
Treating Aortic Valve Stenosis for Vitality Improvement: The TAVI Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
- (a)
- Diagnosis of symptomatic or asymptomatic severe AS requiring AVR according to the current guidelines [4], scheduled for TAVI.
- (b)
- Availability of transcranial Doppler (TCD) ultrasound before and after TAVI.
- (c)
- Availability of TASQ score and MMSE before TAVI and in follow-up.
2.2. Transcranial Doppler Ultrasonography
2.3. Quality of Life Assessment
2.4. Neuropsychological Assessment
2.5. Statistical Analysis
3. Results
3.1. Patient Population
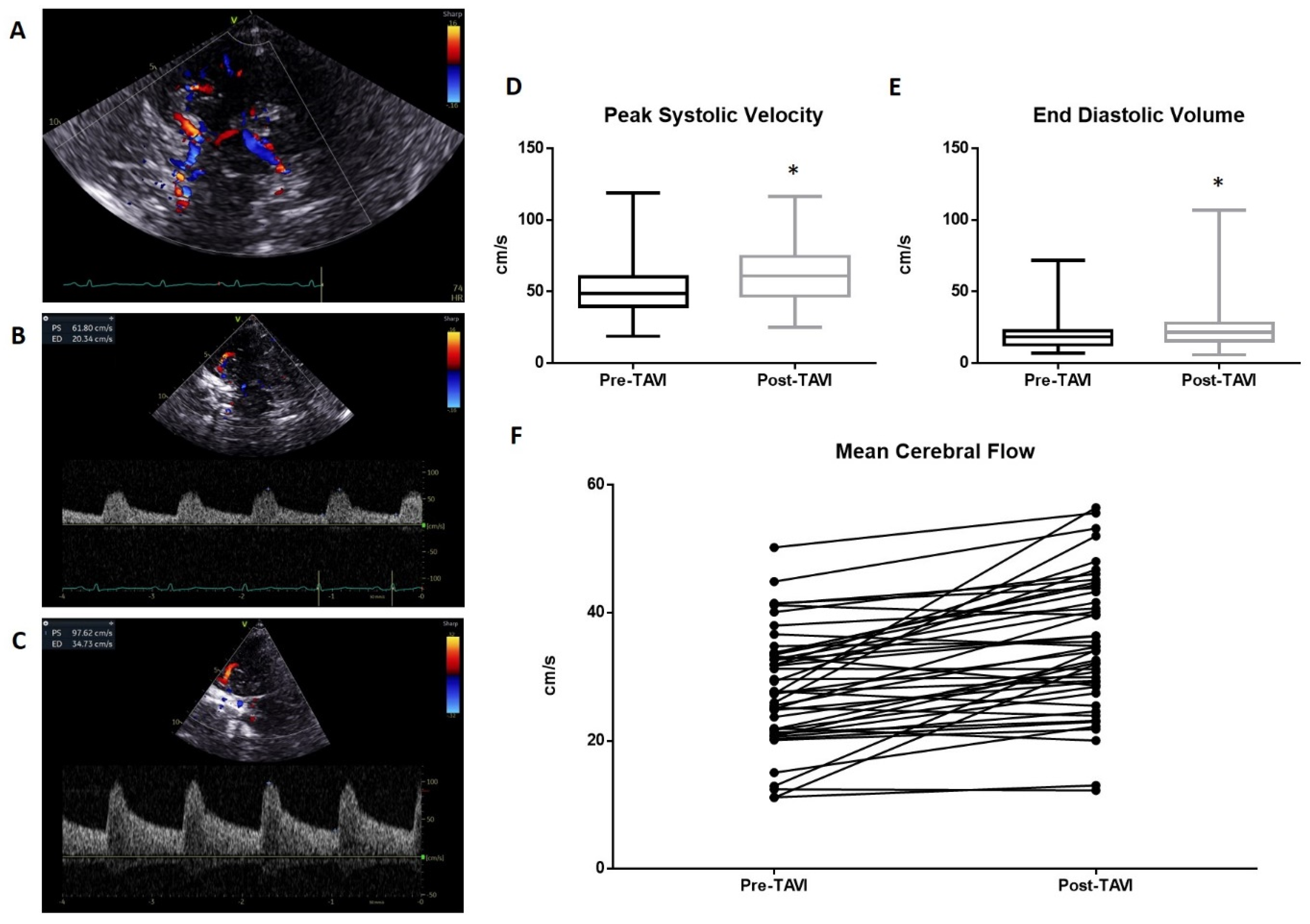
3.2. Transcranial Doppler Ultrasonography
3.3. Quality of Life Assessment
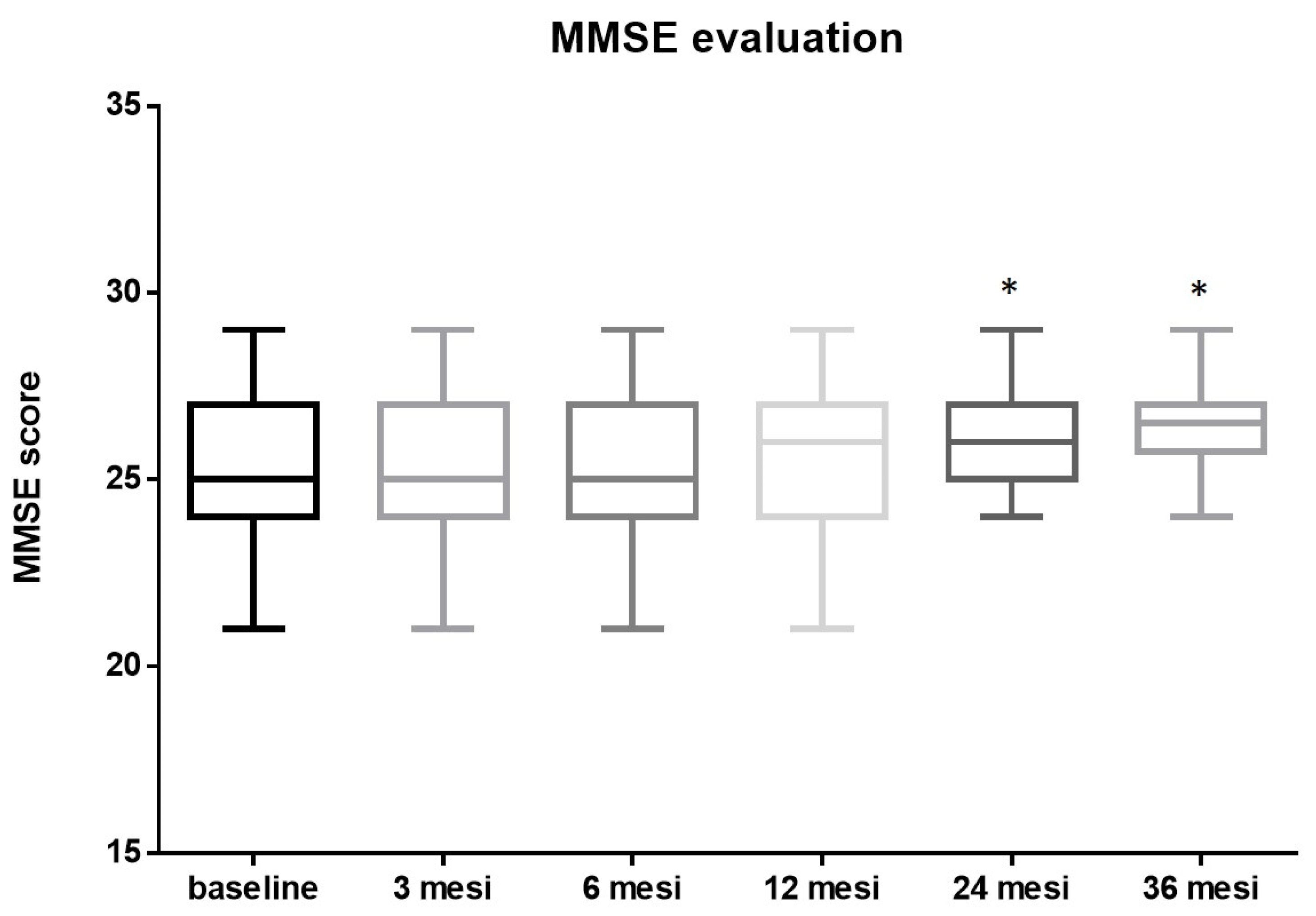
3.4. Neuropsychological Assessment
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Meyer, A.C.; Drefahl, S.; Ahlbom, A.; Lambe, M.; Modig, K. Trends in life expectancy: Did the gap between the healthy and the ill widen or close? BMC Med. 2020, 18, 41. [Google Scholar] [CrossRef] [PubMed]
- d’Arcy, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J.; et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Vahanian, A. Degenerative calcific aortic stenosis: A natural history. Heart 2012, 98, iv7–iv13. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Rajput, F.A.; Zeltser, R. Aortic Valve Replacement; Ineligible Companies. Disclosure: Roman Zeltser Declares No Relevant Financial Relationships with Ineligible Companies; StatPearls: Treasure Island, FL, USA, 2024. [Google Scholar]
- Leon, M.B.; Mack, M.J.; Hahn, R.T.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Alu, M.C.; Madhavan, M.V.; Chau, K.H.; Russo, M.; et al. Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J. Am. Coll. Cardiol. 2021, 77, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Reyes, M.; Reardon, M.J. Transcatheter Valve Replacement: Risk Levels and Contemporary Outcomes. Methodist DeBakey Cardiovasc. J. 2017, 13, 126. [Google Scholar] [CrossRef] [PubMed]
- Haraldstad, K.; Wahl, A.; Andenaes, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2019, 28, 2641–2650. [Google Scholar] [CrossRef] [PubMed]
- Pequeno, N.P.F.; Cabral, N.L.A.; Marchioni, D.M.; Lima, S.; Lyra, C.O. Quality of life assessment instruments for adults: A systematic review of population-based studies. Health Qual. Life Outcomes 2020, 18, 208. [Google Scholar] [CrossRef] [PubMed]
