
Total Neoadjuvant Therapy, Organ Preservation and Beyond: A State-of-the-Art Systematic Review and Critical Appraisal of Locally Advanced Rectal Cancer Management

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Study Selection and Analytical Approach
2.3. Protocol Registration
2.4. Data Synthesis
3. Results
3.1. Risk of Bias Assessment, Study Selection, and Characteristics
3.1.1. Study Selection and Characteristics
3.1.2. Risk of Bias Assessment
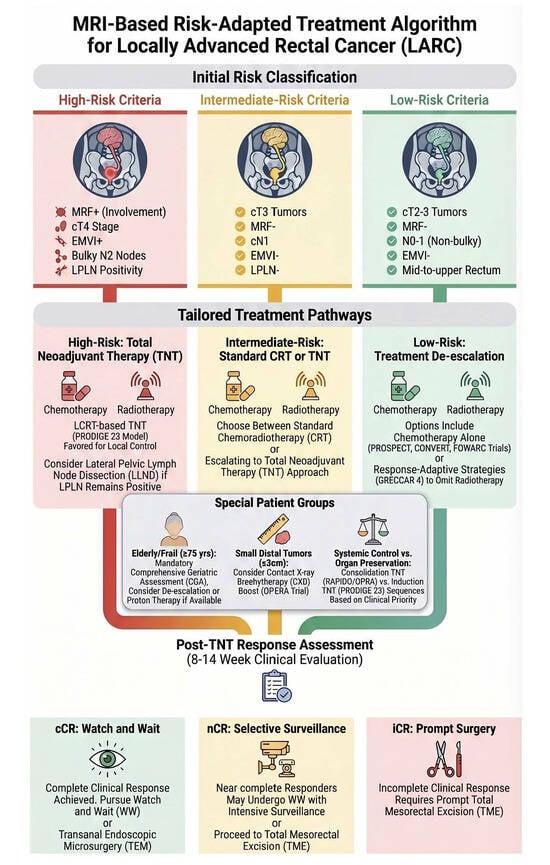
3.1.3. MRI-Based Risk Stratification: Defining Three Clinical Risk Groups
High-Risk Features (Indicate Need for TNT Intensification)
- Threatened or involved mesorectal fascia (MRF+): Tumour or lymph node within ≤1 mm of the mesorectal fascia. Associated with local failure rates > 20% after standard CRT alone.
- cT4 category:
- -
- T4a: tumour invades the visceral peritoneum (peritoneal reflection). High risk of peritoneal dissemination.
- -
- T4b: tumour directly invades adjacent organs (bladder, prostate, seminal vesicles, sacrum, vagina, pelvic sidewall). Very high risk of involved margins and local relapse.
- Extramural vascular invasion (EMVI+): Presence of tumour within veins outside the muscularis propria (serpentine appearance, expansion of vessel). Strongly associated with synchronous and metachronous distant metastases.
- Bulky N2 disease: Multiple regional lymph nodes (≥4) or large nodes (>10–15 mm) in the mesorectum. Indicates high tumour burden and risk of residual disease after CRT.
- LPLN+: Nodes in the internal iliac, obturator, or external iliac chains. Size ≥ 7 mm short axis, or ≥5 mm with malignant features (irregular border, mixed signal intensity, loss of fatty hilum). These nodes are not adequately treated by standard TME and may require lateral lymph node dissection (LLND) after TNT.
- Tumour deposits (TD+): Discrete macroscopic tumour nodules within the mesorectum lacking identifiable residual lymph node architecture. They are associated with a higher risk of local recurrence and distant metastases, independent of nodal status. Their presence should be systematically reported on baseline MRI and considered an indication for treatment intensification, including TNT.
- cT3 with clear MRF (>1 mm).
- cN1 (1–3 small nodes).
- No EMVI.
- No LPLN enlargement.
- TD−.
- cT2–3, MRF−, N0–1 (non-bulky), EMVI−, LPLN−.
- ∙ Mid-upper rectal location (≥5–10 cm from anal verge).
3.2. The Efficacy of Total Neoadjuvant Therapy: A Confirmed Benefit with a Critical Caveat
Baseline Heterogeneity Among TNT Trials: A Critical Comparison
- I.
- The absolute pCR rate (28% in RAPIDO vs. 27.5% in PRODIGE 23) appears similar, but the RAPIDO population was much higher risk. Therefore, the relative benefit of TNT over standard CRT may be greater in higher-risk patients.
- II.
- The increased locoregional recurrence seen in RAPIDO (10% vs. 6%) may be partly explained by the high-risk features (cT4, EMVI+), which are known to predispose to local failure, and by the use of SCRT instead of LCRT.
- III.
- De-escalation trials (PROSPECT, CONVERT, FOWARC) intentionally excluded many high-risk patients (e.g., cT4, MRF+), so their results cannot be generalized to the high-risk LARC population.
3.3. De-Escalation: The PROSPECT Trial and Beyond
3.4. Immunotherapy in MSS Disease: A Paradigm Shift in Waiting, Not Yet Realized
3.5. Organ Preservation: Proven Efficacy in Expert Centers, Questions of Generalizability
3.6. Predictive Factors and Risk Stratification: Informing Personalization and the Role of ctDNA
3.7. Toxicity, Compliance, and Patient-Reported Quality of Life
3.8. Technological Advances in Radiotherapy: MRI-LINAC and Adaptive Planning
3.9. Synthesis of Key Findings
4. Discussion
4.1. Implementation of Total Neoadjuvant Therapy
4.2. Organ Preservation Paradigm and MRI-Guided Selection
4.2.1. Organ Preservation
4.2.2. Integrating MRI into Clinical Decision-Making
4.3. Immunotherapy in MSS Disease: Investigational Only
4.4. Predictive Biomarkers and ctDNA-Guided Therapy: CINTS-R
4.5. Technological Advances in Radiotherapy: MRI-LINAC
4.6. Management of Specific Subgroups: LPLN+ and Elderly
4.7. Health Economics and Real-World Feasibility
4.8. Limitations, Clinical Implications and Future Directions
4.8.1. Review Limitations
4.8.2. Clinical Implications and Future Directions
4.8.3. Future Research Priorities
- (1)
- (2)
- ctDNA-guided therapy: The final results of the CINTS-R trial (2-year DrTF rate) will determine whether ctDNA-guided risk stratification should become standard practice.
- (3)
- Biomarker integration: Validation and clinical implementation of Immunoscore, ctDNA dynamics, and radiomic signatures are paramount.
- (4)
- Understanding and mitigating trade-offs: Further research is required to elucidate the mechanisms behind increased locoregional recurrence risk and optimize radiotherapy techniques.
- (5)
- Health economic analysis: Rigorous cost-effectiveness analyses of TNT, OP strategies, and novel technologies are essential.
- (6)
- Trials for specific subgroups: Dedicated prospective trials are required for elderly/frail patients and those with LPLN+.
