Social Interaction Improved by Oxytocin in the Subclass of Autism with Comorbid Intellectual Disabilities

 ,
, 
Abstract
1. Introduction
2. Chronic Treatment with OT in Randomized Controlled Trials
3. ASD with Comorbidities
4. RCT for Male ASD Subjects with Low IQ
5. Outcomes
6. Real-Life Assessments of Social Interactions
7. Assessment of Harm: Epilepsy
8. Further Consideration
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Elsabbagh, M.; Divan, G.; Koh, Y.J.; Kim, Y.S.; Kauchali, S.; Marcín, C.; Montiel-Nava, C.; Patel, V.; Paula, C.S.; Wang, C.; et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012, 5, 160–179. [Google Scholar] [CrossRef]
- Richards, C.; Jones, C.; Groves, L.; Moss, J.; Oliver, C. Prevalence of autism spectrum disorder phenomenology in genetic disorders: A systematic review and meta-analysis. Lancet Psychiatry 2015, 2, 909–916. [Google Scholar] [CrossRef]
- Swedo, S.E. Autism Spectrum Disorder. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; pp. 50–59. [Google Scholar]
- Kanner, L. Autistic disturbances of affective contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Asperger, H. Die autistischen Psychopathen im Kindesalter. Arch. Psychiatr. Nervenkr. 1944, 117, 76–136. [Google Scholar] [CrossRef]
- Atherton, G.; Cross, L. Seeing More Than Human: Autism and Anthropomorphic Theory of Mind. Front. Psychol. 2018, 9, 528. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Leslie, A.M.; Frith, U. Does the autistic child have a “theory of mind”? Cognition 1985, 21, 37–46. [Google Scholar] [CrossRef]
- Boucher, J. Putting theory of mind in its place: Psychological explanations of the socio-emotional-communicative impairments in autistic spectrum disorder. Autism 2012, 16, 226–246. [Google Scholar] [CrossRef]
- Senju, A.; Southgate, V.; White, S.; Frith, U. Mindblind eyes: An absence of spontaneous theory of mind in Asperger syndrome. Science 2009, 325, 883–885. [Google Scholar] [CrossRef]
- Ozonoff, S.; Iosif, A.M.; Baguio, F.; Cook, I.C.; Hill, M.M.; Hutman, T.; Rogers, S.J.; Rozga, A.; Sangha, S.; Sigman, M.; et al. A prospective study of the emergence of early behavioral signs of autism. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 256–266.e2. [Google Scholar]
- Howlin, P.; Moss, P. Adults with autism spectrum disorders. Can. J. Psychiatry 2012, 57, 275–283. [Google Scholar] [CrossRef]
- Pronin, E. How we see ourselves and how we see others. Science 2008, 320, 1177–1180. [Google Scholar] [CrossRef]
- Barnbaum, D.R. The Ethics of Autism: Among Them but Not of Them; Indiana University Press: Bloomington, Indiana, 2008; pp. 17–66. [Google Scholar]
- McCracken, J.T.; McGough, J.; Shah, B.; Cronin, P.; Hong, D.; Aman, M.G.; Arnold, L.E.; Lindsay, R.; Nash, P.; Hollway, J.; et al. Risperidone in children with autism and serious behavioral problems. N. Engl. J. Med. 2002, 347, 314–321. [Google Scholar] [CrossRef]
- Anagnostou, E. Clinical trials in autism spectrum disorder: evidence, challenges and future directions. Curr. Opin. Neurol. 2018, 31, 119–125. [Google Scholar] [CrossRef]
