


The Impact of Preventive Protocols on Oral Health Outcomes in Cancer Patients Undergoing Chemotherapy or Radiotherapy: A Systematic Review and Meta-Analysis
 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Extraction and Analysis
2.5. Classification of Study Designs
2.6. Meta-Analysis
3. Results
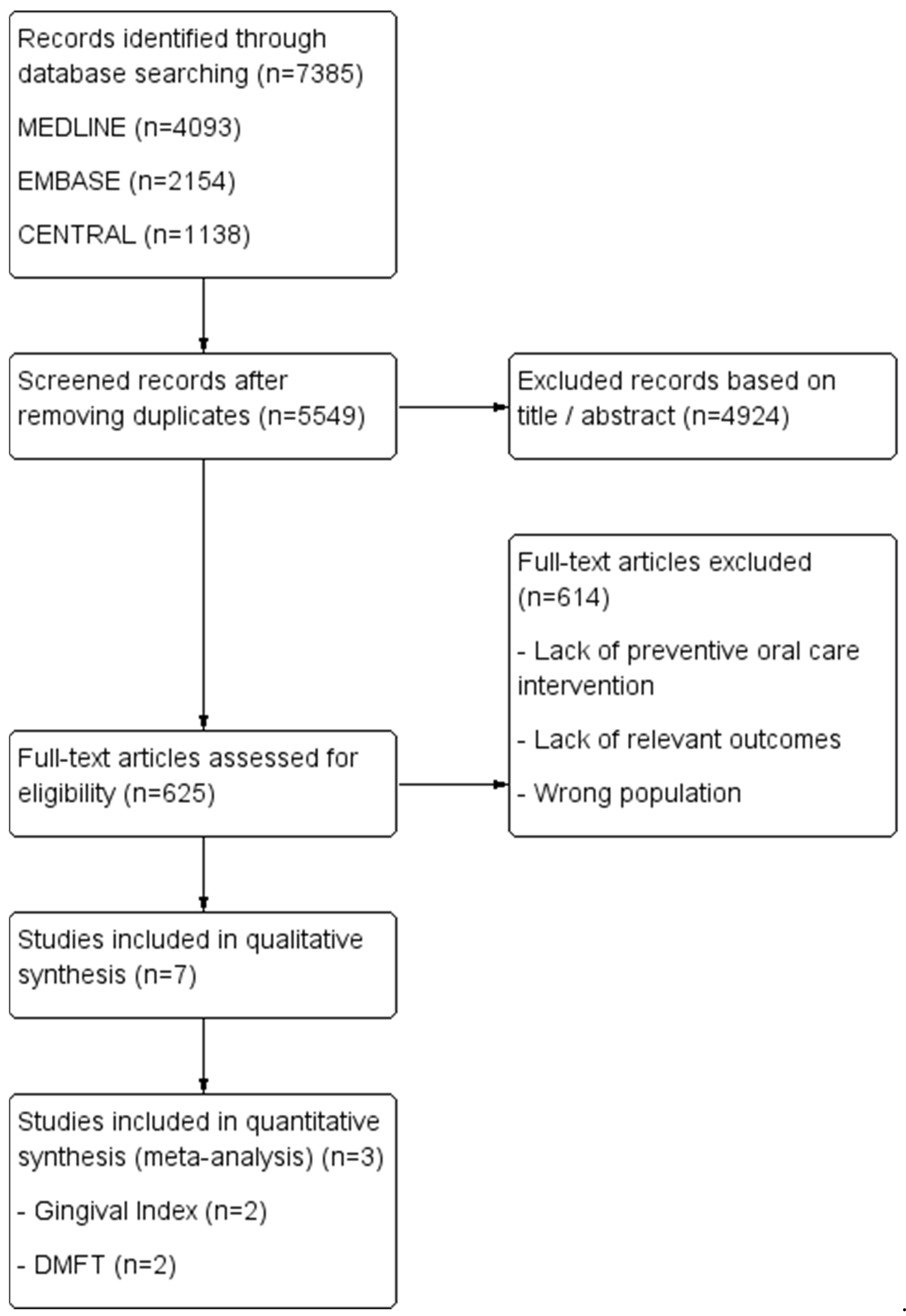
3.1. Study Selection and Screening Results
3.2. Characteristics of the Included Studies for Qualitative Synthesis
3.3. Risk of Bias
3.4. Statistical Findings in Selected Articles
3.5. Results of Meta-Analyses
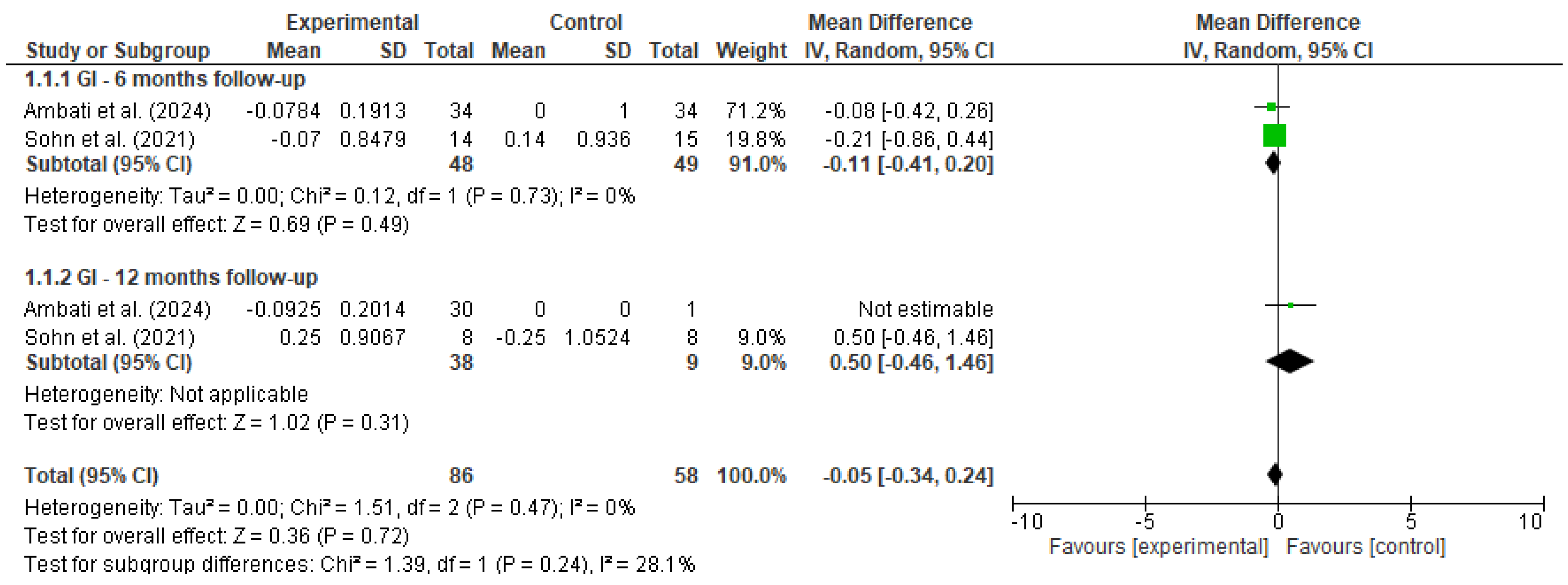
3.5.1. Gingival Index (GI)
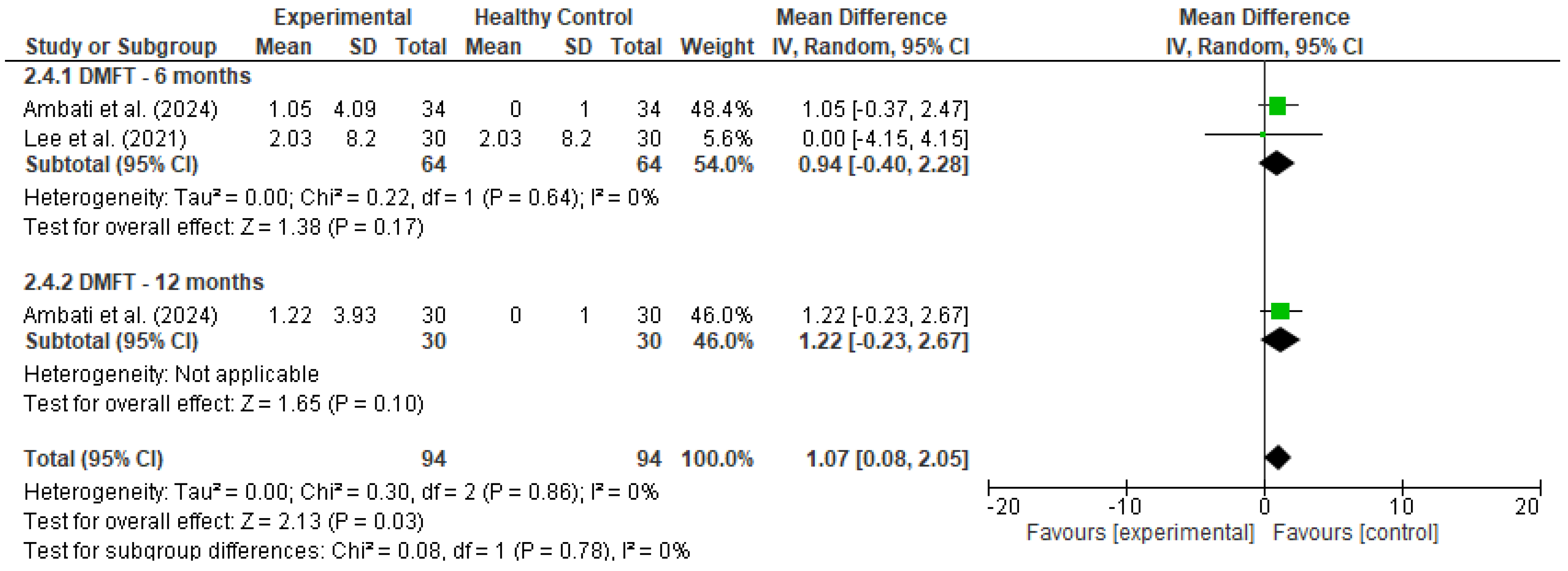
3.5.2. DMFT
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| GI | Gingival Index |
| DMFT | Decayed, Missing, and Filled Teeth |
| RT | Radiotherapy |
| PBMT | Photobiomodulation Therapy |
| OHI-S | Simplified Oral Hygiene Index |
| CPI | Community Periodontal Index |
| OAG | Oral Assessment Guide |
| PI | Plaque Index |
| PD | Probing Depth |
| ORN | Osteoradionecrosis |
| SD | Standard Deviation |
| WMD | Weighted Mean Difference |
| ROBINS-I | Risk Of Bias In Non-randomized Studies of Interventions |
| NIH | National Institutes of Health |
| AXIS | Appraisal Tool for Cross-Sectional Studies |
| MASCC/ISOO | Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology |
| EBMT | European Society for Blood and Marrow Transplantation |
| RevMan | Review Manager |
| CI | Confidence Interval |
References
- Mee, T.; Kirkby, N.F.; Defourny, N.N.; Kirkby, K.J.; Burnet, N.G. The Use of Radiotherapy, Surgery and Chemotherapy in the Curative Treatment of Cancer: Results from the FORTY (Favourable Outcomes from RadioTherapY) Project. Br. J. Radiol. 2023, 96, 20230334. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.A.; Ottaviani, G.; Treister, N.S.; Hanna, G.J. An Overview of Clinical Oncology and Impact on Oral Health. Front. Oral Health 2022, 3, 874332. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.B.; Pedersen, A.M.L.; Vissink, A.; Andersen, E.; Brown, C.G.; Davies, A.N.; Dutilh, J.; Fulton, J.S.; Jankovic, L.; Lopes, N.N.F.; et al. A Systematic Review of Salivary Gland Hypofunction and Xerostomia Induced by Cancer Therapies: Prevalence, Severity and Impact on Quality of Life. Support. Care Cancer 2010, 18, 1039–1060. [Google Scholar] [CrossRef]
- Villafuerte, K.R.V.; de Jesus Hernandez Martinez, C.; Dantas, F.T.; Carrara, H.H.A.; dos Reis, F.J.C.; Palioto, D.B. The Impact of Chemotherapeutic Treatment on the Oral Microbiota of Patients with Cancer: A Systematic Review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 552–566. [Google Scholar] [CrossRef]