- Styra, R.; Dimas, M.; Svitak, K.; Kapoor, M.; Osten, M.; Ouzounian, M.; Devins, G.; Deckert, A.; Horlick, E. Toronto aortic stenosis quality of life questionnaire (TASQ): Validation in TAVI patients. BMC Cardiovasc. Disord. 2020, 20, 209. [Google Scholar] [CrossRef]
- Arnold, S.V.; Spertus, J.A.; Vemulapalli, S.; Li, Z.; Matsouaka, R.A.; Baron, S.J.; Vora, A.N.; Mack, M.J.; Reynolds, M.R.; Rumsfeld, J.S.; et al. Quality-of-Life Outcomes After Transcatheter Aortic Valve Replacement in an Unselected Population. JAMA Cardiol. 2017, 2, 409. [Google Scholar] [CrossRef]
- Eugene, M.; Duchnowski, P.; Prendergast, B.; Wendler, O.; Laroche, C.; Monin, J.L.; Jobic, Y.; Popescu, B.A.; Bax, J.J.; Vahanian, A.; et al. Contemporary Management of Severe Symptomatic Aortic Stenosis. J. Am. Coll. Cardiol. 2021, 78, 2131–2143. [Google Scholar] [CrossRef] [PubMed]
- Stites, S.D.; Harkins, K.; Rubright, J.D.; Karlawish, J. Relationships Between Cognitive Complaints and Quality of Life in Older Adults With Mild Cognitive Impairment, Mild Alzheimer Disease Dementia, and Normal Cognition. Alzheimer Dis. Assoc. Disord. 2018, 32, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Lazar, R.M.; Pavol, M.A.; Bormann, T.; Dwyer, M.G.; Kraemer, C.; White, R.; Zivadinov, R.; Wertheimer, J.C.; Thöne-Otto, A.; Ravdin, L.D.; et al. Neurocognition and Cerebral Lesion Burden in High-Risk Patients Before Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2018, 11, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Kidher, E.; Harling, L.; Sugden, C.; Ashrafian, H.; Casula, R.; Evans, P.; Nihoyannopoulos, P.; Athanasiou, T. Aortic stiffness is an indicator of cognitive dysfunction before and after aortic valve replacement for aortic stenosis. Interact. CardioVascular Thorac. Surg. 2014, 19, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Luo, C.; Lv, D.; Tian, L.; Qu, C. Risk Factors Affecting Cognitive Impairment of the Elderly Aged 65 and Over: A Cross-Sectional Study. Front. Aging Neurosci. 2022, 14, 903794. [Google Scholar] [CrossRef]
- van Houte, J.; Eerdekens, R.; Dieters, E.; te Pas, M.; Wijnbergen, I.; Tonino, P.; Bouwman, A. Immediate hemodynamic effects of transcatheter aortic valve replacement on left ventricular stroke volume and carotid artery blood flow. WFUMB Ultrasound Open 2023, 1, 100008. [Google Scholar] [CrossRef]
