
Therapeutic Effects of Semaglutide on Nonalcoholic Fatty Liver Disease with Type 2 Diabetes Mellitus and Obesity: An Open-Label Controlled Trial

 , , , , and
, , , , and
Abstract
1. Introduction
2. Methods
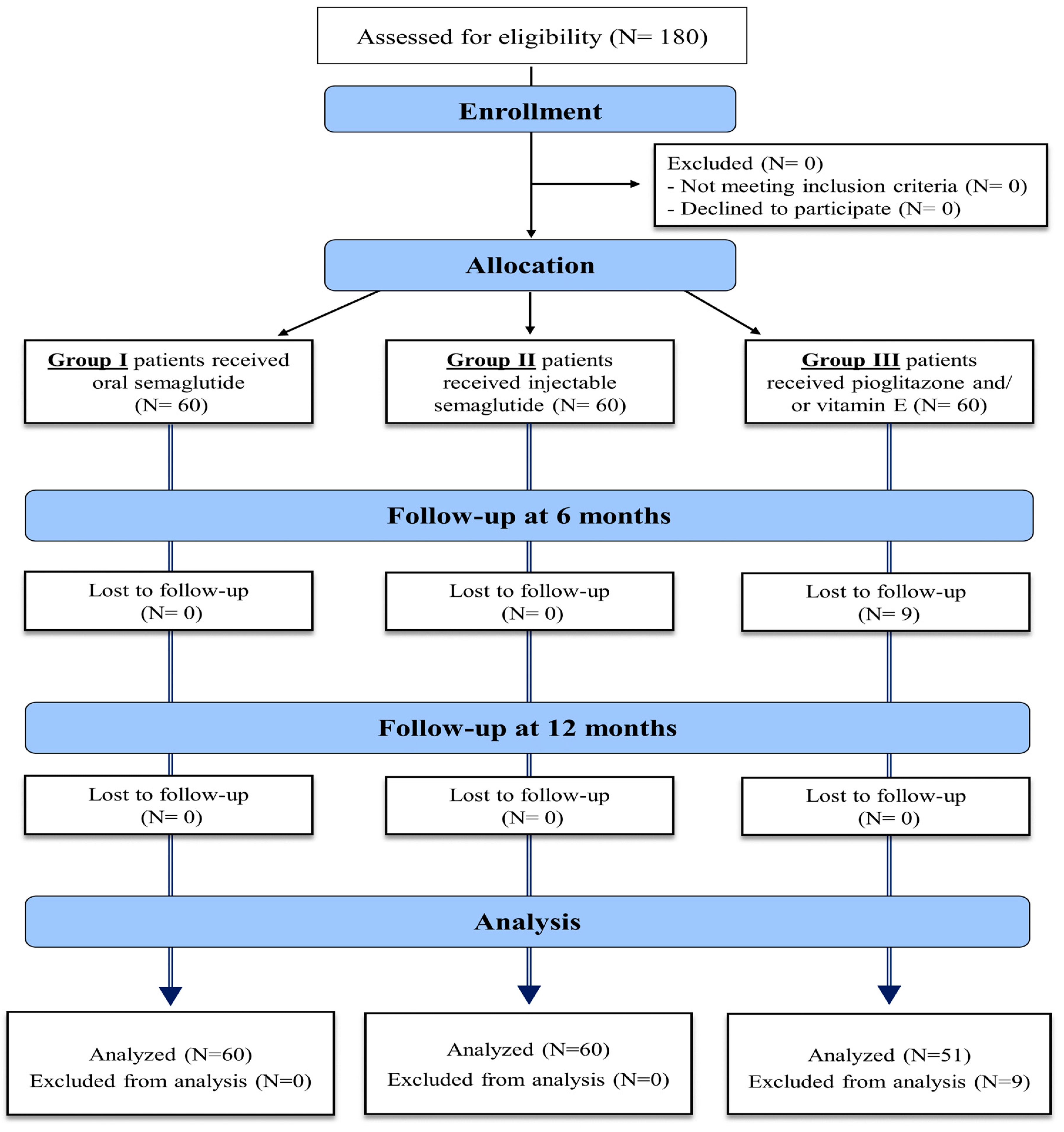
2.1. Study Design
2.2. Sample Size and Technique
2.3. Study Population
2.4. Study Interventions
2.5. Outcome Measures
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Patients
3.2. Changes in BMI, AST, and ALT among the Study Groups
3.3. Changes in Lipid Profile among the Study Groups
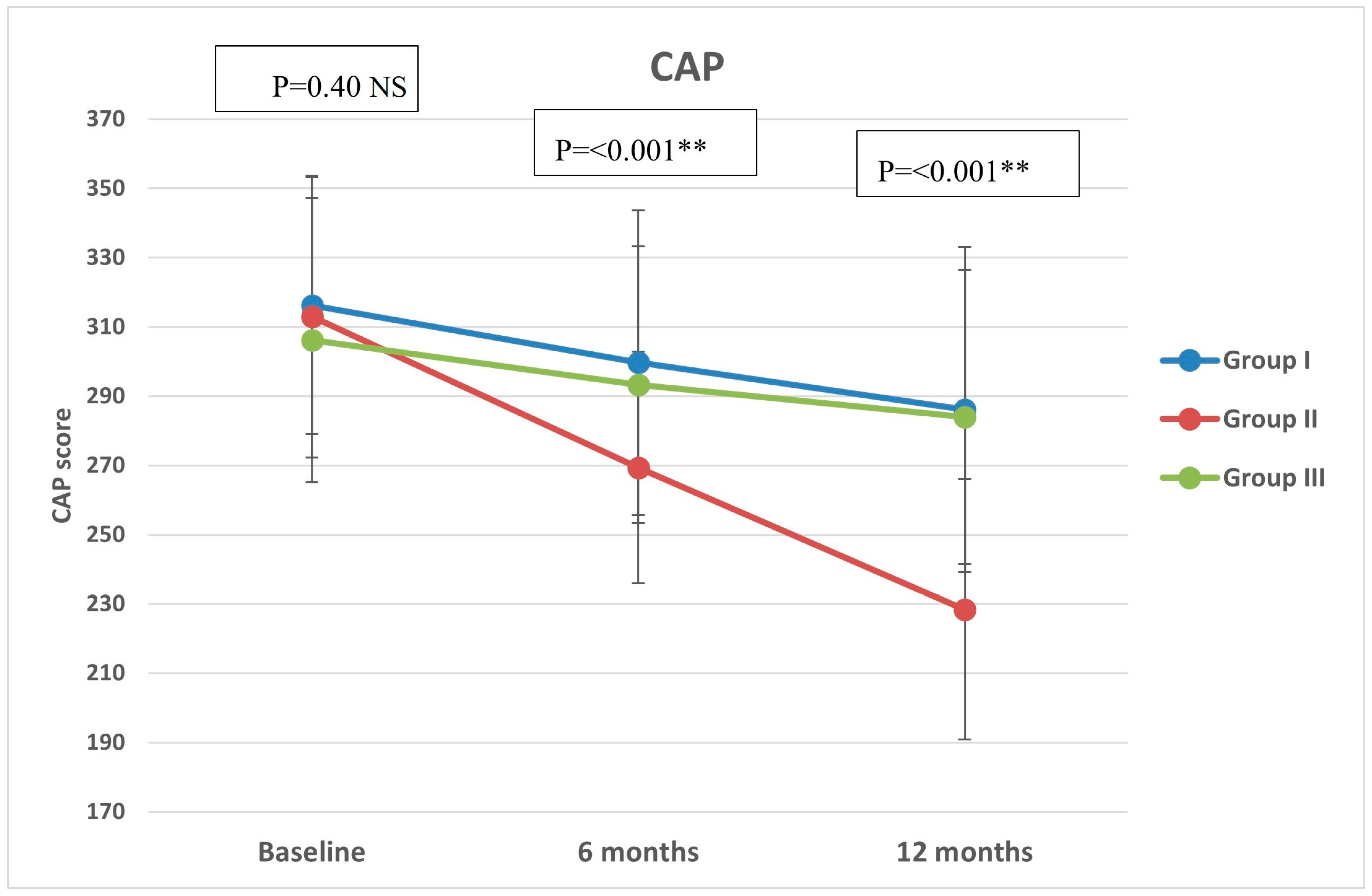
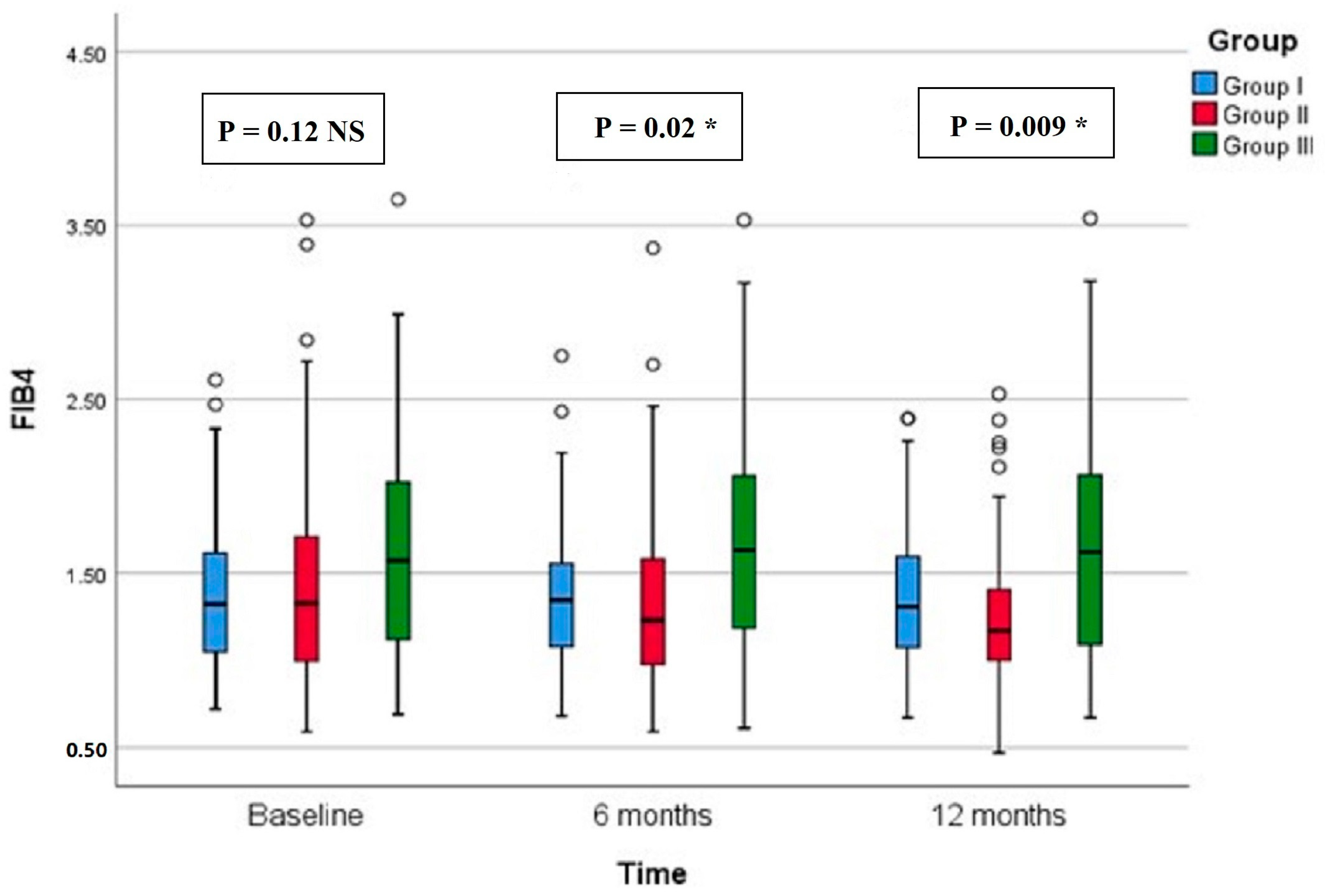
3.4. Changes in Liver Stiffness and Fibrosis Parameters among the Study Groups
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global Burden of NAFLD and NASH: Trends, Predictions, Risk Factors and Prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- Teng, M.L.; Ng, C.H.; Huang, D.Q.; Chan, K.E.; Tan, D.J.; Lim, W.H.; Yang, J.D.; Tan, E.; Muthiah, M.D. Global Incidence and Prevalence of Nonalcoholic Fatty Liver Disease. Clin. Mol. Hepatol. 2023, 29, S32–S42. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The Global Epidemiology of Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH): A Systematic Review. Hepatology 2023, 77, 1335. [Google Scholar] [CrossRef] [PubMed]
- Boccatonda, A.; Andreetto, L.; D’Ardes, D.; Cocco, G.; Rossi, I.; Vicari, S.; Schiavone, C.; Cipollone, F.; Guagnano, M.T. From NAFLD to MAFLD: Definition, Pathophysiological Basis and Cardiovascular Implications. Biomedicines 2023, 11, 883. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Das, S.; Samajdar, S.S.; Joshi, S.R. Role of Semaglutide in the Treatment of Nonalcoholic Fatty Liver Disease or Non-Alcoholic Steatohepatitis: A Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2023, 17, 102849. [Google Scholar] [CrossRef] [PubMed]
- Ghazanfar, H.; Kandhi, S.D.; Nawaz, I.; Javed, N.; Abraham, M.C.; Farag, M.; Mahasamudram, J.; Patel, V.B.; Altaf, F.; Patel, H. Role of Glucagon-Like Peptide-1 Receptor Agonists in the Management of Non-Alcoholic Steatohepatitis: A Clinical Review Article. Cureus 2021, 13, e15141. [Google Scholar] [CrossRef] [PubMed]
- Barritt, A.S.; Marshman, E.; Noureddin, M. Review Article: Role of Glucagon-like Peptide-1 Receptor Agonists in Non-Alcoholic Steatohepatitis, Obesity and Diabetes-What Hepatologists Need to Know. Aliment. Pharmacol. Ther. 2022, 55, 944–959. [Google Scholar] [CrossRef]
- Zhu, Y.; Xu, J.; Zhang, D.; Mu, X.; Shi, Y.; Chen, S.; Wu, Z.; Li, S. Efficacy and Safety of GLP-1 Receptor Agonists in Patients With Type 2 Diabetes Mellitus and Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 769069. [Google Scholar] [CrossRef]