- McDougle, C.J.; Holmes, J.P.; Carlson, D.C.; Pelton, G.H.; Cohen, D.J.; Price, L.H. A double-blind, placebo-controlled study of risperidone in adults with autistic disorder and other pervasive developmental disorders. Arch. Gen. Psychiatry 1998, 55, 633–641. [Google Scholar] [CrossRef]
- Goel, R.; Hong, J.S.; Findling, R.L.; Ji, N.Y. An update on pharmacotherapy of autism spectrum disorder in children and adolescents. Int. Rev. Psychiatry 2018, 30, 78–95. [Google Scholar] [CrossRef]
- Bishop-Fitzpatrick, L.; Minshew, N.J.; Eack, S.M. A systematic review of psychosocial interventions for adults with autism spectrum disorders. J. Autism. Dev. Disord. 2013, 43, 687–694. [Google Scholar] [CrossRef]
- Scahill, L.; Hallett, V.; Aman, M.G.; McDougle, C.J.; Eugene, A.L.; McCracken, J.T.; Tierney, E.; Deng, Y.; Dziura, J.; Vitiello, B. Brief Report: social disability in autism spectrum disorder: results from Research Units on Pediatric Psychopharmacology (RUPP) Autism Network trials. J. Autism Dev. Disord. 2013, 43, 739–746. [Google Scholar] [CrossRef]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The aberrant behavior checklist: A behavior rating scale for the assessment of treatment effects. Am. J. Ment. Defic. 1985, 89, 485–491. [Google Scholar]
- Pedersen, C.A.; Prange, A.J., Jr. Induction of maternal behavior in virgin rats after intracerebroventricular administration of oxytocin. Proc. Natl. Acad. Sci. USA 1979, 76, 6661–6665. [Google Scholar] [CrossRef]
- Jin, D.; Liu, H.X.; Hirai, H.; Torashima, T.; Nagai, T.; Lopatina, O.; Shnayder, N.A.; Yamada, K.; Noda, M.; Seike, T.; et al. CD38 is critical for social behaviour by regulating oxytocin secretion. Nature 2007, 446, 41–45. [Google Scholar] [CrossRef]
- Goodson, J.L.; Thompson, R.R. Nonapeptide mechanisms of social cognition, behavior and species-specific social systems. Curr. Opin. Neurobiol. 2010, 20, 784–794. [Google Scholar] [CrossRef]
- Johnson, Z.V.; Young, L.J. Evolutionary diversity as a catalyst for biological discovery. Integr. Zool. 2018, 13, 616–633. [Google Scholar] [CrossRef]
- Insel, T.R. The challenge of translation in social neuroscience: A review of oxytocin, vasopressin, and affiliative behavior. Neuron 2010, 65, 768–779. [Google Scholar] [CrossRef]
- Torres, N.; Martins, D.; Santos, A.J.; Prata, D.; Veríssimo, M. How do hypothalamic nonapeptides shape youth’s sociality? A systematic review on oxytocin, vasopressin and human socio-emotional development. Neurosci. Biobehav. Rev. 2018, 90, 309–331. [Google Scholar]
- Grinevich, V.; Desarménien, M.G.; Chini, B.; Tauber, M.; Muscatelli, F. Ontogenesis of oxytocin pathways in the mammalian brain: late maturation and psychosocial disorders. Front. Neuroanat. 2015, 8, 164. [Google Scholar] [CrossRef]
- Bartz, J.A.; Zaki, J.; Bolger, N.; Ochsner, K.N. Social effects of oxytocin in humans: Context and person matter. Trends Cogn. Sci. 2011, 15, 301–309. [Google Scholar] [CrossRef]
- Chini, B.; Leonzino, M.; Braida, D.; Sala, M. Learning About Oxytocin: Pharmacologic and Behavioral Issues. Biol. Psychiatry 2014, 76, 360–366. [Google Scholar] [CrossRef]
