
Clinical Importance of B-Type Natriuretic Peptide Levels in Sinus Rhythm at 3 Months After Persistent Atrial Fibrillation Ablation
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Catheter Settings and Ablation Protocol
2.3. Follow Up
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
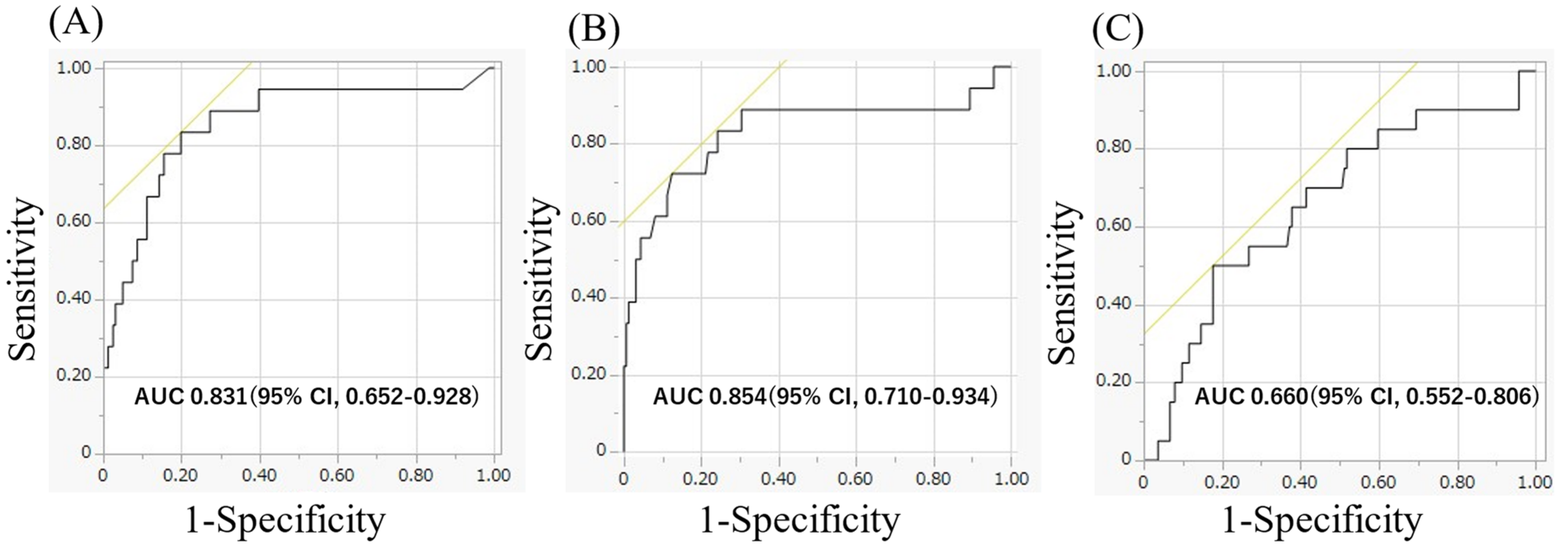
3.2. BNP Levels Before Ablation and 1 Month and 3 Months After Ablation
4. Discussion
4.1. Main Findings
4.2. Importance of BNP
4.3. Association Between BNP Levels and Clinical Outcomes in Patients with AF
4.4. Clinical Implication
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Silvet, H.; Young-Xu, Y.; Walleigh, D.; Ravid, S. Brain Natriuretic Peptide Is Elevated in Outpatients with Atrial Fibrillation. Am. J. Cardiol. 2003, 92, 1124–1127. [Google Scholar] [CrossRef] [PubMed]
- Kerr, B.; Brandon, L. Atrial Fibrillation, Thromboembolic Risk, and the Potential Role of the Natriuretic Peptides, a Focus on BNP and NT-proBNP—A Narrative Review. Int. J. Cardiol. Heart Vasc. 2022, 43, 101132. [Google Scholar] [CrossRef]
- Kim, D.Y.; Kim, S.H.; Ryu, K.H. Tachycardia Induced Cardiomyopathy. Korean Circ. J. 2019, 49, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Ko, D.; Chung, M.K.; Evans, P.T.; Benjamin, E.J.; Helm, R.H. Atrial Fibrillation: A Review: A Review. JAMA 2025, 333, 329–342. [Google Scholar] [CrossRef]
- Patton, K.K.; Ellinor, P.T.; Heckbert, S.R.; Christenson, R.H.; DeFilippi, C.; Gottdiener, J.S.; Kronmal, R.A. N-Terminal pro-B-Type Natriuretic Peptide Is a Major Predictor of the Development of Atrial Fibrillation: The Cardiovascular Health Study: The Cardiovascular Health Study. Circulation 2009, 120, 1768–1774. [Google Scholar] [CrossRef]
- Knudsen, C.W.; Omland, T.; Clopton, P.; Westheim, A.; Wu, A.H.B.; Duc, P.; McCord, J.; Nowak, R.M.; Hollander, J.E.; Storrow, A.B.; et al. Impact of Atrial Fibrillation on the Diagnostic Performance of B-Type Natriuretic Peptide Concentration in Dyspneic Patients: An Analysis from the Breathing Not Properly Multinational Study. J. Am. Coll. Cardiol. 2005, 46, 838–844. [Google Scholar] [CrossRef]
- Charafeddine, K.; Zakka, P.; Bou Dargham, B.; Abdulhai, F.; Zakka, K.; Zouein, F.A.; Refaat, M. Potential Biomarkers in Atrial Fibrillation: Insight into Their Clinical Significance: Insight into Their Clinical Significance. J. Cardiovasc. Pharmacol. 2021, 78, 184–191. [Google Scholar] [CrossRef]