- Vlastra, W.; van Nieuwkerk, A.C.; Bronzwaer, A.S.G.T.; Versteeg, A.; Bron, E.E.; Niessen, W.J.; Mutsaerts, H.J.M.M.; van der Ster, B.J.P.; Majoie, C.B.L.M.; Biessels, G.J.; et al. Cerebral Blood Flow in Patients with Severe Aortic Valve Stenosis Undergoing Transcatheter Aortic Valve Implantation. J. Am. Geriatr. Soc. 2020, 69, 494–499. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Conte, M.; Cavallaro, M.; Scarafile, R.; Riegler, L.; Cocchia, R.; Pezzullo, E.; Carbone, A.; Natale, F.; Santoro, G.; et al. Transcranial Doppler ultrasonography: From methodology to major clinical applications. World J. Cardiol. 2016, 8, 383. [Google Scholar] [CrossRef]
- D’Andrea, A.; Conte, M.; Riegler, L.; Scarafile, R.; Cocchia, R.; Pezzullo, E.; Cavallaro, M.; Di Maio, M.; Natale, F.; Santoro, G.; et al. Transcranial doppler ultrasound: Incremental diagnostic role in cryptogenic stroke part II. J. Cardiovasc. Echogr. 2016, 26, 71. [Google Scholar] [CrossRef]
- D’Andrea, A.; Conte, M.; Scarafile, R.; Riegler, L.; Cocchia, R.; Pezzullo, E.; Cavallaro, M.; Carbone, A.; Natale, F.; Russo, M.; et al. Transcranial Doppler ultrasound: Physical principles and principal applications in Neurocritical care unit. J. Cardiovasc. Echogr. 2016, 26, 28. [Google Scholar] [CrossRef]
- Purkayastha, S.; Sorond, F. Transcranial Doppler Ultrasound: Technique and Application. Semin. Neurol. 2013, 32, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- O’Bryant, S.E.; Humphreys, J.D.; Smith, G.E.; Ivnik, R.J.; Graff-Radford, N.R.; Petersen, R.C.; Lucas, J.A. Detecting Dementia with the Mini-Mental State Examination in Highly Educated Individuals. Arch. Neurol. 2008, 65, 963–967. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 2009, 43, 411–431. [Google Scholar] [CrossRef] [PubMed]
- Lansky, A.J.; Messé, S.R.; Brickman, A.M.; Dwyer, M.; van der Worp, H.B.; Lazar, R.M.; Pietras, C.G.; Abrams, K.J.; McFadden, E.; Petersen, N.H.; et al. Proposed Standardized Neurological Endpoints for Cardiovascular Clinical Trials. J. Am. Coll. Cardiol. 2017, 69, 679–691. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, A.L.; Liu, D.; Gupta, D.K.; Pechman, K.R.; Watchmaker, J.M.; Gordon, E.A.; Rane, S.; Bell, S.P.; Mendes, L.A.; Davis, L.T.; et al. Lower cardiac index levels relate to lower cerebral blood flow in older adults. Neurology 2017, 89, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- van Nieuwkerk, A.C.; Hemelrijk, K.I.; Bron, E.E.; Leeuwis, A.E.; Majoie, C.B.L.M.; Daemen, M.J.A.P.; Moonen, J.E.F.; de Sitter, A.; Bouma, B.J.; van der Flier, W.M.; et al. Cardiac output, cerebral blood flow and cognition in patients with severe aortic valve stenosis undergoing transcatheter aortic valve implantation: Design and rationale of the CAPITA study. Neth. Heart J. 2023, 31, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Rosas, H.D.; Salat, D.H. Age-associated reductions in cerebral blood flow are independent from regional atrophy. NeuroImage 2011, 55, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Shaw, T.G.; Mortel, K.F.; Meyer, J.S.; Rogers, R.L.; Hardenberg, J.; Cutaia, M.M. Cerebral blood flow changes in benign aging and cerebrovascular disease. Neurology 1984, 34, 855. [Google Scholar] [CrossRef]
- Bronzwaer, A.G.T.; Verbree, J.; Stok, W.J.; Daemen, M.; van Buchem, M.A.; van Osch, M.J.P.; van Lieshout, J.J. Aging modifies the effect of cardiac output on middle cerebral artery blood flow velocity. Physiol. Rep. 2017, 5, e13361. [Google Scholar] [CrossRef]
- Bown, C.W.; Do, R.; Khan, O.A.; Liu, D.; Cambronero, F.E.; Moore, E.E.; Osborn, K.E.; Gupta, D.K.; Pechman, K.R.; Mendes, L.A.; et al. Lower Cardiac Output Relates to Longitudinal Cognitive Decline in Aging Adults. Front. Psychol. 2020, 11, 569355. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.E.; Jefferson, A.L. Impact of Cardiovascular Hemodynamics on Cognitive Aging. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Ovsenik, A.; Podbregar, M.; Fabjan, A. Cerebral blood flow impairment and cognitive decline in heart failure. Brain Behav. 2021, 11, e02176. [Google Scholar] [CrossRef] [PubMed]
- van Nieuwkerk, A.C.; Delewi, R.; Wolters, F.J.; Muller, M.; Daemen, M.; Biessels, G.J. Cognitive Impairment in Patients with Cardiac Disease: Implications for Clinical Practice. Stroke 2023, 54, 2181–2191. [Google Scholar] [CrossRef] [PubMed]
- Solla Suárez, P.; Díaz, R.; Herrera, J.; del Valle, R.; Moreno, C.; Almendarez, M.; López, E.; Álvarez, R.; Morís de la Tassa, C.; Gutiérrez, J. Deterioro cognitivo en el paciente mayor con estenosis aórtica grave sintomática. Toma de decisiones terapéuticas e impacto sobre la mortalidad al año. Rev. Neurol. 2023, 76, 127. [Google Scholar] [CrossRef] [PubMed]