- (7)
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Adj CT | Adjuvant Chemotherapy |
| AE | Adverse Event |
| APC | Article Processing Charge (cover letter only) |
| APR | Abdominoperineal Resection |
| ASCO | American Society of Clinical Oncology |
| AV | Anal Verge |
| CAP | College of American Pathologists (tumour regression grading) |
| CapeOX/CAPOX | Capecitabine + Oxaliplatin (chemotherapy regimen) |
| cCR | Clinical Complete Response |
| CEA | Carcinoembryonic Antigen |
| CGA | Comprehensive Geriatric Assessment |
| CI | Confidence Interval |
| CINTS-R | ctDNA-guided neoadjuvant treatment strategy for locally advanced rectal cancer (trial) |
| CNA | Copy Number Alteration |
| CR | Complete Response |
| CRM | Circumferential Resection Margin |
| CRT | Chemoradiotherapy/Chemoradiation |
| CT | Chemotherapy or Computed Tomography |
| ctDNA | Circulating Tumour DNA |
| CTV | Clinical Target Volume |
| CXB | Contact X-ray Brachytherapy |
| DFS | Disease-Free Survival |
| dMMR | Deficient Mismatch Repair |
| DrTF | Disease-related Treatment Failure |
| DWI | Diffusion-Weighted Imaging |
| EBRT | External Beam Radiotherapy |
| ECOG | Eastern Cooperative Oncology Group |
| eCRF | Electronic Case Report Form |
| EDC | Electronic Data Capture |
| ELAPE | Extralevator Abdominoperineal Excision |
| EMBASE | Excerpta Medica dataBASE |
| EMVI | Extramural Vascular Invasion |
| ERUS | Endorectal Ultrasound |
| ESMO | European Society for Medical Oncology |
| EUS | Endoscopic Ultrasound |
| FOLFIRINOX | Folinic acid, Fluorouracil, Irinotecan, Oxaliplatin |
| FOLFOX | Folinic acid, Fluorouracil, Oxaliplatin |
| G2/G3/G4 | Grade 2/Grade 3/Grade 4 (toxicity grading) |
| GI | Gastrointestinal |
| GTV | Gross Tumour Volume |
| Gy | Gray (unit of radiation dose) |
| HR | Hazard Ratio |
| ICI/ICIs | Immune Checkpoint Inhibitor(s) |
| ICR | Incomplete Response |
| IMRT | Intensity-Modulated Radiotherapy |
| irAE | Immune-related Adverse Event |
| ISR | Intersphincteric Resection |
| ITT | Intention-To-Treat |
| LARC | Locally Advanced Rectal Cancer |
| LARS | Low Anterior Resection Syndrome |
| LCRT | Long-Course Radiotherapy/Long-Course Chemoradiotherapy |
| LE | Local Excision |
| LLND | Lateral Lymph Node Dissection |
| LMIC | Low- and Middle-Income Countries |
| LoRP | Library of Reference Plans |
| LPLN | Lateral Pelvic Lymph Node(s) |
| LPLN+ | Lateral Pelvic Lymph Node-Positive |
| LPLN− | Lateral Pelvic Lymph Node-Negative |
| LR | Locoregional Recurrence |
| LRRFS | Locoregional Recurrence-Free Survival |
| MeSH | Medical Subject Headings |
| mFOLFOX6 | Modified FOLFOX regimen (6-drug variant) |
| MFS | Metastasis-Free Survival |
| MMR | Mismatch Repair |
| MPR | Major Pathological Response |
| MR | Magnetic Resonance |
| MRF | Mesorectal Fascia |
| MRF+ | Mesorectal Fascia Involvement/Positive |
| MRF− | Mesorectal Fascia Uninvolved/Negative |
| MRI | Magnetic Resonance Imaging |
| MRI-LINAC | Magnetic Resonance Imaging-guided Linear Accelerator |
| MSI-H | Microsatellite Instability-High |
| MSS | Microsatellite Stable |
| mITT | Modified Intention-To-Treat |
| N+ | Node-Positive |
| N0 | Node-Negative |
| NACRT | Neoadjuvant Chemoradiotherapy |
| NAR | Neoadjuvant Rectal (score) |
| NCCN | National Comprehensive Cancer Network |
| nCRT | Neoadjuvant Chemoradiotherapy |
| NCR | Near-Complete Response |
| nCT | Neoadjuvant Chemotherapy |
| NGS | Next-Generation Sequencing |
| NI | Non-Inferiority |
| NK | Natural Killer (cells) |
| NOM | Non-Operative Management |
| NS | Not Significant |
| OAR | Organ at Risk |
| OP | Organ Preservation |
| OPS | Organ Preservation Strategies |
| OR | Odds Ratio |
| OS | Overall Survival |
| pCR | Pathological Complete Response |
| PD-1 | Programmed Death-1 |
| PD-L1 | Programmed Death-Ligand 1 |
| PET/CT | Positron Emission Tomography/Computed Tomography |
| pMMR | Proficient Mismatch Repair |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PRO | Patient-Reported Outcome |
| PROSPERO | International Prospective Register of Systematic Reviews |
| PTV | Planning Target Volume |
| QALY | Quality-Adjusted Life Year |
| QLQ-C30 | Quality of Life Questionnaire—Core 30 (EORTC) |
| QoL | Quality of Life |
| RCT | Randomised Controlled Trial |
| RNA-seq | RNA Sequencing |
| RoB 2 | Revised Cochrane Risk of Bias tool for randomised trials (version 2) |
| RT | Radiotherapy |
| SAE | Serious Adverse Event |
| SBRT | Stereotactic Body Radiotherapy |
| SCRT | Short-Course Radiotherapy |
| scRNA-seq | Single-Cell RNA Sequencing |
| SIB | Simultaneous Integrated Boost |
| SNI | Selective Nodal Irradiation |
| SNV | Single-Nucleotide Variant |
| TaTME | Transanal Total Mesorectal Excision |
| TCGA | The Cancer Genome Atlas |
| TEM | Transanal Endoscopic Microsurgery |
| TIL | Tumour-Infiltrating Lymphocyte |
| TMB | Tumour Mutational Burden |
| TME | Total Mesorectal Excision |
| TNT | Total Neoadjuvant Therapy |
| TPS | Tumour Proportion Score |
| TRG | Tumour Regression Grade |
| VAF | Variant Allele Frequency |
| W&W | Watch-and-Wait |
| XELOX | Capecitabine + Oxaliplatin (same as CAPOX) |
| yp | Pathological stage after neoadjuvant therapy |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Heald, R.J.; Ryall, R.D. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986, 1, 1479–1482. [Google Scholar] [CrossRef]
