
The Relationship between Walking Speed and Step Length in Older Aged Patients

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
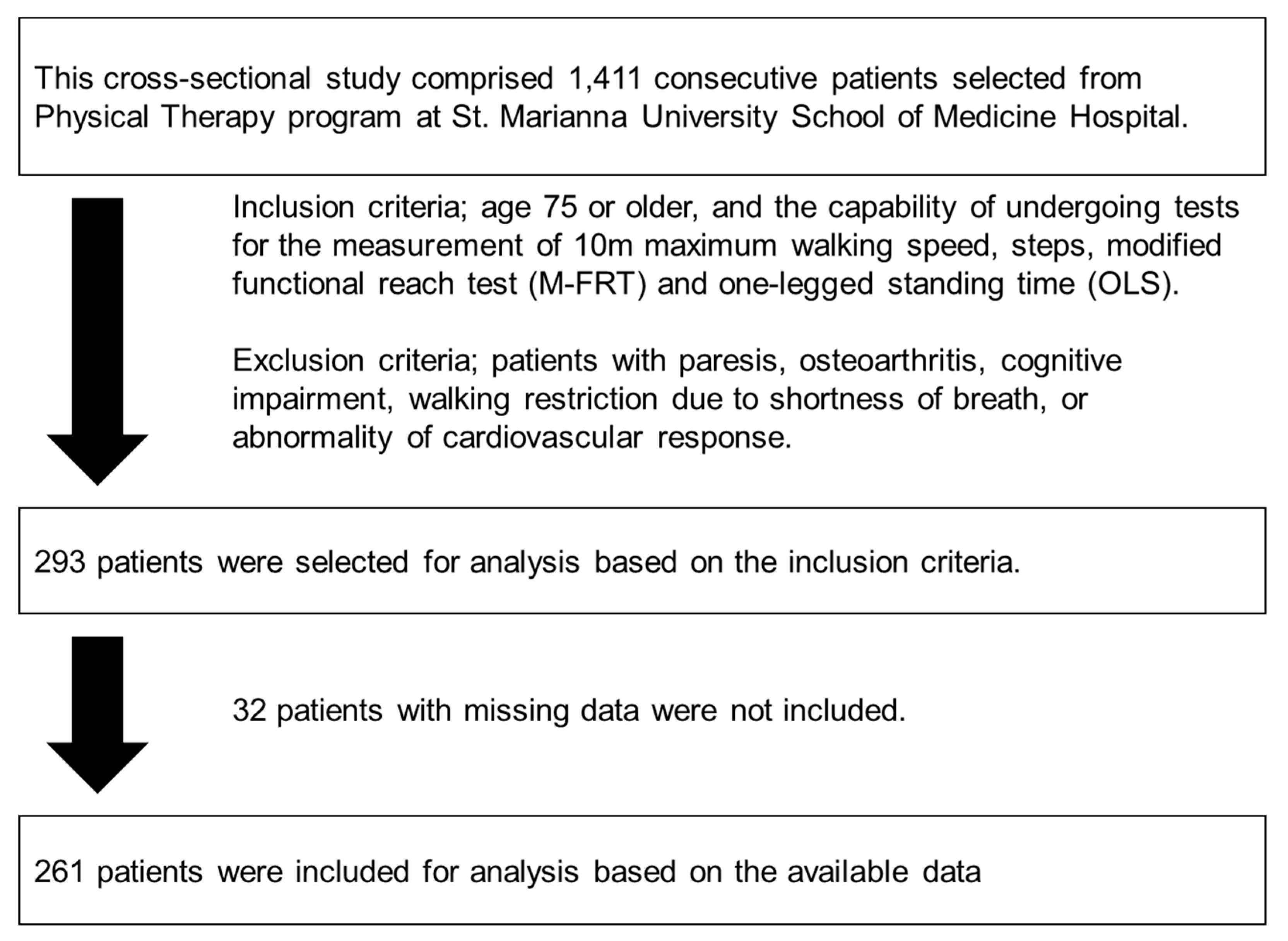
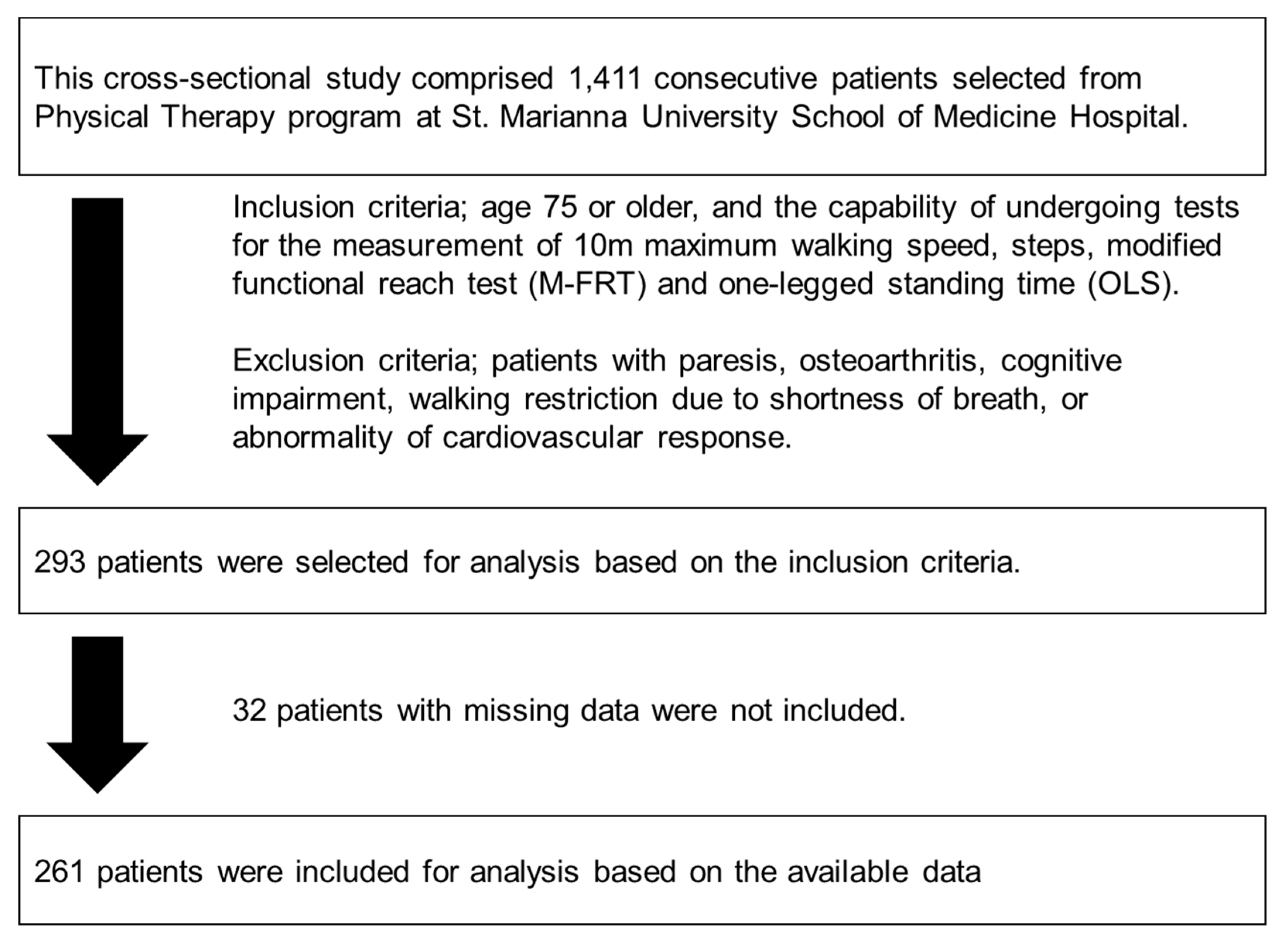
2.1. Study Design
2.2. Data Selection and Extraction
2.3. Ethics
2.4. Statistical Analysis
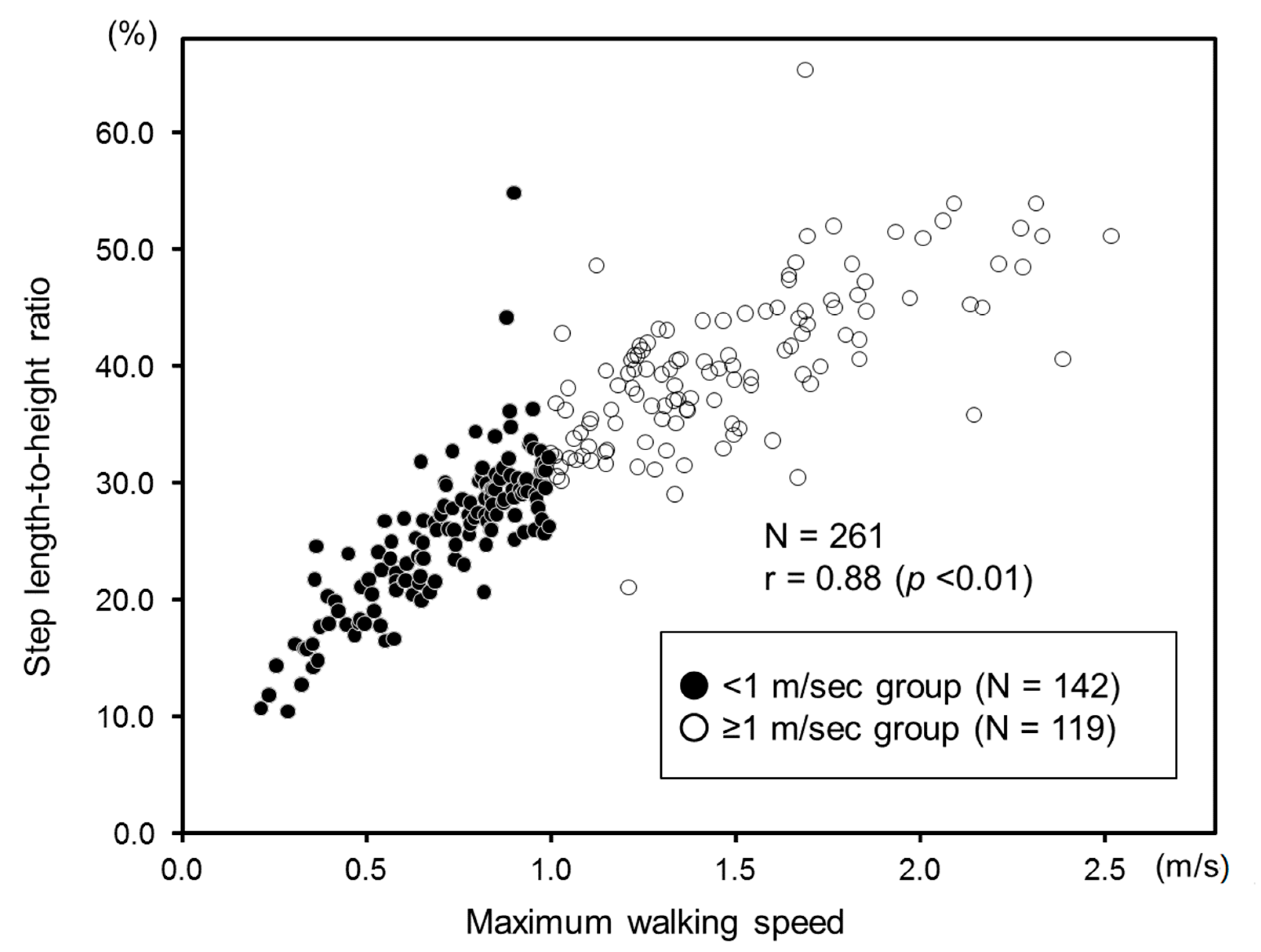
3. Results
3.1. Clinical Characteristics of the Patients
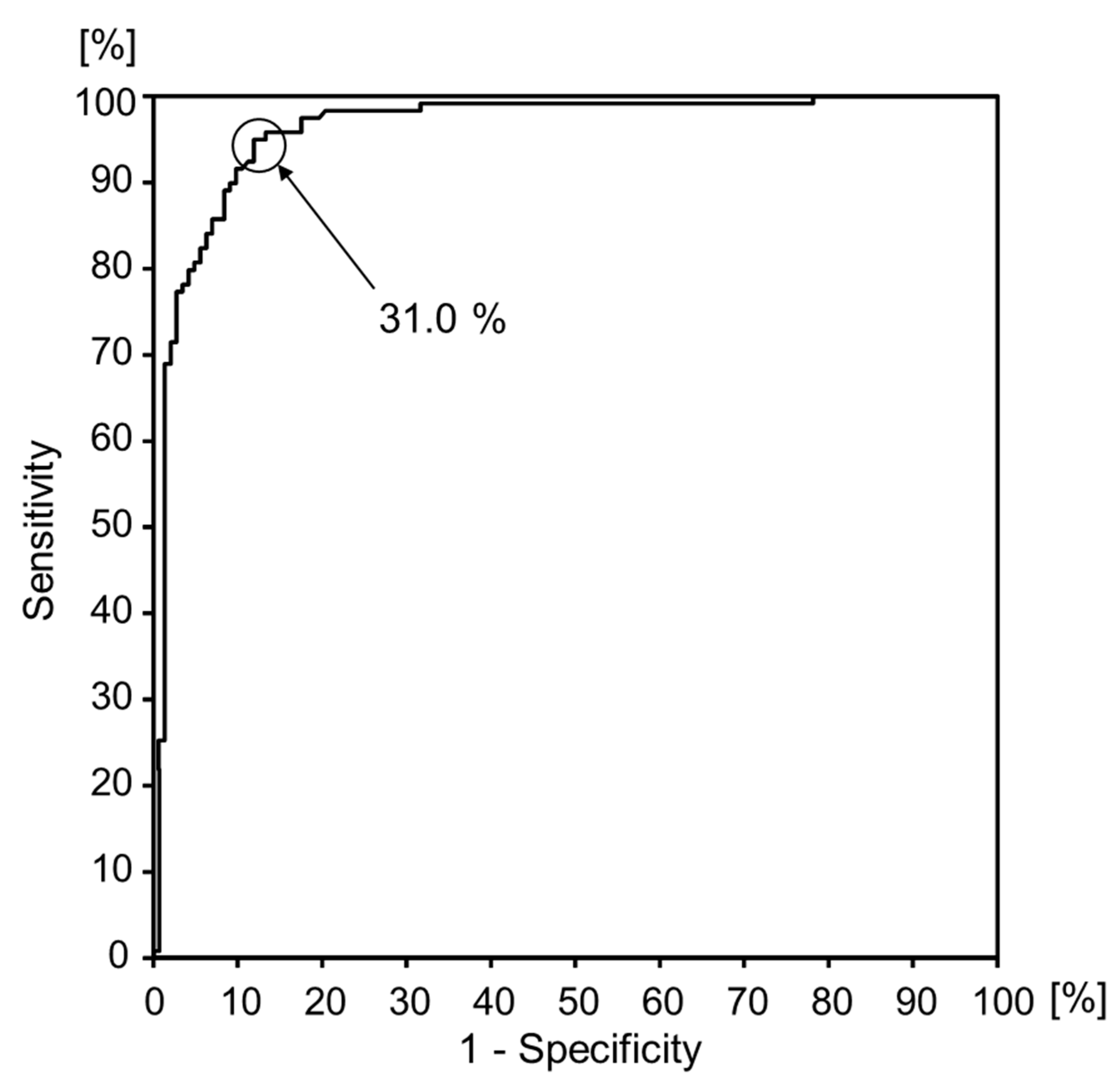
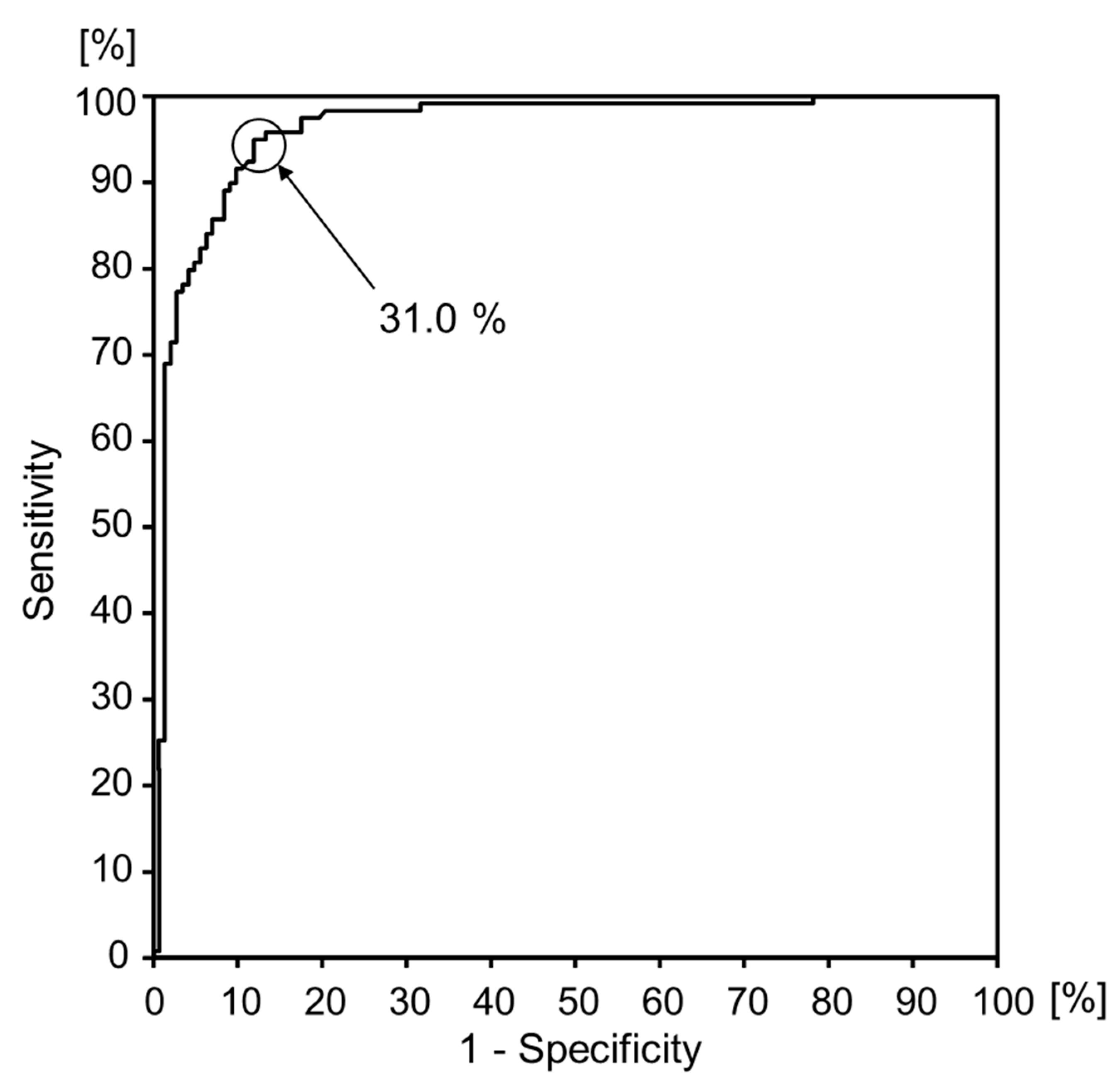
3.2. Risk Scores for Patients Able to Walk 1.0 m/s or Faster in the Maximum Walking Speed Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shumway-Cook, A.; Woolacott, M.H. Motor Control: Theory and Practical Applications; Williams & Wilkins: Baltimore, MD, USA, 1995. [Google Scholar]
