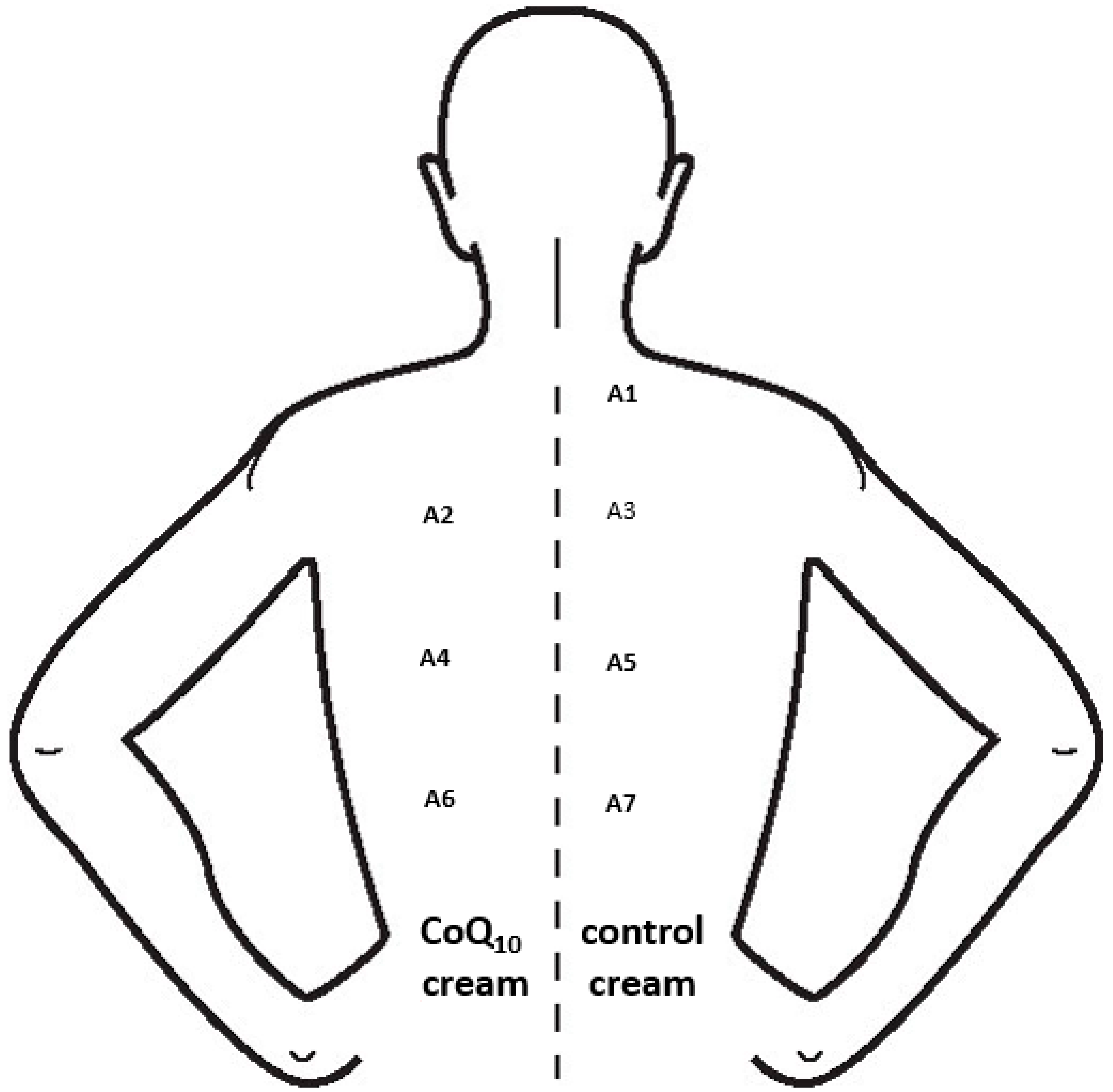
A population of ten females (mean age: 22 years) was recruited for evaluating how the topical application of an antioxidant cream may affect the PAOT-Skin Score
® (Group III). All participants were asked not to take antioxidant supplementation for two weeks or to apply any products over their back on the evening before the experimentation. Both creams with or without reduced CoQ
10 were topically applied on areas of 12 cm
2 from the back according to the protocol described in
Figure 3. In both conditions, PAOT-Skin Score
® (see the Material and Methods section) was evaluated 2, 4, and 6 h after cream application and compared to the measurement performed at T0.