- Takahashi, N. Microbial Ecosystem in the Oral Cavity: Metabolic Diversity in an Ecological Niche and Its Relationship with Oral Diseases. Int. Congr. Ser. 2005, 1284, 103–112. [Google Scholar] [CrossRef]
- Elad, S.; Raber-Durlacher, J.E.; Brennan, M.T.; Saunders, D.P.; Mank, A.P.; Zadik, Y.; Quinn, B.; Epstein, J.B.; Blijlevens, N.M.A.; Waltimo, T.; et al. Basic Oral Care for Hematology-Oncology Patients and Hematopoietic Stem Cell Transplantation Recipients: A Position Paper from the Joint Task Force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) and the European Society for Blood and Marrow Transplantation (EBMT). Support. Care Cancer 2015, 23, 223–236. [Google Scholar] [CrossRef]
- Lalla, R.V.; Bowen, J.; Barasch, A.; Elting, L.; Epstein, J.; Keefe, D.M.; McGuire, D.B.; Migliorati, C.; Nicolatou-Galitis, O.; Peterson, D.E.; et al. MASCC/ISOO Clinical Practice Guidelines for the Management of Mucositis Secondary to Cancer Therapy. Cancer 2014, 120, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.B.; Thariat, J.; Bensadoun, R.-J.; Barasch, A.; Murphy, B.A.; Kolnick, L.; Popplewell, L.; Maghami, E. Oral Complications of Cancer and Cancer Therapy. CA Cancer J. Clin. 2012, 62, 400–422. [Google Scholar] [CrossRef]
- Oral Complications (PDQ®)-NCI. Available online: https://www.cancer.gov/about-cancer/treatment/side-effects/mouth-throat/oral-complications-hp-pdq (accessed on 24 April 2025).