- Harrison, S.A.; Calanna, S.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.; Sejling, A.-S.; Newsome, P.N. Semaglutide for the Treatment of Non-Alcoholic Steatohepatitis: Trial Design and Comparison of Non-Invasive Biomarkers. Contemp. Clin. Trials 2020, 97, 106174. [Google Scholar] [CrossRef]
- Patikorn, C.; Veettil, S.K.; Phisalprapa, P.; Pham, T.; Kowdley, K.V.; Chaiyakunapruk, N. Horizon Scanning of Therapeutic Modalities for Nonalcoholic Steatohepatitis. Ann. Hepatol. 2021, 24, 100315. [Google Scholar] [CrossRef]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.-S.; Harrison, S.A. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Dichtel, L.E. The Glucagon-Like Peptide-1 Receptor Agonist, Semaglutide, for the Treatment of Nonalcoholic Steatohepatitis. Hepatology 2021, 74, 2290–2292. [Google Scholar] [CrossRef] [PubMed]
- Katsuyama, H.; Hakoshima, M.; Kaji, E.; Mino, M.; Kakazu, E.; Iida, S.; Adachi, H.; Kanto, T.; Yanai, H. Effects of Once-Weekly Semaglutide on Cardiovascular Risk Factors and Metabolic Dysfunction-Associated Steatotic Liver Disease in Japanese Patients with Type 2 Diabetes: A Retrospective Longitudinal Study Based on Real-World Data. Biomedicines 2024, 12, 1001. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Vergani, M.; Perseghin, G. Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: Screening, Diagnosis, and Treatment. J. Clin. Med. 2023, 12, 5597. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Muraca, E.; Vergani, M.; Invernizzi, P.; Perseghin, G. Advancements in Pharmacological Treatment of NAFLD/MASLD: A Focus on Metabolic and Liver-Targeted Interventions. Gastroenterol. Rep. 2023, 12, goae029. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Francque, S.; Behling, C.A.; Cejvanovic, V.; Cortez-Pinto, H.; Iyer, J.S.; Krarup, N.; Le, Q.; Sejling, A.-S.; Tiniakos, D.; et al. Artificial Intelligence Scoring of Liver Biopsies in a Phase II Trial of Semaglutide in Nonalcoholic Steatohepatitis. Hepatology 2024, 80, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.; Andersen, G.; Hockings, P.; Johansson, L.; Morsing, A.; Sundby Palle, M.; Vogl, T.; Loomba, R.; Plum-Mörschel, L. Randomised Clinical Trial: Semaglutide versus Placebo Reduced Liver Steatosis but Not Liver Stiffness in Subjects with Non-Alcoholic Fatty Liver Disease Assessed by Magnetic Resonance Imaging. Aliment. Pharmacol. Ther. 2021, 54, 1150–1161. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Abdelmalek, M.F.; Armstrong, M.J.; Jara, M.; Kjær, M.S.; Krarup, N.; Lawitz, E.; Ratziu, V.; Sanyal, A.J.; Schattenberg, J.M.; et al. Semaglutide 2·4 Mg Once Weekly in Patients with Non-Alcoholic Steatohepatitis-Related Cirrhosis: A Randomised, Placebo-Controlled Phase 2 Trial. Lancet Gastroenterol. Hepatol. 2023, 8, 511–522. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Cusi, K.; Hilliard, M.E.; Isaacs, D.; et al. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46, S49–S67. [Google Scholar] [CrossRef]
- Baldassarre, M.P.A.; Di Dalmazi, G.; Coluzzi, S.; Carrieri, F.; Febo, F.; Centorame, G.; Cassino, P.; Piacentino, L.; Baroni, M.G.; Consoli, A.; et al. Oral Semaglutide in Routine Clinical Practice: Characteristics of People with Type 2 Diabetes Started on the Drug and Changes in Their Clinical Parameters after 24 Weeks of Treatment. J. Clin. Med. 2024, 13, 3054. [Google Scholar] [CrossRef]
- Rosenstock, J.; Allison, D.; Birkenfeld, A.L.; Blicher, T.M.; Deenadayalan, S.; Jacobsen, J.B.; Serusclat, P.; Violante, R.; Watada, H.; Davies, M.; et al. Effect of Additional Oral Semaglutide vs Sitagliptin on Glycated Hemoglobin in Adults with Type 2 Diabetes Uncontrolled with Metformin Alone or With Sulfonylurea: The PIONEER 3 Randomized Clinical Trial. JAMA 2019, 321, 1466–1480. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; Biernacki, D.M.; Kalavalapalli, S.; Lomonaco, R.; Subbarayan, S.K.; Lai, J.; Tio, F.; Suman, A.; Orsak, B.K.; Hecht, J.; et al. Role of Vitamin E for Nonalcoholic Steatohepatitis in Patients with Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2019, 42, 1481–1488. [Google Scholar] [CrossRef] [PubMed]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, Vitamin E, or Placebo for Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the Clinical Assessment and Management of Nonalcoholic Fatty Liver Disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Sirli, R.; Sporea, I. Controlled Attenuation Parameter for Quantification of Steatosis: Which Cut-Offs to Use? Can. J. Gastroenterol. Hepatol. 2021, 2021, 6662760. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD Fibrosis Score: A Noninvasive System That Identifies Liver Fibrosis in Patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Cigrovski Berkovic, M.; Rezic, T.; Bilic-Curcic, I.; Mrzljak, A. Semaglutide Might Be a Key for Breaking the Vicious Cycle of Metabolically Associated Fatty Liver Disease Spectrum? World J. Clin. Cases 2022, 10, 6759–6768. [Google Scholar] [CrossRef]
- Godoy-Matos, A.F.; Silva Júnior, W.S.; Valerio, C.M. NAFLD as a Continuum: From Obesity to Metabolic Syndrome and Diabetes. Diabetol. Metab. Syndr. 2020, 12, 60. [Google Scholar] [CrossRef]
