
Cardiac Repair and Clinical Outcomes of Stem Cell Therapy in Heart Failure: A Systematic Review and Meta-Analysis

Abstract
1. Introduction
1.1. Heart Failure with Reduced Ejection Fraction
1.2. Mesenchymal Stem Cells (MSCs)
1.3. Improving LVEF and Secondary Outcomes
1.4. The Importance of This Review
2. Materials and Methods
2.1. Protocol Registration
2.2. Inclusion and Exclusion Criteria
2.2.1. Primary Outcome
2.2.2. Secondary Outcomes
- Measure of cardiac function:
- ○
- Global circumferential strain (GCS)(%): This serves as a prognostic indicator in myocardial disease, particularly when associated with fibrosis [22].
- Functional Capacity: These outcomes are relevant since this particular cohort of patients suffers from a disease that predisposes them to exercise intolerance [23]. The tests used to assess these outcomes are described below.
- ○
- The Minnesota Living with Heart Failure Questionnaire (MLHFQ) is a subjective questionnaire that evaluates the physical and emotional impacts of heart failure on patients [24].
- ○
- The 6-Minute Walk Test (6 MWT) (m) is an inexpensive and easily performed test that has been widely applied in studies that assess HF interventions [25].
- Structural: These outcomes reflect left ventricular remodeling patterns and are independent predictors of survival for HF patients [26].
- ○
- Left ventricular end-diastolic volume index (LVEDVI) (mL/m2).
- ○
- Left ventricular end-systolic volume index (LVESVI) (mL/m2).
- Morphological: A reduction in these outcomes is indicative of less adverse cardiac remodeling and hence reduced wall stress, thereby addressing Laplace’s therapeutics [27].
- ○
- Sphericity (mL).
- ○
- Scar size (%).
- ○
- Scar tissue mass (g).
- Biochemical markers:
2.3. Identification of Studies
2.4. Selection of Studies
2.5. Risk Assessment
2.6. Measures of Treatment Effect
2.7. Assessment of Heterogeneity
3. Results
3.1. Description of the Search
3.2. Study Characteristics
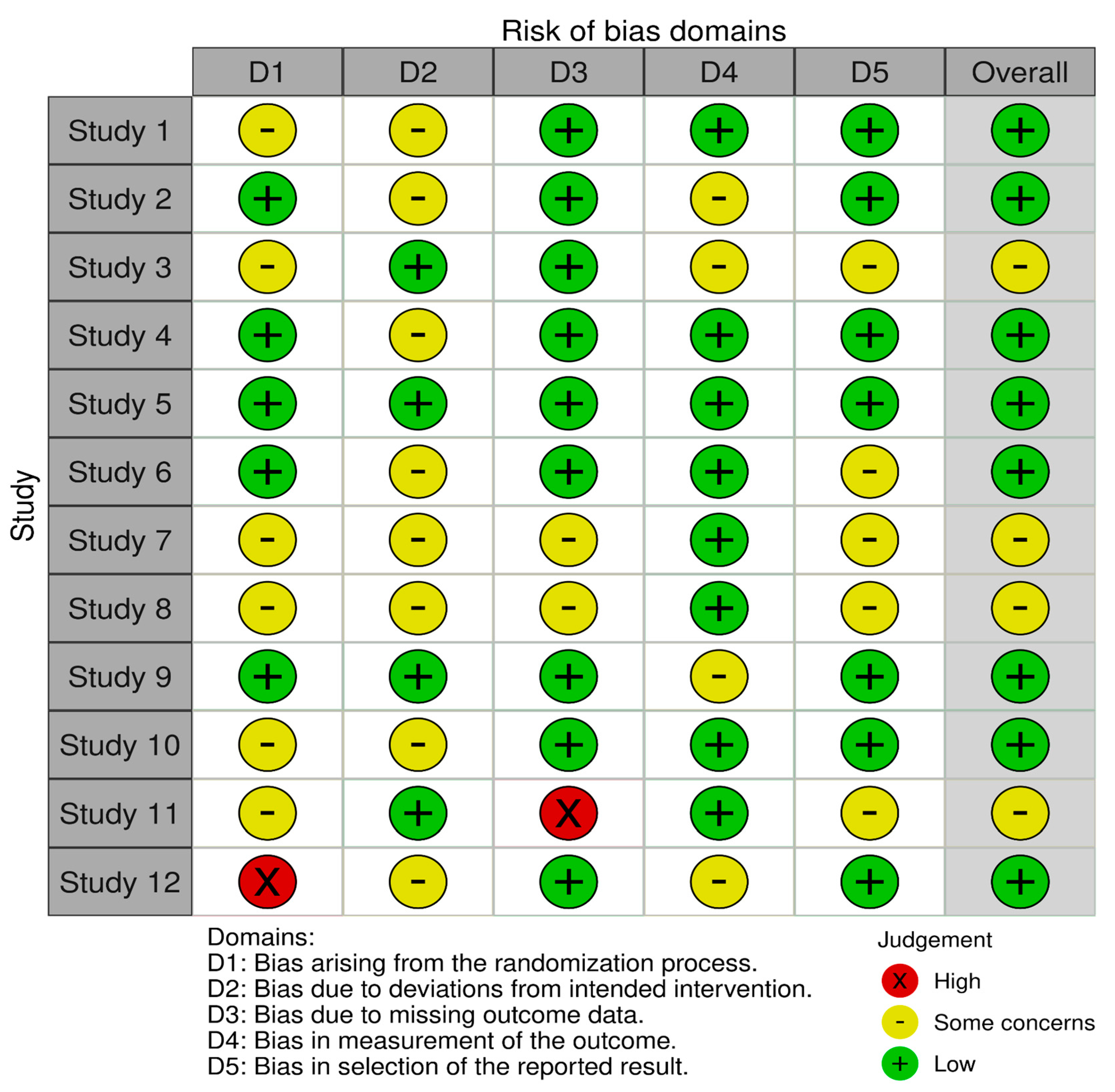
3.3. Risk of Bias in the Included Studies
3.4. Synthesis of the Results
3.4.1. Primary Outcome: LVEF
3.4.2. Secondary Outcomes: Efficacy
3.4.3. Secondary Outcome: Safety/MACE