- Saunders, D.; Koyfman, S.A.; Ismaila, N.; Futran, N.D.; Mowery, Y.M.; Watson, E.; Yang, D.H.; Peterson, D.E. Prevention and Management of Osteoradionecrosis in Patients with Head and Neck Cancer Treated With Radiation Therapy: ISOO-MASCC-ASCO Guideline Clinical Insights. JCO Oncol. Pract. 2024, 20, 1571–1574. [Google Scholar] [CrossRef]
- Villa, A.; Epstein, J.B.; Yarom, N.; Hong, C.; Fulop, C.; Bossi, P.; Elad, S. MASCC/ISOO Clinical Practice Statement: Management of Oral Complications of Targeted Therapy. Support. Care Cancer 2024, 32, 549. [Google Scholar] [CrossRef]
- Hong, C.H.L.; Gueiros, L.A.; Fulton, J.S.; Cheng, K.K.F.; Kandwal, A.; Galiti, D.; Fall-Dickson, J.M.; Johansen, J.; Ameringer, S.; Kataoka, T.; et al. Systematic Review of Basic Oral Care for the Management of Oral Mucositis in Cancer Patients and Clinical Practice Guidelines. Support. Care Cancer 2019, 27, 3949–3967. [Google Scholar] [CrossRef] [PubMed]
- Nathan, C.-A.O.; Asarkar, A.A.; Entezami, P.; Corry, J.; Strojan, P.; Poorten, V.V.; Makitie, A.; Eisbruch, A.; Robbins, K.T.; Smee, R.; et al. Current Management of Xerostomia in Head and Neck Cancer Patients. Am. J. Otolaryngol. 2023, 44, 103867. [Google Scholar] [CrossRef] [PubMed]
- Cerchietti, L.C.A.; Navigante, A.H.; Bonomi, M.R.; Zaderajko, M.A.; Menéndez, P.R.; Pogany, C.E.; Roth, B.M.C. Effect of Topical Morphine for Mucositis-Associated Pain Following Concomitant Chemoradiotherapy for Head and Neck Carcinoma. Cancer 2002, 95, 2230–2236. [Google Scholar] [CrossRef] [PubMed]
- Daugėlaitė, G.; Užkuraitytė, K.; Jagelavičienė, E.; Filipauskas, A. Prevention and Treatment of Chemotherapy and Radiotherapy Induced Oral Mucositis. Medicina 2019, 55, 25. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4. 2023. Available online: https://training.cochrane.org/handbook/current (accessed on 13 February 2024).
- Ambati, P.; Galhotra, V.; Jondhale, S.N.; Dolker, T.; Ravi, M.; Rathod, P. Evaluation of Oral Complications in Children Undergoing Chemotherapy: An Observational Study. J. Indian Soc. Pedod. Prev. Dent. 2024, 42, 184–189. [Google Scholar] [CrossRef]
- Sohn, H.-O.; Park, E.-Y.; Jung, Y.-S.; Lee, J.-Y.; Kim, E.-K. Effects of the Professional Oral Care Management Program on Patients with Head and Neck Cancer after Radiotherapy: A 12-Month Follow-Up. J. Dent. Sci. 2021, 16, 453–459. [Google Scholar] [CrossRef]
- Lee, H.-J.; Han, D.-H.; Kim, J.-H.; Wu, H.-G. The Effect of Comprehensive Oral Care Program on Oral Health and Quality of Life in Patients Undergoing Radiotherapy for Head and Neck Cancer: A Quasi-Experimental Case-Control Study. Medicine 2021, 100, e25540. [Google Scholar] [CrossRef]
- Bertl, K.; Loidl, S.; Kotowski, U.; Heiduschka, G.; Thurnher, D.; Stavropoulos, A.; Schneider-Stickler, B. Oral Health Status and Dental Care Behaviours of Head and Neck Cancer Patients: A Cross-Sectional Study in an Austrian Tertiary Hospital. Clin. Oral Investig. 2016, 20, 1317–1327. [Google Scholar] [CrossRef]
- Amin, M.; Khan, F.R.; Allana, A.; Barolia, R.; Azam, I. Oral Health of Chemotherapy Patients before and after Provision of Oral Hygiene Instructions at a Tertiary Care Hospital: Pre-Post Design. BMC Oral Health 2024, 24, 655. [Google Scholar] [CrossRef]
- Morais, M.O.; Martins, A.F.L.; de Jesus, A.P.G.; de Sousa Neto, S.S.; da Costa, A.W.F.; Pereira, C.H.; Oton-Leite, A.F.; de Freitas, N.M.A.; Leles, C.R.; Mendonça, E.F. A Prospective Study on Oral Adverse Effects in Head and Neck Cancer Patients Submitted to a Preventive Oral Care Protocol. Support. Care Cancer 2020, 28, 4263–4273. [Google Scholar] [CrossRef]
- Frydrych, A.M.; Slack-Smith, L.M.; Parsons, R. Compliance of Post-Radiation Therapy Head and Neck Cancer Patients with Caries Preventive Protocols. Aust. Dent. J. 2017, 62, 192–199. [Google Scholar] [CrossRef] [PubMed]
- ROBINS-I Tool | Cochrane Methods. Available online: https://methods.cochrane.org/robins-i (accessed on 21 March 2025).
- Study Quality Assessment Tools | NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 21 March 2025).