- Kapiteijn, E.; Marijnen, C.A.; Nagtegaal, I.D.; Putter, H.; Steup, W.H.; Wiggers, T.; Rutten, H.J.; Pahlman, L.; Glimelius, B.; Van Krieken, J.H.; et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N. Engl. J. Med. 2001, 345, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Bosset, J.-F.; Collette, L.; Calais, G.; Mineur, L.; Maingon, P.; Radosevic-Jelic, L.; Daban, A.; Bardet, E.; Beny, A.; Ollier, J.-C.; et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N. Engl. J. Med. 2006, 355, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Erlandsson, J.; Holm, T.; Pettersson, D.; Berglund, A.; Cedermark, B.; Radu, C.; Johansson, H.; Machado, M.; Hjern, F.; Hallböök, O.; et al. Optimal fractionation of preoperative radiotherapy and timing to surgery for rectal cancer (Stockholm III): A multicentre, randomised, non-blinded, phase 3, non-inferiority trial. Lancet Oncol. 2017, 18, 336–346. [Google Scholar] [CrossRef]
- Rödel, C.; Graeven, U.; Fietkau, R.; Hohenberger, W.; Hothorn, T.; Arnold, D.; Hofheinz, R.-D.; Ghadimi, M.; Wolff, H.A.; Lang-Welzenbach, M.; et al. Oxaliplatin added to fluorouracil-based preoperative chemoradiotherapy and postoperative chemotherapy of locally advanced rectal cancer (the German CAO/ARO/AIO-04 study): Final results of the multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2015, 16, 979–989. [Google Scholar] [CrossRef]
- Cercek, A.; Roxburgh, C.S.; Strombom, P.; Smith, J.J.; Temple, L.K.; Nash, G.M.; Guillem, J.G.; Paty, P.B.; Yaeger, R.; Stadler, Z.K.; et al. Adoption of Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer. JAMA Oncol. 2018, 4, e180071. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rutten, H.J.; Dulk, M.D.; Lemmens, V.E.; van de Velde, C.J.; Marijnen, C.A. Controversies of total mesorectal excision for rectal cancer in elderly patients. Lancet Oncol. 2008, 9, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Beets-Tan, R.G.; Lambregts, D.M.; Lammering, G.; Nelemans, P.J.; Engelen, S.M.; van Dam, R.M.; Jansen, R.L.; Sosef, M.; Leijtens, J.W.; et al. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J. Clin. Oncol. 2011, 29, 4633–4640. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42, Erratum in Lancet Oncol. 2021, 22, e42. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Bosset, J.-F.; Etienne, P.-L.; Rio, E.; François, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Tang, Y.; Hu, C.; Jiang, L.-M.; Jiang, J.; Li, N.; Liu, W.-Y.; Chen, S.-L.; Li, S.; Lu, N.-N.; et al. Multicenter, Randomized, Phase III Trial of Short-Term Radiotherapy Plus Chemotherapy Versus Long-Term Chemoradiotherapy in Locally Advanced Rectal Cancer (STELLAR). J. Clin. Oncol. 2022, 40, 1681–1692. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, X.; Liu, P.; Xiao, Y.; Meng, W.; Tang, Y.; Zhou, J.; Ding, P.R.; Ding, K.F.; Wang, B.; Guo, Q.; et al. Total neoadjuvant treatment with long-course radiotherapy versus concurrent chemoradiotherapy in local advanced rectal cancer with high risk factors (TNTCRT): A multicenter, randomized, open-label, phase 3 trial. J. Clin. Oncol. 2024, 42, LBA3511. [Google Scholar] [CrossRef]
- Garcia-Aguilar, J.; Patil, S.; Gollub, M.J.; Kim, J.K.; Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Omer, D.M.; Lee, M.; Dunne, R.F.; et al. Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gerard, J.-P.; Barbet, N.; Schiappa, R.; Magné, N.; Martel, I.; Mineur, L.; Deberne, M.; Zilli, T.; Dhadda, A.; Myint, A.S. Neoadjuvant chemoradiotherapy with radiation dose escalation with contact x-ray brachytherapy boost or external beam radiotherapy boost for organ preservation in early cT2-cT3 rectal adenocarcinoma (OPERA): A phase 3, randomised controlled trial. Lancet Gastroenterol. Hepatol. 2023, 8, 356–367. [Google Scholar] [CrossRef] [PubMed]
- Glimelius, B.; Khan, T.; Adolfsson, K.; Angenete, E.; Berglund, Å.; Bonde, K.; Elander, N.; Fokstuen, T.; Haux, J.; Imam, I.; et al. Total neoadjuvant treatment using short-course radiotherapy and four CAPOX cycles in locally advanced rectal cancer with high-risk criteria for recurrence: A Swedish nationwide cohort study (LARCT-US). eClinicalMedicine 2024, 75, 102771. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lin, Z.; Zhang, P.; Chi, P.; Xiao, Y.; Xu, X.; Zhang, A.; Qiu, X.; Wu, J.; Yuan, Y.; Wang, Z.; et al. Neoadjuvant short-course radiotherapy followed by camrelizumab and chemotherapy in locally advanced rectal cancer (UNION): Early outcomes of a multicenter randomized phase III trial. Ann. Oncol. 2024, 35, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Shamseddine, A.; Turfa, R.; Chehade, L.; Zeidan, Y.H.; El Husseini, Z.; Kreidieh, M.; Bouferraa, Y.; Elias, C.; Kattan, J.; Khalifeh, I.; et al. Short-course radiation followed by mFOLFOX-6 plus avelumab for locally-advanced microsatellite stable rectal adenocarcinoma: The Averectal study. Eur. J. Cancer 2025, 222, 115428. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Li, H.-Y.; Wei, L.-C.; Li, N.; Zhang, W.-J.; Lu, Y.-F.; Deng, F.-Y.; Xu, T.-Z.; Shuai, J.-C.; Lei, Z.-F.; et al. Short-course-based TNT with or without PD-1 inhibitor for pMMR locally advanced rectal cancer: Phase 2 results of a randomized trial (STELLAR II). Med 2025, 6, 100807. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Dai, H.; Sha, D.; Yu, Y.; Jing, H.; Sun, C.; Shang, L.; Liu, Y.; Feng, R.; Li, J.; et al. Total neoadjuvant treatment with short-course radiotherapy followed by sintilimab plus capecitabine-oxaliplatin versus short-course radiotherapy followed by capecitabine-oxaliplatin in patients with locally advanced rectal cancer (SPRING-01): A single-centre, open-label, phase 2, randomised controlled trial. Lancet 2025, 26, 1043–1054. [Google Scholar]