- Guimaraes, R.M.; Isaacs, B. Characteristics of the gait in old people who fall. Int. Rehabil. Med. 1980, 2, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Kritchevsky, S.B.; Penninx, B.W.; Nicklas, B.J.; Simonsick, E.M.; Newman, A.B.; Tylavsky, F.A.; Brach, J.S.; Satterfield, S.; Bauer, D.C.; et al. Prognostic value of usual gait speed in well-functioning older people--results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2005, 53, 1675–1680. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Toriida, M.; Tayama, H. A study on the standard of gait evaluation: By an actual investigation of crosswalks. Rigaku. Ryoho. Gaku 1989, 16, 261–266, (In Japanese with English abstract). [Google Scholar]
- Bohannon, R.W. Comfortable and maximum walking speed of adults aged 20–79 years: Reference values and determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Nagasaki, H.; Maruyama, H.; Hashizume, K.; Nakamura, R. Age related changes of the walking cycle during fastest walking in healthy male subjects. Nihon. Ronen. Igakkai Zasshi 1989, 26, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J.; Thomas, S.S.; Higgins, C.; Colliver, J. Stride-dependent changes in gait of older people. J. Neurol. 1991, 238, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ostrosky, K.M.; VanSwearingen, J.M.; Burdett, R.G.; Gee, Z. A comparison of gait characteristics in young and old subjects. Phys. Ther. 1994, 74, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Takami, M.; Fukui, K. Force-plate study of normal walking. Japanese J. Rehabilitation Med. 1987, 24, 93–101, (In Japanese with English abstract). [Google Scholar] [CrossRef]
- Omori, Y.; Kasahara, Y.; Tateishi, M.; Kondo, C.; Matsushima, S.; Suzuki, T.; Tada, M.; Mogamiya, T.; Sasaki, S.; Sasa, M.; et