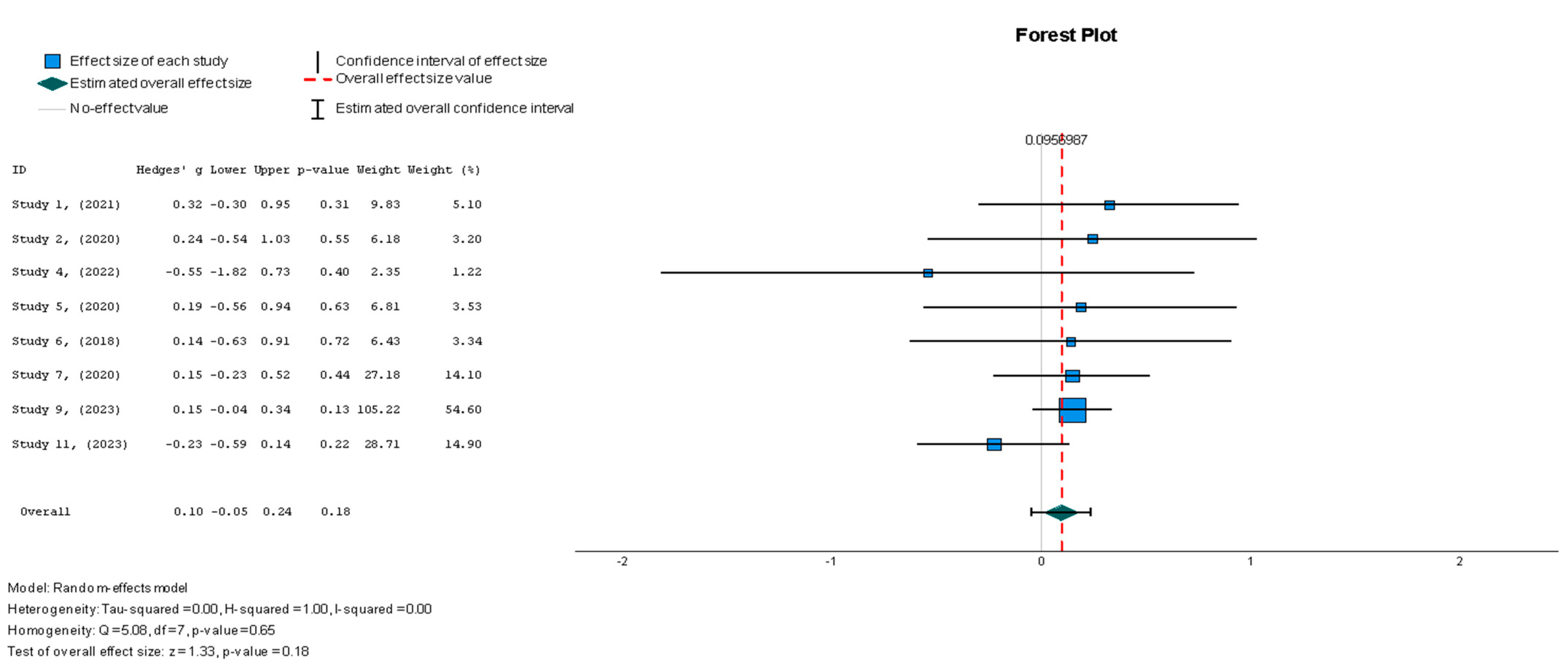
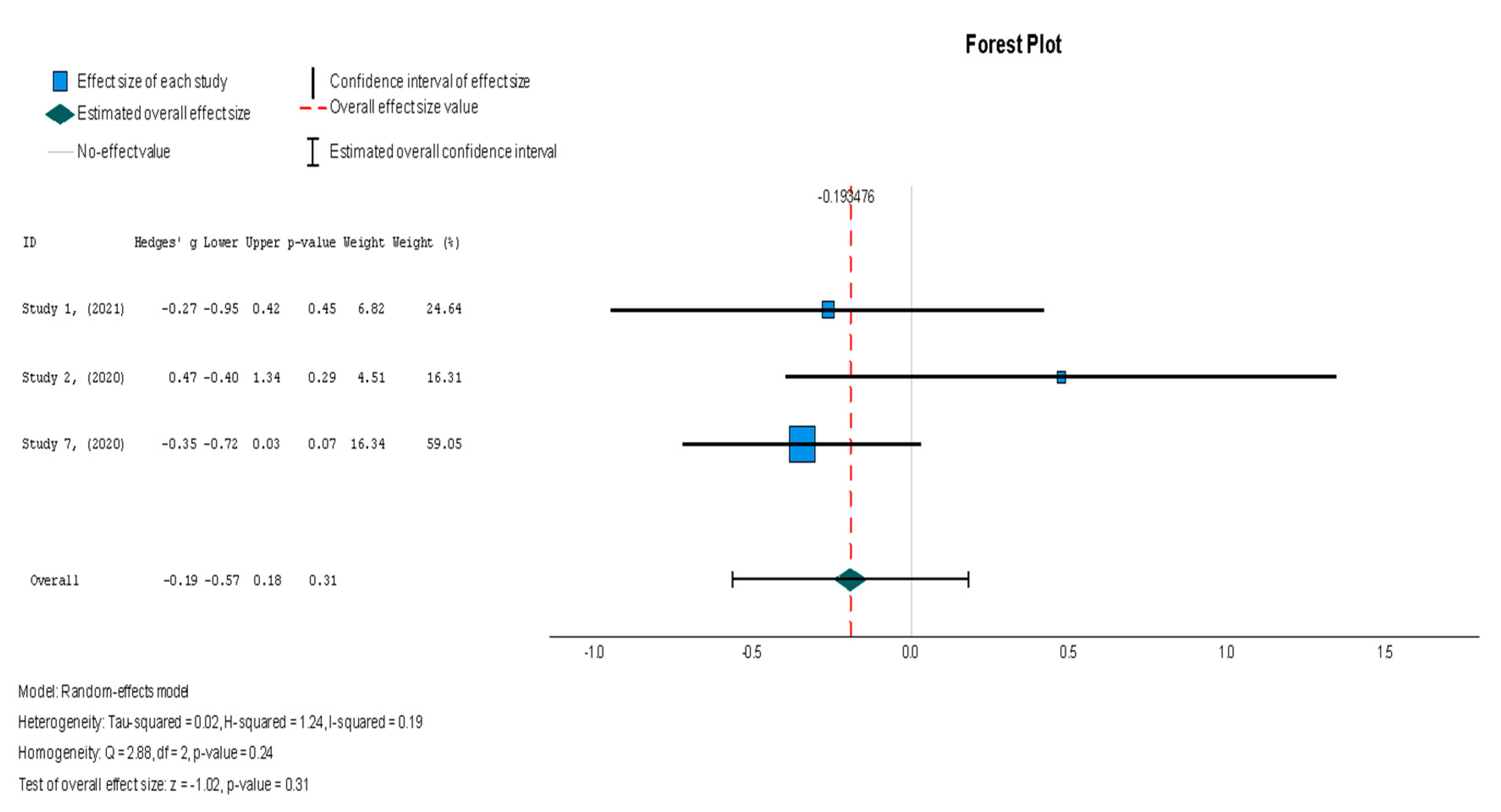
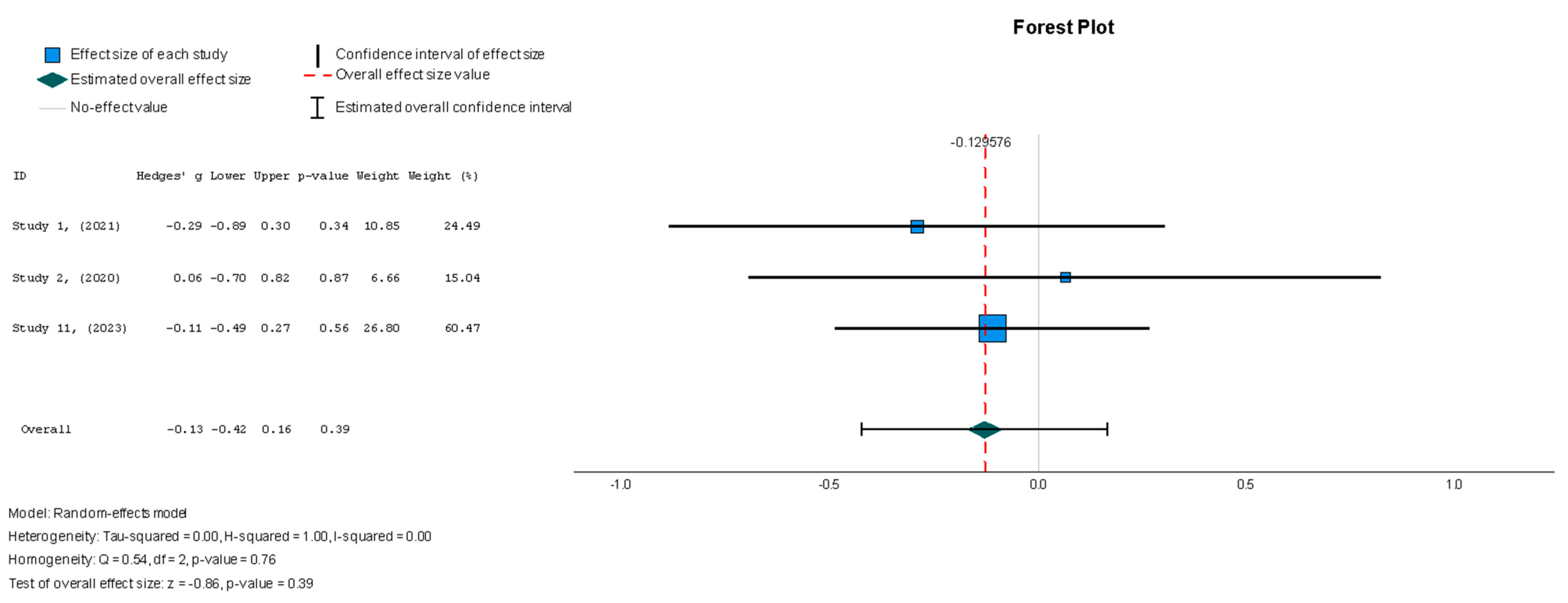
3.5. Meta-Analysis Findings
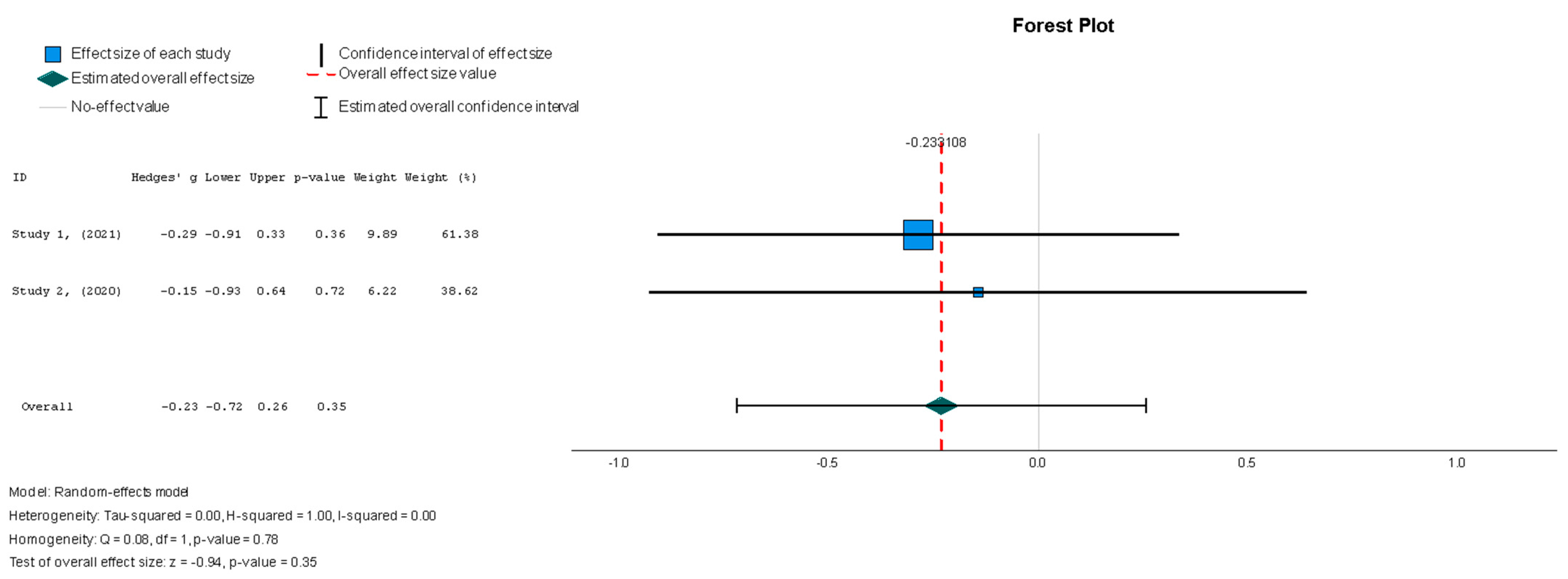
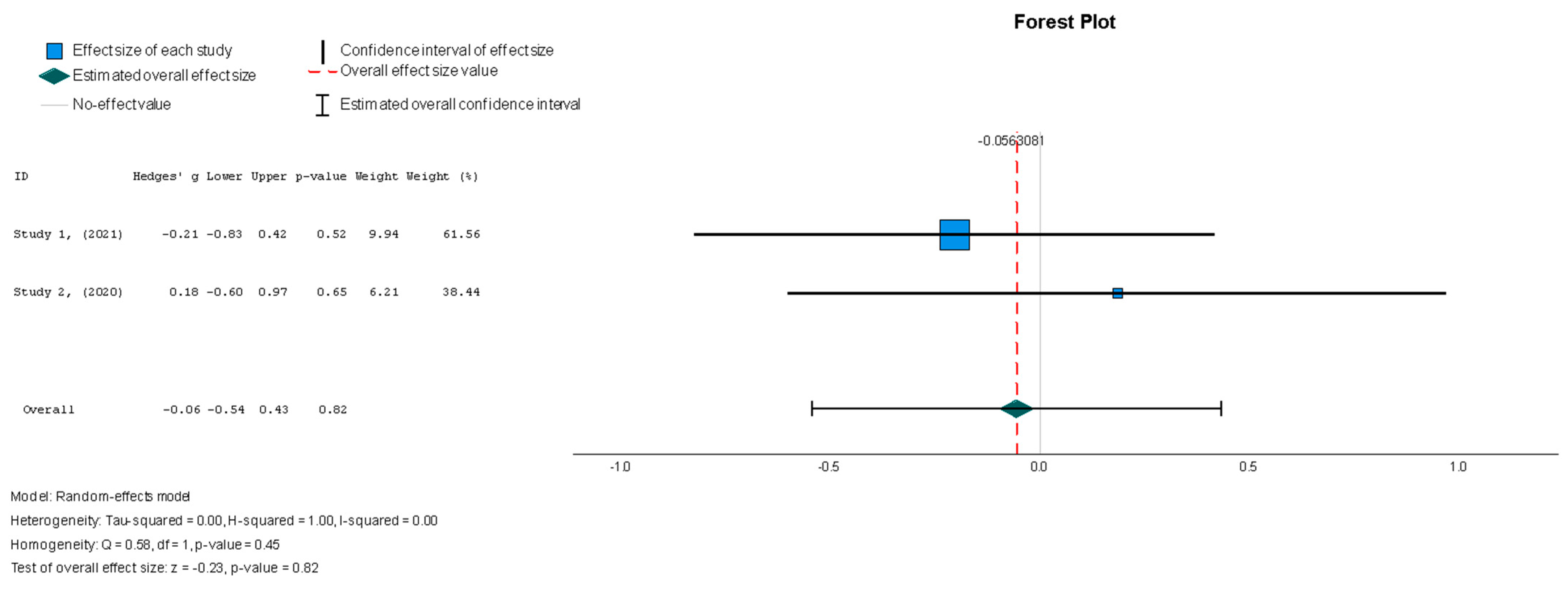
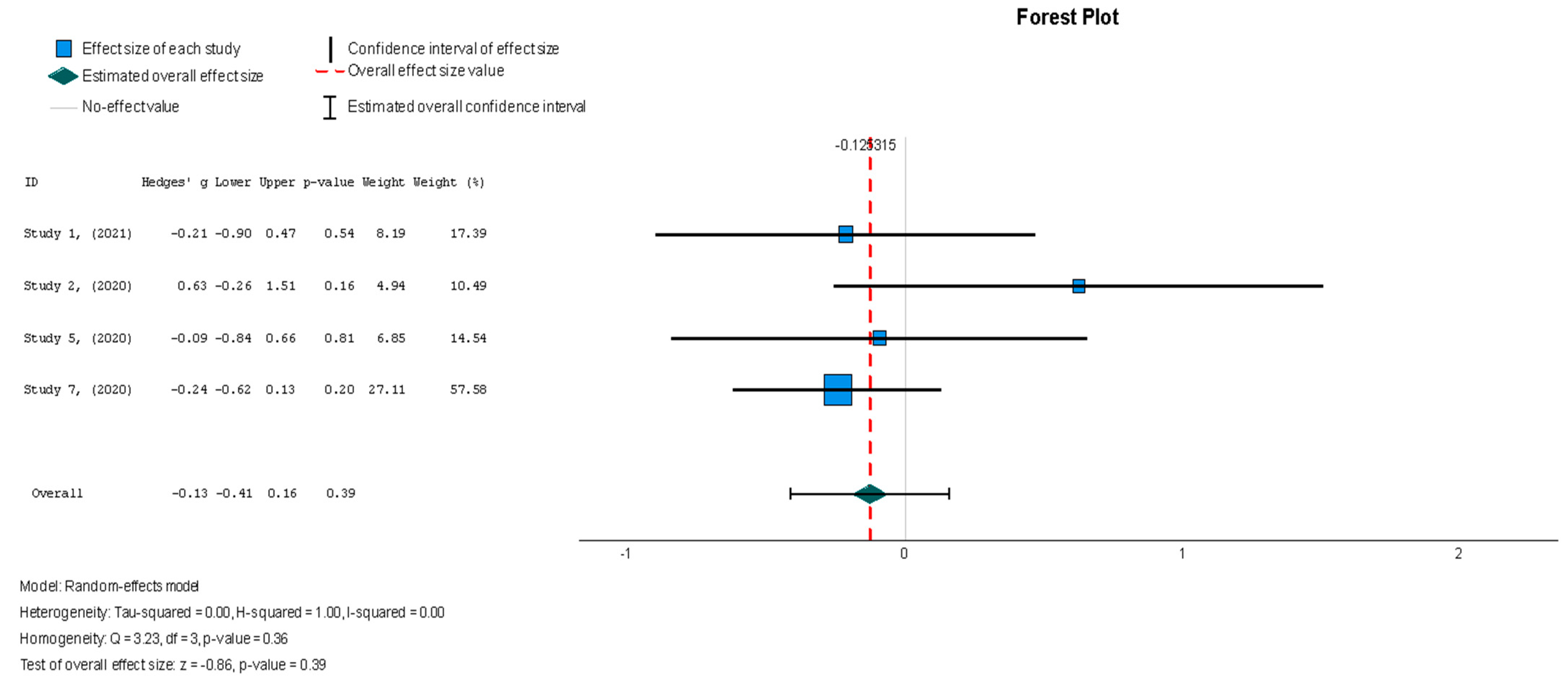
3.5.1. Statistical Analyses of Continuous Outcomes




3.5.2. Statistical Analyses of Binary Outcomes

4. Discussion
4.1. Summary of the Main Results
4.2. Agreements and Disagreements with Other Studies
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HF | heart failure |
| HFrEF | heart failure with reduced ejection fraction |
| HFpEF | heart failure with preserved ejection fraction |
| GDMT | guideline-directed medical therapy |
| SGLT2i | sodium–glucose cotransporter 2 inhibitors |
| ASCs | adult stem cells |
| MSCs | mesenchymal stem cells |
| BM-MSCs | bone-marrow-derived mesenchymal stem cells |
| UC-MSCs | umbilical cord-derived mesenchymal stem cells |
| LVEF | left ventricular ejection fraction |
| QoL | quality of life |
| AHA | American Heart Association |
| RCTs | randomized controlled trials |
| CPCs | cardiosphere-derived cells |
| MI | myocardial infarction |
| IC | intracoronary |
| IM | intramyocardial |
| MRI | magnetic resonance imaging |
| NYHA* | New York heart association |
| CABG** | coronary artery bypass graft |
| PCI*** | percutaneous coronary intervention |
| STEMI**** | ST-elevation myocardial infarction |
References
- Chen, Q.-F.; Chen, L.; Katsouras, C.S.; Liu, C.; Shi, J.; Liang, D.; Xiang, G.; Zhu, H.; Liao, H.; Lin, W.; et al. Global Burden of Heart Failure and Its Underlying Causes in 204 Countries and Territories, 1990–2021. Eur. Heart J.-Qual. Care Clin. Outcomes 2025, qcae110. [Google Scholar] [CrossRef] [PubMed]
- Shams, P.; Malik, A.; Chhabra, L. Heart failure (Congestive heart failure). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Universal Definition and Classification of Heart Failure: A Step in the Right Direction from Failure to Function. American College of Cardiology. Available online: https://www.acc.org/Latest-in-Cardiology/Articles/2021/07/12/12/31/Universal-Definition-and-Classification-of-Heart-Failure (accessed on 6 October 2024).