- Wang, F.; Lai, C.; Lv, Y.; Zhang, F.; Shi, L.; Wang, Y.; Shen, Y.; Xu, L.; Hu, P.; Tang, W.; et al. Efficacy and safety of combining short-course neoadjuvant chemoradiotherapy with enzalofilimab in locally advanced rectal cancer patients with microsatellite stability: A phase II PRECAM experimental study. Int. J. Surg. 2024, 111, 334–345. [Google Scholar] [CrossRef]
- Pedone, C.; Sorcini, B.; Staff, C.; Färlin, J.; Fokstuen, T.; Frödin, J.-E.; Nilsson, P.J.; Martling, A.; Valdman, A. Preoperative short-course radiation therapy with PROtons compared to photons in high-risk RECTal cancer (PRORECT): Initial dosimetric experience. Clin. Transl. Radiat. Oncol. 2022, 39, 100562. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meyer, J.; Koessler, T. Comment on: A phase III randomised trial on the addition of a contact X-ray brachytherapy boost to standard neoadjuvant chemo-radiotherapy for organ preservation in early rectal adenocarcinoma: 5 year results of the OPERA trial. Ann. Oncol. 2025, 36, 601. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhang, X.; Liu, Q.; Li, Y.; Wu, G.; Fu, W.; Yao, H.; Wang, Z.; Xue, H.; Xu, T.; et al. Rationale and design of a multicentre randomised controlled trial on circulating tumour DNA-guided neoadjuvant treatment strategy for locally advanced rectal cancer (CINTS-R). BMJ Open 2025, 15, e090765. [Google Scholar] [CrossRef]
- Zhang, X.; Zhou, J.; Geng, J.; Li, Y.; Huang, F.; Shu, W.; Fu, W.; Zhou, X.; Wu, G.; Jia, W.; et al. Feasibility of ctDNA-guided precision neoadjuvant therapy in locally advanced rectal cancer: Insights from the ongoing CINTS-R trial. Eur. J. Cancer 2025, 234, 116193. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Azad, N.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Garrido-Laguna, I.; et al. Rectal Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 1139–1167. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-N.; Jiang, J.; Jiang, L.-M.; Zhou, H.-T.; Li, N.; Lu, N.-N.; Gao, Y.-H.; Liu, S.-X.; Wang, W.-L.; Wei, L.-C.; et al. Post-hoc analysis of clinicopathological factors affecting lateral lymph node metastasis based on STELLAR study for rectal cancer. Radiother. Oncol. 2024, 200, 110512. [Google Scholar] [CrossRef] [PubMed]
- Manceau, G.; Karoui, M.; Werner, A.; Mortensen, N.J.; Hannoun, L. Comparative outcomes of rectal cancer surgery between elderly and non-elderly patients: A systematic review. Lancet Oncol. 2012, 13, e525–e536. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Zhou, J.; Qiu, H.; Shen, Z.; Wu, B.; Jia, W.; Niu, B.; Li, F.; Yao, H.; Wu, A.; et al. A new treatment strategy for mid-low rectal cancer patients exhibiting a clinical complete or near-complete response to neoadjuvant chemoradiotherapy: Transanal endoscopic microsurgery—A multicenter prospective case-control clinical trial by MONT-R. Eur. J. Cancer 2025, 216, 115156. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, G.; Jia, W.; Xiao, Y.; Wu, A.; Wu, B.; Wang, Z.; Liu, Q.; Yao, H.; Li, F.; et al. CapeOX Versus Capecitabine in Neoadjuvant Chemoradiation for High-Risk Locally Advanced Rectal Cancer: Long-Term Results from MONT-R Randomized Controlled Trial. Int. J. Radiat. Oncol. Biol. Phys. 2025, 125, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Hofheinz, R.-D.; Wenz, F.; Post, S.; Matzdorff, A.; Laechelt, S.; Hartmann, J.T.; Müller, L.; Link, H.; Moehler, M.; Kettner, E.; et al. Chemoradiotherapy with capecitabine versus fluorouracil for locally advanced rectal cancer: A randomised, multicentre, non-inferiority, phase 3 trial. Lancet Oncol. 2012, 13, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Pedersen, K.; Olsen, J.R.; Mutch, M.G.; Chin, R.-I.; Glasgow, S.C.; Wise, P.E.; Silviera, M.L.; Tan, B.R.; Wang-Gillam, A.; et al. Nonoperative Rectal Cancer Management with Short-Course Radiation Followed by Chemotherapy: A Nonrandomized Control Trial. Clin. Color. Cancer 2021, 20, e185–e193. [Google Scholar] [CrossRef] [PubMed]
- Markovina, S.; Youssef, F.; Roy, A.; Aggarwal, S.; Khwaja, S.; DeWees, T.; Tan, B.; Hunt, S.; Myerson, R.J.; Chang, D.T.; et al. Improved Metastasis- and Disease-Free Survival with Preoperative Sequential Short-Course Radiation Therapy and FOLFOX Chemotherapy for Rectal Cancer Compared with Neoadjuvant Long-Course Chemoradiotherapy: Results of a Matched Pair Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Ngan, S.Y.; Burmeister, B.; Fisher, R.J.; Solomon, M.; Goldstein, D.; Joseph, D.; Ackland, S.P.; Schache, D.; McClure, B.; McLachlan, S.-A.; et al. Randomized trial of short-course radiotherapy versus long-course chemoradiation comparing rates of local recurrence in patients with T3 rectal cancer: Trans-Tasman Radiation Oncology Group trial 01.04. J. Clin. Oncol. 2012, 30, 3827–3833, Erratum in J. Clin. Oncol. 2013, 31, 399. [Google Scholar] [CrossRef] [PubMed]
- Sauer, R.; Liersch, T.; Merkel, S.; Fietkau, R.; Hohenberger, W.; Hess, C.; Becker, H.; Raab, H.-R.; Villanueva, M.-T.; Witzigmann, H.; et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J. Clin. Oncol. 2012, 30, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Castan, F.; Etienne, P.-L.; Rio, E.; Mesgouez-Nebout, N.; Evesque, L.; Vendrely, V.; Artignan, X.; Bouché, O.; Gargot, D.; et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiotherapy in patients with locally advanced rectal cancer: Long-term results of the UNICANCER-PRODIGE 23 trial. Ann. Oncol. 2024, 35, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Zwart, W.H.; Temmink, S.J.; Hospers, G.A.; Marijnen, C.A.; Putter, H.; Nagtegaal, I.D.; Blomqvist, L.; Kranenbarg, E.M.-K.; Roodvoets, A.G.; Martling, A.; et al. Oncological outcomes after a pathological complete response following total neoadjuvant therapy or chemoradiotherapy for high-risk locally advanced rectal cancer in the RAPIDO trial. Eur. J. Cancer 2024, 204, 114044. [Google Scholar] [CrossRef] [PubMed]