- Inoue, S.; Murakami, Y.; Sano, K.; Katoh, H.; Shimada, T. Atrium as a Source of Brain Natriuretic Polypeptide in Patients with Atrial Fibrillation. J. Card. Fail. 2000, 6, 92–96. [Google Scholar] [CrossRef]
- De Marchis, G.M.; Krisai, P.; Werlen, L.; Sinnecker, T.; Aeschbacher, S.; Dittrich, T.D.; Polymeris, A.A.; Coslovksy, M.; Blum, M.R.; Rodondi, N.; et al. Biomarker, Imaging, and Clinical Factors Associated with Overt and Covert Stroke in Patients with Atrial Fibrillation. Stroke 2023, 54, 2542–2551. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, H.-S.; Park, H.W.; Choi, E.-K.; Park, J.-K.; Kim, J.-B.; Kang, K.-W.; Shim, J.; Joung, B.; Park, K.-M. Clinical Outcomes of Rhythm Control Strategies for Asymptomatic Atrial Fibrillation According to the Quality-of-Life Score: The CODE-AF (Comparison Study of Drugs for Symptom Control and Complication Prevention of Atrial Fibrillation) Registry. J. Am. Heart Assoc. 2022, 11, e025956. [Google Scholar] [CrossRef]
- Hussein, A.A.; Saliba, W.I.; Martin, D.O.; Shadman, M.; Kanj, M.; Bhargava, M.; Dresing, T.; Chung, M.; Callahan, T.; Baranowski, B.; et al. Plasma B-Type Natriuretic Peptide Levels and Recurrent Arrhythmia after Successful Ablation of Lone Atrial Fibrillation. Circulation 2011, 123, 2077–2082. [Google Scholar] [CrossRef] [PubMed]
- Degener, S.; Pattberg, S.V.; Feuersenger, H.; Bansmann, P.M.; Shin, D.-I.; Krummenauer, F.; Horlitz, M. Predictive Value of B-Type Natriuretic Peptide Levels in Patients with Paroxysmal and Persistent Atrial Fibrillation Undergoing Pulmonary Vein Isolation. J. Interv. Card. Electrophysiol. 2011, 30, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Kawaji, T.; Shizuta, S.; Aizawa, T.; Nishiwaki, S.; Yoshizawa, T.; Nishiuchi, S.; Kato, M.; Yokomatsu, T.; Miki, S.; TRANQUILIZE AF Registry Investigators. Prognostic Importance of B-Type Natriuretic Peptide Level in Patients Undergoing Catheter Ablation for Atrial Fibrillation. Circ. J. 2023, 87, 1730–1739. [Google Scholar] [CrossRef] [PubMed]
- Inohara, T.; Kim, S.; Pieper, K.; Blanco, R.G.; Allen, L.A.; Fonarow, G.C.; Gersh, B.J.; Ezekowitz, M.D.; Kowey, P.R.; Reiffel, J.A.; et al. B-Type Natriuretic Peptide, Disease Progression and Clinical Outcomes in Atrial Fibrillation. Heart 2019, 105, 370–377. [Google Scholar] [CrossRef]
