
The Effect of COVID-19 and COVID-19 Vaccination on Assisted Human Reproduction Outcomes: A Systematic Review and Meta-Analysis
 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
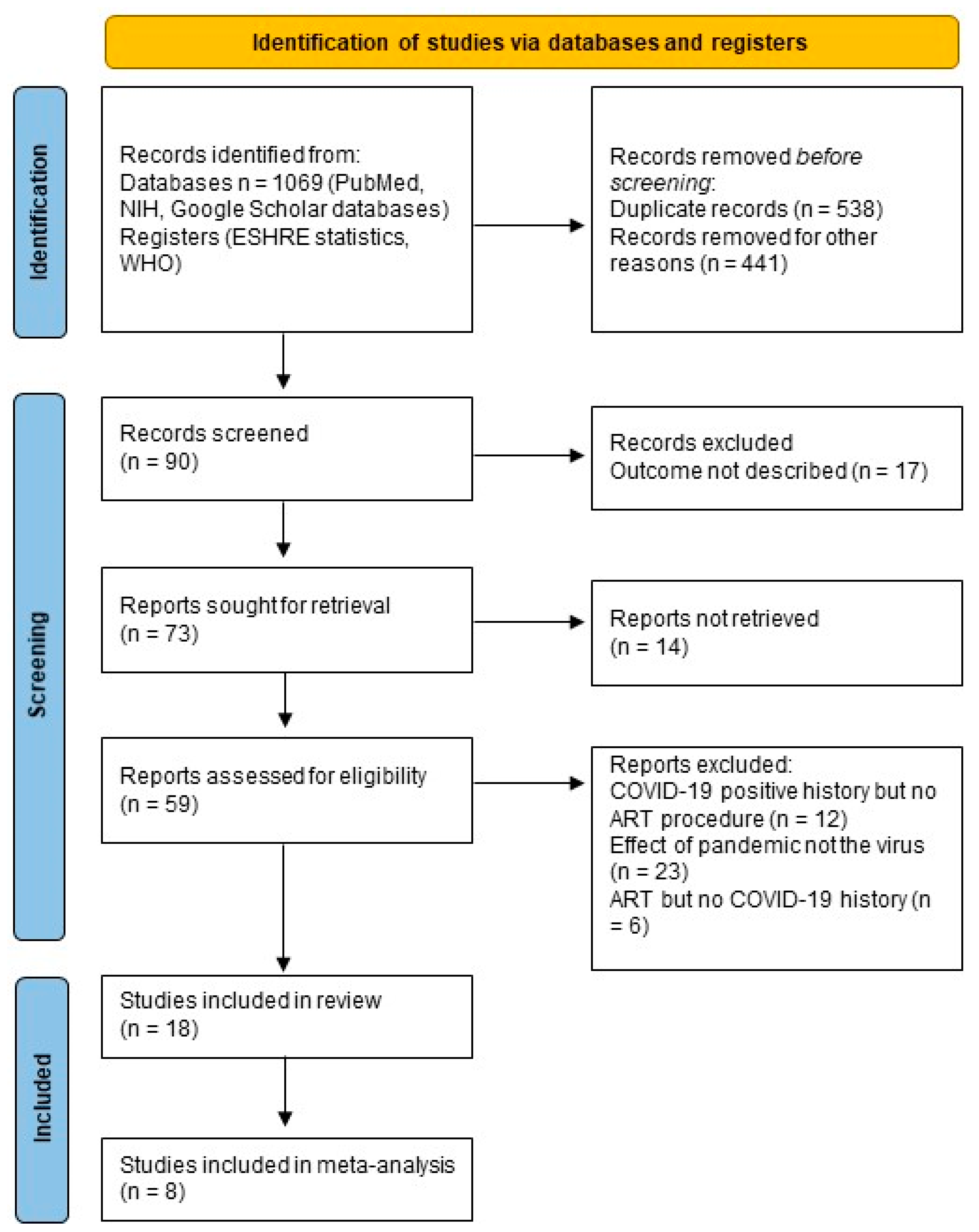
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Study Quality
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Reviewed Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Type | City, Country | Publication Date | No. COVID-19 Vaccinated Participants | Mean Age ± SD | Pregnancy | Birth | Miscarriage |
|---|---|---|---|---|---|---|---|---|
| Huang et al. [51] | retrospective cohort study | China | 9 February 2022 | 66 | 33.7 ± 5.6 | 39/66 (59.1) | ||
| Dong et al. [52] | prospective cohort study | China | 27 June 2022 | 735 infertile couples | 33.15 ± 3.55 | 70/132 (53.03) | ||
| Wang et al. [53] | cohort study | China | 16 December 2022 | 4185 couples | 31.49 (3.70) | 603 couples with clinical pregnancies | ||
| Chen et al. [54] | retrospective study | China | 11 January 2023 | 268 women with inactivated or recombinant COVID-19 | 33.32 ± 5.14 (inactivated) 33.00 ± 5.16 (recombinant) | (inactivated) 46/77 (57.94) (recombinant) 11/15 (3.33) | No data yet | (inactivated) 2/77 (2.60) (recombinant) 2/15 (13.33) |
| Yang et al. [55] | retrospective study | China | 11 October 2023 | 899 | 30.71 ± 3.84 | 141 | ||
| Chillon et al. [56] | observational study | Austria, Germany | 17 March 2023 | 45 | 35.53 (7.00%) | 1 (2.2%) | 6 (13%) | |
| Zhang et al. [57] | case-control study | China | 8 August 2023 | 1084 | 32.00 (30.00–35.00) | 248/1084 (22.88) | 180/1084 (16.61) | 70/504 (13.89) |
| TOTAL | 2362 4920 couples | 1159 | 186 | 74 |
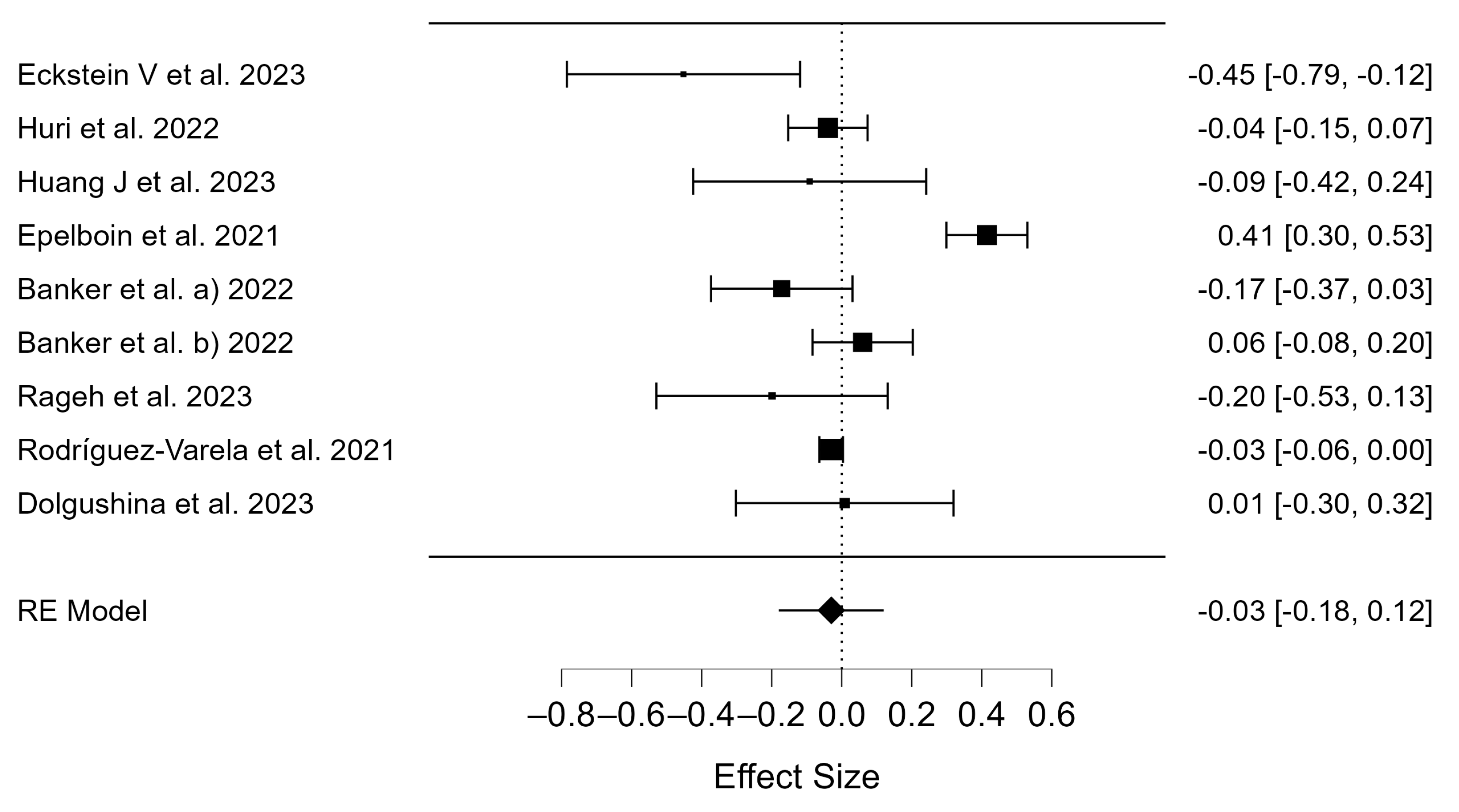
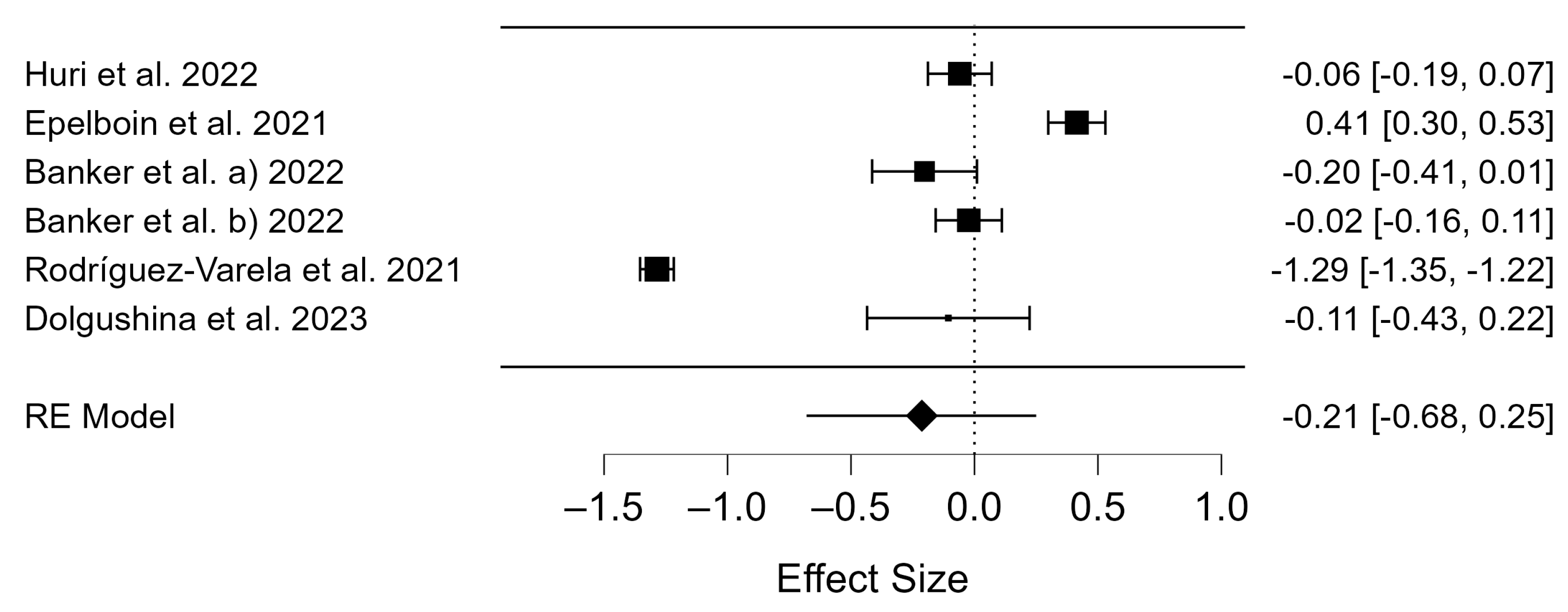
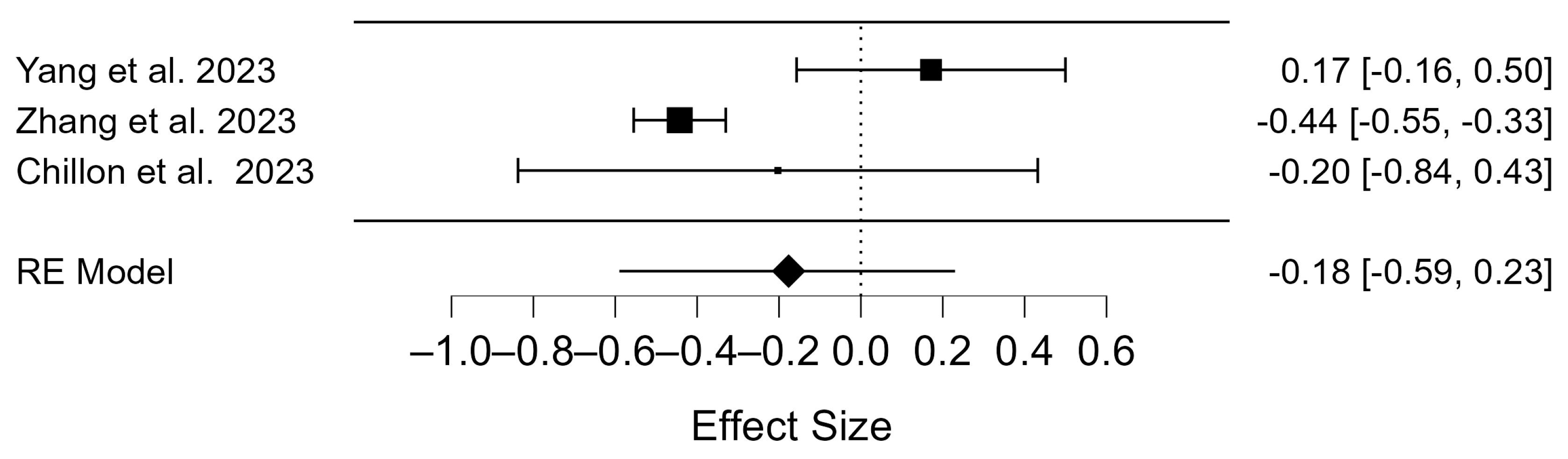
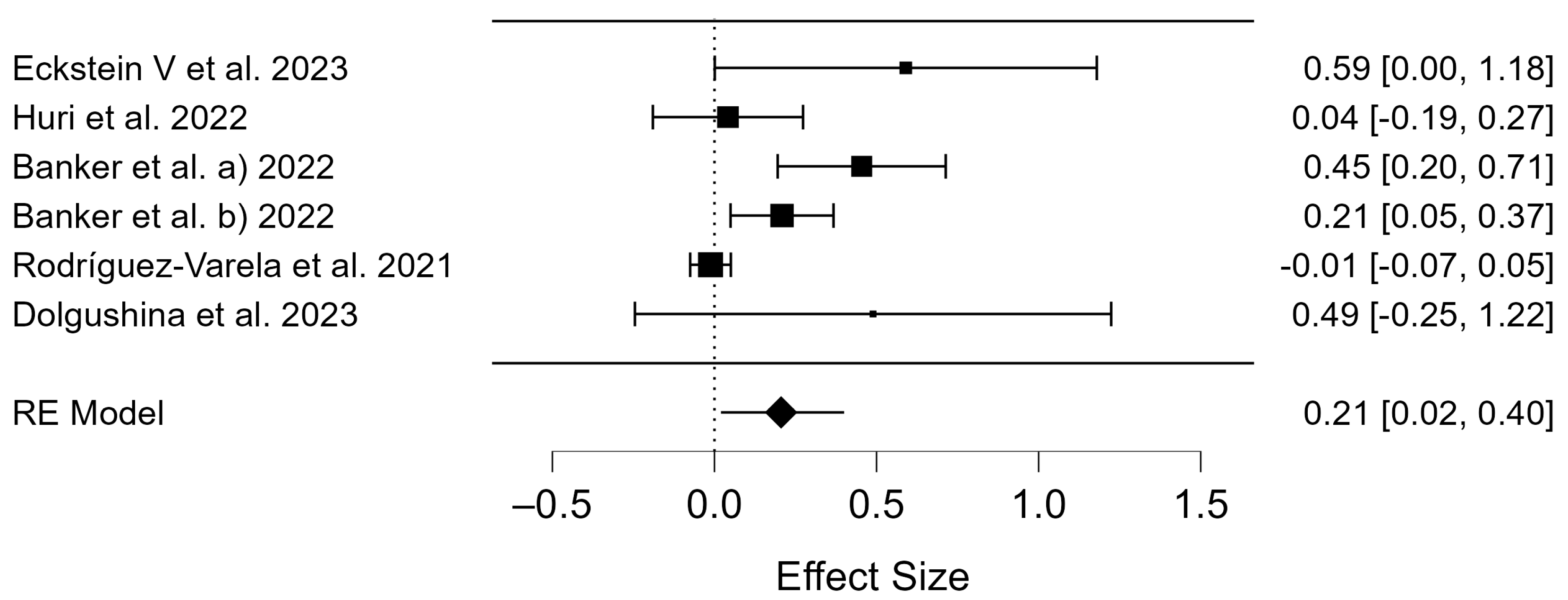