- Niu, S.; Chen, S.; Chen, X.; Ren, Q.; Yue, L.; Pan, X.; Zhao, H.; Li, Z.; Chen, X. Semaglutide Ameliorates Metabolism and Hepatic Outcomes in an NAFLD Mouse Model. Front Endocrinol. 2022, 13, 1046130. [Google Scholar] [CrossRef]
- Lee, H.A.; Kim, H.Y. Therapeutic Mechanisms and Clinical Effects of Glucagon-like Peptide 1 Receptor Agonists in Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2023, 24, 9324. [Google Scholar] [CrossRef]
- Petrovic, A.; Igrec, D.; Rozac, K.; Bojanic, K.; Kuna, L.; Kolaric, T.O.; Mihaljevic, V.; Sikora, R.; Smolic, R.; Glasnovic, M.; et al. The Role of GLP1-RAs in Direct Modulation of Lipid Metabolism in Hepatic Tissue as Determined Using In Vitro Models of NAFLD. Curr. Issues Mol. Biol. 2023, 45, 4544–4556. [Google Scholar] [CrossRef]
- Newsome, P.; Francque, S.; Harrison, S.; Ratziu, V.; Van Gaal, L.; Calanna, S.; Hansen, M.; Linder, M.; Sanyal, A. Effect of Semaglutide on Liver Enzymes and Markers of Inflammation in Subjects with Type 2 Diabetes and/or Obesity. Aliment. Pharmacol. Ther. 2019, 50, 193–203. [Google Scholar] [CrossRef]
- Pratley, R.E.; Aroda, V.R.; Lingvay, I.; Lüdemann, J.; Andreassen, C.; Navarria, A.; Viljoen, A. SUSTAIN 7 investigators Semaglutide versus Dulaglutide Once Weekly in Patients with Type 2 Diabetes (SUSTAIN 7): A Randomised, Open-Label, Phase 3b Trial. Lancet Diabetes Endocrinol. 2018, 6, 275–286. [Google Scholar] [CrossRef]
- Volpe, S.; Lisco, G.; Fanelli, M.; Racaniello, D.; Colaianni, V.; Triggiani, D.; Donghia, R.; Crudele, L.; Rinaldi, R.; Sabbà, C.; et al. Once-Weekly Subcutaneous Semaglutide Improves Fatty Liver Disease in Patients with Type 2 Diabetes: A 52-Week Prospective Real-Life Study. Nutrients 2022, 14, 4673. [Google Scholar] [CrossRef] [PubMed]
- Carretero-Gómez, J.; Carrasco-Sánchez, F.J.; Fernández-Rodríguez, J.M.; Casado-Escribano, P.; Miramontes-González, J.P.; Seguí-Ripoll, J.M.; Ena, J.; Arévalo-Lorido, J.C. Effect of Semaglutide on Fatty Liver Disease Biomarkers in Patients with Diabetes and Obesity. Rev. Clínica Española 2023, 223, 134–143. [Google Scholar] [CrossRef]
- Adeghate, E.A. GLP-1 Receptor Agonists in the Treatment of Diabetic Non–Alcoholic Steatohepatitis Patients. Expert. Opin. Pharmacother. 2024, 25, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Dunphy, J.L.; Taylor, R.G.; Fuller, P.J. Tissue Distribution of Rat Glucagon Receptor and GLP-1 Receptor Gene Expression. Mol. Cell Endocrinol. 