- Jiang, H.; Wang, W.; Wang, C.; Xie, X.; Hou, Y. Association of Pre-Ablation Level of Potential Blood Markers with Atrial Fibrillation Recurrence after Catheter Ablation: A Meta-Analysis. Europace 2017, 19, 392–400. [Google Scholar] [CrossRef]
- Miake, J.; Kato, M.; Ogura, K.; Iitsuka, K.; Okamura, A.; Tomomori, T.; Tsujimoto, D.; Kato, M.; Yamamoto, K. Pre-Ablation Levels of Brain Natriuretic Peptide Are Independently Associated with the Recurrence of Atrial Fibrillation after Radiofrequency Catheter Ablation in Patients with Nonvalvular Atrial Fibrillation. Heart Vessels 2019, 34, 517–526. [Google Scholar] [CrossRef]
- Yuan, Y.; Nie, B.; Gao, B.; Guo, C.; Li, L. Natriuretic Peptides as Predictors for Atrial Fibrillation Recurrence after Catheter Ablation: A Meta-Analysis. Medicine 2023, 102, e33704. [Google Scholar] [CrossRef]
- Sumiyoshi, H.; Tasaka, H.; Yoshida, K.; Chatani, R.; Sakata, A.; Yoshino, M.; Kadota, K. Association between Postprocedural Echocardiographic and Laboratory Data and Clinical Outcomes in Patients with Preserved Ejection Fraction after Catheter Ablation for Atrial Fibrillation. Heart Rhythm 2025, 22, 914–922. [Google Scholar] [CrossRef]
- Matsumoto, S.; Matsunaga-Lee, Y.; Ishimi, M.; Ohnishi, M.; Masunaga, N.; Tachibana, K.; Takano, Y. Clinical Significance of B-Type Natriuretic Peptide Levels at 3 Months after Atrial Fibrillation Ablation. Diseases 2021, 9, 49. [Google Scholar] [CrossRef]
- Wang, H.; Huang, J.; Gu, W.; Hao, X.; Li, G.; Yuan, Y.; Lu, Y. Relationship between Brain Natriuretic Peptide and Thromboembolic Events in Elderly Patients with Nonvalvular Atrial Fibrillation. Cardiol. Res. Pract. 2024, 2024, 5594637. [Google Scholar] [CrossRef]
- Srisujikul, P.; Thiankhaw, K.; Tanprawate, S.; Soontornpun, A.; Wantaneeyawong, C.; Teekaput, C.; Sirimaharaj, N.; Nudsasarn, A. Serum NT-proBNP Level for Predicting Functional Outcomes after Acute Ischemic Stroke. Sci. Rep. 2023, 13, 13903. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, X.; Fang, X.; Feng, S. Efficacy and Safety of Catheter Ablation for Atrial Fibrillation in Patients with Heart Failure with Preserved Ejection Fraction: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2024, 11, 1423147. [Google Scholar] [CrossRef] [PubMed]