- Ciseł, B.; Pietrzak, L.; Michalski, W.; Wyrwicz, L.; Rutkowski, A.; Kosakowska, E.; Cencelewicz, A.; Spałek, M.; Polkowski, W.; Jankiewicz, M.; et al. 5 × 5 Gy and consolidation chemotherapy for clinical T4 and fixed clinical T3 rectal cancer: Long-term results of the randomized Polish II study. Ann. Oncol. 2019, 30, 1298–1303. [Google Scholar] [CrossRef]
- Schrag, D.; Shi, Q.; Weiser, M.R.; Gollub, M.J.; Saltz, L.B.; Musher, B.L.; Goldberg, J.; Al Baghdadi, T.; Goodman, K.A.; McWilliams, R.R.; et al. Preoperative Treatment of Locally Advanced Rectal Cancer. N. Engl. J. Med. 2023, 389, 322–334. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mei, W.-J.; Wang, X.-Z.; Zhang, X.; Sun, Y.-M.; Yang, C.-K.; Lin, J.-Z.; Wu, Z.-G.; Zhang, R.; Wang, W.; Li, Y.; et al. Neoadjuvant Chemotherapy with CAPOX Versus Chemoradiation for Locally Advanced Rectal Cancer with Uninvolved Mesorectal Fascia (CONVERT): Final Results of a Phase III Trial. J. Clin. Oncol. 2026, 44, 970–980. [Google Scholar] [CrossRef]
- Rouanet, P.; Rullier, E.; Lelong, B.; Maingon, P.; Tuech, J.-J.; Pezet, D.; Castan, F.; Nougaret, S.; GRECCAR Study Group. Tailored Strategy for Locally Advanced Rectal Carcinoma (GRECCAR 4): Long-term Results from a Multicenter, Randomized, Open-Label, Phase II Trial. Dis. Colon Rectum 2022, 65, 986–995. [Google Scholar] [CrossRef]
- Verheij, F.S.; Omer, D.M.; Williams, H.; Lin, S.T.; Qin, L.-X.; Buckley, J.T.; Thompson, H.M.; Yuval, J.B.; Kim, J.K.; Dunne, R.F.; et al. Long-Term Results of Organ Preservation in Patients with Rectal Adenocarcinoma Treated with Total Neoadjuvant Therapy: The Randomized Phase II OPRA Trial. J. Clin. Oncol. 2024, 42, 500–506. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Williams, H.; Thompson, H.M.; Lin, S.T.; Verheij, F.S.; Omer, D.M.; Qin, L.-X.; Garcia-Aguilar, J.; On Behalf of the OPRA Consortium. Endoscopic Predictors of Residual Tumor After Total Neoadjuvant Therapy: A Post Hoc Analysis from the Organ Preservation in Rectal Adenocarcinoma Trial. Dis. Colon Rectum 2024, 67, 369–376. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dijkstra, E.A.; Hospers, G.A.; Kranenbarg, E.M.-K.; Fleer, J.; Roodvoets, A.G.; Bahadoer, R.R.; Guren, M.G.; Tjalma, J.J.; Putter, H.; Crolla, R.M.; et al. Quality of life and late toxicity after short-course radiotherapy followed by chemotherapy or chemoradiotherapy for locally advanced rectal cancer—The RAPIDO trial. Radiother. Oncol. 2022, 171, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Fokas, E.; Allgäuer, M.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.-L.; et al. Randomized Phase II Trial of Chemoradiotherapy Plus Induction or Consolidation Chemotherapy as Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer: CAO/ARO/AIO-12. J. Clin. Oncol. 2019, 37, 3212–3222. [Google Scholar] [CrossRef] [PubMed]
- Shamseddine, A.; Zeidan, Y.; Khalifeh, I.M.; Kattan, J.G.; Turfa, R.; Mukherji, D.; Temraz, S.N.; Jamali, F.; Shaib, Y.H.; Soweid, A.; et al. Short-course radiation followed by mFOLFOX-6 plus avelumab for locally advanced rectal adenocarcinoma. J. Clin. Oncol. 2020, 38, 139. [Google Scholar] [CrossRef]
- George, T.J.; Yothers, G.; Rahma, O.E.; Hong, T.S.; Russell, M.M.; You, Y.N.; Parker, W.; Jacobs, S.A.; Lucas, P.C.; Colangelo, L.H.; et al. Long-term results from NRG-GI002: A phase II clinical trial platform using total neoadjuvant therapy (TNT) in locally advanced rectal cancer (LARC). J. Clin. Oncol. 2023, 41, 7. [Google Scholar] [CrossRef]
- Gani, C.; Fokas, E.; Polat, B.; Ott, O.J.; Diefenhardt, M.; Königsrainer, A.; Böke, S.; Kirschniak, A.; Bachmann, R.; Wichmann, D.; et al. Organ preservation after total neoadjuvant therapy for locally advanced rectal cancer (CAO/ARO/AIO-16): An open-label, multicentre, single-arm, phase 2 trial. Lancet Gastroenterol. Hepatol. 2025, 10, 562–572. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chi, P.; Shi, L.; Cui, L.; Gao, J.; Li, W.; Wei, H.; Cheng, L.; Huang, Z.; Cai, G.; et al. Neoadjuvant Modified Infusional Fluorouracil, Leucovorin, and Oxaliplatin with or Without Radiation Versus Fluorouracil Plus Radiation for Locally Advanced Rectal Cancer: Updated Results of the FOWARC Study After a Median Follow-Up of 10 Years. J. Clin. Oncol. 2024, 43, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Xia, F.; Wang, Y.; Wang, H.; Shen, L.; Xiang, Z.; Zhao, Y.; Zhang, H.; Wan, J.; Zhang, H.; Wang, Y.; et al. Randomized Phase II Trial of Immunotherapy-Based Total Neoadjuvant Therapy for Proficient Mismatch Repair or Microsatellite Stable Locally Advanced Rectal Cancer (TORCH). J. Clin. Oncol. 2024, 42, 3308–3318. [Google Scholar] [CrossRef]
- Akiyoshi, T.; Shinozaki, E.; Taguchi, S.; Chino, A.; Hiratsuka, M.; Tominaga, T.; Nonaka, T.; Toda, S.; Matoba, S.; Matsui, S.; et al. Non-operative management after chemoradiotherapy plus consolidation or sandwich (induction with bevacizumab and consolidation) chemotherapy in patients with locally advanced rectal cancer: A multicentre, randomised phase II trial (NOMINATE trial). BMJ Open 2022, 12, e055140. [Google Scholar] [CrossRef]
- Ruppert, R.; Junginger, T.; Kube, R.; Strassburg, J.; Lewin, A.; Baral, J.; Maurer, C.A.; Sauer, J.; Lauscher, J.; Winde, G.; et al. Risk-Adapted Neoadjuvant Chemoradiotherapy in Rectal Cancer: Final Report of the OCUM Study. J. Clin. Oncol. 2023, 41, 4025–4034. [Google Scholar] [CrossRef]