2.7. Antioxidant Intake and PAOT-Skin Score®
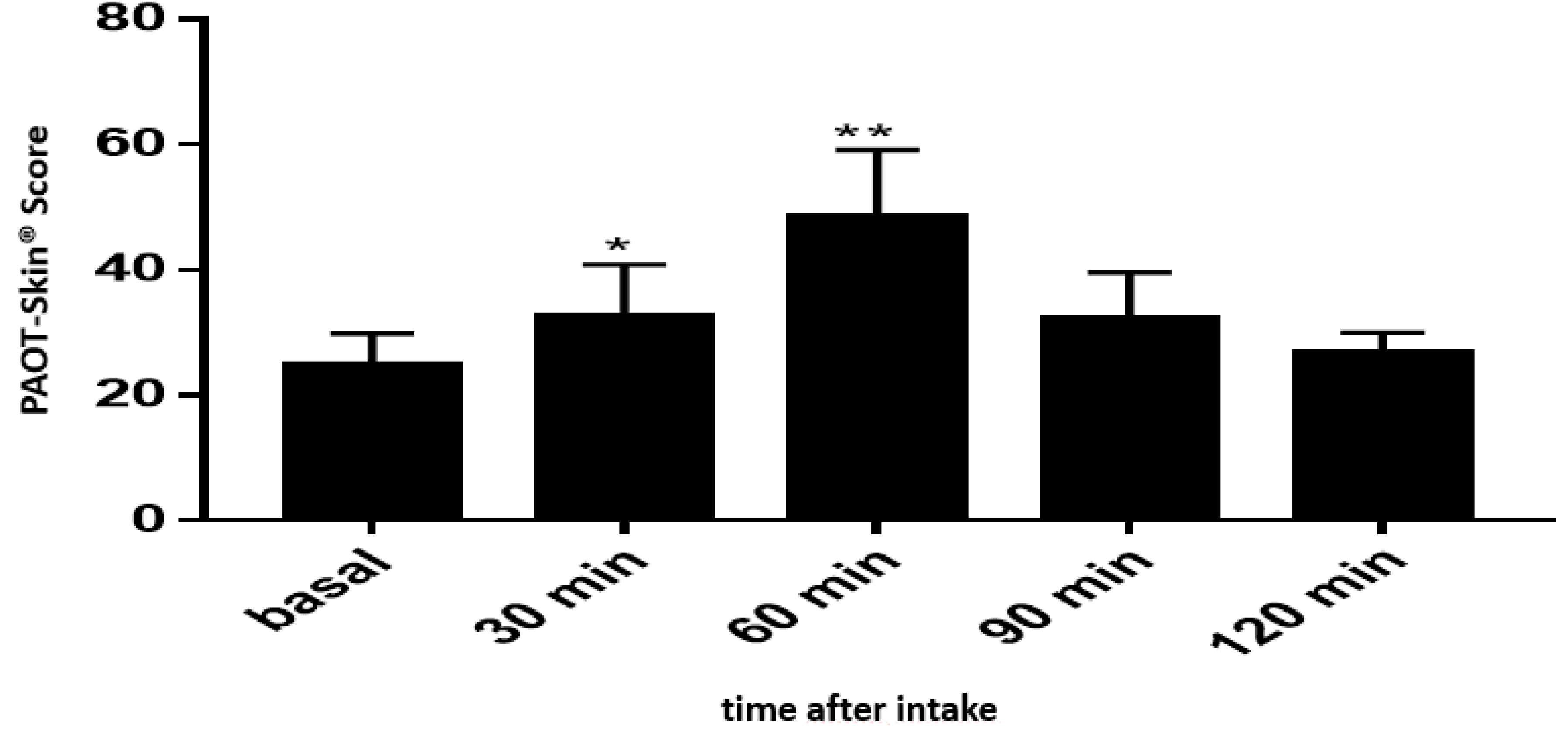
A first intervention study (Group IV) was performed of nine healthy males (25–30 years) in order to check how the intake of orange juice could modulate the PAOT-Skin Score®. An amount of 400 mL of orange juice containing 264 mg vitamin C was ingested by each volunteer being fasted since the evening before the experimentation. The PAOT-Skin Score® was analyzed before ingestion and 30, 60, 90, 120, and 150 min after orange juice intake.