1998, 141, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Pyke, C.; Heller, R.S.; Kirk, R.K.; Ørskov, C.; Reedtz-Runge, S.; Kaastrup, P.; Hvelplund, A.; Bardram, L.; Calatayud, D.; Knudsen, L.B. GLP-1 Receptor Localization in Monkey and Human Tissue: Novel Distribution Revealed with Extensively Validated Monoclonal Antibody. Endocrinology 2014, 155, 1280–1290. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Targher, G. Glucagon-Like Peptide-1 Receptor Agonists for Treatment of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis: An Updated Meta-Analysis of Randomized Controlled Trials. Metabolites 2021, 11, 73. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; Stender, S.; Pietrelli, A.; Mancina, R.M.; Cespiati, A.; Petta, S.; Pelusi, S.; Pingitore, P.; Badiali, S.; Maggioni, M.; et al. Causal Relationship of Hepatic Fat with Liver Damage and Insulin Resistance in Nonalcoholic Fatty Liver. J. Intern. Med. 2018, 283, 356–370. [Google Scholar] [CrossRef] [PubMed]
- Hachuła, M.; Kosowski, M.; Basiak, M.; Okopień, B. Does Therapy with Glucagon-like Peptide 1 Receptor Agonists Have an Effect on Biochemical Markers of Metabolic-Dysfunction-Associated Steatotic Liver Disease (MASLD)? Pleiotropic Metabolic Effect of Novel Antidiabetic Drugs in Patients with Diabetes—Interventional Study. Pharmaceuticals 2023, 16, 1190. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and Cardiovascular Outcomes in Type 2 Diabetes (REWIND): A Double-Blind, Randomised Placebo-Controlled Trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; LEAN trial team; Abouda, G.; et al. Liraglutide Safety and Efficacy in Patients with Non-Alcoholic Steatohepatitis (LEAN): A Multicentre, Double-Blind, Randomised, Placebo-Controlled Phase 2 Study. Lancet 2016, 387, 679–690. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group I (Rybelsus) (n = 60) | Group II (Ozempic) (n = 60) | Group III (Conventional) (n = 60) | Test | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | Mean ± SD | 47.8 ± 5.41 | 46.83 ± 6.99 | 47.35 ± 5.74 | 0.38 | 0.69 | |||
| Range | 35–58 | 29–60 | 37–59 | NS # | |||||
| Variable | No | % | No | % | No | % | Test | p | |
| Sex | Female | 28 | 46.7 | 30 | 50 | 28 | 46.7 | 0.18 | 0.92 |
| Male | 32 | 53.3 | 30 | 50 | 32 | 53.3 | NS $ | ||
| Residence | Rural | 31 | 51.7 | 32 | 53.3 | 31 | 51.7 | 0.05 | 0.98 |
| Urban | 9 | 48.3 | 28 | 46.7 | 29 | 48.3 | NS $ | ||
| Co-morbidities | No | 42 | 70 | 36 | 60 | 47 | 78.3 | 7.41 | 0.49 NS $ |
| HTN | 13 | 21.7 | 19 | 31.7 | 12 | 20 | |||
| IHD | 1 | 1.7 | 1 | 1.7 | 1 | 1.7 | |||
| Gout | 3 | 5 | 3 | 5 | 0 | 0 | |||
| Hypothyroidism | 1 | 1.7 | 1 | 1.7 | 0 | 0 | |||
| Drugs | OHG | 13 | 21.7 | 18 | 30 | 17 | 28.3 | 1.19 | 0.55 NS $ |