- Yamasue, H.; Domes, G. Oxytocin and Autism Spectrum Disorders. Curr. Top. Behav. Neurosci. 2017, 35, 449–465. [Google Scholar]
- Feldman, R. The Neurobiology of Human Attachments. Trends Cogn. Sci. 2017, 21, 80–99. [Google Scholar] [CrossRef]
- Francis, S.M.; Sagar, A.; Levin-Decanini, T.; Liu, W.; Carter, C.S.; Jacob, S. Oxytocin and vasopressin systems in genetic syndromes and neurodevelopmental disorders. Brain Res. 2014, 1580, 199–218. [Google Scholar] [CrossRef]
- Modahl, C.; Green, L.; Fein, D.; Morris, M.; Waterhouse, L.; Feinstein, C.; Levin, H. Plasma oxytocin levels in autistic children. Biol. Psychiatry 1998, 43, 270–277. [Google Scholar]
- Green, L.; Fein, D.; Modahl, C.; Feinstein, C.; Waterhouse, L.; Morris, M. Oxytocin and autistic disorder: alterations in peptide forms. Biol. Psychiatry 2001, 50, 609–613. [Google Scholar] [CrossRef]
- Neumann, I.D.; Slattery, D.A. Oxytocin in General Anxiety and Social Fear: A Translational Approach. Biol. Psychiatry 2016, 79, 213–221. [Google Scholar] [CrossRef]
- Jacobson, J.D.; Ellerbeck, K.A.; Kelly, K.A.; Fleming, K.K.; Jamison, T.R.; Coffey, C.W.; Smith, C.M.; Reese, R.M.; Sands, S.A. Evidence for alterations in stimulatory G proteins and oxytocin levels in children with autism. Psychoneuroendocrinology 2014, 40, 159–169. [Google Scholar] [CrossRef]
- Munesue, T.; Yokoyama, S.; Nakamura, K.; Anitha, A.; Yamada, K.; Hayashi, K.; Asaka, T.; Liu, H.X.; Jin, D.; Koizumi, K.; et al. Two genetic vriants of CD338 in subjects with autism spectrum disorder and controls. Neurosci. Res. 2010, 67, 181–191. [Google Scholar] [CrossRef]
- Sauer, C.; Montag, C.; Wörner, C.; Kirsch, P.; Reuter, M. Effects of a common variant in the CD38 gene on social processing in an oxytocin challenge study: possible links to autism. Neuropsychopharmacology 2012, 37, 1474–1482. [Google Scholar] [CrossRef]
- Feldman, R.; Zagoory-Sharon, O.; Weisman, O.; Schneiderman, I.; Gordon, I.; Maoz, R.; Shalev, I.; Ebstein, R.P. Sensitive parenting is associated with plasma oxytocin and polymorphisms in the OXTR and CD38 genes. Biol. Psychiatry 2012, 72, 175–181. [Google Scholar] [CrossRef]
- Salmina, A.B.; Lopatina, O.; Kuvacheva, N.V.; Higashida, H. Integrative neurochemistry and neurobiology of social recognition and behavior analyzed with respect to CD38-dependent brain oxytocin secretion. Curr. Top. Med. Chem. 2013, 13, 2965–2977. [Google Scholar] [CrossRef]
- Ma, W.J.; Hashii, M.; Munesue, T.; Hayashi, K.; Yagi, K.; Yamagishi, M.; Higashida, H.; Yokoyama, S. Non-synonymous single-nucleotide variations of the human oxytocin receptor gene and autism spectrum disorders: a case-control study in a Japanese population and functional analysis. Mol. Autism 2013, 4, 22. [Google Scholar] [CrossRef]
- Campbell, D.B.; Datta, D.; Jones, S.T.; Batey Lee, E.; Hammock, E.A.; Levitt, P. Association of oxytocin receptor (OXTR) gene variants with multiple phenotype domains of autism spectrum disorder. J. Neurodev. Disord. 2011, 3, 101–112. [Google Scholar] [CrossRef]