- Malgie, J.; Clephas, P.R.D.; Brunner-La Rocca, H.-P.; de Boer, R.A.; Brugts, J.J. Guideline-directed medical therapy for HFrEF: Sequencing strategies and barriers for life-saving drug therapy. Heart Fail. Rev. 2023, 28, 1221–1234. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Jain, V.; Minhas, A.M.K.; Morris, A.A.; Greene, S.J.; Pandey, A.; Khan, S.S.; Fonarow, G.C.; Mentz, R.J.; Butler, J.; Khan, M.S. Demographic and regional trends of heart failure-related mortality in young adults in the US, 1999–2019. JAMA Cardiol. 2022, 7, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, B.A.; Balkan, W.; Winkler, J.; Gyöngyösi, M.; Goliasch, G.; Fernández-Avilés, F.; Hare, J.M. Preclinical studies of stem cell therapy for heart disease. Circ. Res. 2018, 122, 1006–1020. [Google Scholar] [CrossRef]
- Zakrzewski, W.; Dobrzyński, M.; Szymonowicz, M.; Rybak, Z. Stem cells: Past, present, and future. Stem Cell Res. Ther. 2019, 10, 68. [Google Scholar] [CrossRef]
- Rheault-Henry, M.; White, I.; Grover, D.; Atoui, R. Stem cell therapy for heart failure: Medical breakthrough, or dead end? World J. Stem Cells 2021, 13, 236–259. [Google Scholar] [CrossRef] [PubMed]
- Almalki, S.G.; Agrawal, D.K. Key transcription factors in the differentiation of mesenchymal stem cells. Differentiation 2016, 92, 41–51. [Google Scholar] [CrossRef]
- Ullah, I.; Subbarao, R.B.; Rho, G.J. Human mesenchymal stem cells—Current trends and future prospective. Biosci. Rep. 2015, 35, e00191. [Google Scholar] [CrossRef]
- Gopalarethinam, J.; Nair, A.P.; Iyer, M.; Vellingiri, B.; Subramaniam, M.D. Advantages of mesenchymal stem cell over the other stem cells. Acta Histochem. 2023, 125, 152041. [Google Scholar] [CrossRef]
- Bolli, R.; Solankhi, M.; Tang, X.-L.; Kahlon, A. Cell therapy in patients with heart failure: A comprehensive review and emerging concepts. Cardiovasc. Res. 2022, 118, 951–976. [Google Scholar] [CrossRef] [PubMed]
- Mathiasen, A.B.; Qayyum, A.A.; Jørgensen, E.; Helqvist, S.; Fischer-Nielsen, A.; Kofoed, K.F.; Haack-Sørensen, M.; Ekblond, A.; Kastrup, J. Bone marrow-derived mesenchymal stromal cell treatment in patients with severe ischaemic heart failure: A randomized placebo-controlled trial (MSC-HF trial). Eur. Heart J. 2015, 36, 1744–1753. [Google Scholar] [CrossRef] [PubMed]
- Bartolucci, J.; Verdugo, F.J.; González, P.L.; Larrea, R.E.; Abarzua, E.; Goset, C.; Rojo, P.; Palma, I.; Lamich, R.; Pedreros, P.A.; et al. Safety and efficacy of the intravenous infusion of umbilical cord mesenchymal stem cells in patients with heart failure: A phase 1/2 randomized controlled trial (RIMECARD trial [randomized clinical trial of intravenous infusion umbilical cord mesenchymal stem cells on cardiopathy]): A phase 1/2 randomized controlled trial (RIMECARD trial [randomized clinical trial of intravenous infusion umbilical cord mesenchymal stem cells on cardiopathy]). Circ. Res. 2017, 121, 1192–1204. [Google Scholar]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar] [CrossRef]
- Sapna, F.; Raveena, F.; Chandio, M.; Bai, K.; Sayyar, M.; Varrassi, G.; Khatri, M.; Kumar, S.; Mohamad, T. Advancements in heart failure management: A comprehensive narrative review of emerging therapies. Cureus 2023, 15, e46486. [Google Scholar] [CrossRef] [PubMed]
- PRISMA Statement. Available online: https://www.prisma-statement.org (accessed on 22 October 2024).
- Makkar, R.R.; Kereiakes, D.J.; Aguirre, F.; Kowalchuk, G.; Chakravarty, T.; Malliaras, K.; Francis, G.S.; Povsic, T.J.; Schatz, R.; Traverse, J.H.; et al. Intracoronary ALLogeneic heart STem cells to Achieve myocardial Regeneration (ALLSTAR): A randomized, placebo-controlled, double-blinded trial. Eur. Heart J. 2020, 41, 3451–3458. [Google Scholar] [CrossRef]
- Marbán, E. Breakthroughs in cell therapy for heart disease: Focus on cardiosphere-derived cells. Mayo Clin. Proc. 2014, 89, 850–858. [Google Scholar] [CrossRef]
- Kosaraju, A.; Goyal, A.; Grigorova, Y.; Makaryus, A.N. Left Ventricular Ejection Fraction; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Rosen, B.D.; Lima, J.A.C. The prognostic value of global circumferential strain in patients with suspected myocardial disease. JACC Cardiovasc. Imaging 2015, 8, 550–552. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Spoletini, I.; Rosano, G. Monitoring functional capacity in heart failure. Eur. Heart J. Suppl. 2019, 21, M9–M12. [Google Scholar] [CrossRef]
- Bilbao, A.; Escobar, A.; García-Perez, L.; Navarro, G.; Quirós, R. The Minnesota living with heart failure questionnaire: Comparison of different factor structures. Health Qual. Life Outcomes 2016, 14, 23. [Google Scholar] [CrossRef]
- Giannitsi, S.; Bougiakli, M.; Bechlioulis, A.; Kotsia, A.; Michalis, L.K.; Naka, K.K. 6-minute walking test: A useful tool in the management of heart failure patients. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1753944719870084. [Google Scholar] [CrossRef]
- Konstam, M.A.; Kramer, D.G.; Patel, A.R.; Maron, M.S.; Udelson, J.E. Left ventricular remodeling in heart failure: Current concepts in clinical significance and assessment. JACC Cardiovasc. Imaging 2011, 4, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Richardson, W.J.; Clarke, S.A.; Quinn, T.A.; Holmes, J.W. Physiological implications of myocardial scar structure. Compr. Physiol. 2015, 5, 1877–1909. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, B.A.; Rieger, A.C.; Florea, V.; Banerjee, M.N.; Natsumeda, M.; Nigh, E.D.; Landin, A.M.; Rodriguez, G.M.; Hatzistergos, K.E.; Schulman, I.H.; et al. Comparison of mesenchymal stem cell efficacy in ischemic versus nonischemic Dilated Cardiomyopathy. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef]
- Lezaic, L.; Socan, A.; Poglajen, G.; Peitl, P.K.; Sever, M.; Cukjati, M.; Cernelc, P.; Wu, J.C.; Haddad, F.; Vrtovec, B. Intracoronary transplantation of CD34(+) cells is associated with improved myocardial perfusion in patients with nonischemic dilated cardiomyopathy. J. Card. Fail. 2015, 21, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Hamshere, S.; Arnous, S.; Choudhury, T.; Choudry, F.; Mozid, A.; Yeo, C.; Barrett, C.; Saunders, N.; Gulati, A.; Knight, C.; et al. Randomized trial of combination cytokine and adult autologous bone marrow progenitor cell administration in patients with non-ischaemic dilated cardiomyopathy: The REGENERATE-DCM clinical trial. Eur. Heart J. 2015, 36, 3061–3069. [Google Scholar] [CrossRef]
- Caroff, C. Elevated levels of gut microbiota dependent trimethylamine N-oxide: An indicator of cardiovascular disease. Hum. Microbiome J. 2021, 20, 100082. [Google Scholar] [CrossRef]
- RoB 2: A Revised Cochrane Risk-of-Bias Tool for Randomized Trials. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 6 October 2024).
