
Unmasking the Hidden Morbidity of Ocular Diseases in Primary Care Through a Collaboration with Specialists in Remote Areas: A Cross-Sectional Study from Rural Crete, Greece

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Data Collection and Tools
2.4. Ethics Approval
2.5. Statistical Analysis
3. Results
3.1. Demographics
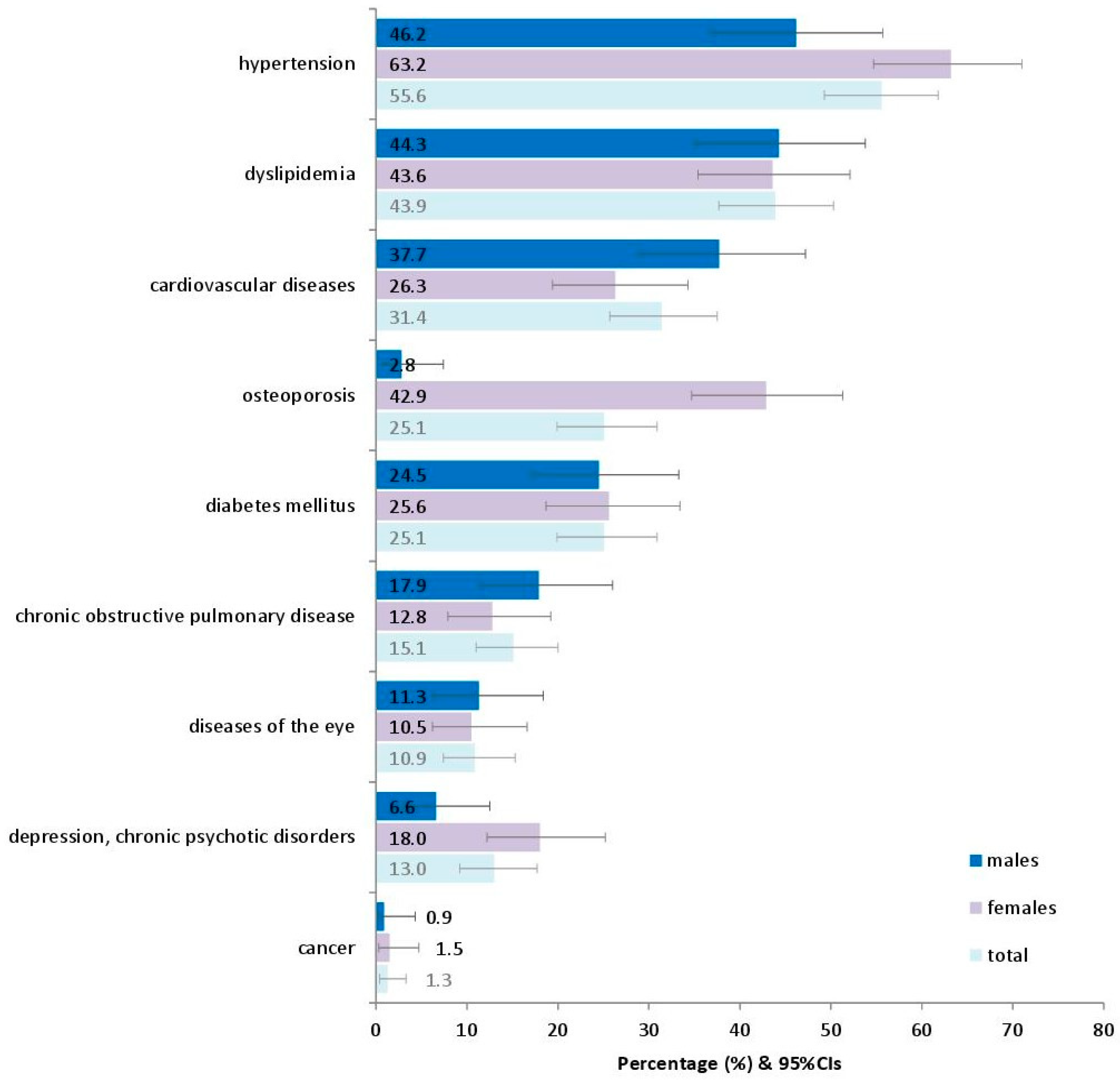
3.2. The Most Frequent Diagnoses
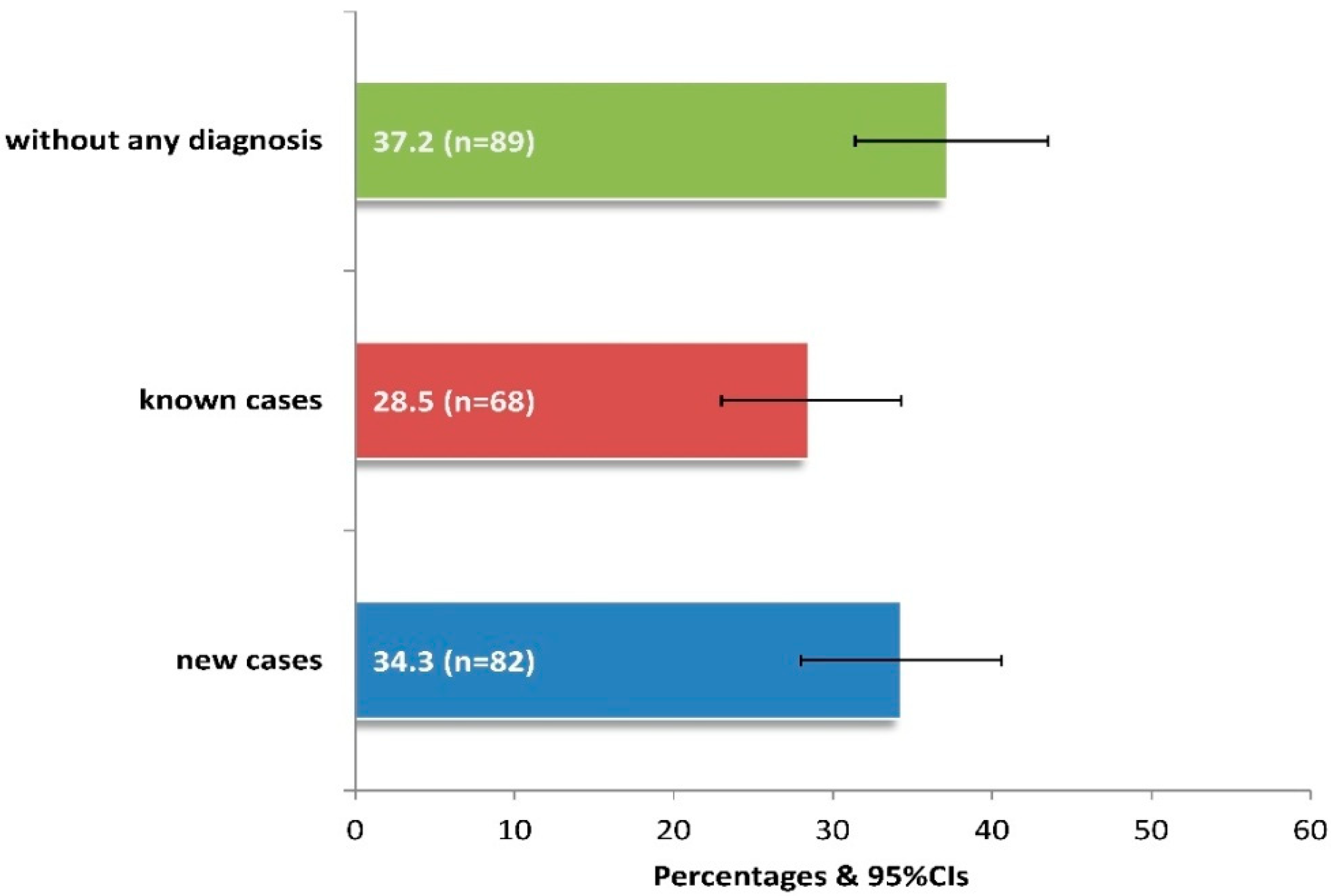
3.3. Hidden Morbidity
3.4. National Eye Institute Visual Function Questionnaire (NEI VFQ-25) Scoring
4. Discussion
4.1. Main Findings
4.2. Discussion of the Study Findings in Light of the Literature
4.3. Study Limitations and Strengths
4.4. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | Corona Virus Disease 2019 |
| CVD | Cardio Vascular Diseases |
| GPs | General Practitioners |
| ICD-10 | International Classification of Diseases-Tenth Revision |
| LSD | Least Significant Difference |
| NEI VFQ-25 | National Eye Institute Visual Function Questionnaire-25 |
| PHC | Primary Healthcare |
| QoL | Quality of Life |
| VI | Visual Impairment |
| VRQoL | Vision-Related Quality of Life |
| VS-QoL | Vision-SpecificQuality of Life |
| WHO | World Health Organization |
References
- World Health Organization. Regional Office for Europe. From Alma-Ata to Astana: Primary Health Care: Reflecting on the Past, Transforming for the Future: Interim Report from the WHO European Region. 2018. Available online: https://iris.who.int/handle/10665/345685 (accessed on 4 December 2024).
