
Evaluation of the Effectiveness of Combined Treatment with Intravaginal Diazepam and Pelvic Floor Rehabilitation in Patients with Vulvodynia by Ultrasound Monitoring of Biometric Parameters of Pelvic Muscles: A Pilot Study

 , , , ,
, , , , 
Abstract
1. Introduction
2. Materials and Methods
- -
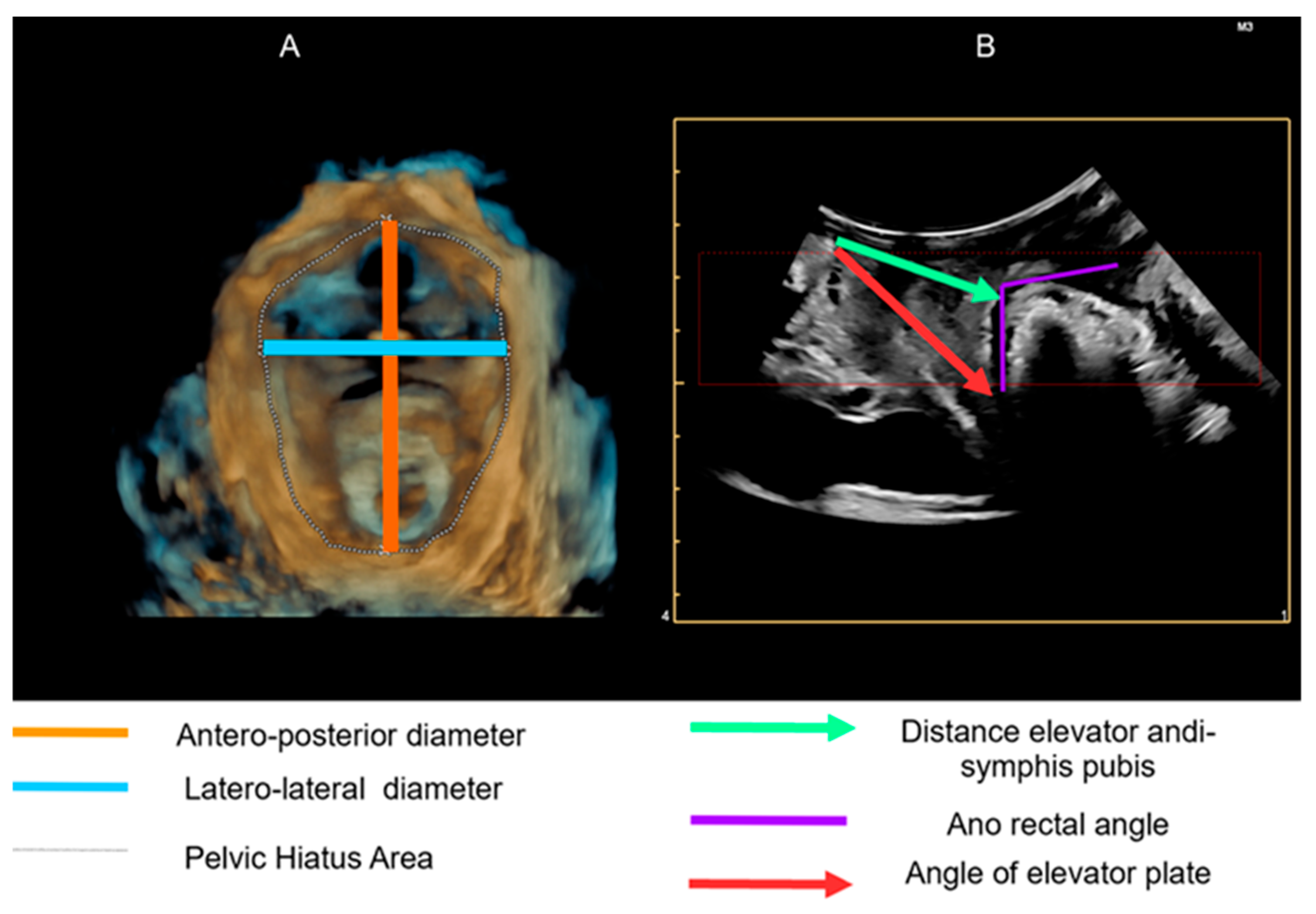
- Ultrasound biometric parameters: symphysis: anus elevator distance, anorectal angle, and diameter of the hiatal area, all assessed trans-labial;
- -
- Clinical parameters: dyspareunia assessed by the Marinoff scale; vulvar pain assessed by the visual analogic scale (VAS);
- -
- The diagnostic approach used is based on that proposed by Bergeron [5].