3.2. Meta-Analysis
3.3. Publication Bias
4. Discussion
4.1. Clinical Pregnancy Rate of COVID-19 Patients
4.2. Birth Rates of COVID-19 Patients
4.3. Miscarriage Rates of COVID-19 Patients
4.4. Clinical Pregnancy Rate of COVID-19 Vaccinated Patients
4.5. Birth Rates of COVID-19 Vaccinated Patients
4.6. Miscarriage Rates of COVID-19 Vaccinated Patients
4.7. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Niemi, M.E.K.; Daly, M.J.; Ganna, A. The Human Genetic Epidemiology of COVID-19. Nat. Rev. Genet. 2022, 23, 533–546. [Google Scholar] [CrossRef]
- Xue, Y.; Xiong, Y.; Cheng, X.; Li, K. Impact of SARS-CoV-2 Infection on Clinical Outcomes of in Vitro Fertilization Treatments: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2023, 14, 1233986. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-Cell RNA-Seq Data Analysis on the Receptor ACE2 Expression Reveals the Potential Risk of Different Human Organs Vulnerable to 2019-nCoV Infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef]
- Kasuga, Y.; Zhu, B.; Jang, K.-J.; Yoo, J.-S. Innate Immune Sensing of Coronavirus and Viral Evasion Strategies. Exp. Mol. Med. 2021, 53, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Schneider, W.M.; Chevillotte, M.D.; Rice, C.M. Interferon-Stimulated Genes: A Complex Web of Host Defenses. Annu. Rev. Immunol. 2014, 32, 513–545. [Google Scholar] [CrossRef]
- Dong, M.; Zhang, J.; Ma, X.; Tan, J.; Chen, L.; Liu, S.; Xin, Y.; Zhuang, L. ACE2, TMPRSS2 Distribution and Extrapulmonary Organ Injury in Patients with COVID-19. Biomed. Pharmacother. 2020, 131, 110678. [Google Scholar] [CrossRef]
- Herrero, Y.; Pascuali, N.; Velázquez, C.; Oubiña, G.; Hauk, V.; de Zúñiga, I.; Peña, M.G.; Martínez, G.; Lavolpe, M.; Veiga, F.; et al. SARS-CoV-2 Infection Negatively Affects Ovarian Function in ART Patients. Biochim. Biophys. Acta Mol. Basis Dis. 2022, 1868, 166295. [Google Scholar] [CrossRef]