- Hartley, D. Rural Health Disparities, Population Health and Rural Culture. Am. J. Public Health 2004, 94, 1675–1678. [Google Scholar] [CrossRef] [PubMed]
- Nunes, F.G.D.S.; Santos, A.M.D.; Carneiro, A.O.; Fausto, M.C.R.; Cabral, L.M.D.S.; Almeida, P.F. Challenges to the provision of specialized care in remote rural municipalities in Brazil. BMC Health Serv. Res. 2022, 22, 1386. [Google Scholar] [CrossRef] [PubMed]
- Latorre-Arteaga, S.; Fernandez-Saez, J.; Gil-Gonzalez, D. Inequities in visual health and health services use in a rural region in Spain. Gac. Sanit. 2018, 32, 439–446. [Google Scholar] [CrossRef]
- Morka, E.D.; Yibekal, B.T.; Tegegne, M.M. Eye care service utilization and associated factors among older adults in Hawassa city, South Ethiopia. PLoS ONE 2020, 15, e0231616. [Google Scholar] [CrossRef]
- Gizaw, Z.; Astale, T.; Kassie, G.M. What improves access to primary healthcare services in rural communities? A systematic review. BMC Prim. Care 2022, 23, 313. [Google Scholar] [CrossRef] [PubMed]
- Stevelink, S.A.; Malcolm, E.M.; Fear, N.T. Visual impairment, coping strategies and impact on daily life: A qualitative study among working-age UK ex-service personnel. BMC Public Health 2015, 15, 1118. [Google Scholar] [CrossRef]
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Zou, M.; Guo, D.; Chen, A.; Young, C.A.; Li, Y.; Zheng, D.; Jin, G. Prevalence of visual impairment among older Chinese population: A systematic review and meta-analysis. J. Glob. Health 2021, 11, 08004. [Google Scholar] [CrossRef]
- Xulu-Kasaba, Z.N.; Kalinda, C. Prevalence of the Burden of Diseases Causing Visual Impairment and Blindness in South Africa in the Period 2010–2020: A Systematic Scoping Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 34. [Google Scholar] [CrossRef]
- Klein, R.; Klein, B.E. The prevalence of age-related eye diseases and visual impairment in aging: Current estimates. Investig. Ophthalmol. Vis. Sci. 2013, 54, ORSF5–ORSF13. [Google Scholar] [CrossRef]
- Baldev, V.F.; Chopra, R.; Batra, N.; Singh, S. Pattern of Ocular Morbidity in the Elderly Population of Northern India. J. Clin. Diagn. Res. 2017, 11, NC20–NC23. [Google Scholar] [CrossRef]
- Syriga, M.; Karampela, Ι.; Dalamaga, Μ.; Karampelas, M. The effect of COVID-19 pandemic on the attendance and clinical outcomes of patients with ophthalmic disease: A mini-review. Metab. Open 2021, 12, 100131. [Google Scholar] [CrossRef]
- Hacker, K.A.; Briss, P.A.; Richardson, L.; Wright, J.; Petersen, R. COVID-19 and Chronic Disease: The Impact Now and in the Future. Prev. Chronic Dis. 2021, 18, E62. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, J.R.; Stagg, B.C.; Andrews, C.; Kumagai, A.; Musch, D.C. Vision Impairment and Receipt of Eye Care among Older Adults in Low- and Middle-Income Countries. JAMA Ophthalmol. 2019, 137, 146–158. [Google Scholar] [CrossRef]
- Gruen, R.L.; Bailie, R.S.; Wang, Z.; Heard, S.; O’Rourke, I.C. Specialist outreach to isolated and disadvantaged communities: A population-based study. Lancet 2006, 368, 130–138. [Google Scholar] [CrossRef]