- -
- Resting symphysis-elevator distance: distance from the lower posterior limit of the anorectal junction;
- -
- Anorectal angle at rest: the angle is measured at the confluence of the drooping lines on the longitudinal axis of the anal canal and the posteroinferior margin of the rectal wall;
- -
- Elevator plate angle: the angle is obtained by the intersection of the horizontal reference line embedded at the level of the pubic symphysis at the crux of the anorectal angle;
- -
- Excipients: hydrophilic excipients, as they are better suited to the vaginal environment. The chosen mixture is based on PEG (polyethylene glycol) 400 and PEG 4000, 7% and 40%, respectively;
- -
- Molds: vaginal ovules containing 12 mg; Active ingredient: diazepam. The composition of a single ovule contains 0.005 g diazepam, 1.5015 g PEG 400, and 1.01 g PEG 4000.
- -
- Pelvic floor evaluation to assess the presence of hypertonus;
- -
- Assessment of the basin;
- -
- Evaluation of the column;
- -
- Functionality and muscle symmetry;
- -
- Capacity for synchronous contraction.
- -
- Pelvic floor activation exercises;
- -
- Respiratory coordination exercises;
- -
- Leg coordination exercises;
- -
- Pelvic floor coordination exercises;
- -
- External massage of the pelvic musculature;
- -
- Pelvic floor muscle stretching;
- -
- Biofeedback;
- -
- Transcutaneous electrical nerve stimulation (TENS) with a vaginal probe and external electrodes;
- -
- Training for muscle-relaxing self-postures and use of a hot water bottle for continuing physiotherapy at home.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bornstein, J.; Goldstein, A.T.; Stockdale, C.K.; Bergeron, S.; Pukall, C.; Zolnoun, D.; Coady, D. International Society for the Study of Vulvovaginal Disease (ISSVD); the International Society for the Study of Women’s Sexual Health (ISSWSH); the International Pelvic Pain Society (IPPS). 2015 ISSVD, ISSWSH and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia. Obstet. Gynecol. 2016, 127, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Rubal, C.; Pereira, A.; Sastre, L.C.; Pérez-Cejuela, B.A.; Gámiz, S.H.; Chaves, P.; Medina, T.P. Managing Vulvodynia with Central Sensitization: Challenges and Strategies. J. Clin. Med. 2023, 12, 3851. [Google Scholar] [CrossRef] [PubMed]
- Gómez, I.; Coronado, P.J.; Martín, C.M.; Alonso, R.; Guisasola Campa, F.J. Study on the Prevalence and Factors Associated to Vulvodynia in Spain. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 240, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Schlaeger, J.M.; Patil, C.L.; Steffen, A.D.; Pauls, H.A.; Roach, K.L.; Thornton, P.D.; Hartmann, D.; Kobak, W.H.; Yao, Y.; Suarez, M.L.; et al. Sensory pain characteristics of vulvodynia and their association with nociceptive and neuropathic pain: An online survey pilot study. Pain. Rep. 2019, 4, e713. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, S.; Reed, B.D.; Wesselmann, U.; Bohm-Starke, N. Vulvodynia. Nat. Rev. Dis. Primers 2020, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Morin, M.; Bergeron, S.; Khalifé, S.; Mayrand, M.H.; Binik, Y.M. Morphometry of pelvic floor muscles in women with and without provoked vestibulodyna using 4D ultrasound. J. Sex. Med. 2014, 11, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Thibault-Gagnon, S.; McLean, L.; Goldfinger, C.; Pukall, C.; Chamberlain, S. Differences in the biometry of the levator hiatus at rest, during contraction and during valsalva maneuver between women with and without provoked vestibulodynia assessed by transperineal ultrasound imaging. J. Sex. Med. 2016, 13, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Gentilcore-Saulnier, E.; McLean, L.; Goldfinger, C.; Pukall, C.F.; Chamberlain, S. Pelvic floor muscle assessment outcomes in women with and without provoked vestibulodynia and the impact of a physical therapy program. J. Sex. Med. 2010, 6, 1003–1022. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.T.; Pukall, C.F.; Brown, C.; Bergeron, S.; Stein, A.; Kellogg-Spadt, S. Vulvodynia: Assessment and treatment. J. Sex. Med. 2016, 13, 572–590. [Google Scholar] [CrossRef] [PubMed]
- Ben-Aroya, Z.; Edwards, L. Vulvodynia. Semin. Cutan. Med. Surg. 2015, 34, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Bardin, M.G.; Giraldo, P.C.; Martinho, N. Pelvic Floor Biometric Changes Assessed by 4D Translabial Ultrassound in Women With Vulvodynia Submitted to Physical Therapy: A Pilot Study of a Randomized Controlled Trial. J. Sex. Med. 2020, 17, 2236–2246. [Google Scholar] [CrossRef] [PubMed]
- Murina, F.; Felice, R.; Di Francesco, S.; Oneda, S. Vaginal diazepam plus transcutaneous electrical nerve stimulation to treat vestibulodynia: A randomized controlled trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Carrico, D.J.; Peters, K.M. Vaginal diazepam use with urogenital pain/pelvic floor dysfunction: Serum diazepam levels and efficacy data. Urol. Nurs. 2011, 31, 279. [Google Scholar] [CrossRef] [PubMed]
- Rogalski, M.J.; Kellogg-Spadt, S.; Hoffmann, A.R.; Fariello, J.Y.; Whitmore, K.E. Retrospective chart review of vaginal diazepam suppository use in high tone pelvic floor dysfunction. Int. Urogynecol. J. 2010, 21, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Crisp, C.C.; Vaccaro, C.M.; Estano, M.V.l.; Oakley, S.H.; Kleeman, S.D.; Fellner, A.N.; Pauls, R.N. Intra-vaginal diazepam for high-tone pelvic floor dysfunction: A randomized placebo-controlled trial. Int. Urogynecol J. 2013, 24, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Goldfinger, C.; Pukall, C.F.; Gentilcore-Saulnier, E.; McLean, L.; Chamberlain, S. A prospective study of pelvic floor physical therapy: Pain and psychosexual outcomes in provoked vestibulodynia. J. Sex. Med. 2009, 6, 1955–1968. [Google Scholar] [CrossRef] [PubMed]
- Calafiore, D.; Marotta, N.; Curci, C.; Agostini, F.; De Socio, R.I.; Inzitari, M.T.; Ferraro, F.; Bernetti, A.; Ammendolia, A.; de Sire, A. Efficacy of Rehabilitative Techniques on Pain Relief in Patients With Vulvodynia: A Systematic Review and Meta-Analysis. Phys. Ther. 2024, 104, pzae054. [Google Scholar] [CrossRef] [PubMed]
- Angelos, P. Interventions to Improve Informed Consent: Perhaps Surgeons Should Speak Less and Listen More. JAMA Surg. 2020, 155, 13–14. [Google Scholar] [CrossRef] [PubMed]
- Penteado, S.R.L.; Bonduki, C.E.; de Araújo, T.R.E.; Alves, S.V.; de Luccas Batista, N.M.T.; Ambrogini, C.C.; Sartori, M.G.F. Individualized multidisciplinary therapy for vulvodynia. J. Obstet. Gynaecol. Res. 2024, 50, 147–174. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Time | Case Arm Mean (Standard Deviation) | Control Arm Mean (Standard Deviation) | |
|---|---|---|---|
| Symphysis-elevator distance | Before treatment | 3.9 (0.3) | 3.9 (0.4) |
| 6 months | 4 (0.3) | 3.5 (0.4) | |
| p-value for variation | 0.23 | 0.01 | |
| Anorectal angle | Before treatment | 122.6 (2.9) | 122.4 (2.4) |
| 6 months | 123.7 (3.1) | 121.4 (2.3) | |
| p-value for variation | 0.28 | 0.01 | |
| Elevator plate angle | Before treatment | 9 (2.3) | 8.7 (2.5) |
| 6 months | 9.4 (2.3) | 8.2 (2.4) | |