- Taylor, F.G.; Quirke, P.; Heald, R.J.; Moran, B.J.; Blomqvist, L.; Swift, I.R.; Sebag-Montefiore, D.; Tekkis, P.; Brown, G. Preoperative magnetic resonance imaging assessment of circumferential resection margin predicts disease-free survival and local recurrence: 5-year follow-up results of the MERCURY study. J. Clin. Oncol. 2014, 32, 34–43. [Google Scholar] [CrossRef]
- Yang, L.; Cui, X.; Wu, F.; Chi, Z.; Xiao, L.; Wang, X.; Liang, Z.; Li, X.; Yu, Q.; Lin, X.; et al. The efficacy and safety of neoadjuvant chemoradiotherapy combined with immunotherapy for locally advanced rectal cancer patients: A systematic review. Front. Immunol. 2024, 15, 1392499. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, L.; Meng, X.; Wu, Q.; Wei, Y.; Liang, S.; Su, T. Comparative efficacy of neoadjuvant short-course versus long-course radiotherapy-based regimens with or without immunotherapy for locally advanced pMMR rectal cancer: A systematic review and network meta-analysis. BMC Med. 2026, 24, 258. [Google Scholar] [CrossRef]
- Bascoul-Mollevi, C.; Gourgou, S.; Borg, C.; Etienne, P.-L.; Rio, E.; Rullier, E.; Juzyna, B.; Castan, F.; Conroy, T. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER PRODIGE 23): Health-related quality of life longitudinal analysis. Eur. J. Cancer 2023, 186, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Li, H.; Xu, T.; Shi, J.; Shuai, J.; Liu, S.; Wang, W.; Zhu, Y.; Wei, L.; Cai, Y.; et al. Quality of Life and Functional Outcomes in Patients with Locally Advanced Rectal Cancer Receiving Total Neoadjuvant Therapy Versus Concurrent Chemoradiation Therapy: An Analysis of the STELLAR Trial. Int. J. Radiat. Oncol. Biol. Phys. 2025, 122, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Yang, X.; Qin, S.; Li, X.; Dai, J.; Tang, Y.; Men, K. Efficient strategy for magnetic resonance image-guided adaptive radiotherapy of rectal cancer using a library of reference plans. Phys. Imaging Radiat. Oncol. 2025, 33, 100747. [Google Scholar] [CrossRef]
- Bujko, K.; Wyrwicz, L.; Rutkowski, A.; Malinowska, M.; Pietrzak, L.; Kryński, J.; Michalski, W.; Olędzki, J.; Kuśnierz, J.; Zając, L.; et al. Long-course oxaliplatin-based preoperative chemoradiation versus 5 × 5 Gy and consolidation chemotherapy for cT4 or fixed cT3 rectal cancer: Results of a randomized phase III study. Ann. Oncol. 2016, 27, 834–842. [Google Scholar] [CrossRef] [PubMed]
- El Sissy, C.; Kirilovsky, A.; Eynde, M.V.D.; Muşină, A.-M.; Anitei, M.-G.; Romero, A.M.S.; Marliot, F.; Junca, A.; Doyen, J.; Mlecnik, B.; et al. A Diagnostic Biopsy-Adapted Immunoscore Predicts Response to Neoadjuvant Treatment and Selects Patients with Rectal Cancer Eligible for a Watch-and-Wait Strategy. Clin. Cancer Res. 2020, 26, 5198–5207. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial/Analysis (Primary Publication) | Phase | Sample Size | Control Arm | Experimental Arm | Primary Endpoint(s) |
|---|---|---|---|---|---|
| Historical Standard Treatment | |||||
| CAO/ARO/AIO-94 [4] | III | 823 | Postop CRT | Preop CRT | OS |
| EORTC 22921 [5] | III | 1011 | Preop RT alone | Preop CRT → ±Adj CT | OS, DFS |
| Stockholm III [6] | III | 550 | SCRT (5 × 5 Gy) with immediate surgery | SCRT with delayed surgery (4–8 weeks) | Local recurrence, survival |
| CAO/ARO/AIO-04 [7] | III | 1265 | 5-FU + LCRT | 5-FU + oxaliplatin + LCRT | 3-year DFS |
| Landmark Phase III TNT Trials | |||||
| RAPIDO [11,38] | III | 920 | LCRT → TME (±Adj CT) | SCRT → CT (CAPOX/FOLFOX) → TME | 3-year DrTF |
| PRODIGE 23 [12,37] | III | 461 | LCRT → TME → Adj CT | 6× FOLFIRINOX → LCRT → TME → 6× mFOLFOX6 | 3-year DFS |
| STELLAR [13] | III | 599 | LCRT → TME → 6× CAPOX | SCRT → 4× CAPOX → TME → 2× CAPOX | 3-year DFS |
| TNTCRT [14] | III | 458 | LCRT + capecitabine → TME → Adj CAPOX | LCRT + 6× CAPOX (1 ind, 2 conc, 3 cons) → TME | 3-year DFS |
| Polish II long-term [39] | III | 515 | LCRT + oxaliplatin | SCRT + 3× FOLFOX4 → TME | OS, DFS, local failure |
| Neoadjuvant Chemotherapy Without Routine RT (De-escalation) | |||||
| PROSPECT [40] | III | 1194 | LCRT (5.5 weeks) → TME | mFOLFOX6 (6 cycles) → TME (± selective LCRT) | 5-year DFS (NI) |
| CONVERT [41] | III | 663 | LCRT + capecitabine → TME | 4× CAPOX → TME | 3-year LRRFS (NI) |
| GRECCAR 4 [42] | II | 148 | Response-adaptive (induction CT → good responders → surgery; poor responders → CRT) | - | pCR, OP rate |
| Immunotherapy-TNT Trials | |||||
| UNION [18] | III | 231 | LCRT → 2× CAPOX → TME → 6× CAPOX | SCRT → 2× CAPOX + Camrelizumab → TME → 6× CAPOX + Camrelizumab | pCR |
| STELLAR II [20] | II | 218 | SCRT → 4× CAPOX → TME/WW → 2× CAPOX | SCRT → 4× CAPOX + Sintilimab → TME/WW → 2× CAPOX + Sintilimab | CR rate |
| SPRING-01 [21] | II | 98 | SCRT → 6× CAPOX → TME | SCRT → 6× CAPOX + Sintilimab → TME | pCR |
| PRECAM [22] | II | 34 | (single-arm) | SCRT → 2× CAPEOX + 6× Enzalofilimab → TME | pCR |
| Organ Preservation and Sequencing | |||||
| OPRA [15] | II | 324 | Induction: CRT → TME/WW | Consolidation: CRT → TME/WW | 3-year DFS; OP |
| OPERA [16] | III | 148 | LCRT + EBRT Boost → TME/LE/WW | LCRT + CXB Boost → TME/LE/WW | 3-year OP rate |
| MONT-R TEM [30,31] | Prospective case–control | 80 | Radical surgery (TME) | TEM local excision (cCR/near-cCR) | 5-year DFS |
| Predictive Factor and Subgroup Analyses | |||||
| OPRA Response Grade [43,44] | Post hoc | 324 | Analysis correlating 3-tier response with outcomes | - | OP and DFS by CCR/NCR/ICR |
| STELLAR LPLN Analysis [28] | Post hoc | 599 | Subgroup analysis of LPLN+ patients | - | Outcomes in LPLN+ |
| RAPIDO pCR Analysis [45] | Post hoc | 920 | Analysis of factors associated with pCR | - | Factors for pCR; prognosis of pCR |