- Jadoon, M.Z.; Dineen, B.; Bourne, R.R.; Shah, S.P.; Khan, M.A.; Johnson, G.J.; Gilbert, C.E.; Khan, M.D. Prevalence of Blindness and Visual Impairment in Pakistan: The Pakistan National Blindness and Visual Impairment Survey. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4749. [Google Scholar] [CrossRef]
- Touloumi, G.; Karakosta, A.; Kalpourtzi, N.; Gavana, M.; Vantarakis, A.; Kantzanou, M.; Hajichristodoulou, C.; Chlouverakis, G.; Trypsianis, G.; Voulgari, P.V.; et al. High prevalence of cardiovascular risk factors in adults living in Greece: The EMENO National Health Examination Survey. BMC Public Health 2020, 20, 1665. [Google Scholar] [CrossRef]
- Tsiligianni, I. Respiratory health in Greece. Lancet Respir. Med. 2020, 8, e65–e66. [Google Scholar] [CrossRef]
- Pistolla, G.; Tsilimparis, M.K.; Prastacos, P.; Sifaki-Pistolla, D.; Philalithis, A.; Pallikaris, I.G. Ophthalmological disorders in rural areas of Crete: A geospatial analysis. Rural Remote Health 2013, 13, 2020. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, E.; Zoli, M.; Gonzalez-Freire, M.; Salive, M.E.; Studenski, S.A.; Ferrucci, L. Aging and Multimorbidity: New Tasks, Priorities, and Frontiers for Integrated Gerontological and Clinical Research. J. Am. Med. Dir. Assoc. 2015, 16, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.; Monnat, S.M.; Green, J.J.; Hunter, L.M.; Sliwinski, M.J. Rural Population Health and Aging: Toward a Multilevel and Multidimensional Research Agenda for the 2020s. Am. J. Public Health 2020, 110, 1328–1331. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.D.; Christ, S.L.; Lam, B.L.; Feaster, D.J.; McCollister, K.; Lee, D.J. Patterns of Chronic Conditions and Their Association with Visual Impairment and Health Care Use. JAMA Ophthalmol. 2020, 138, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Assi, L.; Chamseddine, F.; Ibrahim, P.; Sabbagh, A.; Rosman, L.; Congdon, N.; Evans, J.; Ramke, J.; Kuper, H.; Burton, M.J.; et al. A Global Assessment of Eye Health and Quality of Life. A Systematic Review of Systematic Reviews. JAMA Ophthalmol. 2021, 139, 526–541. [Google Scholar] [CrossRef] [PubMed]
- Owsley, C.; McGwin, G., Jr. Depression and the 25-item National. Eye Institute Visual Function Questionnaire in older adults. Ophthalmology 2004, 111, 2259–2264. [Google Scholar] [CrossRef]
- Labiris, G.; Katsanos, A.; Fanariotis, M.; Zacharaki, F.; Chatzoulis, D.; Kozobolis, V.P. Vision-specific quality of life in Greek glaucoma patients. J. Glaucoma 2010, 19, 39–43. [Google Scholar] [CrossRef]
- Tsilimbaris, M.K.; Kontadakis, G.; Tsika, C.; Papageorgiou, D.; Charoniti, M. Effect of Panretinal Photocoagulation Treatment on Vision-Related Quality of Life of Patients with Proliferative Diabetic Retinopathy. Retina 2013, 33, 756–761. [Google Scholar] [CrossRef]
- Köberlein, J.; Beifus, C.; Schaffert, C.; Finger, R.P. The economic burden of visual impairment and blindness: A systematic review. BMJ Open 2013, 3, e003471. [Google Scholar] [CrossRef]
- Lionis, C.; Tedeschi, P.; Saridaki, A. 11 Greece. In Building Primary Care in a Changing Europe: Case Studies [Internet]; Kringos, D.S., Boerma, W.G.W., Hutchinson, A., Saltman, R.B., Eds.; European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459023/ (accessed on 3 February 2025).