- Okamoto, Y.; Ishitobi, M.; Wada, Y.; Kosaka, H. The Potential of Nasal Oxytocin Administration for Remediation of Autism Spectrum Disorders. CNS Neurol. Disord. Drug. Targets 2016, 15, 564–577. [Google Scholar] [CrossRef]
- Hollander, E.; Novotny, S.; Hanratty, M.; Yaffe, R.; DeCaria, C.M.; Aronowitz, B.R.; Mosovich, S. Oxytocin infusion reduces repetitive behaviors in adults with autistic and Asperger’s disorders. Neuropsychopharmacology 2003, 28, 193–198. [Google Scholar] [CrossRef]
- Hollander, E.; Bartz, J.; Chaplin, W.; Phillips, A.; Sumner, J.; Soorya, L.; Anagnostou, E.; Wasserman, S. Oxytocin increases retention of social cognition in autism. Biol. Psychiatry 2007, 61, 498–503. [Google Scholar] [CrossRef]
- Guastella, A.J.; Einfeld, S.L.; Gray, K.M.; Rinehart, N.J.; Tonge, B.J.; Lambert, T.J.; Hickie, I.B. Intranasal oxytocin improves emotion recognition for youth with autism spectrum disorders. Biol. Psychiatry 2010, 67, 692–694. [Google Scholar] [CrossRef]
- Andari, E.; Duhamel, J.R.; Zalla, T.; Herbrecht, E.; Leboyer, M.; Sirigu, A. Promoting social behavior with oxytocin in high-functioning autism spectrum disorders. Proc. Natl. Acad. Sci. USA 2010, 107, 4389–4394. [Google Scholar] [CrossRef]
- Bakermans-Kranenburg, M.J.; van Ijzendoorn, M.H. Sniffing around oxytocin: review and meta-analyses of trials in healthy and clinical groups with implications for pharmacotherapy. Transl. Psychiatry 2013, 3, e258. [Google Scholar] [CrossRef]
- Domes, G.; Heinrichs, M.; Kumbier, E.; Grossmann, A.; Hauenstein, K.; Herpertz, S.C. Effects of intranasal oxytocin on the neural basis of face processing in autism spectrum disorder. Biol. Psychiatry 2013, 74, 164–171. [Google Scholar] [CrossRef]
- Watanabe, T.; Abe, O.; Kuwabara, H.; Yahata, N.; Takano, Y.; Iwashiro, N.; Natsubori, T.; Aoki, Y.; Takao, H.; Kawakubo, Y. Mitigation of sociocommunicational deficits of autism through oxytocin-induced recovery of medial prefrontal activity: A randomized trial. JAMA Psychiatry 2014, 71, 166–175. [Google Scholar] [CrossRef]
- Domes, G.; Kumbier, E.; Heinrichs, M.; Herpertz, S.C. Oxytocin promotes facial emotion recognition and amygdala reactivity in adults with Asperger syndrome. Neuropsychopharmacology 2014, 39, 698–706. [Google Scholar] [CrossRef]
- Alvares, G.A.; Quintana, D.S.; Whitehouse, A.J. Beyond the hype and hope: Critical considerations for intranasal oxytocin research in autism spectrum disorder. Autism Res. 2017, 10, 25–41. [Google Scholar] [CrossRef]
- DeMayo, M.M.; Song, Y.J.C.; Hickie, I.B.; Guastella, A.J. A Review of the Safety, Efficacy and Mechanisms of Delivery of Nasal Oxytocin in Children: Therapeutic Potential for Autism and Prader-Willi Syndrome, and Recommendations for Future Research. Paediatr. Drugs 2017, 19, 391–410. [Google Scholar] [CrossRef]
- Yamasue, H. Promising evidence and remaining issues regarding the clinical application of oxytocin in autism spectrum disorders. Psychiatry Clin. Neurosci. 2016, 70, 89–99. [Google Scholar] [CrossRef]