- Natale, F.; Golino, P.; Cimmino, G. Angiotensin-converting enzyme inhibitors, statins and the polypill in cardiovascular diseases prevention: Ignorance is bliss or not? J. Hypertens. 2024, 42, 746–748. [Google Scholar] [CrossRef] [PubMed]
- Gruhn, N.; Larsen, F.S.; Boesgaard, S.; Knudsen, G.M.; Mortensen, S.A.; Thomsen, G.; Aldershvile, J. Cerebral Blood Flow in Patients With Chronic Heart Failure Before and After Heart Transplantation. Stroke 2001, 32, 2530–2533. [Google Scholar] [CrossRef] [PubMed]
- Massaro, A.R.; Dutra, A.P.; Almeida, D.R.; Diniz, R.V.Z.; Malheiros, S.M.F. Transcranial Doppler assessment of cerebral blood flow: Effect of cardiac transplantation. Neurology 2006, 66, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Suarez, I.M.; Scheer, A.; Chasland, L.C.; Thomas, H.J.; Correia, M.A.; Dembo, L.G.; Naylor, L.H.; Maiorana, A.J.; Green, D.J. Cerebral Blood Flow during Exercise in Heart Failure: Effect of Ventricular Assist Devices. Med. Sci. Sports Exerc. 2019, 51, 1372–1379. [Google Scholar] [CrossRef]
- Leone, A.; Gracia Baena, J.M.; Marsal Mora, J.R.; Llorca Cardeñosa, S.; Calaf Vall, I.; Zielonka, M.; Godoy, P. Impact of severe aortic stenosis on quality of life. PLoS ONE 2023, 18, e0287508. [Google Scholar] [CrossRef]
- Leeuwis, A.E.; Smith, L.A.; Melbourne, A.; Hughes, A.D.; Richards, M.; Prins, N.D.; Sokolska, M.; Atkinson, D.; Tillin, T.; Jäger, H.R.; et al. Cerebral Blood Flow and Cognitive Functioning in a Community-Based, Multi-Ethnic Cohort: The SABRE Study. Front. Aging Neurosci. 2018, 10, 279. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, A.; Kocurek, J.; Sinning, J.-M.; Wagner, M.; Becker, B.V.; Vogel, M.; Schröder, T.; Wolfsgruber, S.; Vasa-Nicotera, M.; Hammerstingl, C.; et al. Cognitive Trajectory After Transcatheter Aortic Valve Implantation. Circ. Cardiovasc. Interv. 2013, 6, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Schoenenberger, A.W.; Zuber, C.; Moser, A.; Zwahlen, M.; Wenaweser, P.; Windecker, S.; Carrel, T.; Stuck, A.E.; Stortecky, S. Evolution of Cognitive Function After Transcatheter Aortic Valve Implantation. Circ. Cardiovasc. Interv. 2016, 9, e003590. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Campelo-Parada, F.; Regueiro, A.; Del Trigo, M.; Chiche, O.; Chamandi, C.; Allende, R.; Cordoba-Soriano, J.G.; Paradis, J.-M.; De Larochellière, R.; et al. Serial Changes in Cognitive Function Following Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 68, 2129–2141. [Google Scholar] [CrossRef] [PubMed]
