
Prognostic Role of Lymphocyte-to-Monocyte Ratio (LMR) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations (DEM-TACE or cTACE) of the Liver: Exploring the Link between Tumor Microenvironment and Interventional Radiology


 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Treatment
2.3. Outcomes and Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
- -
- Based on the ROC curve analysis, a cut-off value of 2.24 was chosen to divide the population into a low LMR group and a high LMR group. An area under the curve of 0.851 highlights good accuracy in predicting 6-month PFS;
- -
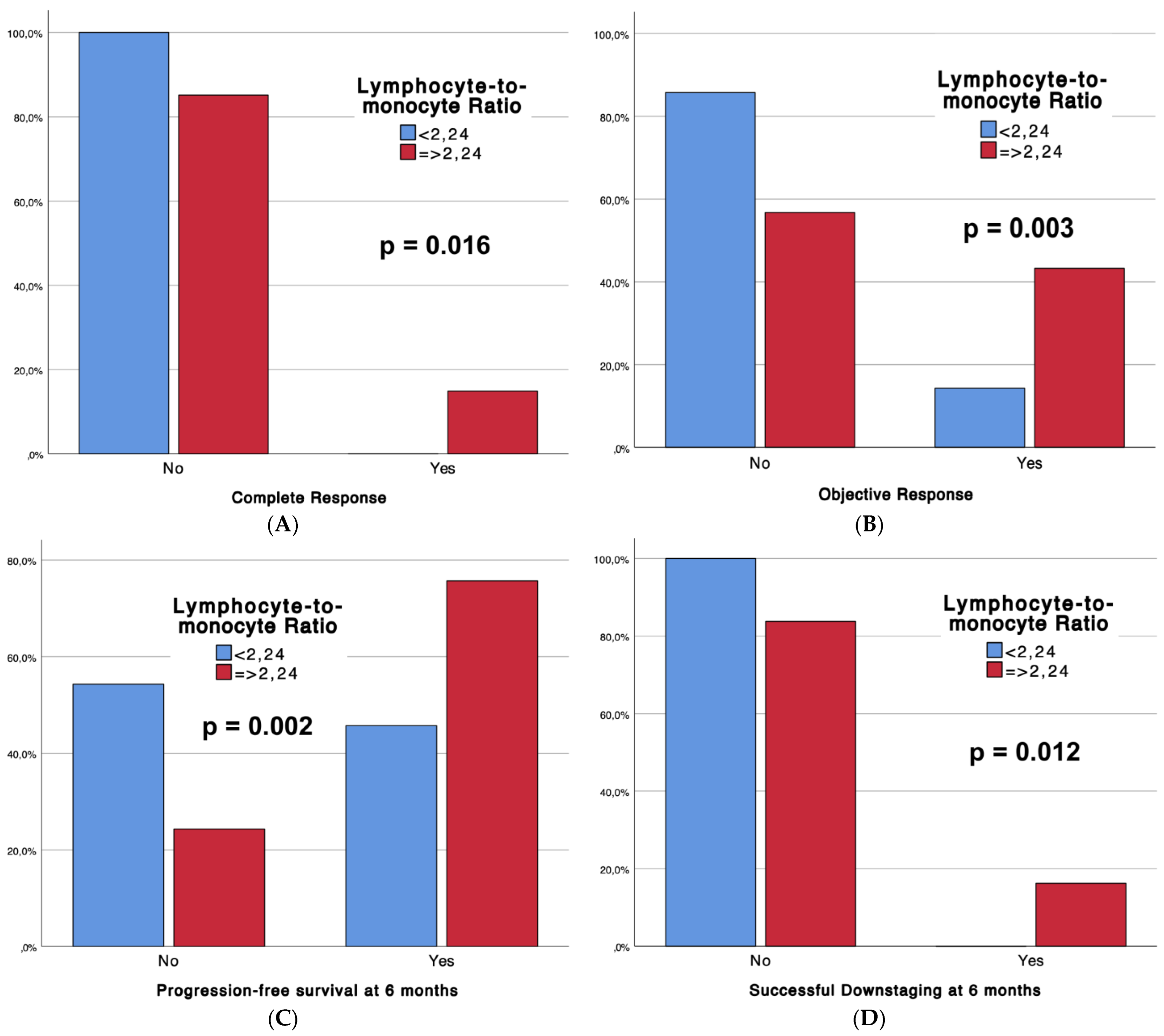
- Strong correlations between the LMR and treatment response, progression-free survival, and successful downstaging at 6 months are noted;
- -
- Hepatitis C virus infection, alpha-fetoprotein levels, lymphocyte count, and the LMR emerged as significant predictors affecting objective response occurrence and progression-free survival at 6 months. The LMR, categorized as <2.24 and ≥2.24, proved to be a robust predictor in both analyses (p = 0.001 and p < 0.001, respectively). These results underscore the prognostic role of the LMR in predicting treatment response and short-term outcomes in patients with stage B HCC undergoing TACE.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.E.; de Lope, C.R.; Bruix, J. Current strategy for staging and treatment: The BCLC update and future prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef]
- Kudo, M.; Arizumi, T.; Ueshima, K.; Sakurai, T.; Kitano, M.; Nishida, N. Subclassification of BCLC B Stage Hepatocellular Carcinoma and Treatment Strategies: Proposal of Modified Bolondi’s Subclassification (Kinki Criteria). Dig. Dis. 2015, 33, 751–758. [Google Scholar] [CrossRef]
- Minici, R.; Ammendola, M.; Manti, F.; Siciliano, M.A.; Minici, M.; Komaei, I.; Currò, G.; Laganà, D. Safety and Efficacy of Degradable Starch Microspheres Transcatheter Arterial Chemoembolization (DSM-TACE) in the Downstaging of Intermediate-Stage Hepatocellular Carcinoma (HCC) in Patients With a Child-Pugh Score of 8–9. Front. Pharmacol. 2021, 12, 634087. [Google Scholar] [CrossRef]
- Yao, F.Y.; Mehta, N.; Flemming, J.; Dodge, J.; Hameed, B.; Fix, O.; Hirose, R.; Fidelman, N.; Kerlan, R.K., Jr.; Roberts, J.P. Downstaging of hepatocellular cancer before liver transplant: Long-term outcome compared to tumors within Milan criteria. Hepatology 2015, 61, 1968–1977. [Google Scholar] [CrossRef]
- Su, T.-H.; Hsu, S.-J.; Kao, J.-H. Paradigm shift in the treatment options of hepatocellular carcinoma. Liver Int. 2022, 42, 2067–2079. [Google Scholar] [CrossRef]
- Mazzaferro, V. Squaring the circle of selection and allocation in liver transplantation for HCC: An adaptive approach. Hepatology 2016, 63, 1707–1717. [Google Scholar] [CrossRef]