- Guastella, A.J.; Hickie, I.B. Oxytocin Treatment, Circuitry, and Autism: A Critical Review of the Literature Placing Oxytocin Into the Autism Context. Biol. Psychiatry 2016, 79, 234–242. [Google Scholar] [CrossRef]
- Aoki, Y.; Watanabe, T.; Abe, O.; Kuwabara, H.; Yahata, N.; Takano, Y.; Iwashiro, N.; Natsubori, T.; Takao, H.; Kawakubo, Y. Oxytocin’s neurochemical effects in the medial prefrontal cortex underlie recovery of task-specific brain activity in autism: A randomized controlled trial. Mol. Psychiatry 2015, 20, 447–453. [Google Scholar] [CrossRef]
- Auyeung, B.; Lombardo, M.V.; Heinrichs, M.; Chakrabarti, B.; Sule, A.; Deakin, J.B. Oxytocin increases eye contact during a real-time, naturalistic social interaction in males with and without autism. Transl. Psychiatry 2015, 5, e507. [Google Scholar] [CrossRef]
- Quintana, D.S.; Westlye, L.T.; Hope, S.; Nærland, T.; Elvsåshagen, T.; Dørum, E.; Rustan, Ø.; Valstad, M.; Rezvaya, L.; Lishaugen, H.; et al. Dose-dependent social-cognitive effects of intranasal oxytocin delivered with novel Breath Powered device in adults with autism spectrum disorder: A randomized placebo-controlled double-blind crossover trial. Transl. Psychiatry 2017, 7, e1136. [Google Scholar] [CrossRef]
- Munesue, T.; Nakamura, H.; Kikuchi, M.; Miura, Y.; Takeuchi, N.; Anme, T.; Nanba, E.; Adachi, K.; Tsubouchi, K.; Sai, Y.; et al. Oxytocin for Male Subjects with Autism Spectrum Disorder and Comorbid Intellectual Disabilities: A Randomized Pilot Study. Front. Psychiatry 2016, 7, 2. [Google Scholar] [CrossRef]
- Kosaka, H.; Okamoto, Y.; Munesue, T.; Yamasue, H.; Inohara, K.; Fujioka, T.; Anme, T.; Orisaka, M.; Ishitobi, M.; Jung, M.; et al. Oxytocin efficacy is modulated by dosage and oxytocin receptor genotype in young adults with high-functioning autism: A 24-week randomized clinical trial. Transl. Psychiatry 2016, 6, e872. [Google Scholar] [CrossRef]
- Yamasue, H.; Okada, T.; Munesue, T.; Kuroda, M.; Fujioka, T.; Uno, Y.; Matsumoto, K.; Kuwabara, H.; Mori, D.; Okamoto, Y.; et al. Effect of intranasal oxytocin on the core social symptoms of autism spectrum disorder: A randomized clinical trial. Mol. Psychiatry 2018. [Google Scholar] [CrossRef]
- Anagnostou, E.; Soorya, L.; Chaplin, W.; Bartz, J.; Halpern, D.; Wasserman, S.; Wang, A.T.; Pepa, L.; Tanel, N.; Kushki, A.; et al. Intranasal oxytocin versus placebo in the treatment of adults with autism spectrum disorders: A randomized controlled trial. Mol. Autism 2012, 3, 16. [Google Scholar] [CrossRef]
- Dadds, M.R.; MacDonald, E.; Cauchi, A.; Williams, K.; Levy, F.; Brennan, J. Nasal oxytocin for social deficits in childhood autism: A randomized controlled trial. J. Autism. Dev. Disord. 2014, 44, 521–531. [Google Scholar] [CrossRef]
- Guastella, A.J.; Gray, K.M.; Rinehart, N.J.; Alvares, G.A.; Tonge, B.J.; Hickie, I.B.; Keating, C.M.; Cacciotti-Saija, C.; Einfeld, S.L. The effects of a course of intranasal oxytocin on social behaviors in youth diagnosed with autism spectrum disorders: A randomized controlled trial. J. Child Psychol. Psychiatry 2015, 56, 444–452. [Google Scholar] [CrossRef]