- Pagnesi, M.; Martino, E.A.; Chiarito, M.; Mangieri, A.; Jabbour, R.J.; Van Mieghem, N.M.; Kodali, S.K.; Godino, C.; Landoni, G.; Colombo, A.; et al. Silent cerebral injury after transcatheter aortic valve implantation and the preventive role of embolic protection devices: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 221, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, G.; Renon, F.; Bianchi, R.; Tartaglione, D.; Cappelli Bigazzi, M.; Loffredo, F.; Golino, P.; Cimmino, G. Asymptomatic Stroke in the Setting of Percutaneous Non-Coronary Intervention Procedures. Medicina 2021, 58, 45. [Google Scholar] [CrossRef] [PubMed]
- Liimatainen, J.; Peräkylä, J.; Järvelä, K.; Sisto, T.; Yli-Hankala, A.; Hartikainen, K.M. Improved cognitive flexibility after aortic valve replacement surgery. Interact. CardioVascular Thorac. Surg. 2016, 23, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Lazar, R.M.; Myers, T.; Gropen, T.I.; Leesar, M.A.; Davies, J.; Gerstenecker, A.; Norling, A.; Pavol, M.A.; Marshall, R.S.; Kodali, S. Cerebral blood flow and neurocognition in patients undergoing transcatheter aortic valve replacement for severe aortic stenosis. Eur. Heart J. Open 2024, 4, oead124. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Park, S.; Kim, S. Effects of Participation in Social Activities on Cognitive Function Among Middle-Aged and Older Adults in Korea. Int. J. Environ. Res. Public Health 2018, 15, 2315. [Google Scholar] [CrossRef]
- Christelis, D.; Dobrescu, L.I. The causal effect of social activities on cognition: Evidence from 20 European countries. Soc. Sci. Med. 2020, 247, 112783. [Google Scholar] [CrossRef]
- Lim, G.B. Suitability of TAVI in low-risk patients. Nat. Rev. Cardiol. 2023, 20, 284. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.B. Another Early Win for TAVI in Low-Risk Patients. N. Engl. J. Med. 2024, 390, 1623–1625. [Google Scholar] [CrossRef]
- Forrest, J.K.; Deeb, G.M.; Yakubov, S.J.; Gada, H.; Mumtaz, M.A.; Ramlawi, B.; Bajwa, T.; Teirstein, P.S.; DeFrain, M.; Muppala, M.; et al. 3-Year Outcomes After Transcatheter or Surgical Aortic Valve Replacement in Low-Risk Patients With Aortic Stenosis. J. Am. Coll. Cardiol. 2023, 81, 1663–1674. [Google Scholar] [CrossRef]