- Rajak, P.; Roy, S.; Dutta, M.; Podder, S.; Sarkar, S.; Ganguly, A.; Mandi, M.; Khatun, S. Understanding the Cross-Talk between Mediators of Infertility and COVID-19. Reprod. Biol. 2021, 21, 100559. [Google Scholar] [CrossRef]
- Mokhtari, T.; Hassani, F.; Ghaffari, N.; Ebrahimi, B.; Yarahmadi, A.; Hassanzadeh, G. COVID-19 and Multiorgan Failure: A Narrative Review on Potential Mechanisms. J. Mol. Histol. 2020, 51, 613–628. [Google Scholar] [CrossRef]
- Wang, Z.; Xu, X. scRNA-Seq Profiling of Human Testes Reveals the Presence of the ACE2 Receptor, A Target for SARS-CoV-2 Infection in Spermatogonia, Leydig and Sertoli Cells. Cells 2020, 9, 920. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Geng, X.; Tan, Y.; Li, Q.; Xu, C.; Xu, J.; Hao, L.; Zeng, Z.; Luo, X.; Liu, F.; et al. New Understanding of the Damage of SARS-CoV-2 Infection Outside the Respiratory System. Biomed. Pharmacother. 2020, 127, 110195. [Google Scholar] [CrossRef]
- Verrienti, P.; Cito, G.; Di Maida, F.; Tellini, R.; Cocci, A.; Minervini, A.; Natali, A. The Impact of COVID-19 on the Male Genital Tract: A Qualitative Literature Review of Sexual Transmission and Fertility Implications. Clin. Exp. Reprod. Med. 2022, 49, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Saksena, S.; Sadri-Ardekani, H. ACE2 Receptor Expression in Testes: Implications in Coronavirus Disease 2019 Pathogenesis†. Biol. Reprod. 2020, 103, 449–451. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Xie, W.; Li, D.; Shi, L.; Mao, Y.; Xiong, Y.; Zhang, Y.; Zhang, M. Effect of SARS-CoV-2 Infection upon Male Gonadal Function: A Single Center-Based Study. MedRxiv 2020, 2020-03. [Google Scholar] [CrossRef]