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological Quality (Risk of Bias) Assessment Tools for Primary and Secondary Medical Studies: What Are They and Which Is Better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a Critical Appraisal Tool to Assess the Quality of Cross-Sectional Studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed]
- Pispero, A.; Lombardi, N.; Manfredi, M.; Varoni, E.M.; Sardella, A.; Lodi, G. Oral Infections in Oral Cancer Survivors: A Mini-Review. Front. Oral Health 2022, 3, 970074. [Google Scholar] [CrossRef]
- Yusuf, K.; Sampath, V.; Umar, S. Bacterial Infections and Cancer: Exploring This Association And Its Implications for Cancer Patients. Int. J. Mol. Sci. 2023, 24, 3110. [Google Scholar] [CrossRef]
- Deng, J.; Jackson, L.; Epstein, J.B.; Migliorati, C.A.; Murphy, B.A. Dental Demineralization and Caries in Patients with Head and Neck Cancer. Oral Oncol. 2015, 51, 824–831. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Database | Search String |
|---|---|
| Medline | ((“Oral Health” [Mesh] OR “Dental Care” [Mesh] OR “Preventive Dentistry” [Mesh] OR “Mouth Diseases/prevention and control” [Mesh] OR “Fluorides” [Mesh] OR “Fluoride Therapy” [Mesh]) AND (“Neoplasms”[Mesh] OR “Chemotherapy” [Mesh] OR “Radiotherapy” [Mesh] OR “Cancer Patients” [Mesh] OR “Oncology Patients” [Mesh])) |
| Embase | (‘oral health’/exp OR ‘dental care’/exp OR ‘preventive dentistry’/exp OR ‘mouth disease prevention’/exp OR ‘fluoride’/exp OR ‘fluoride therapy’/exp) AND (‘neoplasm’/exp OR ‘cancer patient’/exp OR ‘chemotherapy’/exp OR ‘radiotherapy’/exp) |
| Central | (“Preventive Dentistry” OR “Dental Prophylaxis” OR “Fluoride Therapy” OR “Oral Hygiene” OR “Mouth Rinses” OR “Fluoride”) AND (“Cancer Patients” OR “Neoplasms” OR “Oncology”) AND (“Chemotherapy” OR “Radiotherapy” OR “Antineoplastic Agents”) AND (“Oral Health” OR “Oral Mucositis” OR “Xerostomia” OR “Dental Care”) |
| Study | Intervention | Outcome Measures | Key Findings |
|---|---|---|---|
| Ambati et al. [18] | Oral hygiene education, fluoride varnish, SDF, sealants, mouthwash, and topical analgesics | Mucositis severity, gingival index, oral hygiene index, dental caries (DMFT) | Oral mucositis severity decreased over time; however, caries remained prevalent, underscoring the need for continued preventive care. |
| Lee et al. [20] | Oral health education (4 sessions), fluoride varnish, daily fluoride mouthrinse | Plaque index, salivary flow rate, bleeding on probing, dental caries, quality of life | Oral health and quality of life improved significantly following preventive care; multidisciplinary collaboration recommended. |
| Bertl et al. [21] | Self-reported preventive behaviors: dental visits, hygiene practices, mouthwash use | Dental caries (DMFT), periodontal disease, probing depth, bleeding on probing | Low compliance with preventive behaviors was associated with poorer oral health; highlights the gap in post-treatment dental care. |
| Amin et al. [22] | Oral hygiene instruction over six weeks | Simplified Oral Hygiene Index (OHI-S), Community Periodontal Index (CPI) | Significant improvement in oral hygiene in 26% of participants; patient education shown to be effective. |
| Morais et al. [23] | Preventive oral care including hygiene, restorations, hydration, PBMT | Oral mucositis severity, pain, dysphagia, quality of life, RT interruption | Preventive program combined with PBMT effectively reduced mucositis and improved treatment continuity. |
| Sohn et al. [19] | Professional hygiene care weekly during RT and quarterly post-RT, fluoride varnish | Plaque index, gingival index, dental caries, periodontal attachment loss | Regular hygiene care was effective in maintaining oral health over 12 months post-radiotherapy. |