| Insulin | 6 | 10 | 7 | 11.7 | 4 | 6.7 | 0.91 | 0.63 NS $ | |
| ACEI | 1 | 1.7 | 3 | 5 | 1 | 1.6 | 1.65 | 0.44 NS $ | |
| ARB + CCB | 3 | 5 | 4 | 6.7 | 3 | 5 | 0.21 | 0.90 NS $ | |
| BB | 0 | 0 | 1 | 1.7 | 0 | 0 | 2.01 | 0.37 NS $ | |
| Thiazide | 0 | 0 | 1 | 1.7 | 0 | 0 | 2.01 | 0.37 NS $ | |
| Smoking | No | 40 | 66.7 | 44 | 73.3 | 38 | 63.3 | 1.43 | 0.49 |
| Yes | 20 | 33.3 | 16 | 26.7 | 22 | 36.7 | NS $ | ||
| PA U/S | Mild fatty | 16 | 26.6 | 23 | 38.3 | 24 | 40 | 6.01 | |
| Moderate | 31 | 51.7 | 32 | 53.4 | 26 | 43.3 | 0.20 | ||
| Severe | 13 | 21.7 | 5 | 8.3 | 10 | 16.7 | NS $ | ||
| FBG: (mg/dL) | Mean ± SD | 110.22 ± 23.09 | 120.58 ± 32.32 | 113.65 ± 22.68 | 2.40 | 0.09 NS # | |||
| HbA1c: (%) | Mean ± SD | 7.6 ± 0.57 | 7.8 ± 0.87 | 7.41 ± 0.64 | 2.26 | 0.11 NS # | |||
| WBCs: (×103/mm3) | Mean ± SD | 8.17 ± 2.09 | 8.13 ± 1.79 | 8.81 ± 1.5 | 2.65 | 0.07 NS # | |||
| Hb: (g/dL) | Mean ± SD | 12.13 ± 0.98 | 12.37 ± 1.37 | 12.32 ± 0.90 | 0.77 | 0.47 NS # | |||
| Platelets: (×103/mm3) | Mean ± SD | 265.4 ± 53.39 | 269.53 ± 61.42 | 284.53 ± 49.33 | 2.02 | 0.14 NS # | |||
| T. Bilirubin: (mg/dL) | Median (range) | 0.7 (0.4–1.2) | 0.72(0.4–2.3) | 0.76(0.38–1.3) | 1.06 | 0.59 NS ^ | |||
| D. Bilirubin: (mg/dL) | Median (range) | 0.16(0.08–0.7) | 0.18(0.08–1.2) | 0.19(0.08–0.68) | 2.61 | 0.27 NS ^ | |||
| Albumin: (g/dL) | Mean ± SD | 4.13 ± 0.33 | 4.01 ± 0.35 | 4.02 ± 0.27 | 2.79 | 0.06 NS # | |||
| Total protein: (g/dL) | Mean ± SD | 7.35 ± 0.38 | 7.36 ± 0.37 | 7.47 ± 0.34 | 2.15 | 0.12 NS # | |||
| ALP: (U/L) | Mean ± SD | 100.83 ± 23.24 | 98.53 ± 18.77 | 106.55 ± 25.12 | 2 | 0.14 NS # | |||
| INR: | Mean ± SD | 0.98 ± 0.09 | 1 ± 0.09 | 1.02 ± 0.08 | 2.67 | 0.07 NS # | |||
| Creatinine: (mg/dL) | Mean ± SD | 0.73 ± 0.11 | 0.76 ± 0.15 | 0.75 ± 0.15 | 0.60 | 0.55 NS # | |||
| Urea: (mg/dL) | Mean ± SD | 13.49 ± 2.21 | 13.83 ± 2.24 | 13.95 ± 1.87 | 0.07 | 0.93 NS # | |||
| Variable | Group I (Rybelsus) (n = 60) | Group II (Ozempic) (n = 60) | Group III (Conventional) (n = 51) | Test | p | Post hoc † | |
|---|---|---|---|---|---|---|---|
| BMI: (kg/m2) | Baseline: | 33.06 ± 2.1 | 33.57 ± 2.17 | 32.69 ± 2.04 | 2.48 # | 0.09 NS | - |
| 6 months | 31.02 ± 3.08 | 29.65 ± 3.59 | 31.78 ± 2.89 | 6.28 # | 0.002 * | 0.06 NS 1 0.42 NS 2 0.002 *3 | |
| 12 months | 29.92 ± 3.15 | 28.25 ± 3.36 | 31.71 ± 3.43 | 15.08 # | <0.001 ** | 0.02 *1 0.43 NS 2 <0.001 **3 | |
| Post hoc Bonferroni | <0.001 **a <0.001 **b <0.001 **c | <0.001 **a <0.001 **b <0.001 **c | 0.12 NS a 0.03 *b 0.98 NS c | ||||
| % of reduction | 9.44% | 16% | 5.94% | ||||
| AST: (U/L) | Baseline: | 45.5 (19–88) | 38 (18–180) | 50 (10–161) | 0.59 | 0.75 NS | - |