- Watanabe, T.; Kuroda, M.; Kuwabara, H.; Aoki, Y.; Iwashiro, N.; Tatsunobu, N.; Takao, H.; Nippashi, Y.; Kawakubo, Y.; Kunimatsu, A.; et al. Clinical and neural effects of six-week administration of oxytocin on core symptoms of autism. Brain 2015, 138, 3400–3412. [Google Scholar] [CrossRef]
- Yatawara, C.J.; Einfeld, S.L.; Hickie, I.B.; Davenport, T.A.; Guastella, A.J. The effect of oxytocin nasal spray on social interaction deficits observed in young children with autism: A randomized clinical crossover trial. Mol. Psychiatry 2016, 21, 1225–1231. [Google Scholar] [CrossRef]
- Parker, K.J.; Oztan, O.; Libove, R.A.; Sumiyoshi, R.D.; Jackson, L.P.; Karhson, D.S.; Summers, J.E.; Hinman, K.E.; Motonaga, K.S.; Phillips, J.M.; et al. Intranasal oxytocin treatment for social deficits and biomarkers of response in children with autism. Proc. Natl. Acad. Sci. USA 2017, 114, 8119–8124. [Google Scholar] [CrossRef]
- Baird, G.; Simonoff, E.; Pickles, A.; Chandler, S.; Loucas, T.; Meldrum, D.; Charman, T. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). Lancet 2006, 368, 210–215. [Google Scholar] [CrossRef]
- Tager-Flusberg, H.; Kasari, C. Minimally verbal school-aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Res. 2013, 6, 468–478. [Google Scholar] [CrossRef]
- Cai, Q.; Feng, L.; Yap, K.Z. Systematic review and meta-analysis of reported adverse events of long-term intranasal oxytocin treatment for autism spectrum disorder. Psychiatry Clin. Neurosci. 2018, 72, 140–151. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000; pp. 69–84. [Google Scholar]
- Humble, M.B.; Uvnäs-Moberg, K.; Engström, I.; Bejerot, S. Plasma oxytocin changes and anti-obsessive response during serotonin reuptake inhibitor treatment: A placebo controlled study. BMC Psychiatry 2013, 13, 344. [Google Scholar] [CrossRef]
- Russell, A.J.; Mataix-Cols, D.; Anson, M.; Murphy, D.G. Obsessions and compulsions in Asperger syndrome and high-functioning autism. Br. J. Psychiatry 2005, 186, 525–528. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the Mind in the Eyes” Test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2012, 42, 241–251. [Google Scholar] [CrossRef]
- Kosaka, H.; Munesue, T.; Ishitobi, M.; Asano, M.; Omori, M.; Sato, M.; Anme, T.; Orisaka, M.; Ishitobi, M.; Jung, M.; et al. Long-term oxytocin administration improves social behaviors in a girl with autistic disorder. BMC Psychiatry 2012, 12, 110. [Google Scholar] [CrossRef]
- Tachibana, M.; Kagitani-Shimono, K.; Mohri, I.; Yamamoto, T.; Sanefuji, W.; Nakamura, A.; Oishi, M.; Kimura, T.; Onaka, T.; Ozono, K.; et al. Long-term administration of intranasal oxytocin is a safe and promising therapy for early adolescent boys with autism spectrum disorders. J. Child Adolesc. Psychopharmacol. 2013, 23, 123–127. [Google Scholar] [CrossRef]
- Anagnostou, E.; Soorya, L.; Brian, J.; Dupuis, A.; Mankad, D.; Smile, S.; Jacob, S. Intranasal oxytocin in the treatment of autism spectrum disorders: A review of literature and early safety and efficacy data in youth. Brain Res. 2014, 1580, 188–198. [Google Scholar] [CrossRef]