| Frydrych et al. [24] | Dietary advice, dental care, hygiene instruction, fluoride use over 12 months | Compliance with care protocols and the development of caries | Non-compliance with preventive strategies was significantly associated with increased risk of caries. |
| Study | Design | Risk of Bias Tool | Overall Risk of Bias |
|---|---|---|---|
| Ambati et al. [18] | Prospective observational pre–post study | NIH Pre–Post Tool | Moderate |
| Lee et al. [20] | Quasi-experimental (pre–post, no control group) | ROBINS-I | Moderate |
| Bertl et al. [21] | Cross-sectional | AXIS | Moderate |
| Amin et al. [22] | Prospective observational pre–post study | NIH Pre–Post Tool | Moderate |
| Morais et al. [23] | Prospective cohort study with pre–post assessments | NIH Pre–Post Tool | Moderate |
| Sohn et al. [19] | Prospective cohort study | ROBINS-I | Low |
| Frydrych et al. [24] | Retrospective observational pre–post study | NIH Pre–Post Tool | Moderate |
| Study | Outcome Measure | Reported Results |
|---|---|---|
| Ambati et al. [18] | Oral mucositis (WHO scale) | Baseline (n = 44): Grade 0: 25 (56.8%), I: 9 (20.5%), II: 4 (9.1%), III: 4 (9.1%), IV: 2 (4.5%) First follow-up (3–6 months) (n = 34): Grade 0: 19 (55.88%), I: 8 (23.52%), II: 5 (14.70%), III: 1 (2.95%), IV: 1 (2.95%) Second follow-up (9–12 months) (n = 30): Grade 0: 25 (83.3%), I: 4 (13.3%), III: 1 (3.3%) |
| Gingival Index (mean ± SD) | Baseline (n = 44): 0.0983 ± 0.21549 First follow-up (n = 34): 0.0199 ± 0.06565 Second follow-up (n = 30): 0.0058 ± 0.03195 | |
| Oral hygiene index; simplified (DI-S) (mean ± SD) | Baseline (n = 44): 1.5820 ± 1.13729 First follow-up (n = 34): 1.3350 ± 0.85867 Second follow-up (n = 30): 1.6213 ± 1.14416 | |
| DMFT (mean ± SD) | Baseline (n = 44): 3.9773 ± 3.92659 First follow-up (n = 34): 5.0294 ± 4.23181 Second follow-up (n = 30): 5.2000 ± 3.92516 | |
| Lee et al. [20] | DMFT (mean ± SD) | Experimental group (n = 31): before: 5.45 ± 5.64; after 6 months: 5.45 ± 5.77; p = 1.000 Control group (no preventive dental care) (n = 30): before: 6.37 ± 8.12; after 6 months: 8.40 ± 8.27; p = 0.006 * |
| Plaque score (O’Leary percentage) (mean ± SD) | Experimental group (n = 31): before: 24.70 ± 22.23; after 6 months: 5.90 ± 5.00; p < 0.001 * Control group (n = 30): before: 15.74 ± 12.25; after 6 months: 21.52 ± 20.61; p = 0.113 | |
| Bleeding on probing (mean ± SD) | Experimental group (n = 31): before: 8.41 ± 12.32; after 6 months: 2.83 ± 6.64; p = 0.004 * Control group (n = 30): before: 8.85 ±10.56; after 6 months: 10.41 ± 13.25; p = 0.388 | |
| Salivary flowrate (mL/min, mean ± SD) | Experimental group (n = 31): before: 1.18 ± 0.56; after 6 months: 0.88 ± 0.41; p = 0.027 * Control group (n = 30): before: 1.29 ± 0.72; after 6 months: 0.66 ± 0.42; p = 0.001 * | |
| Bertl et al. [21] | Presence of periodontitis | Dental consultation prior to treatment: No = 19/22 present, Yes = 17/24 present Last dental check-up: <12 months = 19/28 present, ≥12 months = 17/18 present Frequency of professional tooth cleaning: <1/year = 22/27 present, ≥1/year = 14/19 present |
| ≥1 Tooth with probing pocket depth (PD) ≥ 5 mm | Dental consultation prior to treatment: no = 10/22 present, yes = 9/24 present Last dental check-up: <12 months = 13/28 present, ≥12 months = 6/18 present Frequency of professional tooth cleaning: <1/year = 10/27 present, ≥1/year = 9/19 present | |
| ≥1 Tooth with caries | Dental consultation prior to treatment: no = 17/20 present, yes = 16/24 present Last dental check-up: <12 months = 17/27 present, ≥12 months = 16/17 present Frequency of professional tooth cleaning: <1/year = 23/26 present, ≥1/year = 10/18 present | |
| Plaque index (%) (mean ± SD) | Frequency of professional tooth cleaning: <1/year = 73.4 ± 26.5, ≥1/year = 54.4 ± 31.8 | |