- Bridwell, R.E.; Merrill, D.R.; Griffith, S.A.; Wray, J.; Oliver, J.J. A Coronavirus Disease 2019 (COVID-19) Patient with Bilateral Orchitis. Am. J. Emerg. Med. 2021, 42, 260.e3–260.e5. [Google Scholar] [CrossRef]
- Xu, J.; Qi, L.; Chi, X.; Yang, J.; Wei, X.; Gong, E.; Peh, S.; Gu, J. Orchitis: A Complication of Severe Acute Respiratory Syndrome (SARS)1. Biol. Reprod. 2006, 74, 410–416. [Google Scholar] [CrossRef]
- Gagliardi, L.; Bertacca, C.; Centenari, C.; Merusi, I.; Parolo, E.; Ragazzo, V.; Tarabella, V. Orchiepididymitis in a Boy with COVID-19. Pediatr. Infect. Dis. J. 2020, 39, e200. [Google Scholar] [CrossRef]
- Li, H.; Xiao, X.; Zhang, J.; Zafar, M.I.; Wu, C.; Long, Y.; Lu, W.; Pan, F.; Meng, T.; Zhao, K.; et al. Impaired Spermatogenesis in COVID-19 Patients. EClinicalMedicine 2020, 28, 100604. [Google Scholar] [CrossRef]
- Larasati, T.; Noda, T.; Fujihara, Y.; Shimada, K.; Tobita, T.; Yu, Z.; Matzuk, M.M.; Ikawa, M. Tmprss12 Is Required for Sperm Motility and Uterotubal Junction Migration in Mice†. Biol. Reprod. 2020, 103, 254–263. [Google Scholar] [CrossRef]
- Batiha, O.; Al-Deeb, T.; Al-zoubi, E.; Alsharu, E. Impact of COVID-19 and Other Viruses on Reproductive Health. Andrologia 2020, 52, e13791. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Y.; Wu, L.; Niu, S.; Song, C.; Zhang, Z.; Lu, G.; Qiao, C.; Hu, Y.; Yuen, K.-Y.; et al. Structural and Functional Basis of SARS-CoV-2 Entry by Using Human ACE2. Cell 2020, 181, 894–904.e9. [Google Scholar] [CrossRef]
- Scopus Preview—Scopus—Document Details—Single-Cell Transcriptome Analysis of the Novel Coronavirus (SARS-CoV-2) Associated Gene ACE2 Expression in Normal and Non-Obstructive Azoospermia (NOA) Human Male Testes. Available online: https://www.scopus.com/record/display.uri?eid=2-s2.0-85085124021&origin=inward&txGid=c40616db96674ffe52e0079abee92424 (accessed on 4 March 2024).