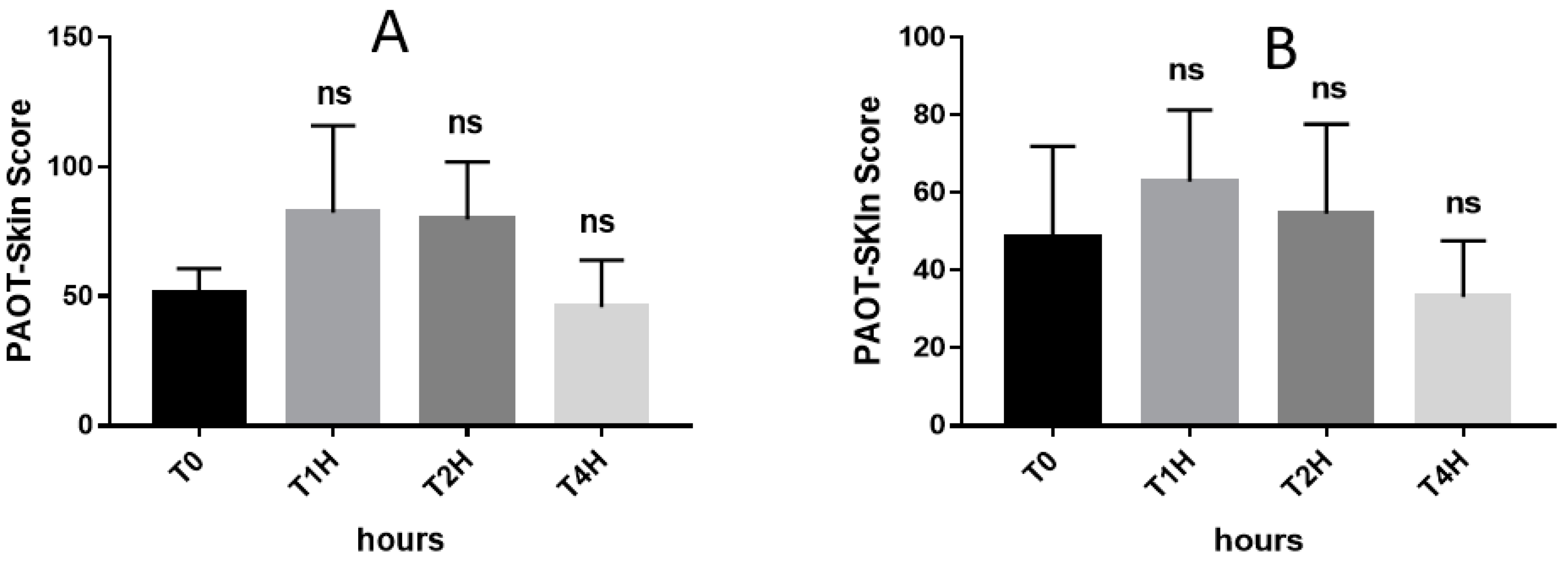
In a second interventional study, six males (45 ± 7 years), fasted for 12 h, received 144 mg vitamin C (two capsules of 72 mg) either as synthetic (n = 3; synthetic vitamin C supplement, Group Va) or natural (n = 3; Arkovital® Pure’Energie containing natural vitamin C, Group Vb) forms (Arkopharma, Carros, France). The PAOT-Skin Score® was examined before and 1, 2, and 4 h after supplement intake.