| No. of teeth with caries (mean ± SD) | Frequency of professional tooth cleaning: <1/year = 7.2 ± 7.2, ≥1/year = 1.9 ± 2.3 | |
| No. of teeth with PD ≥ 5 mm (Mean ± SD) | Frequency of professional tooth cleaning: <1/year = 6.2 ± 7.7, ≥1/year = 3.5 ± 5.1 | |
| Amin et al. [22] | Oral hygiene index change (OHI) if brushing | Brushing: no change = 34 (72.3%), change = 13 (27.7%) Not brushing: no change = 5 (83.3%), change = 1 (16.7%); p = 1.00 |
| Oral hygiene index change (OHI) if flossing | Flossing: no change = 6 (85.7%), change = 1 (14.3%) No flossing: no change = 33 (73.0%), change = 13 (27.0%); p = 0.81 | |
| Oral hygiene index change (OHI) according to date of last dental visit | <6 months: no change = 3 (73.0%), change = 1 (27.0%) >6 months: no change = 27 (60.0%), change = 6 (40.0%) >1 year: no change = 3 (81.8%), change = 2 (18.2%) Never: no change = 6 (54.6%), change = 5 (45.5%); p = 0.22 | |
| Morais et al. [23] | Oral Assessment Guide (OAG) (mean ± SD) | First exam (post-consent): 10 ± 2.0; second exam (1st RT session): 10 ± 4.0; third exam (15th RT session): 12 ± 2.0 * |
| Plaque control record (O’Leary percentage) (mean ± SD) | First exam: 68.0 ± 34.9; second exam: 55.7 ± 37.9 *; third exam: 50.0 ± 39.1 * | |
| Periodontal screening and recording (PSR) by sextant (mean ± SD) | S1: 1st: 2.0 ± 2.0; 2nd: 1.0 ± 3.0; 3rd: 1.0 ± 3.0 S2: 1st: 2.0 ± 3.0; 2nd: 1.0 ± 2.0 *; 3rd: 0.0 ± 1.0 * S3: 1st: 2.0 ± 2.0; 2nd: 1.0 ± 3.0; 3rd: 1.5 ± 3.0 S4: 1st: 2.0 ± 1.0; 2nd: 1.0 ± 2.0 *; 3rd: 1.0 ± 2.0 S5: 1st: 2.0 ± 1.0; 2nd: 1.0 ± 2.0 *; 3rd: 1.0 ± 1.0 * S6: 1st: 1.0 ± 2.0; 2nd: 0.0 ± 2.0 *; 3rd: 0.0 ± 1.0 * | |
| Sohn et al. [19] | Decayed tooth (mean ± SD) | Baseline: healthy group: 0.00 ± 0.00; vulnerable group: 1.29 ± 1.38; p = 0.001 * Six-month follow-up: healthy (n = 15): 0.00 ± 0.00 → 0.07 ± 0.26, p = 0.33; vulnerable (n = 14): 1.29 ± 1.38 → 1.57 ± 2.14, p = 0.391 Twelve-month follow-up: healthy (n = 8): 0.00 ± 0.00 → 0.13 ± 0.354, p = 0.351; vulnerable (n = 8): 0.88 ± 1.126 → 1.13 ± 1.356, p = 0.699 |
| Plaque index (Loe and Silness) (mean ± SD) | Healthy group: 0.67 ±1.04; vulnerable group: 1.00 ± 0.96; p = 0.29 Six-month follow-up: healthy (n = 15): 0.66 ± 1.04 → 0.80 ± 1.26, p = 0.653; vulnerable (n = 14): 1.00 ± 0.96 → 0.92 ± 0.99, p = 0.793 Twelve-month follow-up: healthy (n = 8): 0.50 ± 1.069 → 0.75 ± 0.707, p = 0.451; vulnerable (n = 8): 1.00 ± 1.069 → 0.50 ± 0.756, p = 0.104 | |
| Gingival index (mean ± SD) | Baseline: healthy group: 1.27 ± 0.96; vulnerable group: 1.43 ± 0.75; p = 0.77 Six-month follow-up: healthy (n = 15): 1.26 ± 0.96 → 1.40 ± 0.91, p = 0.546; vulnerable (n = 14): 1.42 ± 0.75 → 1.35 ± 0.92, p = 0.793 Twelve-month follow-up: healthy (n = 8): 1.25 ± 1.035 → 1.00 ± 1.069, p = 0.685; vulnerable (n = 8): 1.25 ± 0.886 → 1.50 ± 0.926, p = 0.668 | |
| Periodontal pocket depth (mean ± SD) | Baseline: healthy group: 2.67 ± 0.488; vulnerable group: 3.86 ± 1.231; p = 0.005 * Six-month follow-up: healthy (n = 15): 2.66 ± 0.48 → 2.13 ± 0.74, p = 0.041 *; vulnerable (n = 14): 3.85 ± 1.23 → 2.92 ± 1.26, p = 0.031 * Twelve-month follow-up: healthy (n = 8): 2.75 ± 0.463 → 2.38 ± 0.744, p = 0.197; vulnerable (n = 8): 4.00 ± 0.926 → 2.63 ± 0.518, p = 0.008 * | |
| Frydrych et al. [24] | Dental caries at cancer diagnosis | Dental attendance: yes = 38, no = 5 (p = 0.2676) Dietary advice: yes = 33, no = 10 (p = 0.0044 *) Fluoride use: yes = 34, no = 8 (p = 0.0138 *) Oral hygiene instruction: yes = 34, no = 8 (p = 0.0632) |
| Dental caries after cancer treatment | Dental attendance: yes = 14, no = 5 (p = 0.0041 *) Dietary advice: yes = 14, no = 5 (p = 0.0339 *) Fluoride use: yes = 15, no = 5 (p = 0.0183 *) Oral hygiene instruction: yes = 14, no = 6 (p = 0.0087 *) | |