- Tountas, Y.; Karnaki, P.; Pavi, E.; Souliotis, K. The “unexpected” growth of the private health sector in Greece. Health Policy 2005, 74, 167–180. [Google Scholar] [CrossRef]
- Lionis, C.; Symvoulakis, E.K.; Markaki, A.; Petelos, E.; Papadakis, S.; Sifaki-Pistolla, D.; Papadakakis, M.; Souliotis, K.; Tziraki, C. Integrated people-centred primary health care in Greece: Unravelling Ariadne’s thread. Prim. Health Care Res. Dev. 2019, 20, e113. [Google Scholar] [CrossRef]
- Marinos, G.; Vasileiou, I.; Katsargyris, A.; Klonaris, C.P.; Korombelis, P.; Michail, O.; Valatsou, A.; Griniatsos, J.; Vlasis, K.; Siasos, G.; et al. Management of minor medical problems and trauma: The role of general practice. Rural Remote Health 2009, 9, 1019. [Google Scholar] [CrossRef]
- Merga, H.; Amanuel, D.; Fekadu, L.; Dube, L. A community-based cross-sectional study of eye care service utilization among the adult population in southern Ethiopia. Sage Open Med. 2023, 11, 20503121231197865. [Google Scholar] [CrossRef] [PubMed]
- Micheletti, J.M.; Hendrick, A.M.; Khan, F.N.; Ziemer, D.C.; Pasquel, F.J. Current and Next Generation Portable Screening Devices for Diabetic Retinopathy. J. Diabetes Sci. Technol. 2016, 10, 295–300. [Google Scholar] [CrossRef]
- Mangione, C.M.; Lee, P.P.; Gutierrez, P.R.; Spritzer, K.; Berry, S.; Hays, R.D. National Eye Institute Visual Function Questionnaire Field Test Investigators. Development of the 25-Item National Eye Institute Visual Function Questionnaire. Arch. Ophthalmol. 2001, 119, 1050–1058. [Google Scholar] [CrossRef]
- Labiris, G.; Katsanos, A.; Fanariotis, M.; Tsirouki, T.; Pefkianaki, M.; Chatzoulis, D.; Tsironi, E. Psychometric properties of the Greek version of the NEI-VFQ 25. BMC Ophthalmol. 2008, 8, 4. [Google Scholar] [CrossRef]
- Singh, M.M.; Murthy, G.V.; Venkatraman, R.; Rao, S.P.; Nayar, S. A study of ocular morbidity among elderly population in a rural area of central India. Indian J. Ophthalmol. 1997, 45, 61–65. [Google Scholar] [PubMed]
- Thevi, T.; Basri, M.; Reddy, S. Prevalence of eye diseases and visual impairment among the rural population—A case study of temerloh hospital. Malays. Fam. Physician 2012, 30, 6–10. [Google Scholar] [PubMed]
- Bai, Y.; Yi, H.; Zhang, L.; Shi, Y.; Ma, X.; Congdon, N.; Zhou, Z.; Boswell, M.; Rozelle, S. An investigation of vision problems and the vision care system in rural China. Southeast Asian J. Trop. Med. Public Health 2014, 45, 1464–1473. [Google Scholar] [PubMed]
- Williams, A.M.; Botsford, B.; Mortensen, P.; Park, D.; Waxman, E.L. Delivering mobile eye care to underserved communities while providing training in ophthalmology to medical students: Experience of the Guerrilla Eye Service. Clin. Ophthalmol. 2019, 13, 337–346. [Google Scholar] [CrossRef]
- Cicinelli, M.V.; Marmamula, S.; Khanna, R.C. Comprehensive eye care—Issues, challenges, and way forward. Indian J. Ophthalmol. 2020, 68, 316–323. [Google Scholar] [CrossRef]
- Keel, S.; Lee, P.Y.; Foreman, J.; van Wijngaarden, P.; Taylor, H.R.; Dirani, M. Participant referral rate in the National Eye Health Survey (NEHS). PLoS ONE 2017, 12, e0174867. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | n | % | |