al. Non-linear relationship between step length and lower extremity muscle strength in older male patients. Sogo Rehabilitation 2016, 44, 53–56. (In Japanese) [Google Scholar]
- Katoh, M.; Yamasaki, H. Test-retest reliability of isometric leg muscle strength measurements made using a hand-held dynamometer restrained by a belt: Comparisons during and between Sessions. J. Phys. Ther. Sci. 2009, 21, 239–243. [Google Scholar] [CrossRef]
- Morio, Y.; Omori, Y.; Izawa, K.P.; Tanaka, A.; Watanabe, S.; Beppu, M.; Kawama, K. The development of Functional Reach Test using the telescoping rod. Sogo Rehabilitation 2007, 35, 487–493. (In Japanese) [Google Scholar]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, 192–197. [Google Scholar] [CrossRef]
- Saito, T.; Izawa, K.P.; Watanabe, S. Association Between the Functional Independence and Difficulty Scale and Physical Functions in Community-Dwelling Japanese Older Adults Using Long-term Care Services. J. Geriatr. Phys. Ther. 2018, 41, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, M.; Morimoto, Y.; Kimura, M.; Fuchimoto, K.; Fuchimoto, T. A kinematic analysis of walking and physical fitness testing in elderly women. Can J. Sport Sci. 1991, 16, 223–228. [Google Scholar] [PubMed]
- Yamasaki, H.; Yokoyama, H.; Aoki, U.; Kurosawa, K.; Yamada, S.; Aoki, H.; Tanabe, K.; Osada, N. Relationship between muscle strength in knee extensors and gait speed, independent gait in the elderly patients. Sogo Rehabilitation 1998, 26, 689–692. (In Japanese) [Google Scholar]
- Rantanen, T.; Era, P.; Heikkinen, E. Maximal isometric strength and mobility among 75-year-old men and women. Age Ageing 1994, 23, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Omori, Y.; Yokoyama, H.; Terao, U.; Hiraki, K.; Kondo, M.; Kasahara, Y.; Yamasaki, H.; Sasa, M. The necessary value of isometric knee extension muscle force for road crossing in the old male patients. Sogo Rehabilitation 2005, 33, 1141–1144. (In Japanese) [Google Scholar]
- Yamade, H.; Takahashi, S.; Goto, Y. Examination of the efficient step of the paradoxical walking exercise in Parkinson’s disease. Rigakuryoho Kagaku 2012, 27, 529–533, (In Japanese with English abstract). [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | ≥1 m/s Group (N = 119) | <1 m/s Group (N = 142) | p Value |
|---|---|---|---|
| Age, years | 80.2 ± 4.9 | 82.8 ± 5.5 | <0.01 |
| Male/Female, N | 62/57 | 70/72 | 0.71 * |
| Height, cm | 155.8 ± 8.7 | 153.4 ± 9.4 | 0.03 |
| BMI, kg/m2 | 21.6 ± 2.9 | 19.9 ± 3.7 | <0.01 |
| Knee extension muscle force a, kgf/kg | 0.45 ± 0.15 | 0.29 ± 0.09 | <0.01 |
| M-FRT b (cm) | 32.9 ± 5.7 | 26.0 ± 5.0 | <0.01 |
| OLS (s) | 15.1 ± 18.0 | 2.0 ± 2.2 | <0.01 |
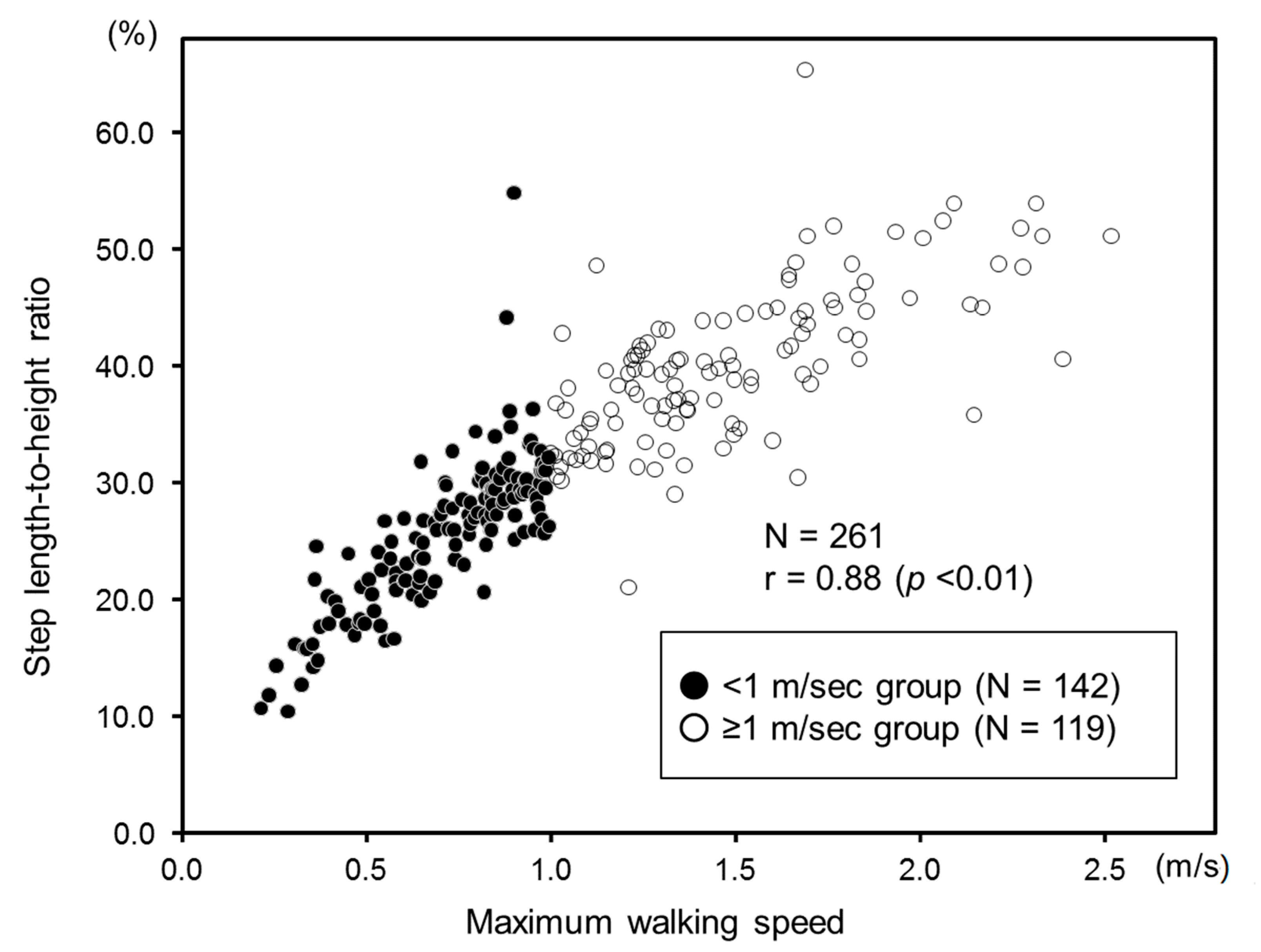
| Stride-to-height ratio (%) | 40.0 ± 6.7 | 25.7 ± 6.3 | <0.01 |
| Risk Scores for Patients | OR (95% CI) | p Value |
|---|---|---|
| Age (OR per 3 years) | 1.21 (0.89–1.63) | 0.23 |
| Height (OR per 3 cm) | 0.98 (0.85–1.14) | 0.83 |
| BMI (OR per 1 kg/m2) | 1.04 (0.92–1.17) | 0.51 |
| Knee extension muscle force a (OR per 0.03 kgf/kg) | 1.18 (1.01–1.37) | 0.03 |
| M-FRT b (OR per 3 cm) | 1.10 (0.80–1.52) | 0.56 |
| OLS (OR per 3 s) | 1.44 (0.95–2.18) | 0.08 |
| Stride-to-height ratio (OR per 3%) | 2.91 (2.03–4.15) | <0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morio, Y.; Izawa, K.P.; Omori, Y.; Katata, H.; Ishiyama, D.; Koyama, S.; Yamano, Y. The Relationship between Walking Speed and Step Length in Older Aged Patients. Diseases 2019, 7, 17. https://doi.org/10.3390/diseases7010017
Morio Y, Izawa KP, Omori Y, Katata H, Ishiyama D, Koyama S, Yamano Y. The Relationship between Walking Speed and Step Length in Older Aged Patients. Diseases. 2019; 7(1):17. https://doi.org/10.3390/diseases7010017
Chicago/Turabian StyleMorio, Yuji, Kazuhiro P. Izawa, Yoshitsugu Omori, Hironobu Katata, Daisuke Ishiyama, Shingo Koyama, and Yoshihisa Yamano. 2019. "The Relationship between Walking Speed and Step Length in Older Aged Patients" Diseases 7, no. 1: 17. https://doi.org/10.3390/diseases7010017
APA StyleMorio, Y., Izawa, K. P., Omori, Y., Katata, H., Ishiyama, D., Koyama, S., & Yamano, Y. (2019). The Relationship between Walking Speed and Step Length in Older Aged Patients. Diseases, 7(1), 17. https://doi.org/10.3390/diseases7010017