- Pasqualotto, E.; Ternes, C.M.P.; Chavez, M.P.; Polanczyk, C.A.; Ferreira, R.O.M.; Nienkötter, T.; de Oliveira Almeida, G.; Bertoli, E.; Clemente, M.R.C.; d’Avila, A.; et al. Catheter Ablation for Atrial Fibrillation in Heart Failure with Reduced Ejection Fraction Patients: A Meta-Analysis. Heart Rhythm 2024, 21, 1604–1612. [Google Scholar] [CrossRef]
- Kawamura, M.; Munetsugu, Y.; Kawasaki, S.; Onishi, K.; Onuma, Y.; Kikuchi, M.; Tanno, K.; Kobayashi, Y. Type III Procollagen-N-Peptide as a Predictor of Persistent Atrial Fibrillation Recurrence after Cardioversion. Europace 2012, 14, 1719–1725. [Google Scholar] [CrossRef]
- Anter, E.; Jessup, M.; Callans, D.J. Atrial Fibrillation and Heart Failure: Treatment Considerations for a Dual Epidemic. Circulation 2009, 119, 2516–2525. [Google Scholar] [CrossRef]
- Carlisle, M.A.; Fudim, M.; DeVore, A.D.; Piccini, J.P. Heart Failure and Atrial Fibrillation, like Fire and Fury. JACC Heart Fail. 2019, 7, 447–456. [Google Scholar] [CrossRef]
- Marine, J.E.; Yang, E. Assessing Interplay between Atrial Fibrillation and Heart Failure in Patients with Cardiac Implantable Electronic Devices. JACC Clin. Electrophysiol. 2022, 8, 194–196. [Google Scholar] [CrossRef]
- Kanaoka, K.; Nishida, T.; Iwanaga, Y.; Nakai, M.; Tonegawa-Kuji, R.; Nishioka, Y.; Myojin, T.; Okada, K.; Noda, T.; Kusano, K.; et al. Oral Anticoagulation after Atrial Fibrillation Catheter Ablation: Benefits and Risks. Eur. Heart J. 2024, 45, 522–534. [Google Scholar] [CrossRef]
- Fei, Z.-T.; Yao, P.-C.; Chen, M.; Fei, Y.-D.; Li, W.; Zhang, P.-P.; Sun, J.; Wang, Q.-S.; Li, Y.-G. Real World Risk of Discontinuing Oral Anticoagulation after Successful Catheter Ablation for Atrial Fibrillation. Heliyon 2024, 10, e32516. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1–e156. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Non Recurrence (n = 160) | Recurrence (n = 18) | p-Value |
|---|---|---|---|
| Age, y | 66 (54, 78) | 70 (50, 75) | p = 0.50 |
| Male gender, n (%) | 81 (50.6) | 10 (55.6) | p = 0.69 |
| Boddy mass index, kg/m2 | 24.4 (21.0, 30.4) | 25.2 (18.5, 30.8) | p = 0.96 |
| CHAD2DS2-VASc score | 2 (0, 4) | 2.5 (0.9, 5) | p = 0.06 |
| Hypertension, n (%) | 79 (49) | 15 (83) | p < 0.01 |
| Heart failure, n (%) | 46 (29) | 6 (33) | p = 0.71 |
| LVEF, % | 57 (35, 66) | 55 (35, 70) | p = 0.75 |
| LAVI, ml/m3 | 41 (30, 59.8) | 53 (31.5, 82.5) | p = 0.03 |
| eGFR, mL/min/1.73 m2 | 65.9 (40.9, 82.7) | 68.6 (25.2, 89.0) | p = 0.51 |