2.8. Relationship between PAOT-Skin Score® and Biomarkers of Oxidative Stress
Thirty subjects (12 females and 18 males, mean age: 42.9 ± 14.9 years) were selected to compare the PAOT-Skin Score
® with some demographic data and blood or urinary biochemical OS biomarkers (Group VI). Estimation of dietary vitamin C and total polyphenol intakes was achieved using a homemade food frequency questionnaire (FFQ) [
6]. Dietary antioxidants were calculated by multiplying the consumption frequency of each item by the polyphenol content of selected portions. Data on the polyphenol content in foods were extracted from the Phenol-Explorer database which provides data on 502 polyphenol compounds in 452 foods.
2.9. Statistical Analysis
In the study performed in Group I, the distribution normality of PAOT-Skin Score® was tested with the Shapiro–Wilk test. The comparison of all quantitative parameters was performed using the variance analysis (ANOVA) or the Kriskal–Wallis (KW) non-parametric test in the case of asymmetric distribution. In Groups III, IV, and V, t tests were determined using the GraphPad Prism 7. p values < 0.05 were considered as being significant. In Group VI, association between blood OS biomarkers and PAOT-Skin Scores® was determined by the Pearson correlation coefficient or Spearman, in the case of asymmetric distribution. Results were considered as significant for p < 0.05.
4. Discussion
Exploring skin as a matrix for evidencing in vivo OS may represent a promising and complementary analytical method to classical blood biomarker analysis. Major advantages for examining SOSS are multiple: easy access, large surface and, overall, the unique possibility to explore using electrochemical detection for the redox equilibrium between antioxidants and oxidants produced by continual skin exposure to both external and internal sources of ROS production.
Thanks to sensitive reference and working electrodes, our electrochemical method was perfectly able to register potential modifications induced by the interaction of pure antioxidants or sources of oxidant production, respectively, with the oxidized or reduced mediator M contained in the ECG gel (
Table 1). Using ascorbic acid as a reference molecule, the PAOT-Score
® of antioxidants present in the skin, such as glutathione, uric acid, β-carotene, and α-tocopherol [
24], were, respectively, 936, 329, 224, and 155 AAE/L gel). With respect to oxidant sources, it is of interest to note that sodium hypochlorite, tert-buytl hydroperoxide, and hydrogen peroxide, being naturally produced in the skin [
11], exhibited the highest POT-Score
® when compared to superoxide anion taken as the reference system.
When applied to the skin, we confirmed that the ECG gel coupled to sensitive microelectrodes was able to evaluate the SOSS resulting from global potential modifications induced by interactions of oxidized/reduced M with both skin antioxidants (PAOT-Skin
®) and pro-oxidants (POT-Skin
®). The method robustness appeared to be adequate since respective CV inter- (54 measurements) and intra-assay (27 measurements) were of 12.46 ± 4.29% and 7 ± 2.5% (
Table 2 and
Table 3). This can be considered as acceptable for an in vivo methodology. Of high interest was the determination of normal PAOT-Skin Score
® reference values (0–62.94). To the best of our knowledge, such observations have never been conducted for skin OS status. Having in hand this parameter may, therefore, open the door to future clinical studies on populations known to be submitted to high OS, such as smokers or patients having type II diabetes, cardiovascular diseases, or cancer.