- Otto, C.M. Alignment and divergence in European and North American aortic stenosis guidelines. EuroInterv. J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2022, 17, e1123–e1125. [Google Scholar] [CrossRef] [PubMed]
- Natale, F.; Aronne, L.; Credendino, M.; Siciliano, A.; Allocca, F.; Weizs, S.H.; Martone, F.; Marco, G.M.d.; Calabrò, P.; Tedesco, M.A.; et al. Which is the correct management of patients with asymptomatic severe calcific aortic stenosis after symptomatic spontaneous calcium cerebral embolism? J. Cardiovasc. Med. 2011, 12, 428–429. [Google Scholar] [CrossRef] [PubMed]
- Natale, F.; Baldini, L.; Di Marco, G.M.; Aronne, L.; Calabro, P.; Russo, M.G.; Calabro, R. Management of patients with asymptomatic severe aortic stenosis and severe anemia. Am. J. Cardiol. 2010, 105, 423. [Google Scholar] [CrossRef] [PubMed]
- Yashige, M.; Inoue, K.; Zen, K.; Kobayashi, R.; Nakamura, S.; Fujimoto, T.; Takamatsu, K.; Sugino, S.; Yamano, M.; Yamano, T.; et al. Gastrointestinal Angiodysplasia before and after Treatment of Severe Aortic Stenosis. N. Engl. J. Med. 2023, 389, 1530–1532. [Google Scholar] [CrossRef] [PubMed]
- Sugino, S.; Inoue, K.; Zen, K.; Yashige, M.; Kobayashi, R.; Takamatsu, K.; Ito, N.; Iwai, N.; Hirose, R.; Doi, T.; et al. Gastrointestinal Angiodysplasia in Patients with Severe Aortic Stenosis: The Endoscopic Features of Heyde’s Syndrome. Digestion 2023, 104, 468–479. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study Population (n = 47) | |
|---|---|
| Demographics | |
| Age, y | 79.3 ± 4.4 |
| Female sex | 26 (54%) |
| Medical history | |
| Previous myocardial infarction | 7 |
| Previous PCI | 1 |
| Previous CABG | 2 |
| Diabete Mellitus | 24 |
| Hypertension | 43 |
| Hystory of coronary artery disease | 28 |
| Atrial fibrillation | 12 |
| GFR < 30 mL/min per 1.73 m2 | 8 |
| NYHA class | I: 3; II: 25; III: 19 |
| Angina pectoris | 11 |
| Syncope | 3 |
| Medication | |
| Beta-blockers | 24 |
| ACE-inhibitors/ARBs | 29 |
| ARNI | 15 |
| Diuretics | 22 |
| Calcium channel blockers | 8 |
| MRA | 11 |
| Risk scores | |
| EuroSCORE II, % | 7.8 ± 2.8% |
| Echocardiographic characteristics pre TAVI | |
| Aortic maximum gradient, mmHg | 69 ± 24 |
| Aortic mean gradient, mmHg | 46 ± 8 |
| Aortic valve area, cm2 | 0.6 ± 0.2 |
| SVi, mL/m2 | 36.4 ± 4.2 |
| LVEF, % | 41 ± 8 |