- Rajput, S.K.; Logsdon, D.M.; Kile, B.; Engelhorn, H.J.; Goheen, B.; Khan, S.; Swain, J.; McCormick, S.; Schoolcraft, W.B.; Yuan, Y.; et al. Human Eggs, Zygotes, and Embryos Express the Receptor Angiotensin 1-Converting Enzyme 2 and Transmembrane Serine Protease 2 Protein Necessary for Severe Acute Respiratory Syndrome Coronavirus 2 Infection. F&S Sci. 2021, 2, 33–42. [Google Scholar] [CrossRef]
- Wu, M.; Ma, L.; Xue, L.; Zhu, Q.; Zhou, S.; Dai, J.; Yan, W.; Zhang, J.; Wang, S. Co-Expression of the SARS-CoV-2 Entry Molecules ACE2 and TMPRSS2 in Human Ovaries: Identification of Cell Types and Trends with Age. Genomics 2021, 113, 3449–3460. [Google Scholar] [CrossRef] [PubMed]
- Stanley, K.E.; Thomas, E.; Leaver, M.; Wells, D. Coronavirus Disease-19 and Fertility: Viral Host Entry Protein Expression in Male and Female Reproductive Tissues. Fertil. Steril. 2020, 114, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Reis, F.M.; Bouissou, D.R.; Pereira, V.M.; Camargos, A.F.; dos Reis, A.M.; Santos, R.A. Angiotensin-(1-7), Its Receptor Mas, and the Angiotensin-Converting Enzyme Type 2 Are Expressed in the Human Ovary. Fertil. Steril. 2011, 95, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Tanacan, A.; Yazihan, N.; Erol, S.A.; Anuk, A.T.; Yucel Yetiskin, F.D.; Biriken, D.; Ozgu-Erdinc, A.S.; Keskin, H.L.; Moraloglu Tekin, O.; Sahin, D. The Impact of COVID-19 Infection on the Cytokine Profile of Pregnant Women: A Prospective Case-Control Study. Cytokine 2021, 140, 155431. [Google Scholar] [CrossRef]
- Yu, N.; Li, W.; Kang, Q.; Xiong, Z.; Wang, S.; Lin, X.; Liu, Y.; Xiao, J.; Liu, H.; Deng, D.; et al. Clinical Features and Obstetric and Neonatal Outcomes of Pregnant Patients with COVID-19 in Wuhan, China: A Retrospective, Single-Centre, Descriptive Study. Lancet Infect. Dis. 2020, 20, 559–564. [Google Scholar] [CrossRef]
- Zeng, L.; Xia, S.; Yuan, W.; Yan, K.; Xiao, F.; Shao, J.; Zhou, W. Neonatal Early-Onset Infection With SARS-CoV-2 in 33 Neonates Born to Mothers with COVID-19 in Wuhan, China. JAMA Pediatr. 2020, 174, 722–725. [Google Scholar] [CrossRef]
- Matar, R.; Alrahmani, L.; Monzer, N.; Debiane, L.G.; Berbari, E.; Fares, J.; Fitzpatrick, F.; Murad, M.H. Clinical Presentation and Outcomes of Pregnant Women with Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2021, 72, 521–533. [Google Scholar] [CrossRef]
- Wong, S.F.; Chow, K.M.; Leung, T.N.; Ng, W.F.; Ng, T.K.; Shek, C.C.; Ng, P.C.; Lam, P.W.Y.; Ho, L.C.; To, W.W.K.; et al. Pregnancy and Perinatal Outcomes of Women with Severe Acute Respiratory Syndrome. Am. J. Obstet. Gynecol. 2004, 191, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wang, L.; Fang, C.; Peng, S.; Zhang, L.; Chang, G.; Xia, S.; Zhou, W. Clinical Analysis of 10 Neonates Born to Mothers with 2019-nCoV Pneumonia. Transl. Pediatr. 2020, 9, 510–560. [Google Scholar] [CrossRef]
- Wei, M.; Yuan, J.; Liu, Y.; Fu, T.; Yu, X.; Zhang, Z.-J. Novel Coronavirus Infection in Hospitalized Infants Under 1 Year of Age in China. JAMA 2020, 323, 1313–1314. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Chen, G.; Hou, H.; Liao, Q.; Chen, J.; Bai, H.; Lee, S.; Wang, C.; Li, H.; Cheng, L.; et al. Analysis of Sex Hormones and Menstruation in COVID-19 Women of Childbearing Age. Reprod. Biomed. Online 2021, 42, 260–267. [Google Scholar] [CrossRef] [PubMed]
- 1 in 6 People Globally Affected by Infertility: WHO. Available online: https://www.who.int/news/item/04-04-2023-1-in-6-people-globally-affected-by-infertility (accessed on 23 November 2023).