| p-value for variation | <0.01 | 0.01 | |
| Hiatal area diameter | Before treatment | 1.3 (0.4) | 1.3 (0.4) |
| 6 months | 1.4 (0.5) | 1.1 (0.4) | |
| p-value for variation | <0.01 | 0.01 | |
| Marinoff scale | Before treatment | 2.3 (0.5) | 2.4 (0.5) |
| 6 months | 1.4 (0.7) | 3.4 (1.2) | |
| p-value for variation | 0.01 | 0.03 | |
| VAS scale | Before treatment | 5.8 (1) | 5.5 (1.3) |
| 6 months | 2.8 (0.9) | 6.4 (1) | |
| p-value for variation | 0.01 | 0.06 |
| Case Arm Mean (Standard Deviation) | Control Arm Mean (Standard Deviation) | p-Value | |
|---|---|---|---|
| Symphysis-elevator distance | 0.1 (0.2) | −0.3 (0.1) | <0.01 |
| Anorectal angle | 1 (2.6) | −1 (0.7) | 0.1 |
| Elevator plate angle | 0.4 (0.3) | −0.5 (0.3) | <0.01 |
| Hiatal area diameter | 0.1 (0.1) | −0.2 (0.2) | <0.01 |
| Marinoff scale | −0.9 (0.9) | 1 (1.2) | <0.01 |
| VAS scale | −3 (0.8) | 0.9 (1.1) | <0.01 |
| Unadjusted Model | |||
|---|---|---|---|
| Estimate | SE | p-value | |
| Treatment | −3.9 | 0.4 | <0.01 |
| Adjusted model | |||
| Estimate | SE | p-value | |
| Treatment | −3.8 | 0.3 | <0.01 |
| Symphysis-elevator distance | −2.6 | 0.7 | <0.01 |
| Anorectal angle | −0.1 | 0.1 | 0.54 |
| Elevator plate angle | −0.2 | 0.1 | 0.02 |
| Hiatal area diameter | 3.4 | 0.6 | <0.01 |
| Unadjusted Model | |||
|---|---|---|---|
| Estimate | SE | p-value | |
| Treatment | −1.9 | 0.5 | <0.01 |
| Adjusted model | |||
| Estimate | SE | p-value | |
| Treatment | −1.9 | 0.5 | <0.01 |
| Symphysis-elevator distance | 1.1 | 1.5 | 0.46 |
| Anorectal angle | 0 | 0.2 | 0.92 |
| Elevator plate angle | −0.1 | 0.2 | 0.55 |
| Hiatal area diameter | 0.5 | 1.1 | 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merlino, L.; Ciminello, E.; Volpicelli, A.I.; Tillier, S.; Pasquali, M.F.; Dominoni, M.; Gardella, B.; Senatori, R.; Dionisi, B.; Piccioni, M.G. Evaluation of the Effectiveness of Combined Treatment with Intravaginal Diazepam and Pelvic Floor Rehabilitation in Patients with Vulvodynia by Ultrasound Monitoring of Biometric Parameters of Pelvic Muscles: A Pilot Study. Diseases 2024, 12, 174. https://doi.org/10.3390/diseases12080174
Merlino L, Ciminello E, Volpicelli AI, Tillier S, Pasquali MF, Dominoni M, Gardella B, Senatori R, Dionisi B, Piccioni MG. Evaluation of the Effectiveness of Combined Treatment with Intravaginal Diazepam and Pelvic Floor Rehabilitation in Patients with Vulvodynia by Ultrasound Monitoring of Biometric Parameters of Pelvic Muscles: A Pilot Study. Diseases. 2024; 12(8):174. https://doi.org/10.3390/diseases12080174
Chicago/Turabian StyleMerlino, Lucia, Enrico Ciminello, Agnese Immacolata Volpicelli, Stefano Tillier, Marianna Francesca Pasquali, Mattia Dominoni, Barbara Gardella, Roberto Senatori, Barbara Dionisi, and Maria Grazia Piccioni. 2024. "Evaluation of the Effectiveness of Combined Treatment with Intravaginal Diazepam and Pelvic Floor Rehabilitation in Patients with Vulvodynia by Ultrasound Monitoring of Biometric Parameters of Pelvic Muscles: A Pilot Study" Diseases 12, no. 8: 174. https://doi.org/10.3390/diseases12080174
APA StyleMerlino, L., Ciminello, E., Volpicelli, A. I., Tillier, S., Pasquali, M. F., Dominoni, M., Gardella, B., Senatori, R., Dionisi, B., & Piccioni, M. G. (2024). Evaluation of the Effectiveness of Combined Treatment with Intravaginal Diazepam and Pelvic Floor Rehabilitation in Patients with Vulvodynia by Ultrasound Monitoring of Biometric Parameters of Pelvic Muscles: A Pilot Study. Diseases, 12(8), 174. https://doi.org/10.3390/diseases12080174