| Tricuspid regurgitation | No/trace: 9; mild: 11; moderate/severe: 10 |
| Mitral regurgitation | No/trace: 11; mild: 23; moderate/severe: 6 |
| Aortic regurgitation | No/trace: 12; mild: 15; moderate/severe: 1 |
| Procedural details/valve type | |
| Transfemoral access | 45 |
| Trans-subclavian access | 2 |
| Echocardiographic characteristics post TAVI | |
| Aortic maximum gradient, mmHg | 15.6 ± 10.3 |
| Aortic mean gradient, mmHg | 9.8 ± 4.2 |
| SVi, mL/m2 | 39.7 ± 6.8 |
| LVEF, % | 44 ± 7 |
| Baseline | 3 Months | 6 Months | 12 Months | 24 Months | 36 Months | |
|---|---|---|---|---|---|---|
| TASQ physical symptoms | 7.8 ± 2.1 | 7 ± 1.7 | 6.9 ± 1.8 | 6.1 ± 1.7 | 6.2 ± 2.1 | 5.8 ± 2.8 |
| TASQ physical limitations | 16.4 ± 5 | 17.3 ± 3.8 | 14.7 ± 2.9 | 14.2 ± 4.3 | 13.9 ± 5.1 | 13.4 ± 4.2 |
| TASQ emotional impact | 29.7 ± 13.3 | 30.1 ± 9.2 | 29.1 ± 8.9 | 27.2 ± 8.3 | 21.2 ± 8.6 | 20.2 ± 7.8 |
| TASQ social limitations | 7.9 ± 2.5 | 8.3 ± 3.1 | 7.8 ± 3 | 6.8 ± 2.7 | 5.9 ± 2.9 | 4.9 ± 1.7 |
| TASQ health expectations | 4.4 ± 1.8 | 4 ± 1.5 | 4 ± 1.6 | 3.9 ± 1.9 | 2.9 ± 2.1 | 2.8 ± 1.7 |
| TASQ overall summary | 63.4 ± 25.9 | 65.6 ± 16.7 | 62.6 ± 17.6 | 59.9 ± 15.9 | 54.7 ± 12.6 | 51.6 ± 11.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tartaglione, D.; Prozzo, D.; Bianchi, R.; Ciccarelli, G.; Cappelli Bigazzi, M.; Natale, F.; Golino, P.; Cimmino, G. Treating Aortic Valve Stenosis for Vitality Improvement: The TAVI Study. Diseases 2024, 12, 175. https://doi.org/10.3390/diseases12080175
Tartaglione D, Prozzo D, Bianchi R, Ciccarelli G, Cappelli Bigazzi M, Natale F, Golino P, Cimmino G. Treating Aortic Valve Stenosis for Vitality Improvement: The TAVI Study. Diseases. 2024; 12(8):175. https://doi.org/10.3390/diseases12080175
Chicago/Turabian StyleTartaglione, Donato, Dario Prozzo, Renatomaria Bianchi, Giovanni Ciccarelli, Maurizio Cappelli Bigazzi, Francesco Natale, Paolo Golino, and Giovanni Cimmino. 2024. "Treating Aortic Valve Stenosis for Vitality Improvement: The TAVI Study" Diseases 12, no. 8: 175. https://doi.org/10.3390/diseases12080175
APA StyleTartaglione, D., Prozzo, D., Bianchi, R., Ciccarelli, G., Cappelli Bigazzi, M., Natale, F., Golino, P., & Cimmino, G. (2024). Treating Aortic Valve Stenosis for Vitality Improvement: The TAVI Study. Diseases, 12(8), 175. https://doi.org/10.3390/diseases12080175