|---|---|---|---|
| Gender | Males | 106 | 44.4 |
| Females | 133 | 55.6 | |
| Age, years | Mean ± Stand. dev. [min, max] | 66.4 ± 14.8 [40, 100] | |
| 40–59 | 73 | 30.5 | |
| 60–79 | 118 | 49.4 | |
| 80+ | 48 | 20.1 | |
| Education | None | 113 | 47.3 |
| Primary school | 82 | 34.2 | |
| High school | 41 | 17.2 | |
| University | 3 | 1.3 | |
| Family status | Unmarried, divorced, widows | 51 | 21.3 |
| Married | 188 | 78.7 | |
| Number of offspring | None | 16 | 6.7 |
| 1 | 14 | 5.9 | |
| 2 | 38 | 15.9 | |
| 3+ | 171 | 71.5 | |
| Occupation | Unemployed | 15 | 6.3 |
| Retired, household | 134 | 56.1 | |
| Public sector worker, self-employed, etc. | 19 | 7.9 | |
| Livestock farmer | 63 | 26.4 | |
| Farmer | 8 | 3.3 | |
| Chronic conditions | 3+ | 107 | 44.8 |
| Diseases of the eye | yes | 26 | 10.9 |
| Characteristics | Refractive Errors a | Cataract | Glaucoma | Hypertension | Dyslipidemia | Cardiovascular Diseases | Osteoporosis | Diabetes Mellitus | Chronic Obstructive Pulmonary Disease | Diseases of the Eye | Depression-Chronic Psychotic Disorders | Cancer | Dementia | Asthma | Parkinson’s Disease | Chronic Conditions (3+) b | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| Number | 141 | 59.0 | 52 | 21.8 | 28 | 11.7 | 133 | 55.6 | 105 | 43.9 | 75 | 31.4 | 60 | 25.1 | 60 | 25.1 | 36 | 15.1 | 26 | 10.9 | 31 | 13.0 | 3 | 1.3 | 2 | 0.8 | 1 | 0.4 | 1 | 0.4 | 107 | 44.8 |
| Gender | ||||||||||||||||||||||||||||||||
| Males | 53 | 50.0 | 26 | 24.5 | 9 | 8.5 | 49 | 46.2 | 47 | 44.3 | 40 | 37.7 | 3 | 2.8 | 26 | 24.5 | 19 | 17.9 | 12 | 11.3 | 7 | 6.6 | 1 | 0.9 | 2 | 1.9 | 1 | 0.9 | 1 | 0.9 | 42 | 39.6 |
| Females | 88 | 66.2 | 26 | 19.5 | 19 | 14.3 | 84 | 63.2 | 58 | 43.6 | 35 | 26.3 | 57 | 42.9 | 34 | 25.6 | 17 | 12.8 | 14 | 10.5 | 24 | 18.0 | 2 | 1.5 | - | - | - | 65 | 48.9 | |||
| Age, years | ||||||||||||||||||||||||||||||||
| 40–59 | 22 | 30.1 | 2 | 2.7 | 4 | 5.5 | 15 | 20.5 | 21 | 28.8 | 5 | 6.8 | 5 | 6.8 | 10 | 13.7 | 1 | 1.4 | 4 | 5.5 | 11 | 15.1 | - | - | - | 1.4 | - | 8 | 11.0 | |||
| 60–79 | 83 | 70.3 | 34 | 28.8 | 14 | 11.9 | 78 | 66.1 | 65 | 55.1 | 43 | 36.4 | 33 | 28.0 | 32 | 27.1 | 25 | 21.2 | 13 | 11.0 | 13 | 11.0 | 3 | 2.5 | - | - | - | 66 | 55.9 | |||
| 80+ | 36 | 75.0 | 16 | 33.3 | 10 | 20.8 | 40 | 83.3 | 19 | 39.6 | 27 | 56.3 | 22 | 45.8 | 18 | 37.5 | 10 | 20.8 | 9 | 18.8 | 7 | 14.6 | - | 2 | 4.2 | - | 1 | 2.1 | 33 | 68.8 | ||
| Education | ||||||||||||||||||||||||||||||||
| None | 79 | 69.9 | 38 | 33.6 | 12 | 10.6 | 78 | 69.0 | 52 | 46.0 | 44 | 38.9 | 47 | 41.6 | 32 | 28.3 | 20 | 17.7 | 16 | 14.2 | 15 | 13.3 | 3 | 2.7 | 1 | 0.9 | - | - | 63 | 55.8 | ||
| Primary School | 46 | 56.1 | 13 | 15.9 | 13 | 15.9 | 44 | 53.7 | 37 | 45.1 | 23 | 28.0 | 13 | 15.9 | 23 | 28.0 | 15 | 18.3 | 7 | 8.5 | 8 | 9.8 | - | 1 | 1.2 | 1 | 1.2 | 1 | 1.2 | 36 | 43.9 | |
| High School | 15 | 36.6 | 1 | 2.4 | 3 | 7.3 | 11 | 26.8 | 16 | 39.0 | 7 | 17.1 | - | 5 | 12.2 | 1 | 2.4 | 2 | 4.9 | 8 | 19.5 | - | - | - | - | 8 | 19.5 | |||||
| University | 1 | 33.3 | - | - | - | - | 1 | 33.3 | - | - | - | 1 | 33.3 | - | - | - | - | - | - | |||||||||||||