- Fu, R.; Vandermeer, B.W.; Shamliyan, T.A.; O’Neil, M.E.; Yazdi, F.; Fox, S.H.; Morton, S.C. Handling continuous outcomes in quantitative synthesis. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. [Google Scholar]
- Gallis, J.A.; Turner, E.L. Relative measures of association for binary outcomes: Challenges and recommendations for the global health researcher. Ann. Glob. Health 2019, 85, 137. [Google Scholar] [CrossRef]
- 9.5.2 Identifying and Measuring Heterogeneity. Available online: https://handbook-5-1.cochrane.org/chapter_9/9_5_2_identifying_and_measuring_heterogeneity.htm (accessed on 6 October 2024).
- Covidence. Covidence—Better Systematic Review Management. Available online: https://www.covidence.org/reviews/328043 (accessed on 19 October 2024).
- Bolli, R.; Perin, E.C.; Willerson, J.T.; Yang, P.C.; Traverse, J.H.; Henry, T.D.; Pepine, C.J.; Mitrani, R.D.; Hare, J.M.; Murphy, M.P.; et al. Allogeneic mesenchymal cell therapy in anthracycline-induced cardiomyopathy heart failure patients: The CCTRN SENECA trial. JACC CardioOncol 2020, 2, 581–595. [Google Scholar] [CrossRef]
- Bolli, R.; Mitrani, R.D.; Hare, J.M.; Pepine, C.J.; Perin, E.C.; Willerson, J.T.; Traverse, J.H.; Henry, T.D.; Yang, P.C.; Murphy, M.P.; et al. A Phase II study of autologous mesenchymal stromal cells and c-kit positive cardiac cells, alone or in combination, in patients with ischaemic heart failure: The CCTRN CONCERT-HF trial. Eur. J. Heart Fail. 2021, 23, 661–674. [Google Scholar] [CrossRef]
- Mathiasen, A.B.; Qayyum, A.A.; Jørgensen, E.; Helqvist, S.; Kofoed, K.F.; Haack-Sørensen, M.; Ekblond, A.; Kastrup, J. Bone marrow-derived mesenchymal stromal cell treatment in patients with ischaemic heart failure: Final 4-year follow-up of the MSC-HF trial. Eur. J. Heart Fail. 2020, 22, 884–892. [Google Scholar] [CrossRef]
- Qayyum, A.A.; Mouridsen, M.; Nilsson, B.; Gustafsson, I.; Schou, M.; Nielsen, O.W.; Hove, J.D.; Mathiasen, A.B.; Jørgensen, E.; Helqvist, S.; et al. Danish phase II trial using adipose tissue derived mesenchymal stromal cells for patients with ischaemic heart failure. ESC Heart Fail. 2023, 10, 1170–1183. [Google Scholar] [CrossRef] [PubMed]
- Qayyum, A.A.; van Klarenbosch, B.; Frljak, S.; Cerar, A.; Poglajen, G.; Traxler-Weidenauer, D.; Nadrowski, P.; Paitazoglou, C.; Vrtovec, B.; Bergmann, M.W.; et al. Effect of allogeneic adipose tissue-derived mesenchymal stromal cell treatment in chronic ischaemic heart failure with reduced ejection fraction—The SCIENCE trial. Eur. J. Heart Fail. 2023, 25, 576–587. [Google Scholar] [CrossRef]
- Perin, E.C.; Borow, K.M.; Henry, T.D.; Mendelsohn, F.O.; Miller, L.W.; Swiggum, E.; Adler, E.D.; Chang, D.H.; Fish, R.D.; Bouchard, A.; et al. Randomized trial of targeted transendocardial mesenchymal precursor cell therapy in patients with heart failure. J. Am. Coll. Cardiol. 2023, 81, 849–863. [Google Scholar] [CrossRef]
- Drabik, L.; Mazurek, A.; Dzieciuch-Rojek, M.; Tekieli, L.; Czyż, Ł.; Kwiecień, E.; Kułaga, A.; Mikunda, A.; Chmiel, J.; Płazak, W.; et al. Trans-endocardial delivery of progenitor cells to compromised myocardium using the “needle techniqueänd risk of myocardial injury. Postep. Kardiol. Interwencyjnej 2022, 18, 423–430. [Google Scholar]
- He, X.; Wang, Q.; Zhao, Y.; Zhang, H.; Wang, B.; Pan, J.; Li, J.; Yu, H.; Wang, L.; Dai, J.; et al. Effect of intramyocardial grafting collagen scaffold with mesenchymal stromal cells in patients with chronic ischemic heart disease: A randomized clinical trial: A randomized clinical trial. JAMA Netw. Open 2020, 3, e2016236. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Cho, J.H.; Lee, Y.H.; Lee, J.H.; Kim, S.S.; Kim, M.Y.; Lee, M.G.; Kang, W.Y.; Lee, K.S.; Ahn, Y.K.; et al. Improvement in left ventricular function with intracoronary mesenchymal stem cell therapy in a patient with anterior wall ST-segment elevation myocardial infarction. Cardiovasc. Drugs Ther. 2018, 32, 329–338. [Google Scholar] [CrossRef]
- Sato, Y.; Kuragaichi, T.; Saga, S.; Nakayama, H.; Obata, T.; Watanabe, M.; Fujikura, K.; Watanabe, M.; Hata, K.-I.; Ohgushi, H. Safety of intravenous autologous bone marrow-derived mesenchymal cell transplantation in 5 patients with reduced left ventricular ejection fraction. Circ. Rep. 2021, 3, 550–554. [Google Scholar] [CrossRef]
- Domae, K.; Miyagawa, S.; Yoshikawa, Y.; Fukushima, S.; Hata, H.; Saito, S.; Kainuma, S.; Kashiyama, N.; Iseoka, H.; Ito, E.; et al. Clinical outcomes of autologous stem cell-patch implantation for patients with heart failure with nonischemic dilated cardiomyopathy. J. Am. Heart Assoc. 2021, 10, e008649. [Google Scholar] [CrossRef]
- Borenstein, M. How to understand and report heterogeneity in a meta-analysis: The difference between I-squared and prediction intervals. Integr. Med. Res. 2023, 12, 101014. [Google Scholar] [CrossRef]
- Jayaraj, J.S.; Janapala, R.N.; Qaseem, A.; Usman, N.; Fathima, N.; Kashif, T.; Reddy, V.K.; Bakshi, S. Efficacy and safety of stem cell therapy in advanced heart failure patients: A systematic review with a meta-analysis of recent trials between 2017 and 2019. Cureus 2019, 11, e5585. [Google Scholar] [CrossRef] [PubMed]
- Kalou, Y.; Al-Khani, A.M.; Haider, K.H. Bone marrow mesenchymal stem cells for heart failure treatment: A systematic review and meta-analysis. Heart Lung Circ. 2023, 32, 870–880. [Google Scholar] [CrossRef]