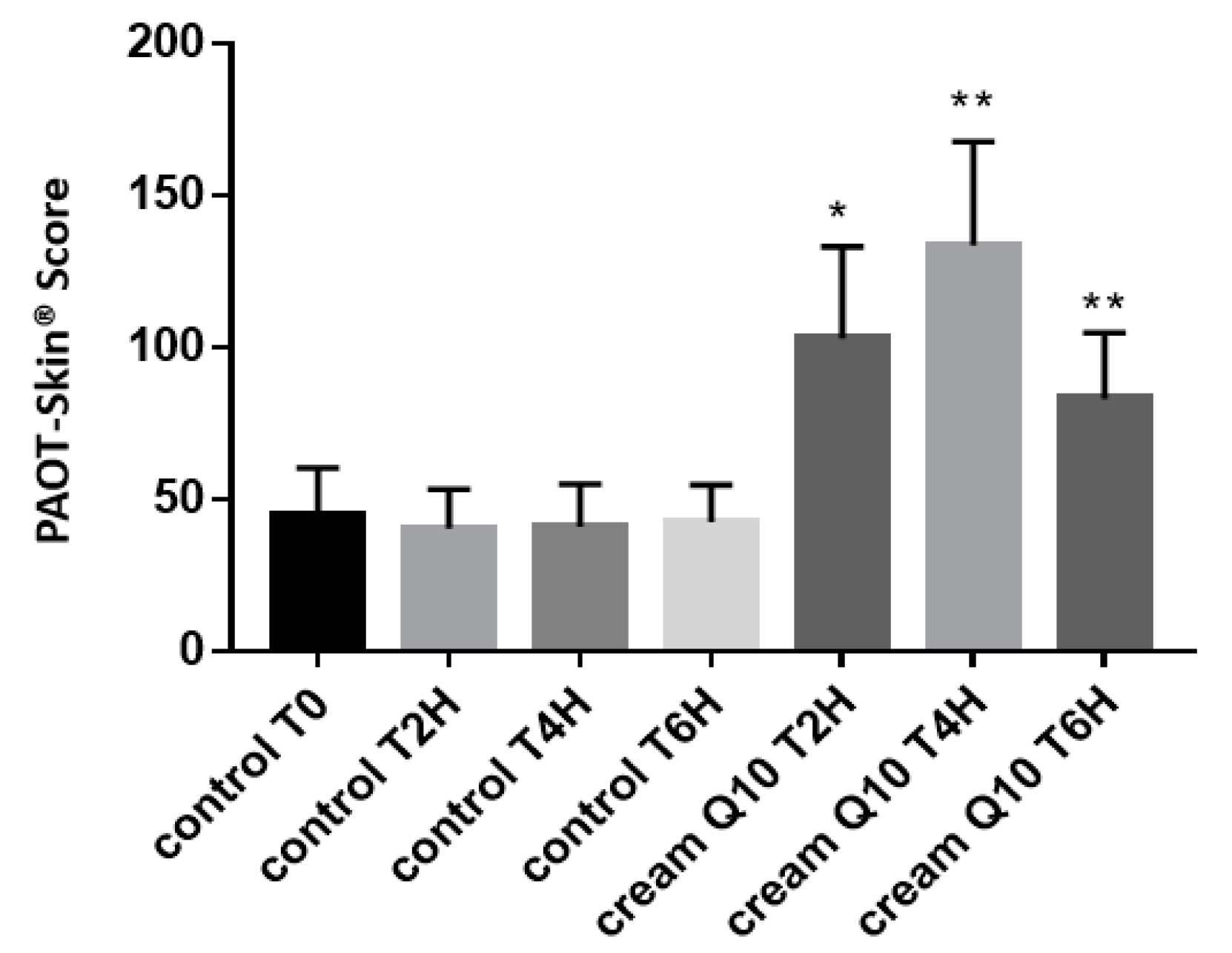
As antioxidants are one of the preferred way for reducing the ageing effect of skin, we investigated with our electrochemical system the impact of a cream enriched in reduced CoQ
10 (ubiquinol) on the PAOT-Skin Score
®. In addition to having potent antioxidant properties [
25], the redox system of oxidized ubiquinone (ubiquinone)/reduced ubiquinone (ubiquinol) plays a major role in the mitochondrial electron transport chain. When compared to a control cream, topical application of reduced CoQ
10 cream resulted, up to six hours after application, in a significant increase of the PAOT-Skin Score
® (150% at four hours) activity as shown in
Figure 5. When compared to the technique described earlier by Ziosi et al. [
26], for the routine evaluation of in vivo efficacy of antioxidant cream, our methodology is easier to use. Indeed, it did not require skin samples collected with adhesive tapes and, then, skin antioxidant extraction from the tapes for analysis by the luminescence method.