| Dental extractions after treatment | Dental attendance: yes = 18, no = 4 (p = 0.0746) Dietary advice: yes = 17, no = 5 (p = 0.1284) Fluoride use: yes = 18, no = 5 (p = 0.0482 *) Oral hygiene instruction: yes = 18, no = 5 (p = 0.1385) | |
| Development of osteoradionecrosis (ORN) | Dental attendance: yes = 14, no = 2 (p = 0.6164) Dietary advice: yes = 13, no = 4 (p = 0.0861) Fluoride use: yes = 12, no = 5 (p = 0.0127 *) Oral hygiene instruction: yes = 10, no = 7 (p = 0.0006 *) |
| Study | Outcome Measure | Reported Results |
|---|---|---|
| Ambati et al. [18] | Gingival index (mean ± SD) | Baseline: 0.0983 ± 0.21549; 3–6 M: 0.0199 ± 0.06565; 9–12 M: 0.0058 ± 0.03195 |
| Oral hygiene index (DI-S) (mean ± SD) | Baseline: 1.5820 ± 1.13729; 3–6 M: 1.3350 ± 0.85867; 9–12 M: 1.6213 ± 1.14416 | |
| DMFT (mean ± SD) | Baseline: 3.98 ± 3.93; 3–6 M: 5.03 ± 4.23; 9–12 M: 5.20 ± 3.93 | |
| Plaque score (O’Leary %) | Before: 24.70 ± 22.23; after 6 M: 5.90 ± 5.00; p < 0.001 | |
| Lee et al. [20] | DMFT (mean ± SD) | Before: 5.45 ± 5.64; after 6 M: 5.45 ± 5.77; control: before 6.37 ± 8.12 → 8.40 ± 8.27 |
| Plaque score (O’Leary %) | Before: 15.74 ± 12.25; after: 21.52 ± 20.61; p = 0.113 | |
| Bertl et al. [21] | Plaque index (%) | <1/year: 73.4 ± 26.5; ≥1/year: 54.4 ± 31.8 |
| No. of teeth with caries (mean ± SD) | <1/year: 7.2 ± 7.2; ≥1/year: 1.9 ± 2.3 | |
| DMFT (mean ± SD) | Varied by group and timepoint | |
| Plaque index (Loe and Silness) | Baseline: 1.00 ± 0.96; 12 M: healthy: 0.75, vulnerable: 0.50 | |
| Amin et al. [22] | Oral hygiene index change | Change rate brushing vs. no brushing; flossing vs. no flossing |
| Morais et al. [23] | Plaque control record (O’Leary %) | 1st: 68.0 ± 34.9; 2nd: 55.7 ± 37.9; 3rd: 50.0 ± 39.1 |
| Periodontal screening and recording (PSR) | Sextant-wise reduction over 3 visits | |
| Sohn et al. [19] | Plaque index (Loe and Silness) | Baseline: healthy, 0.67 ± 1.04; vulnerable, 1.00 ± 0.96; NS |
| Gingival index | Baseline to 12 M: non-significant changes | |
| Periodontal pocket depth (mean ± SD) | Baseline: healthy, 2.67; vulnerable, 3.86; ↘ after 6 M and 12 M | |
| DMFT (dental caries at diagnosis and after) | Fluoride, diet advice, and attendance linked to lower caries | |
| Frydrych et al. [24] | Dental caries after cancer treatment | p values for reduction in caries across behaviors |
| Oral hygiene instruction impact | Instruction linked to improved caries/ORN prevention |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moussa, C.; Estrade, L.; Glomet, J.; Rochefort, G.Y.; Denis, F.; Daou, M.H. The Impact of Preventive Protocols on Oral Health Outcomes in Cancer Patients Undergoing Chemotherapy or Radiotherapy: A Systematic Review and Meta-Analysis. Diseases 2025, 13, 186. https://doi.org/10.3390/diseases13060186
Moussa C, Estrade L, Glomet J, Rochefort GY, Denis F, Daou MH. The Impact of Preventive Protocols on Oral Health Outcomes in Cancer Patients Undergoing Chemotherapy or Radiotherapy: A Systematic Review and Meta-Analysis. Diseases. 2025; 13(6):186. https://doi.org/10.3390/diseases13060186
Chicago/Turabian StyleMoussa, Carol, Laurent Estrade, Jeremy Glomet, Gael Y. Rochefort, Frédéric Denis, and Maha H. Daou. 2025. "The Impact of Preventive Protocols on Oral Health Outcomes in Cancer Patients Undergoing Chemotherapy or Radiotherapy: A Systematic Review and Meta-Analysis" Diseases 13, no. 6: 186. https://doi.org/10.3390/diseases13060186
APA StyleMoussa, C., Estrade, L., Glomet, J., Rochefort, G. Y., Denis, F., & Daou, M. H. (2025). The Impact of Preventive Protocols on Oral Health Outcomes in Cancer Patients Undergoing Chemotherapy or Radiotherapy: A Systematic Review and Meta-Analysis. Diseases, 13(6), 186. https://doi.org/10.3390/diseases13060186