- Afzal, M.R.; Samanta, A.; Shah, Z.I.; Jeevanantham, V.; Abdel-Latif, A.; Zuba-Surma, E.K.; Dawn, B. Adult bone marrow cell therapy for ischemic heart disease: Evidence and insights from randomized controlled trials. Circ. Res. 2015, 117, 558–575. [Google Scholar] [CrossRef] [PubMed]
- Krishna Mohan, G.V.; Tirumandyam, G.; Vemulapalli, H.S.; Vajje, J.; Asif, H.; Saleem, F. Mesenchymal stem cell therapy for a better prognosis of heart failure: A systematic review and meta-analysis of randomized controlled trials. Cureus 2023, 15, e43037. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Chen, Q. Mesenchymal stem cell therapy for heart failure: A meta-analysis. Herz 2020, 45, 557–563. [Google Scholar] [CrossRef]
- Fan, M.; Huang, Y.; Chen, Z.; Xia, Y.; Chen, A.; Lu, D.; Wu, Y.; Zhang, N.; Qian, J. Efficacy of mesenchymal stem cell therapy in systolic heart failure: A systematic review and meta-analysis. Stem Cell Res. Ther. 2019, 10, 150. [Google Scholar] [CrossRef]
- Golpanian, S.; Wolf, A.; Hatzistergos, K.E.; Hare, J.M. Rebuilding the damaged heart: Mesenchymal stem cells, Cell-Based therapy, and engineered heart tissue. Physiol. Rev. 2016, 96, 1127–1168. [Google Scholar] [CrossRef]
- Cashman, T.J.; Gouon-Evans, V.; Costa, K.D. Mesenchymal stem cells for cardiac therapy: Practical challenges and potential mechanisms. Stem Cell Rev. Rep. 2012, 9, 254–265. [Google Scholar] [CrossRef]
- White, S.J.; Chong, J.J.H. Mesenchymal stem cells in cardiac repair: Effects on myocytes, vasculature, and fibroblasts. Clin. Ther. 2020, 42, 1880–1891. [Google Scholar] [CrossRef]
- Neuber, S.; Emmert, M.Y.; Nazari-Shafti, T.Z. Hopes and hurdles of employing mesenchymal stromal cells in the treatment of cardiac fibrosis. Int. J. Mol. Sci. 2021, 22, 13000. [Google Scholar] [CrossRef]
- Huang, Y.; Wu, Q.; Tam, P.K.H. Immunomodulatory mechanisms of mesenchymal stem cells and their potential clinical applications. Int. J. Mol. Sci. 2022, 23, 10023. [Google Scholar] [CrossRef] [PubMed]
- Hanna, A.; Frangogiannis, N.G. Inflammatory cytokines and chemokines as therapeutic targets in heart failure. Cardiovasc. Drugs Ther. 2020, 34, 849–863. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S.A.; Doree, C.; Mathur, A.; Taggart, D.P.; Martin-Rendon, E. Stem cell therapy for chronic ischaemic heart disease and congestive heart failure. Cochrane Database Syst. Rev. 2016, 12, CD007888. [Google Scholar] [CrossRef] [PubMed]
- Brunskill, S.J.; Hyde, C.J.; Doree, C.J.; Watt, S.M.; Martin-Rendon, E. Route of delivery and baseline left ventricular ejection fraction, key factors of bone-marrow-derived cell therapy for ischaemic heart disease. Eur. J. Heart Fail. 2009, 11, 887–896. [Google Scholar] [CrossRef]
- Ahmed, Z.T.; Zain Al-Abeden, M.S.; Al Abdin, M.G.; Muqresh, M.A.; Al Jowf, G.I.; Eijssen, L.M.T.; Haider, K.H. Dose-response relationship of MSCs as living Bio-drugs in HFrEF patients: A systematic review and meta-analysis of RCTs. Stem Cell Res. Ther. 2024, 15, 165. [Google Scholar] [CrossRef]
- Gyöngyösi, M.; Haller, P.M.; Blake, D.J.; Martin Rendon, E. Meta-Analysis of Cell Therapy Studies in Heart Failure and Acute Myocardial Infarction. Circ. Res. 2018, 123, 301–308. [Google Scholar] [CrossRef]
- Wang, W.; Han, Z.C. Heterogeneity of human mesenchymal Stromal/Stem cells. Adv. Exp. Med. Biol. 2019, 165–177. [Google Scholar] [CrossRef]
- Lee, H.; Cho, H.-J.; Han, Y.; Lee, S.H. Mid- to long-term efficacy and safety of stem cell therapy for acute myocardial infarction: A systematic review and meta-analysis. Stem Cell Res. Ther. 2024, 15, 290. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms |
|---|---|
| PubMed | “Heart Failure”[Mesh] OR “Cardiac Failure”[tw] “Heart Failure, Systolic”[Mesh] OR “Systolic Heart Failure”[tw] OR “Adult Stem Cells”[Mesh] OR “Adult Stem Cell”[tw] OR “Stem Cell Research”[Mesh] OR “Stem cell therapy”[tw] OR “Stem cell”[tw] OR “Mesenchymal stem cell therapy”[tw] AND “Ventricular Function, Left”[Mesh] |
| Scopus | TITLE-ABS-KEY (heart AND failure OR cardiac AND failure OR systolic AND heart AND failure AND stem AND cell OR stem AND cell AND therapy OR mesenchymal AND stem AND cell AND left AND ventricular AND function) AND (INDEXTERMS (“clinical trials” OR “clinical trials as a topic” OR “randomized controlled trial” OR “Randomized Controlled Trials as Topic” OR “controlled clinical trial” OR “Controlled Clinical Trials” OR “random allocation” OR “Double-Blind Method” OR “Single-Blind Method” OR “Cross-Over Studies” OR “Placebos” OR “multicenter study” OR “double blind procedure” OR “single blind procedure” OR “crossover procedure” OR “clinical trial” OR “controlled study” OR “randomization” OR “placebo”)) AND (LIMIT-TO (OA, “all”)) AND (LIMIT-TO (DOCTYPE, “ar”)) AND (LIMIT-TO (PUBYEAR, 202) OR LIMIT-TO (PUBYEAR, 2022) OR LIMIT-TO (PUBYEAR, 2021) OR LIMIT-TO (PUBYEAR, 2020) OR LIMIT-TO (PUBYEAR, 2019) OR LIMIT-TO (PUBYEAR, 2018)) AND (LIMIT-TO (LANGUAGE, “English”)) |
| EBSCO Medline | Heart Failure AND Stem cells AND left ventricular ejection fraction |
| EBSCO CINAHL | Heart Failure AND Stem cells AND left ventricular ejection fraction |
| Cochrane Library | Stem cell therapy AND Heart Failure AND Left Ventricular Function |
| ScienceDirect | Heart failure AND mesenchymal stem cell therapy AND left ventricular ejection fraction |