| 6 months | 45 (18–82) | 36 (20–105) | 48 (21–141) | 17.5 ^ | <0.001 ** | 0.004 *1 0.99 NS 2 <0.001 **3 | |
| 12 months | 43.5 (30–73) | 34.5 (23–70) | 44 (21–115) | 29.3 ^ | <0.001 ** | <0.001 **1 0.97 NS 2 <0.001 **3 | |
| Post hoc Nemenyi test | 0.55 NS a 0.40 NS b 0.15 NS c | 0.01 *a <0.001 **b 0.18 NS c | 0.28 NS a 0.06 NS b 0.50 NS c | ||||
| % of reduction | 4.40% | 17.64% | 12% | ||||
| ALT: (U/L) | Baseline: | 38 (18–137) | 30.5 (18–137) | 44 (20–116) | 5.12 ^ | 0.08 NS | - |
| 6 months | 36.5 (14–123) | 27 (18–68) | 43 (29–114) | 50.8 ^ | <0.001 ** | <0.001 **1 0.01 *2 <0.001 **3 | |
| 12 months | 36 (22–59) | 26 (16–48) | 42 (27–114) | 80.2 ^ | <0.001 ** | <0.001 **1 0.001 *2 <0.001 **3 | |
| Post hoc Nemenyi test | 0.20 NS a 0.052 NS b 0.18 NS c | <0.001 **a <0.001 **b 0.23 NS c | 0.84 NS a 0.65 NS b 0.06 NS c | ||||
| % of reduction | 11.55% | 27.62% | 6.9% | ||||
| Variable | Group I (Rybelsus) (n = 60) | Group II (Ozempic) (n = 60) | Group III (Conventional) (n = 51) | Test | p | Post hoc Tukey | |
|---|---|---|---|---|---|---|---|
| Total cholesterol content: (mg/dL) | Baseline: | 238.06 ± 66.75 | 218.79 ± 38.22 | 229.58 ± 48.56 | 2.01 | 0.14 NS # | - |
| 6 months | 208.3 ± 43.85 | 190.7 ± 18.34 | 214.75 ± 40.66 | 6.81 | 0.001 *# | 0.02 *1 0.61 NS 2 0.002 *3 | |
| 12 months | 203.25 ± 22.68 | 182.08 ± 11.22 | 197.1 ± 28.5 | 15.2 | <0.001 **# | <0.001 **1 0.30 NS 2 0.001 *3 | |
| Post hoc Bonferroni | 0.002 *a <0.001 **b 0.93 NS c | <0.001 **a <0.001 **b <0.001 **c | 0.30 NS a <0.001 **b 0.02 *c | ||||
| % of reduction | 8.02% | 14.03% | 10.73% | ||||
| TGs: (mg/dL) | Baseline: | 178.49 ± 75.53 | 172.96 ± 66.81 | 181.98 ± 71.07 | 0.23 | 0.80 NS # | - |
| 6 months | 147.62 ± 44.44 | 124.42 ± 33.5 | 161.78 ± 57.76 | 9.59 | <0.001 **# | 0.02 *1 0.24 NS 2 <0.001 **3 | |
| 12 months | 125.07 ± 27.46 | 98.75 ± 24.48 | 128.02 ± 44.41 | 14.2 | <0.001 **# | <0.001 **1 0.88 NS 2 <0.001 **3 | |
| Post hoc Bonferroni | 0.002 *a <0.001 **b <0.001 **c | <0.001 **a <0.001 **b <0.001 **c | 0.35 NS a <0.001 **b 0.03 *c | ||||
| % of reduction | 24.59% | 39.25% | 14.86% | ||||
| LDL: (mg/dL) | Base line: | 118.88 ± 41.06 | 134.68 ± 32.63 | 121.5 ± 43.20 | 2.79 | 0.06 NS # | - |
| 6 months | 110.38 ± 27.86 | 106.32 ± 18.98 | 107.22 ± 26.71 | 0.44 | 0.64 NS # | - | |
| 12 months | 102.1 ± 18.52 | 97.67 ± 13.08 | 101.88 ± 21.78 | 1.14 | 0.32 NS # | - | |
| Post hoc Bonferroni | 0.12 NS a 0.007 *b 0.02 *c | <0.001 **a <0.001 **b <0.001 **c | 0.06 NS a 0.006 *b 0.54 NS c | ||||
| % of reduction | 20.83% | 26.67% | 16.54% | ||||