| CINTS-R [25,26] | III RCT | 470 (planned) | Conventional nCRT | ctDNA-guided: high-risk → TNT; low-risk → nCRT; dMMR/TMB-H → immunotherapy | 2-year DrTF |
| Radiotherapy Modality | |||||
| PRORECT [23] | Dosimetric | 128 (plan) | Photon CRT | Proton CRT | Dosimetric comparison; predicted acute ≥ G2 GI toxicity |
| MRI-LINAC LoRP [46] | Retrospective | 10 pts (50 fractions) | Conventional couch shift/fully adaptive | Library of reference plans (LoRP) | Target coverage, treatment time |
| Other Key Trials | |||||
| Averectal [19,47] | II | 44 | Single-arm: SCRT → 6× mFOLFOX-6 + Avelumab → TME | - | pCR vs. historical |
| NRG-GI002 [48] | II platform | 178 (EA1), 185 (EA2) | FOLFOX → CRT → TME | EA2: + Pembrolizumab during CRT | NAR score reduction |
| CAO/ARO/AIO-16 [49] | II | 91 | Single-arm: CRT → 3× FOLFOX → Response → TME/WW | - | CCR rate |
| CAO/ARO/AIO-12 [46] | II | 306 | Induction FOLFOX → CRT → TME | CRT → Consolidation FOLFOX → TME | pCR rate |
| FOWARC 10-year [50] | III | 495 | 5-FU + LCRT | mFOLFOX6 ± LCRT | 10-year DFS |
| TORCH [51] | II | 130 (planned) | ICI before vs. after SCRT | ICI after SCRT | CR |
| NORMAL-R [33] | II | 19 | SCRT → CT → non-operative for CCR | - | cCR at 1 year |
| NOMINATE [52] | II | 66 (planned) | CRT → 6× CapeOx | 3× CapeOx + Bev → CRT → 3× CapeOx | pCR/CCR ≥ 2 years |
| OCUM [53] | Prospective | 1099 | Upfront TME (mrMRF−, low-risk) | nCRT → TME (mrMRF+ and/or cT4 and/or lower third cT3, high-risk) | 5-year LR rate |
| Trial/Analysis | Primary Efficacy Endpoint | pCR/cCR Rate | Key Efficacy Insights |
|---|---|---|---|
| RAPIDO [11] | 3-year DrTF: 23.7% vs. 30.4% * | 28% vs. 14% * | TNT reduced distant metastases (20.0% vs. 26.8%) and improved DrTF. |
| PRODIGE 23 [12] | 7-year DFS: 67.6% vs. 62.5%; 7-year OS: 81.9% vs. 76.1% | 28% vs. 12% * | TNT improved DFS, reduced distant metastases (17.8% vs. 25.5%), and showed OS benefit. |
| STELLAR [28] | 3-year DFS: 64.5% vs. 62.3% (NI) | 21.8% vs. 12.3% * | SCRT-based TNT was non-inferior to LCRT-based therapy. |
| TNTCRT [14] | 3-year DFS: 77.0% vs. 67.9% * (HR 0.623); 3-year MFS: 83.0% vs. 74.2% * | 27.5% vs. 9.9% * | LCRT-based TNT with CAPOX significantly improved DFS, MFS, and pCR. |
| PROSPECT [40] | 5-year DFS: 80.8% vs. 81.7% (NI) | 21.4% vs. 24.0% (NS) | FOLFOX with selective LCRT non-inferior to routine LCRT; 9.1% required salvage LCRT. |
| CONVERT [41] | 3-year LRRFS: 96.3% vs. 97.4% (NI not formally met) | ~20% vs. ~22% | nCT offered comparable DFS/OS with significantly less long-term toxicity. |
| FOWARC 10-year [50] | 10-year DFS: 60.5–62.6% vs. 52.5% (NS); 10-year LR: 9.6% vs. 10.8% (NS) | ~28% vs. ~14% * | mFOLFOX6 alone non-inferior to CRT at 10 years; pCR predicts excellent survival. |
| GRECCAR 4 [42] | 5-year DFS (response-adaptive) | ypT0 rates: Arm A: 10%, Arm B: 60%, Arm C: 15%, overall: 24% | Good responders to induction CT can avoid CRT without compromising outcomes. |
| UNION [18] | - | 39.8% vs. 15.3% * | Adding camrelizumab to SCRT + CAPOX nearly tripled pCR rate in MSS. |
| STELLAR II [20] | - | CR: 44.0% vs. 22.9% * | Adding sintilimab increased cCR rate in MSS. |
| SPRING-01 [21] | - | pCR: 59.2% vs. 32.7%; CR: 61.2% vs. 32.7% | Adding sintilimab to SCRT + CAPOX significantly increased pCR and CR rates (p = 0.015). |
| PRECAM [22] | - | pCR: 62.5%; MPR (TRG 0–1): 75% | Short-course nCRT + enzalofilimab achieved highest pCR in MSS LARC to date. |
| NRG-GI002 [48] | NAR score diff: 2.9 (p = 0.21); 3-year OS: 95% vs. 87% * | Not reported | Pembrolizumab added to TNT improved 3-year OS but not DFS; NAR reduction not significant. |
| Averectal [19,47] | - | pCR: 36% | SCRT + mFOLFOX-6 + avelumab achieved 36% pCR. |
| OPRA [15] | 5-year DFS: ~70% (both arms) | CCR/NCR: 76% vs. 72% | 5-year TME-free survival: 54% (Consolidation) vs. 39% (Induction) *; Consolidation favored for OP. |
| OPERA [16] | - | CCR/NCR: 92% vs. 64% * | 5-year OP: 79% (CXB) vs. 56% (EBRT) *; CXB boost superior. |
| MONT-R TEM [30,31] | 5-year DFS: 75.6% vs. 80.9% (NS); 5-year OS: 93.2% vs. 88.2% (NS) | pCR (TEM): 57.9% ypT0 | TEM after cCR/near-cCR provides comparable survival with better function. |
| RAPIDO pCR | 5-year OS after pCR: >90% (both arms) | - | Predictors of pCR: TNT (OR 2.70), CEA < 5 µg/L, tumor < 40 mm. |
| OPRA Grade | 3-year DFS: 88% (CCR) vs. 69% (NCR) vs. 56% (ICR) | - | 3-year OP: 77% (CCR) vs. 40% (NCR); three-tier response highly prognostic. |
| STELLAR LPLN [28] | 3-year DFS in LPLN+: 51.7% vs. 66.2% (LPLN−) | - | LPLN+ remains a negative prognostic factor despite TNT. |
| CINTS-R (interim) [25,26] | Primary endpoint (2-year DrTF) not yet reported | - | ctDNA-guided stratification feasible; substantial discordance with clinical risk. |
| Polish II long-term [39] | 8-year OS: 49% vs. 49% (NS); 8-year DFS: 43% vs. 41% (NS) | 16% vs. 12% (NS) | Early OS benefit of SCRT-based TNT lost with longer follow-up; no difference in late complications. |
| MONT-R chemo [30,31] | 3-year DFS: comparable (NS) | 25.5% vs. 25.3% (NS) | Adding oxaliplatin to nCRT improved tumor regression (CAP 0–1: 58.6% vs. 46.8% *) but not survival. |
| Trial | cT4 (%) | cN2 (%) | EMVI+ (%) | MRF+ (%) | Other High-Risk Features | Radiotherapy Backbone | pCR Rate (TNT Arm) | 3-Year DFS/OS |
|---|---|---|---|---|---|---|---|---|
| High-risk LARC trials | ||||||||
| RAPIDO [11] | 74% | 86% | 53% | ~35–40% | - | SCRT (5 × 5 Gy) | 28% | 3-year DrTF 23.7% (improved) |
| PRODIGE 23 [12] | 26% | ~70% | Not reported | Not reported | - | LCRT (50.4 Gy) | 27.5% | 7-year OS 81.9% (improved) |