| Study No. | Author, Year | Study Type | Number of Participants (MSC Group/Control Group) | Mean Age of Participants (MSC Group/Control Group) | Mean LVEF at Baseline (MSC Group/Control Group) | NYHA* Class III and IV (MSC Group/Control Group) | Method of Stem Cell Delivery | Control Group | Type of MSC | Patient Population | Follow-Up Time |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bolli, Roberto et al. (2021) [38] | Phase 2, randomized, placebo-controlled study with parallel assignment and quadruple masking | 125 | 62.5 | 28.6 ± 6.1 | 80% NYHA class 2, 15% NYHA class 3 | Transendocardial injection | Placebo | Autologous BM- MSCs | EF ≤ 40% on optimal GDMT | 12 months |
| 2 | Bolli, Roberto et al. (2020) [37] | Phase I, randomized, placebo-controlled trial with quadruple masking | 37 | 56.6 ± 11.8 | 33 ± 5.3% | 84% NYHA class 2 | Intramyocardial injections | Placebo | Allogeneic MSCs | EF ≤ 45% on optimal GDMT | 12 months |
| 3 | Domae, Keitaro et al. (2021) [47] | Open-label single-arm interventional study | 24 | 53.5 ± 2.6 | - | 33.3% NYHA class 2, 62.5% NYHA class 3 | Stem cell patch implantation | - | Autologous skeletal stem cells | EF < 35% on optimal medical treatment | 47.5 ± 4.3 months |
| 4 | Drabik, Leszek et al. (2022) [43] | Randomized control trial | 10 | 60.8 ± 7.1 | 22.8 ± 4.5 CSCs, 27.8 ± 5.8 sham | - | Transendocardial injection | Sham procedure | Autologous BM- MSCs, cultured to form cardiopoietic stem cells | - | 30 days |
| 5 | He, Xiaojun et al. (2020) [44] | Randomized double-blind clinical trial | 50 | 62.6 ± 8.3 | 29.63% ± 6.03% in MSCs; 27.98% ± 7.39 in control | 50% NYHA class 3 and 50% NYHA class 4 in MSCs; 58.3% NYHA class 3 and 41.7% NYHA class 4 in control | Intramyocardial injections while undergoing CABG** | CABG alone | Homologous, allogeneic UC-MSCs | LVEF ≤ 40% | 12 months |
| 6 | Kim, Su Hyun et al. (2018) [45] | Randomized controlled trial | 26 | 55.3 ± 8.6 in MSCs; 57.8 ± 8.9 in control | 35.1 ± 4.5 in MSCs; 37.4 ± 1.7 in control | - | Intracoronary infusion after 30 days from PCI*** | No sham procedure | Autologous BM-derived MSCs | LVEF ≤ 40% in patients who underwent PCI for a STEMI**** | 12 months |
| 7 | Makkar, Raj R et al. (2020) [19] | Multicenter randomized double-blind placebo-controlled trial | 142 | 55 ± 11 in CDCs; 54 ± 10 in control | 39.9 ± 6.6 in CDCs; 38.8 ± 8.2 in control | 43.3% class 2 and 1.1% class 3 in CDCs; 52.3% class 2 and 11.4% class 3 in control | Intracoronary infusion | Intracoronary infusion of placebo | Allogeneic cardiosphere-derived cells (CAP-1002) | LVEF ≤ 40% with prior MI | 12 months |
| 8 | Mathiasen, Anders B et al. (2020) [39] | Phase II, single-center, randomized, double-blind, placebo-controlled trial | 60 | 66.1 ± 7.7 in MSCs; 64.2 ± 10.6 in control | - | 27.5% class 2 and 72.5% class 3 in MSCs; 25.0% class 2 and 75.0% class 3 in control | intramyocardial injections | Intramyocardial injections of placebo (saline) | Autologous BM-MSCs | Ischemic HF with LVEF ≤ 45% | 4 years |
| 9 | Perin, Emerson C et al. (2023) [42] | Phase 3, multinational, randomized, double-blind, sham-controlled clinical trial | 565 | 62.7 ± 10.9 in MSCs; 62.7 ± 10.9 in control | 28.6 ± 6.7 in MSCs; 28.6 ± 6.9 in control | 38.2% class 2 and 61.8 class 3 in MSCs; 36.9% class 2 and 63.1% class 4 in control | Transendocardial injections | Sham control procedure | Allogeneic bone-marrow-derived mesenchymal precursor cells | LVEF ≤ 40% | 12 months |
| 10 | Qayyum, Abbas Ali et al. (2023) [40] | Multi-center, double-blind, placebo-controlled phase II study | 81 | 67.0 ± 9.0 in ASCs; 66.6 ± 8.1 in control | 34.2 ± 7.9 in ASCs; 31.4 ± 7.2 in control | Mean NYHA class 2.2 ± 0.4 in ASCs and 2.3 ± 0.4 in control | Intramyocardial injections | Placebo (saline) injection | Allogenic adipose-tissue-derived mesenchymal Stromal cells | LVEF ≤ 45% | 12 months |
| 11 | Qayyum, Abbas Ali et al. (2023) [41] | Multicenter, double-blind, placebo-controlled phase II trial | 133 | 66.4 ± 8.1 in ASCs; 64.0 ± 8.8 in control | 31.6 ± 7.2 in ASCs; 32.0 ± 8.9 in control | 68.9% class 2 and 31.1% class 3 in ASCs; 69.8% class 2 and 30.2% class 3 in control | Intramyocardial injections | Placebo (saline) injection | Allogenic adipose-tissue-derived mesenchymal stromal cells | LVEF ≤ 45% | 12 months |
| 12 | Sato, Yukihito et al. (2021) [46] | Preliminary, interventional, single-arm, open-label study | 5 | 70.0 ± 4.0 | 29.2 ± 7.6 | - | Intravenous infusion | Autologous BM- MSCs | LVEF ≤ 45% | 6 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muslem, S.; AlTurani, M.; Maqsood, M.B.; Qaseer, M.A. Cardiac Repair and Clinical Outcomes of Stem Cell Therapy in Heart Failure: A Systematic Review and Meta-Analysis. Diseases 2025, 13, 136. https://doi.org/10.3390/diseases13050136
Muslem S, AlTurani M, Maqsood MB, Qaseer MA. Cardiac Repair and Clinical Outcomes of Stem Cell Therapy in Heart Failure: A Systematic Review and Meta-Analysis. Diseases. 2025; 13(5):136. https://doi.org/10.3390/diseases13050136
Chicago/Turabian StyleMuslem, Salman, Mariam AlTurani, Muhammad Bilal Maqsood, and Maryam Al Qaseer. 2025. "Cardiac Repair and Clinical Outcomes of Stem Cell Therapy in Heart Failure: A Systematic Review and Meta-Analysis" Diseases 13, no. 5: 136. https://doi.org/10.3390/diseases13050136
APA StyleMuslem, S., AlTurani, M., Maqsood, M. B., & Qaseer, M. A. (2025). Cardiac Repair and Clinical Outcomes of Stem Cell Therapy in Heart Failure: A Systematic Review and Meta-Analysis. Diseases, 13(5), 136. https://doi.org/10.3390/diseases13050136