- Kaplan, E. A generalized epileptiform convulsion after intra-amniotic prostaglandin with intravenous oxytocin infusion: A case report. S. Afr. Med. J. 1978, 53, 27–29. [Google Scholar]
- Pedlow, P.R. Syntocinon induced convulsion. J. Obstet. Gynaecol. Br. Common. 1970, 77, 1113–1114. [Google Scholar] [CrossRef]
- Loyens, E.; Vermoesen, K.; Schallier, A.; Michotte, Y.; Smolders, I. Proconvulsive effects of oxytocin in the generalized pentylenetetrazol mouse model are mediated by vasopressin 1a receptors. Brain Res. 2012, 1436, 43–50. [Google Scholar] [CrossRef]
- Sala, M.; Braida, D.; Lentini, D.; Busnelli, M.; Bulgheroni, E.; Capurro, V.; Finardi, A.; Donzelli, A.; Pattini, L.; Rubino, T.; et al. Pharmacologic rescue of impaired cognitive flexibility, social deficits, increased aggression, and seizure susceptibility in oxytocin receptor null mice: A neurobehavioral model of autism. Biol. Psychiatry 2011, 69, 875–882. [Google Scholar] [CrossRef]
- Amiet, C.; Gourfinkel-An, I.; Bouzamondo, A.; Tordjman, S.; Baulac, M.; Lechat, P.; Tordjman, S.; Cohen, D. Epilepsy in autism is associated with intellectual disability and gender: Evidence from a meta-analysis. Biol. Psychiatry 2008, 64, 577–582. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Liang, M.; Munesue, S.; Deguchi, K.; Harashima, A.; Furuhara, K.; Yuhi, T.; Zhong, J.; Akther, S.; Goto, H.; et al. Vascular RAGE transports oxytocin into the brain to elicit its maternal bonding behaviour in mice. Commun. Biol. in press. [CrossRef]

{kind=link}
| Study | Drug | Age | IQ | Male/Female | Dose/day | Duration | Primary Outcomes | Effect | Other Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Anagnostou 2012 | OT | 33.2 | 99 | 9/1 | 48 IU | 6 weeks | DANNA GCI-I RBS-R | No No No | Reading mind improved |
| Anagnostou 2012 | PL | 33.8 | 118 | 7/2 | |||||
| Dadds 2014 | OT | 11.8 | 19/0 | 24 IU | 4 days | Eye-contact Child verbal contact Social skills | No No No | ||
| Dadds 2014 | PL | 10.7 | 19/0 | ||||||
| Guastella 2015 | OT | 13.9 | 80 | 26/0 | 18 or 24 IU | 4 or 8 weeks | SRS CGI-I | No No | |
| Guastella 2015 | PL | 14.0 | 93 | 24/0 | |||||
| Watanabe 2015 | OL | 35.1 | 109 | 9/0 | 48 IU | 6 weeks | ADOS recip. | Improved | |
| Watanabe 2015 | PL | 29.3 | 101 | 9/0 | |||||
| Yatawara 2015 | OT | 5.7 | 97 | 14/1 | 24 IU | 5 weeks | SRS-P RBS-R | Improved No | |
| Yatawara 2015 | PL | 6.7 | 97 | 13/1 | |||||
| Munesue 2016 | OT | 22.6 | 24.9 | 15/0 | 16 IU | 8 weeks | CARS | No | Social interaction improved |
| Munesue 2016 | PL | 37.5 | 24.9 | 14/0 | |||||
| Kosaka 2016 | OT | 23.1 | 99.2 | 15/2 | 16 IU | 12 weeks | CGI-I IRSA | Improved No | |
| Kosaka 2016 | OT | 24.8 | 102.3 | 13/6 | 32 IU | 12 weeks | CGI-I IRSA | Improved No | Dose- and SNP-dependen-tly improved |
| Kosaka 2016 | PL | 24.9 | 98.5 | 15/3 | |||||
| Parker 2017 | OT | 9.4 | 65 | 13/1 | 24 IU | 4 weeks | SRS | Improved | |
| Parker 2017 | PL | 8.1 | 67 | 14/0 | |||||
| Yamasue 2019 | OT | 27.6 | 106 | 53/0 | 48 IU | 6 weeks | ADOS | No | Repetitive behavior improved |
| Yamasue 2019 | PL | 26.3 | 108 | 53/0 |
| A. Verbal Communication |