| STELLAR [13] | 37% | 74% | Not reported | Not reported | - | SCRT (5 × 5 Gy) | 21.8% | 3-year DFS 64.5% (NI) |
| TNTCRT [14] | Included (cT4a–b) | Included | Included | Included | Enlarged lateral nodes | LCRT (50–50.4 Gy) | 27.5% | 3-year DFS 77.0% (improved) |
| Polish II [39] | Majority cT4 or fixed cT3 | Not specified | Not specified | Not specified | Locally recurrent (3%) | SCRT (5 × 5 Gy) | 16% | 8-year OS 49% (NS) |
| MONT-R chemo [30,31] | High-risk (cT4, cN2, EMVI+, MRF+) | Included | Included | Included | - | LCRT | 25.5% (CapeOX) | 3-year DFS comparable (NS) |
| Lower-risk/de-escalation trials | ||||||||
| PROSPECT [40] | 0% (excluded cT4) | ~75% (cN1–2) | Not specified | 0% (CRM-negative) | Mid-upper rectal tumors | LCRT (selective) | 21.4% (FOLFOX alone) | 5-year DFS 80.8% (NI) |
| CONVERT [41] | 0% (excluded cT4b, MRF+) | Included (cN2 allowed) | 17–22% | 0% (uninvolved MRF) | Distance 5–12 cm from AV | None (nCT alone) | ~20% | 3-year DFS 89.2% (comparable) |
| FOWARC [50] | ~25–27% (cT4a–b) | ~60–70% | Not reported | ~31–35% | - | LCRT (in RT arms) | 27.5% (mFOLFOX + RT) | 10-year DFS 60–62% (NS) |
| Trial | Acute Grade ≥ 3 Toxicity (Pre-Operative) | Completion of Planned Pre-Operative Therapy | Notable Toxicity and Clinical Safety Observations |
|---|---|---|---|
| RAPIDO [45] | 47.6% vs. 24.7% * (TNT vs. CRT) | 84.6% vs. 90.0% * | No significant difference in global QoL, bowel function (LARS), or chronic toxicity at 3 years. |
| PRODIGE 23 [57] | 46.9% vs. 35.6% * (TNT vs. CRT) | 89.6% vs. 98.7% * | TNT transiently reduced QoL during CT; long-term QoL converged. Baseline physical function prognostic. |
| STELLAR [58] | 26.5% vs. 12.6% * (TNT vs. CRT) | 82.6% vs. 95.2% * | At 6-year follow-up, no clinically significant difference in global QoL or anal function (Wexner). |
| TNTCRT [14] | Thrombocytopenia (10.3% grade 3–4 in TNT arm) | High in both arms | TNT well tolerated; no significant difference in severe post-op morbidity. |
| PROSPECT [40] | 41.0% vs. 22.6% * (FOLFOX vs. CRT) | 89.5% vs. 84.3% | FOLFOX: higher neuropathy, fatigue, nausea; CRT: higher diarrhea. Long-term: CRT worse sexual function. |
| CONVERT [41] | Grade 2–4 long-term AEs: 16.0% vs. 26.3% * | ~90% both arms | nCT significantly reduced proctitis (33.6% vs. 41.7%, p = 0.049) and long-term toxicity. |
| FOWARC 10-year [50] | Not reported in long-term update | Not reported | Long-term survival comparable; pCR associated with excellent outcomes (10-year OS 92.4%). |
| GRECCAR 4 [42] | Not reported | High | Response-adaptive strategy feasible; good responders avoided CRT toxicity. |
| UNION [18] | ~45% vs. ~35% | ~88% both arms | Adding camrelizumab increased irAEs (rash, thyroiditis) typically grade 1–2. |
| STELLAR II [20] | 34.5% vs. 19.4% * (iTNT vs. TNT) | High both arms | Grade 3–4 irAEs: 5.5%; manageable. |
| SPRING-01 [21] | Grade 3–4: 33% vs. 35% (NS) | 82% vs. 84% | Most common grade 3–4: thrombocytopenia (12% vs. 22%). No treatment-related deaths in iTNT arm. |
| PRECAM [22] | Grade 3: 2/32 (6.25%) | 32/34 completed | Adverse events: tenesmus (78.1%), diarrhea (62.5%), leukopenia (40.6%); manageable. |
| NRG-GI002 [48] | Not reported in long-term | Not reported | No unexpected safety signals with pembrolizumab. |
| OPRA [43] | ~38% (induction) vs. ~41% (consolidation) | ~85% | No significant difference in late toxicity between sequences. |
| CAO/ARO/AIO-16 [49] | 36% (during TNT) | 90/91 RT; 82/88 CT | Sustained CCR patients had better bowel function (lower LARS/Wexner) at 18/36 months vs. immediate TME. |
| OPERA [24] | Not reported | High | CXB boost well tolerated; no increase in severe late toxicity. |
| MONT-R TEM [30,31] | Not applicable (post-nCRT) | - | TEM: significantly shorter operation time, less blood loss, shorter hospital stay, better sphincter function (Wexner 1 vs. 4, LARS 0 vs. 17). |
| PRORECT [23] | Acute ≥ G2 Diarrhea: 10% vs. 27% * (Proton vs. Photon) | Similar | Dosimetric comparison suggested proton therapy reduces acute GI toxicity. |
| MRI-LINAC LoRP [46] | Not reported | - | LoRP reduced treatment session duration by >20 min vs. fully adaptive; 92% of LoRP plans acceptable vs. 74% for couch shift. |
| Polish II long-term [39] | Acute toxicity lower in SCRT-based TNT | ~85% | Late grade 3+ complications: 11% vs. 9% (NS); no difference in late toxicity. |
| MONT-R chemo [30,31] | Grade 3–4: 14.1% vs. 9.3% (NS) | ~91% | CapeOX increased tumor regression (CAP 0–1) without significant increase in severe AEs. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Ismaili, N. Total Neoadjuvant Therapy, Organ Preservation and Beyond: A State-of-the-Art Systematic Review and Critical Appraisal of Locally Advanced Rectal Cancer Management. Diseases 2026, 14, 182. https://doi.org/10.3390/diseases14050182
Ismaili N. Total Neoadjuvant Therapy, Organ Preservation and Beyond: A State-of-the-Art Systematic Review and Critical Appraisal of Locally Advanced Rectal Cancer Management. Diseases. 2026; 14(5):182. https://doi.org/10.3390/diseases14050182
Chicago/Turabian StyleIsmaili, Nabil. 2026. "Total Neoadjuvant Therapy, Organ Preservation and Beyond: A State-of-the-Art Systematic Review and Critical Appraisal of Locally Advanced Rectal Cancer Management" Diseases 14, no. 5: 182. https://doi.org/10.3390/diseases14050182
APA StyleIsmaili, N. (2026). Total Neoadjuvant Therapy, Organ Preservation and Beyond: A State-of-the-Art Systematic Review and Critical Appraisal of Locally Advanced Rectal Cancer Management. Diseases, 14(5), 182. https://doi.org/10.3390/diseases14050182