Among antioxidants, the roles of vitamin C in skin health have been reviewed in a recent paper by Pullar et al. [
27]. In addition to an antioxidant effect, the presence of a high concentration of vitamin C in the skin has been associated with many potential functions, such as collagen formation, inhibition of melanogenesis, interaction with cell signaling pathways, and the modulation of epigenetic pathways.
Figure 6 depicts that our electrochemical methodology was able to show the in vivo antioxidant effect of orange juice (264 mg vitamin C) intake as evidenced by the 33.9% (
p = 0.047) and 99.3% (
p = 0.011) increase of the PAOT-Skin Score
®, respectively, 30 and 60 min after the 400 mL intake of the beverage. As shown in
Figure 7, a similar increase could also be observed after oral intake of 144 mg natural or synthetic vitamin C in tablets. Statistical analysis revealed, however, that these increases were not statistically significant. This may be attributed to the small number of participants in our study. Similar experiments should be repeated in the long-term using higher doses in vitamin C. Costa et al. [
28] reported an improvement of visible signs of skin ageing in men (
n = 12) after an oral supplementation of 27 mg vitamin C but for six months. On the other hand, McArdel et al. [
29] evidenced that oral vitamin C supplements, at 500 mg vitamin C/day, taken by 12 volunteers for eight weeks resulted in significant rises in plasma and skin vitamin C content.
The great novelty of the present study was to evaluate how the SOSS was associated, or not, with some epidemiological data and classical blood OS biomarkers. In Group VI, we were unable to highlight any association or correlation with all demographic data shown in
Table 4. By contrast, results were more encouraging with OS blood biomarkers.
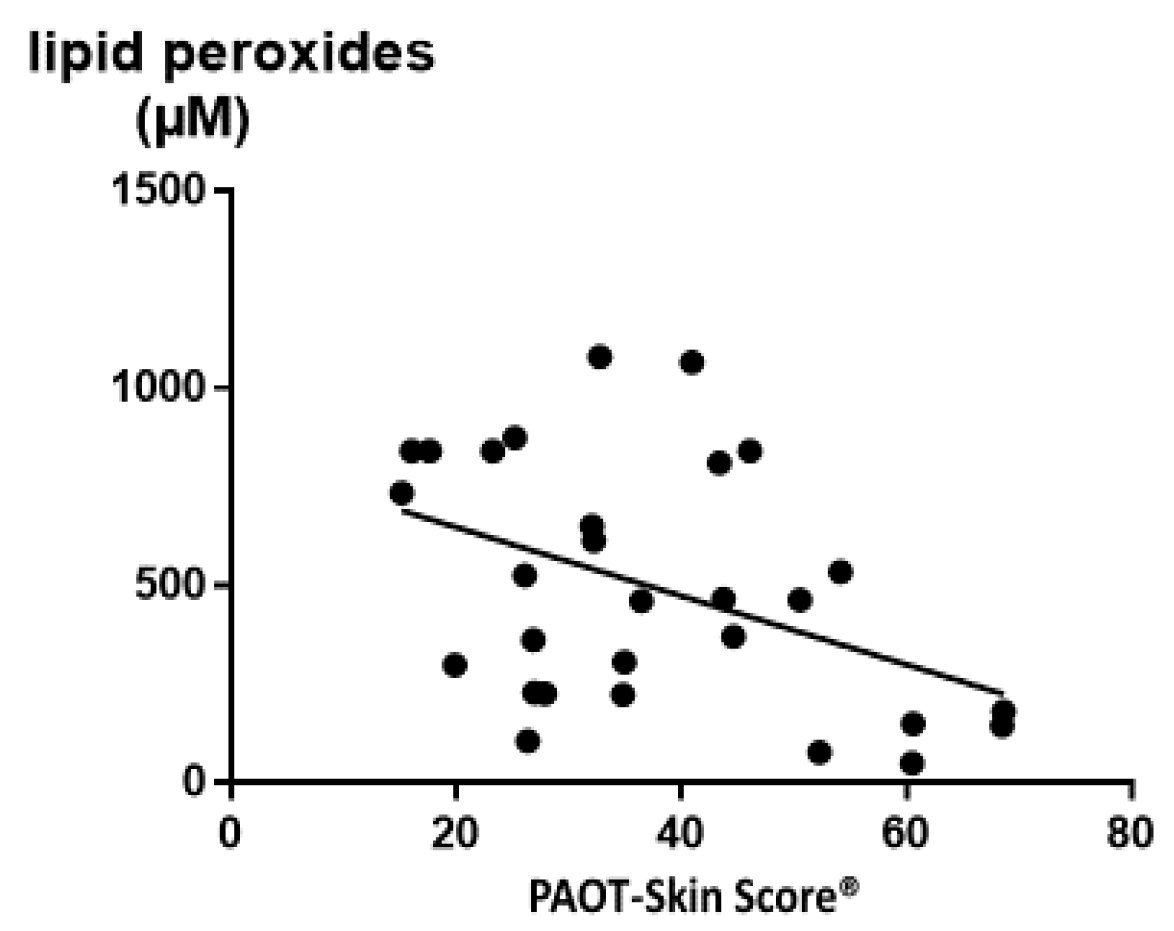
Table 5 shows that all investigated parameters, including antioxidants, trace elements, and oxidative damage biomarkers, were in the normal reference values as established in our hospital routine laboratory. Exceptions were observed for plasma lipid peroxides and the Cu/Zn ratio with a level higher than the upper reference values. Of high interest was evidence of a negative and significant correlation between the PAOT-Skin Score