| HDL: (mg/dL) | Base line: | 46.25 ± 5.45 | 45.6 ± 6.37 | 44.39 ± 5.18 | 1.48 | 0.23 NS # | - |
| 6 months | 45.85 ± 3.86 | 51 ± 4.62 | 46.22 ± 4.31 | 26.6 | <0.001 **# | <0.001 **1 0.90 NS 2 <0.001 **3 | |
| 12 months | 48.02 ± 3.62 | 50.08 ± 2.45 | 46.67 ± 4.36 | 13.4 | <0.001 **# | 0.004 *1 0.11 NS 2 <0.001 **3 | |
| Post hoc Bonferroni | 0.99 NS a 0.12 NS b <0.001 **c | <0.001 **a <0.001 **b 0.50 NS c | 0.15 NS a 0.06 NS b 0.99 NS c | ||||
| % of increase | 5.39% | 11.91% | 6.62% | ||||
| Variable | Group I (Rybelsus) (n = 60) | Group II (Ozempic) (n = 60) | Group III (Conventional) (n = 51) | KW | p | Post hoc Dunn’s | |
|---|---|---|---|---|---|---|---|
| NFS: | Baseline: | −1.36 (−3.17 to 0.6) | −1.2 (−4.46 to 0.68) | −1.49 (−3.54 to 0.89) | 1.93 | 0.38 | - |
| 6 months | −1.64 (−3.26 to 0.39) | −1.54 (−4.37 to 0.46) | −1.61 (−3.75 to 0.98) | 1.62 | 0.45 | - | |
| 12 months | −1.69 (−3.49 to 0.42) | −1.46 (−4.96 to 0.09) | −1.71 (−4.06 to 1.08) | 0.93 | 0.63 | - | |
| Post hoc Nemenyi test | <0.001 **a <0.001 **b 0.51 NS c | 0.70 NS a 0.003 *b 0.13 NS c | 0.11 NS a 0.003 *b 0.71 NS c | ||||
| % of reduction | 20.74% | 13.73% | 15.28% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gad, A.I.; Ibrahim, N.F.; Almadani, N.; Mahfouz, R.; Nofal, H.A.; El-Rafey, D.S.; Ali, H.T.; EL-Hawary, A.T.; Sadek, A.M.E.M. Therapeutic Effects of Semaglutide on Nonalcoholic Fatty Liver Disease with Type 2 Diabetes Mellitus and Obesity: An Open-Label Controlled Trial. Diseases 2024, 12, 186. https://doi.org/10.3390/diseases12080186
Gad AI, Ibrahim NF, Almadani N, Mahfouz R, Nofal HA, El-Rafey DS, Ali HT, EL-Hawary AT, Sadek AMEM. Therapeutic Effects of Semaglutide on Nonalcoholic Fatty Liver Disease with Type 2 Diabetes Mellitus and Obesity: An Open-Label Controlled Trial. Diseases. 2024; 12(8):186. https://doi.org/10.3390/diseases12080186
Chicago/Turabian StyleGad, Ahmed I., Nevin F. Ibrahim, Noura Almadani, Rasha Mahfouz, Hanaa A. Nofal, Dina S. El-Rafey, Hossam Tharwat Ali, Amr T. EL-Hawary, and Ayman M. E. M. Sadek. 2024. "Therapeutic Effects of Semaglutide on Nonalcoholic Fatty Liver Disease with Type 2 Diabetes Mellitus and Obesity: An Open-Label Controlled Trial" Diseases 12, no. 8: 186. https://doi.org/10.3390/diseases12080186
APA StyleGad, A. I., Ibrahim, N. F., Almadani, N., Mahfouz, R., Nofal, H. A., El-Rafey, D. S., Ali, H. T., EL-Hawary, A. T., & Sadek, A. M. E. M. (2024). Therapeutic Effects of Semaglutide on Nonalcoholic Fatty Liver Disease with Type 2 Diabetes Mellitus and Obesity: An Open-Label Controlled Trial. Diseases, 12(8), 186. https://doi.org/10.3390/diseases12080186