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing ‘Reviewers’ to ‘Authors’ Assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, V.; Glaß, K.; Leßmann, M.-E.; Schaar, J.; Klimova, A.; Wimberger, P.; Goeckenjan, M. Assisted Reproduction after SARS-CoV-2-Infection: Results of a Single-Center Cohort-Study. Arch. Gynecol. Obstet. 2023, 309, 305–313. [Google Scholar] [CrossRef]
- Huri, M.; Noferi, V.; Renda, I.; Piazzini, F.; Benemei, S.; Coccia, M.E. The COVID-19 Pandemic Impact on the Outcome of Medically Assisted Reproduction Pregnancies. Front. Reprod. Health 2022, 4, 860425. [Google Scholar] [CrossRef]
- Rageh, K.E.A.; Farag, E.A.; Behery, M.A.; Badreldin, M.A.; Ali, E.A. The Impact of Previous Exposure to COVID-19 on the Outcome of ICSI Cycles. JBRA Assist. Reprod. 2023, 27, 367–372. [Google Scholar] [CrossRef]
- Engels Calvo, V.; Cruz Melguizo, S.; Abascal-Saiz, A.; Forcén Acebal, L.; Sánchez-Migallón, A.; Pintado Recarte, P.; Cuenca Marín, C.; Marcos Puig, B.; Del Barrio Fernández, P.G.; Nieto Velasco, O.; et al. Perinatal Outcomes of Pregnancies Resulting from Assisted Reproduction Technology in SARS-CoV-2-Infected Women: A Prospective Observational Study. Fertil. Steril. 2021, 116, 731–740. [Google Scholar] [CrossRef]
- Rodríguez-Varela, C.; Mariani, G.; Dolz, P.; García-Velasco, J.A.; Serra, V.; Pellicer, A.; Labarta, E. Impact of COVID-19 on Infertility Treatments: Not Even a Global Pandemic Was Strong Enough to Hamper Successful Pregnancies. Life 2021, 12, 6. [Google Scholar] [CrossRef]
- Ata, B.; Gianaroli, L.; Lundin, K.; Mcheik, S.; Mocanu, E.; Rautakallio-Hokkanen, S.; Tapanainen, J.S.; Vermeulen, N.; Veiga, A. Outcomes of SARS-CoV-2 Infected Pregnancies after Medically Assisted Reproduction. Hum. Reprod. 2021, 36, 2883–2890. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Liu, Y.; Xia, L.; Zhao, Y.; Tian, L.; Xu, D.; Su, Q.; Hu, Y.; Xie, Q.; Chen, J.; et al. Effect of Prior Female SARS-CoV-2 Infection on IVF Outcomes: A Prospective Cohort Study. Front. Endocrinol. 2023, 14, 1239903. [Google Scholar] [CrossRef]
- Epelboin, S.; Labrosse, J.; De Mouzon, J.; Fauque, P.; Gervoise-Boyer, M.-J.; Levy, R.; Sermondade, N.; Hesters, L.; Bergère, M.; Devienne, C.; et al. Obstetrical Outcomes and Maternal Morbidities Associated with COVID-19 in Pregnant Women in France: A National Retrospective Cohort Study. PLoS Med. 2021, 18, e1003857. [Google Scholar] [CrossRef] [PubMed]
- Ziert, Y.; Abou-Dakn, M.; Backes, C.; Banz-Jansen, C.; Bock, N.; Bohlmann, M.; Engelbrecht, C.; Gruber, T.M.; Iannaccone, A.; Jegen, M.; et al. Maternal and Neonatal Outcomes of Pregnancies with COVID-19 after Medically Assisted Reproduction: Results from the Prospective COVID-19-Related Obstetrical and Neonatal Outcome Study. Am. J. Obstet. Gynecol. 2022, 227, e1–e495. [Google Scholar] [CrossRef]
- Dolgushina, N.V.; Menzhinskaya, I.V.; Ermakova, D.M.; Frankevich, N.A.; Vtorushina, V.V.; Sukhikh, G.T. The Effect of COVID-19 Severity, Associated Serum Autoantibodies and Time Interval after the Disease on the Outcomes of Fresh Oocyte ART Cycles in Non-Vaccinated Patients. J. Clin. Med. 2023, 12, 4370. [Google Scholar] [CrossRef] [PubMed]
- Banker, M.; Arora, P.; Banker, J.; Shah, A.; Gupta, R.; Shah, S. Impact of COVID-19 Pandemic on Clinical and Embryological Outcomes of Assisted Reproductive Techniques. J. Hum. Reprod. Sci. 2022, 15, 150–156. [Google Scholar] [CrossRef]
- Madjunkov, M.; Dviri, M.; Librach, C. A Comprehensive Review of the Impact of COVID-19 on Human Reproductive Biology, Assisted Reproduction Care and Pregnancy: A Canadian Perspective. J. Ovarian Res. 2020, 13, 140. [Google Scholar] [CrossRef]
- Age and Infertility: The Biological Clock: Fact or Fiction? Available online: https://fertilitycenterlv.com/blog/your-biological-clock-fact-or-fiction-the-effects-of-age-on-female-fertility/ (accessed on 22 November 2023).