| BNP before ablation, pg/mL | 99.2 (44.5, 288.2) | 142.8 (32.2, 450.1) | p = 0.14 |
| Non Recurrence (n = 160) | Recurrence (n = 18) | p-Value | |
|---|---|---|---|
| BNP at 1 month after ablation, pg/mL | 35.7 (9.9, 107.2) | 70.0 (19.4, 167.4) | p = 0.22 |
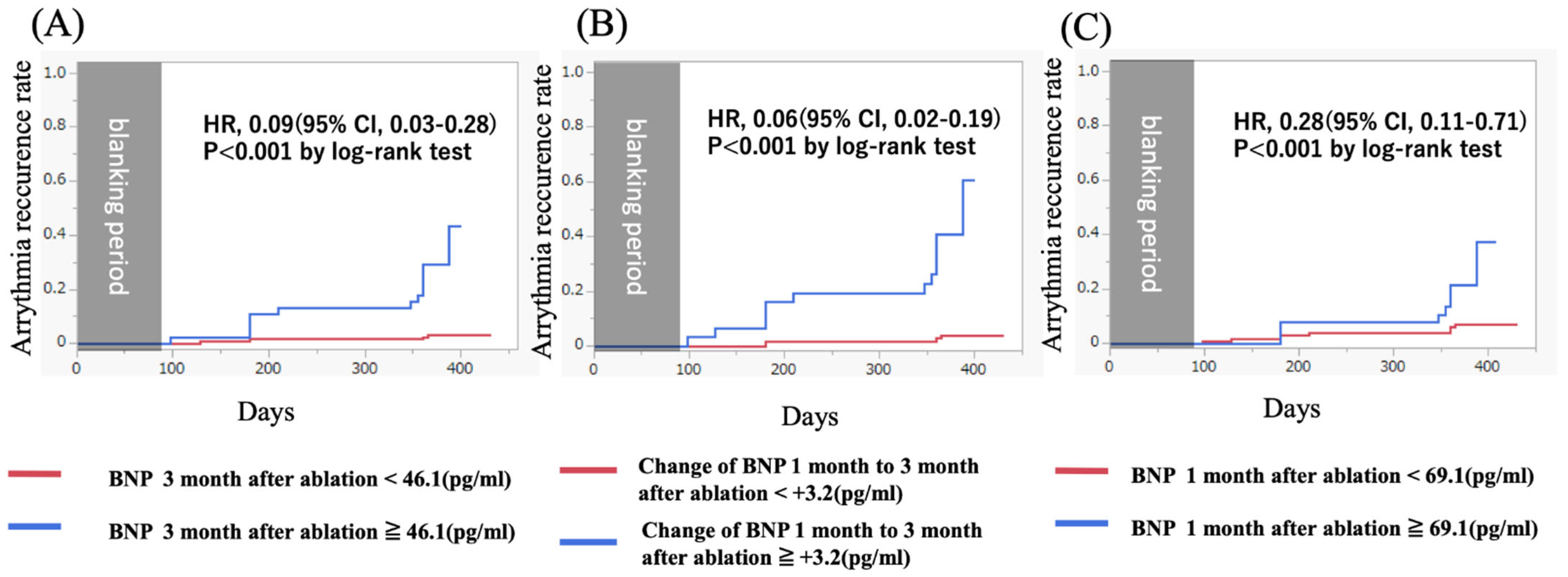
| BNP at 3 months after ablation, pg/mL | 22.5 (6.4, 70.1) | 75.7 (26.0, 269.3) | p < 0.001 |
| BNP changes from 1 month to 3 months after ablation, pg/mL | −11.1 (−53, 5.7) | 17.8 (−58.3, 180.5) | p < 0.001 |
| Prognostic Factor | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (≥70 years) | 1.90 (0.75–4.81) | p = 0.18 | ||
| Gender (female vs. male) | 1.15 (0.45–2.96) | p = 0.77 | ||
| CHAD2DS2-VASc score (≥3) | 1.75 (0.70–4.42) | p = 0.23 | ||
| Boddy mass index (≥25 kg/m2) | 1.33 (0.53–3.38) | p = 0.54 | ||
| Heart failure | 1.11 (0.41–2.97) | p = 0.84 | ||
| LAVI (≥40 mL/m3) | 1.42 (0.72–2.79) | p = 0.31 | ||
| BNP 3 months after ablation (<46.1) pg/mL) | 0.09 (0.03–0.28) | p < 0.001 | 0.06 (0.02–0.28) | p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, J.; Matsuda, T.; Koyanagi, Y.; Yoshihiro, K.; Gibo, Y.; Usumoto, S.; Igawa, W.; Okabe, T.; Isomura, N.; Ochiai, M. Clinical Importance of B-Type Natriuretic Peptide Levels in Sinus Rhythm at 3 Months After Persistent Atrial Fibrillation Ablation. Diseases 2025, 13, 126. https://doi.org/10.3390/diseases13040126
Saito J, Matsuda T, Koyanagi Y, Yoshihiro K, Gibo Y, Usumoto S, Igawa W, Okabe T, Isomura N, Ochiai M. Clinical Importance of B-Type Natriuretic Peptide Levels in Sinus Rhythm at 3 Months After Persistent Atrial Fibrillation Ablation. Diseases. 2025; 13(4):126. https://doi.org/10.3390/diseases13040126
Chicago/Turabian StyleSaito, Jumpei, Toshihiko Matsuda, Yui Koyanagi, Katsuya Yoshihiro, Yuma Gibo, Soichiro Usumoto, Wataru Igawa, Toshitaka Okabe, Naoei Isomura, and Masahiko Ochiai. 2025. "Clinical Importance of B-Type Natriuretic Peptide Levels in Sinus Rhythm at 3 Months After Persistent Atrial Fibrillation Ablation" Diseases 13, no. 4: 126. https://doi.org/10.3390/diseases13040126
APA StyleSaito, J., Matsuda, T., Koyanagi, Y., Yoshihiro, K., Gibo, Y., Usumoto, S., Igawa, W., Okabe, T., Isomura, N., & Ochiai, M. (2025). Clinical Importance of B-Type Natriuretic Peptide Levels in Sinus Rhythm at 3 Months After Persistent Atrial Fibrillation Ablation. Diseases, 13(4), 126. https://doi.org/10.3390/diseases13040126