| A-1. His mother said the following: “My sister’s family lives nearby and they visit two or three times a month. When they visited, I felt that my son interrupted my conversations with my sister more often than before.” |
| A-2. “He joined in with the family conversation.” |
| A-3. “When my son was alone with me, he did not initiate conversation very often before, but recently he has done so somewhat more frequently.” |
| A-4. His mother said the following: “When I have picked up my son at the school, he recently has begun to speak, for example, that he had done his best today or that he had acted violently. Previously, he only spoke when I asked him.” |
| B. Flexibility in Behavior |
| B-1. His mother said the following: “Recently, my son has been less lethargic and did not wander around as much as that seen previously.” |
| B-2. “My son sometimes has drawn pictures of Anpanman (a cartoon character) as always at home. Recently, Anpanman’s expression has appeared to soften. He did not write very often in the past but has been writing a lot lately.” |
| B-3. “There was one thing that he always wanted to buy, Donbei (instant udon noodles), whenever we go to a convenience store. However, the other day, when we told him, ‘Stop buying that,’ he did so. We have not experienced anything like this before.” |
| B-4. “When we tell him to stop a given restricted behavior, he sometimes stops.” |
| C. Sympathy |
| C-1. “He cared for his young brother, when the brother came back during a holiday.” |
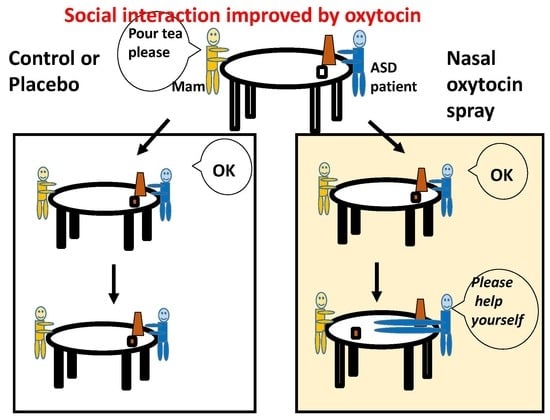
| C-2. “He handed me my tea cup after filling it with tea, when I asked him to pour tea.” |
| C-3. “He looked at us with a calm face for a long time.” |
| D. Attitude toward Life |
| D-1. “Recent entries in the correspondence book from the vocational aid center indicated that he seemed to be more motivated while at work.” |
| E. Self-Harm |
| E-1. “Self-injurious behaviors have lessened a little” |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higashida, H.; Munesue, T.; Kosaka, H.; Yamasue, H.; Yokoyama, S.; Kikuchi, M. Social Interaction Improved by Oxytocin in the Subclass of Autism with Comorbid Intellectual Disabilities. Diseases 2019, 7, 24. https://doi.org/10.3390/diseases7010024
Higashida H, Munesue T, Kosaka H, Yamasue H, Yokoyama S, Kikuchi M. Social Interaction Improved by Oxytocin in the Subclass of Autism with Comorbid Intellectual Disabilities. Diseases. 2019; 7(1):24. https://doi.org/10.3390/diseases7010024
Chicago/Turabian StyleHigashida, Haruhiro, Toshio Munesue, Hirotaka Kosaka, Hidenori Yamasue, Shigeru Yokoyama, and Mitsuru Kikuchi. 2019. "Social Interaction Improved by Oxytocin in the Subclass of Autism with Comorbid Intellectual Disabilities" Diseases 7, no. 1: 24. https://doi.org/10.3390/diseases7010024
APA StyleHigashida, H., Munesue, T., Kosaka, H., Yamasue, H., Yokoyama, S., & Kikuchi, M. (2019). Social Interaction Improved by Oxytocin in the Subclass of Autism with Comorbid Intellectual Disabilities. Diseases, 7(1), 24. https://doi.org/10.3390/diseases7010024