- Huang, J.; Xia, L.; Lin, J.; Liu, B.; Zhao, Y.; Xin, C.; Ai, X.; Cao, W.; Zhang, X.; Tian, L.; et al. No Effect of Inactivated SARS-CoV-2 Vaccination on in Vitro Fertilization Outcomes: A Propensity Score-Matched Study. J. Inflamm. Res. 2022, 15, 839–849. [Google Scholar] [CrossRef]
- Dong, M.; Wu, S.; Zhang, X.; Zhao, N.; Qi, J.; Zhao, D.; Sang, Y.; Tan, J. Effects of COVID-19 Vaccination Status, Vaccine Type, and Vaccination Interval on IVF Pregnancy Outcomes in Infertile Couples. J. Assist. Reprod. Genet. 2022, 39, 1849–1859. [Google Scholar] [CrossRef]
- Wang, C.; Tang, D.; Liu, J.; Zhang, S.; Xu, Y.; Qiao, J.; Cao, Y. Association Between COVID-19 Vaccination and Artificial Insemination Outcomes for Couples Experiencing Infertility. JAMA Netw. Open 2022, 5, e2247216. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, X.; Lin, G.; Gong, F.; Hocher, B. Safety of COVID-19 Vaccination in Women Undergoing IVF/ICSI Treatment—Clinical Study and Systematic Review. Front. Immunol. 2023, 13, 1054273. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Dong, Y.; Li, G.; Yin, B.; Tang, X.; Jia, L.; Zhang, X.; Yang, W.; Wang, C.; Peng, X.; et al. Pregnancy Outcomes Following Natural Conception and Assisted Reproduction Treatment in Women Who Received COVID-19 Vaccination Prior to Conception: A Population-Based Cohort Study in China. Front. Med. 2023, 10, 1250165. [Google Scholar] [CrossRef] [PubMed]
- Chillon, T.S.; Weiss, G.; Demircan, K.; Minich, W.B.; Schenk, M.; Schomburg, L. Antibodies to SARS-CoV-2 in Follicular Fluids and Their Association with Assisted Reproduction. Front. Immunol. 2023, 14, 1120328. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-L.; Chen, Y.-H.; Zhang, S.-P.; Wu, X.-Q.; Wang, X.-P. Effects of the Severe Acute Respiratory Syndrome Coronavirus 2 Inactivated Vaccine on the Outcome of Frozen Embryo Transfers: A Large Scale Clinical Study. Int. J. Womens Health 2023, 15, 1305–1316. [Google Scholar] [CrossRef]
- European IVF Monitoring Consortium (EIM), for the European Society of Human Reproduction and Embryology (ESHRE); Wyns, C.; Geyter, C.D.; Calhaz-Jorge, C.; Kupka, M.S.; Motrenko, T.; Smeenk, J.; Bergh, C.; Tandler-Schneider, A.; Rugescu, I.A.; et al. ART in Europe, 2018: Results Generated from European Registries by ESHRE. Hum. Reprod. Open 2022, 2022, hoac022. [Google Scholar] [CrossRef]
- European IVF Monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE); Smeenk, J.; Wyns, C.; De Geyter, C.; Kupka, M.; Bergh, C.; Cuevas Saiz, I.; De Neubourg, D.; Rezabek, K.; Tandler-Schneider, A.; et al. ART in Europe, 2019: Results Generated from European Registries by ESHRE. Hum. Reprod. 2023, 38, dead197. [Google Scholar] [CrossRef]
- Smeenk, J.; Wyns, C.; De Geyter, C.; Bergh, C.; Cuevas, I.; de Neubourg, D.; Kupka, M.S.; Rezabek, K.; Rugescu, I.; Tandler-Schneider, A.; et al. O-153 Assisted Reproductive Technology (ART) in Europe 2020 and Development of a Strategy of Vigilance: Preliminary Results Generated from European Registers by the ESHRE EIM Consortium. Hum. Reprod. 2023, 38, dead093.014. [Google Scholar] [CrossRef]
- Qiao, J.; National Expert Group for Quality Management on Assisted Reproductive Technology. Impacts of COVID-19 pandemics on the services of assisted reproductive technology in Chinese mainland: A national cross-sectional survey. Chin. J. Reprod. Contracept. 2021, 41, 7–11. [Google Scholar]
- Wei, L.; Zhang, J.; Deng, X.; Luo, C.; Bo, L.; Gao, S.; Qian, F.; Lu, S.; Mao, C. Impacts of the COVID-19 Pandemic on Chinese Assisted Reproductive Technology Institutions and Human Sperm Banks: Reflections in the Post-Pandemic Era. J. Health Popul. Nutr. 2023, 42, 82. [Google Scholar] [CrossRef]
- Allotey, J.; Fernandez, S.; Bonet, M.; Stallings, E.; Yap, M.; Kew, T.; Zhou, D.; Coomar, D.; Sheikh, J.; Lawson, H.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Adamson, G.D.; de Mouzon, J.; Chambers, G.M.; Zegers-Hochschild, F.; Mansour, R.; Ishihara, O.; Banker, M.; Dyer, S. International Committee for Monitoring Assisted Reproductive Technology: World Report on Assisted Reproductive Technology, 2011. Fertil. Steril. 2018, 110, 1067–1080. [Google Scholar] [CrossRef] [PubMed]
- Balachandren, N.; Davies, M.C.; Hall, J.A.; Stephenson, J.M.; David, A.L.; Barrett, G.; O’Neill, H.C.; Ploubidis, G.B.; Yasmin, E.; Mavrelos, D. SARS-CoV-2 Infection in the First Trimester and the Risk of Early Miscarriage: A UK Population-Based Prospective Cohort Study of 3041 Pregnancies Conceived during the Pandemic. Hum. Reprod. 2022, 37, 1126–1133. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical Transmission of Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef] [PubMed]