® and lipid peroxides (r = −0.43,
p = 0.020) resulting from oxidative damage to lipids induced by ROS (
Figure 8). We also found that the PAOT-Skin Score
® was negatively correlated with copper (r = −0.42,
p = 0.022) and the Cu/Zn ratio (r = −0.49,
p = 0.006), both parameters being considered as sources of increased oxidant production through the Fenton reaction (
Table 6). All these observations are in agreement with other papers, with us showing that increased Cu/Zn ratio positively correlated with plasma lipid peroxides, more particularly in women taking contraceptive pills [
30]. At least statistical analysis revealed a positive and significant correlation between the PAOT-Skin Score
® and the γ-tocopherol/α-tocopherol ratio (r = 0.43;
p = 0.020). To our knowledge, no study has investigated in such a deep way potential relationships between SOSS and so large a battery of OS blood biomarkers. Using resonance Raman spectroscopy as the noninvasive methodology, one study has evidenced a significant and positive correlation (r = 0.62,
p < 0.001) between total plasma carotenoid concentrations and skin carotenoid intensities [
13]. However, the major drawback of this method was that it only detected a specific type of antioxidant while skin includes antioxidant enzymes and low-molecular weight antioxidants, such as vitamins C and E, ubiquinone, uric acid, and thiol compounds.
Even if the major limitation of our method was to give a global response, evidence of correlations between some OS blood markers and SOSS allowed, however, to consider our simple and noninvasive approach as a potential screening and inexpensive method for evidencing OS in pathologies such as cancer, diabetes, and neurodegenerative and cardiovascular diseases. Moreover, studies actually under investigation in our laboratory indicate that the PAOT-Skin Score
® could also be associated with the present electrochemical system adapted for liquid samples [
31]. In Group III, data indicated a positive correlation between the PAOT-Urine Score
® and the polyphenols/creatinine ratio (r = 0.41;
p = 0.017) as well as a negative correlation with the oxidized DNA/creatinine ratio (r = −0.48;
p = 0.0092).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}