| Family status | ||||||||||||||||||||||||||||||||
| Unmarried, Divorced, Widowed | 37 | 72.5 | 15 | 29.4 | 3 | 5.9 | 34 | 66.7 | 24 | 47.1 | 20 | 39.2 | 31 | 60.8 | 15 | 29.4 | 9 | 17.9 | 13 | 25.5 | 8 | 15.7 | 1 | 2.0 | - | - | - | 30 | 58.8 | |||
| Married | 104 | 55.3 | 37 | 19.7 | 25 | 13.3 | 99 | 52.7 | 81 | 43.1 | 55 | 29.3 | 29 | 15.4 | 45 | 23.9 | 27 | 14.4 | 13 | 6.9 | 23 | 12.2 | 2 | 1.1 | 2 | 1.1 | 1 | 0.5 | 1 | 0.5 | 77 | 41.0 |
| Number of offsprings | ||||||||||||||||||||||||||||||||
| none | 9 | 56.3 | 4 | 25.0 | 3 | 18.8 | 8 | 50.0 | 3 | 18.8 | 7 | 43.8 | 6 | 37.5 | 3 | 18.8 | 4 | 25.0 | 2 | 12.5 | 2 | 12.5 | 1 | 6.3 | 1 | 6.3 | - | 1 | 6.3 | 8 | 50.0 | |
| 1 | 8 | 57.1 | 5 | 35.7 | - | 7 | 5.0 | 3 | 21.4 | 6 | 42.9 | - | 2 | 14.3 | 2 | 14.3 | 2 | 14.3 | 1 | 7.1 | - | - | - | - | 4 | 28.6 | ||||||
| 2 | 19 | 50.0 | 9 | 23.7 | 4 | 10.5 | 17 | 44.7 | 18 | 47.4 | 5 | 13.2 | 10 | 26.3 | 7 | 18.4 | 8 | 21.1 | 6 | 15.8 | 5 | 13.2 | - | - | - | - | 13 | 34.2 | ||||
| 3+ | 105 | 61.4 | 34 | 19.9 | 21 | 12.3 | 101 | 59.1 | 81 | 47.4 | 57 | 33.3 | 44 | 25.7 | 48 | 28.1 | 22 | 12.9 | 16 | 9.4 | 23 | 13.5 | 2 | 1.2 | 1 | 0.6 | 1 | 0.6 | - | 82 | 48.0 | |
| Occupation | ||||||||||||||||||||||||||||||||
| Unemployed | 5 | 33.3 | - | 3 | 20.0 | 3 | 20.0 | 4 | 26.7 | - | 1 | 6.7 | 3 | 20.0 | 1 | 6.7 | - | 3 | 20.0 | - | - | - | - | 4 | 26.7 | |||||||
| Retired, Household | 98 | 73.1 | 38 | 28.4 | 17 | 12.7 | 90 | 67.2 | 63 | 47.0 | 57 | 42.5 | 51 | 38.1 | 36 | 26.9 | 27 | 20.1 | 19 | 14.2 | 21 | 15.7 | 2 | 1.5 | 2 | 1.5 | - | 1 | 0.7 | 77 | 57.5 | |
| Public Sector Worker, Self-Employed, Etc. | 8 | 42.1 | 1 | 5.3 | 2 | 10.5 | 5 | 26.3 | 5 | 26.3 | 5 | 26.3 | - | 2 | 10.5 | 1 | 5.3 | 3 | 15.8 | 4 | 21.1 | - | - | - | - | 3 | 15.8 | |||||
| Livestock Farmer | 29 | 46.0 | 12 | 19.0 | 6 | 9.5 | 32 | 50.8 | 30 | 47.6 | 10 | 15.9 | 8 | 12.7 | 17 | 27.0 | 6 | 9.5 | 4 | 6.3 | 2 | 3.2 | 1 | 1.6 | - | - | - | 21 | 33.3 | |||
| Farmer | 1 | 12.5 | 1 | 12.5 | - | 3 | 37.5 | 3 | 37.5 | 3 | 37.5 | - | 2 | 25.0 | 1 | 12.5 | - | 1 | 12.5 | - | - | 1 | 12.5 | - | 2 | 25.0 | ||||||
| Chronic conditions | ||||||||||||||||||||||||||||||||
| 3+ | 80 | 74.8 | 36 | 33.6 | 19 | 17.8 | 92 | 86.0 | 76 | 71.0 | 60 | 56.1 | 39 | 36.4 | 50 | 46.7 | 28 | 26.2 | 20 | 18.7 | 21 | 19.6 | 3 | 2.8 | 2 | 1.9 | - | 1 | 0.9 | -- | -- | |
| Characteristics | Without Diagnosis | Known Cases | New Diagnosed Cases | p-Value |
|---|---|---|---|---|
| n (%) | ||||
| Number | 89 (37.2) | 68 (28.5) | 82 (34.3) | - |
| Gender | ||||
| Males | 41 (46.1) | 27 (39.7) | 38 (46.3) | 0.660 |
| Females | 48 (53.9) | 41 (60.3) | 44 (53.7) | |
| Age, years | ||||
| 40–59 | 47 (52.8) | 13 (19.1) | 13 (15.9) | <0.001 |
| 60–79 | 34 (38.2) | 31 (45.6) | 53 (64.6) | |
| 80+ | 8 (9.0) | 24 (35.3) | 16 (19.5) | |
| Education | ||||
| None | 26 (29.2) | 34 (50.0) | 53 (64.6) | <0.001 |
| Primary School | 33 (37.1) | 27 (39.7) | 22 (26.8) | |
| High School | 30 (33.7) | 5 (7.4) | 6 (7.3) | |
| University | - | 2 (2.9) | 1 (1.2) | |
| Family status | ||||
| Unmarried, Divorced, Widowed | 15 (16.9) | 18 (26.5) | 18 (22.0) | 0.341 |