- Setti, P.E.L.-; Cirillo, F.; Immediata, V.; Morenghi, E.; Canevisio, V.; Ronchetti, C.; Baggiani, A.; Albani, E.; Patrizio, P. First Trimester Pregnancy Outcomes in a Large IVF Center from the Lombardy County (Italy) during the Peak COVID-19 Pandemic. Sci. Rep. 2021, 11, 16529. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Zou, Y.; Guo, Y.; Lv, X.; Chen, J.; Guo, X.; Liu, Q. Effect of COVID-19 Inactivated Vaccine on Peripheral Blood Anti-Β2-GPI Antibody and Outcomes in Vitro Fertilization-Embryo Transplantation. Int. Immunopharmacol. 2023, 122, 110596. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Wang, M.; Xue, X.; Li, N.; Chen, L.; Shi, J. Association between Time Interval from COVID-19 Vaccination to In Vitro Fertilization and Pregnancy Rate after Fresh Embryo Transfer. JAMA Netw. Open 2022, 5, e2236609. [Google Scholar] [CrossRef]
- Cao, M.; Wu, Y.; Lin, Y.; Xu, Z.; Liang, Z.; Huang, Q.; Li, S.; Liu, H.; An, C.; Luo, Y.; et al. Inactivated Covid-19 Vaccine Did Not Undermine Live Birth and Neonatal Outcomes of Women with Frozen-Thawed Embryo Transfer. Hum. Reprod. 2022, 37, 2942–2951. [Google Scholar] [CrossRef]
- Zauche, L.H.; Wallace, B.; Smoots, A.N.; Olson, C.K.; Oduyebo, T.; Kim, S.Y.; Petersen, E.E.; Ju, J.; Beauregard, J.; Wilcox, A.J.; et al. Receipt of mRNA Covid-19 Vaccines and Risk of Spontaneous Abortion. N. Engl. J. Med. 2021, 385, 1533–1535. [Google Scholar] [CrossRef]
- Wu, Y.; Cao, M.; Lin, Y.; Xu, Z.; Liang, Z.; Huang, Q.; Li, S.; Li, L.; Meng, Y.; An, C.; et al. Inactivated COVID-19 Vaccination Does Not Affect In Vitro Fertilization Outcomes in Women. Hum. Reprod. 2022, 37, 2054–2062. [Google Scholar] [CrossRef]
- Allahbadia, G. Will Procreation Ever Be The Same After COVID-19? J. Obstet. Gynaecol. India 2021, 71, 1–6. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]




| Study | Study Type | City, Country | Publication Date | No. COVID-19 Positive Participants | Mean Age ± SD | Pregnancy | Birth | Miscarriage |
|---|---|---|---|---|---|---|---|---|
| Eckstein V et al. [38] | cohort-study | Germany | 10 October 2023 | 1581 treatment cycles | 35.8 ± 4.1 (23.1–49.5) | 19/87 (21.84%) | not published yet | 10/19 (52.63%) |
| Huri et al. [39] | retro-prospective cohort study | Florence, Italy | 25 April 2022 | 749 | 219 (100%) | 165 (22.02%) | 98 | |
| Rageh et al. [40] | observational study | Manama, Bahrain; Kingdom of Saudi Arabia | 12 September 2023 | 88 | 32.14 ± (4.773) | 32 (36.4%) | ||
| Engels Calvo et al. [41] | multicenter, prospective, observational study | 78 Spanish centers | 12 April 2021 | 74 | 39.6 | 74 (5.5%) | ||
| Rodríguez-Varela et al. [42] | retrospective, multicentric, and double-arm study | Spain, Lisbon and Rome | 21 December 2021 | 6 | 38.6 | 6 | 39 (4.5%)-overall miscarriage rate | |
| ESHRE COVID-19 Working Group et al. [43] | retrospective, multicentric studies | 32 countries worldwide | 13 September 2021 | 105 | 33.7 ± 6.1 | 25 | 67 | 10 (12.5%) |
| Huang J et al. [44] | prospective cohort study | China | 4 October 2023 | 252 | 32.3 ± 5.0 | 83 (70.3%) | ||
| Epelboin et al. [45] | prospective clinical study | France | 30 November 2021. | 16 | 31.1 (±5.9) | 16 (1.8%) | No data | |
| Ziert et al. [46] | multicentric, prospective, observational study | Germany, Austria | 19 April 2022 | 65 | 34.09 ± 5.12 | 65 | 57/65 (87,69%) | 0/57 (0.0) |
| Dolgushina et al. [47] | observational prospective study | Russia | 29 June 2023 | 135 | 34 (31–37) | 39 (28.9%) | 30 (22.2%) | 31 (23.1%) |
| Banker et al. [48] | retrospective cohort study | Ahmedabad, India | 30 June 2022 | 606 | 30.7 | 47.6% Fresh ET 68.7% Frozen ET | 32.4% Fresh ET 46.3% Frozen ET | 10% Fresh ET 6.73% Frozen ET |
| TOTAL | 2096 | 562 | 335 | 188 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milostić-Srb, A.; Srb, N.; Talapko, J.; Meštrović, T.; Žiger, T.; Pačarić, S.; Fureš, R.; Makarović, V.; Škrlec, I. The Effect of COVID-19 and COVID-19 Vaccination on Assisted Human Reproduction Outcomes: A Systematic Review and Meta-Analysis. Diseases 2024, 12, 201. https://doi.org/10.3390/diseases12090201
Milostić-Srb A, Srb N, Talapko J, Meštrović T, Žiger T, Pačarić S, Fureš R, Makarović V, Škrlec I. The Effect of COVID-19 and COVID-19 Vaccination on Assisted Human Reproduction Outcomes: A Systematic Review and Meta-Analysis. Diseases. 2024; 12(9):201. https://doi.org/10.3390/diseases12090201
Chicago/Turabian StyleMilostić-Srb, Andrea, Nika Srb, Jasminka Talapko, Tomislav Meštrović, Tihomil Žiger, Stana Pačarić, Rajko Fureš, Vedrana Makarović, and Ivana Škrlec. 2024. "The Effect of COVID-19 and COVID-19 Vaccination on Assisted Human Reproduction Outcomes: A Systematic Review and Meta-Analysis" Diseases 12, no. 9: 201. https://doi.org/10.3390/diseases12090201
APA StyleMilostić-Srb, A., Srb, N., Talapko, J., Meštrović, T., Žiger, T., Pačarić, S., Fureš, R., Makarović, V., & Škrlec, I. (2024). The Effect of COVID-19 and COVID-19 Vaccination on Assisted Human Reproduction Outcomes: A Systematic Review and Meta-Analysis. Diseases, 12(9), 201. https://doi.org/10.3390/diseases12090201