| Married | 74 (83.1) | 50 (73.5) | 64 (78.0) | |
| Number of offsprings | ||||
| none | 5 (5.6) | 6 (8.8) | 5 (6.1) | 0.912 |
| 1 | 6 (6.7) | 4 (5.9) | 4 (4.9) | |
| 2 | 17 (19.1) | 9 (13.2) | 12 (14.6) | |
| 3+ | 61 (68.5) | 49 (72.1) | 61 (74.4) | |
| Occupation | ||||
| Unemployed | 5 (5.6) | 6 (8.8) | 4 (4.9) | 0.001 |
| Retired, Household | 38 (42.7) | 47 (69.1) | 49 (59.8) | |
| Public Sector Worker, Self-Employed, etc. | 12 (13.5) | 4 (5.9) | 3 (3.7) | |
| Livestock Farmer | 27 (30.3) | 10 (14.7) | 26 (31.7) | |
| Farmer | 7 (7.9) | 1 (1.5) | - | |
| Chronic conditions | ||||
| 3+ | 17 (19.1) | 46 (67.6) | 44 (53.7) | <0.001 |
| Without Diagnosis (n = 89) | Known Cases (n = 68) | New Diagnosed Cases (n = 82) | ||
|---|---|---|---|---|
| Scale and Subscales | Mean (Stand. Dev.) | p-Value | ||
| Visual Function Questionnaire (VFQ-25) | 90.6 (17.6) | 71.5 (26.3) | 81.9 (17.4) | <0.001 |
| General Health | 68.8 (19.5) | 49.1 (23.7) | 54.1 (18.8) | <0.001 |
| General Vision | 74.6 (16.7) | 56.3 (20.6) | 67.3 (16.4) | <0.001 |
| Ocular Pain | 83.8 (19.5) | 64.0 (26.9) | 69.7 (27.9) | <0.001 |
| Near Activities | 91.0 (20.1) | 70.8 (30.8) | 81.3 (20.0) | <0.001 |
| Distance Activities | 93.5 (18.5) | 70.7 (32.2) | 83.1 (20.6) | <0.001 |
| Vision-specific Social Functioning | 95.4 (18.2) | 81.0 (30.6) | 89.3 (18.5) | <0.001 |
| Vision-specific Mental Health | 89.5 (18.9) | 64.9 (30.8) | 83.1 (19.8) | <0.001 |
| Vision-specific Role Difficulties | 93.7 (19.3) | 74.2 (31.0) | 87.0 (19.2) | <0.001 |
| Vision-specific Dependency | 95.6 (18.3) | 79.0 (31.8) | 91.5 (20.5) | <0.001 |
| Color Vision | 94.7 (19.4) | 83.8 (29.9) | 88.7 (21.2) | 0.006 |
| Peripheral Vision | 94.4 (21.2) | 71.3 (31.2) | 79.0 (26.8) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chliveros, K.; Linardakis, M.; Tsiligianni, I.; Tsilimbaris, M.; Pallikaris, I.; Lionis, C. Unmasking the Hidden Morbidity of Ocular Diseases in Primary Care Through a Collaboration with Specialists in Remote Areas: A Cross-Sectional Study from Rural Crete, Greece. Diseases 2025, 13, 137. https://doi.org/10.3390/diseases13050137
Chliveros K, Linardakis M, Tsiligianni I, Tsilimbaris M, Pallikaris I, Lionis C. Unmasking the Hidden Morbidity of Ocular Diseases in Primary Care Through a Collaboration with Specialists in Remote Areas: A Cross-Sectional Study from Rural Crete, Greece. Diseases. 2025; 13(5):137. https://doi.org/10.3390/diseases13050137
Chicago/Turabian StyleChliveros, Konstantinos, Manolis Linardakis, Ioanna Tsiligianni, Miltiadis Tsilimbaris, Ioannis Pallikaris, and Christos Lionis. 2025. "Unmasking the Hidden Morbidity of Ocular Diseases in Primary Care Through a Collaboration with Specialists in Remote Areas: A Cross-Sectional Study from Rural Crete, Greece" Diseases 13, no. 5: 137. https://doi.org/10.3390/diseases13050137
APA StyleChliveros, K., Linardakis, M., Tsiligianni, I., Tsilimbaris, M., Pallikaris, I., & Lionis, C. (2025). Unmasking the Hidden Morbidity of Ocular Diseases in Primary Care Through a Collaboration with Specialists in Remote Areas: A Cross-Sectional Study from Rural Crete, Greece. Diseases, 13(5), 137. https://doi.org/10.3390/diseases13050137