- Yao, F.Y.; Hirose, R.; LaBerge, J.M.; Davern, T.J.; Bass, N.M.; Kerlan, R.K.; Merriman, R.; Feng, S.; Freise, C.E.; Ascher, N.L.; et al. A prospective study on downstaging of hepatocellular carcinoma prior to liver transplantation. Liver Transpl. 2005, 11, 1505–1514. [Google Scholar] [CrossRef] [PubMed]
- Sandow, T.A.; Arndt, S.E.; Albar, A.A.; DeVun, D.A.; Kirsch, D.S.; Gimenez, J.M.; Bohorquez, H.E.; Gilbert, P.J.; Thevenot, P.T.; Nunez, K.G.; et al. Assessment of Response to Transcatheter Arterial Chemoembolization with Doxorubicin-eluting Microspheres: Tumor Biology and Hepatocellular Carcinoma Recurrence in a 5-year Transplant Cohort. Radiology 2018, 286, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Minici, R.; Ammendola, M.; Manti, F.; Siciliano, M.A.; Giglio, E.; Minici, M.; Melina, M.; Currò, G.; Laganà, D. Safety and Efficacy of Degradable Starch Microspheres Transcatheter Arterial Chemoembolization as a Bridging Therapy in Patients with Early Stage Hepatocellular Carcinoma and Child-Pugh Stage B Eligible for Liver Transplant. Front. Pharmacol. 2021, 12, 634084. [Google Scholar] [CrossRef]
- Cheng, A.-L.; Kang, Y.-K.; Chen, Z.; Tsao, C.-J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.-S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Rossi, J.-F.; Lu, Z.Y.; Massart, C.; Levon, K. Dynamic Immune/Inflammation Precision Medicine: The Good and the Bad Inflammation in Infection and Cancer. Front. Immunol. 2021, 12, 595722. [Google Scholar] [CrossRef]
- Mei, J.; Sun, X.-Q.; Lin, W.-P.; Li, S.-H.; Lu, L.-H.; Zou, J.-W.; Wei, W.; Guo, R.-P. Comparison of the Prognostic Value of Inflammation-Based Scores in Patients with Hepatocellular Carcinoma After Anti-PD-1 Therapy. J. Inflamm. Res. 2021, 14, 3879–3890. [Google Scholar] [CrossRef]
- Wang, C.; Wang, M.; Zhang, X.; Zhao, S.; Hu, J.; Han, G.; Liu, L. The neutrophil-to-lymphocyte ratio is a predictive factor for the survival of patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Ann. Transl. Med. 2020, 8, 541. [Google Scholar] [CrossRef] [PubMed]
- Xue, T.-C.; Jia, Q.-A.; Ge, N.-L.; Zhang, B.-H.; Wang, Y.-H.; Ren, Z.-G.; Ye, S.-L. The platelet-to-lymphocyte ratio predicts poor survival in patients with huge hepatocellular carcinoma that received transarterial chemoembolization. Tumour Biol. 2015, 36, 6045–6051. [Google Scholar] [CrossRef]
- Iseda, N.; Itoh, S.; Yoshizumi, T.; Tomiyama, T.; Morinaga, A.; Shimagaki, T.; Wang, H.; Kurihara, T.; Toshima, T.; Nagao, Y.; et al. Lymphocyte-to-C-reactive protein ratio as a prognostic factor for hepatocellular carcinoma. Int. J. Clin. Oncol. 2021, 26, 1890–1900. [Google Scholar] [CrossRef] [PubMed]
- Ozawa, T.; Ishihara, S.; Kawai, K.; Kazama, S.; Yamaguchi, H.; Sunami, E.; Kitayama, J.; Watanabe, T. Impact of a lymphocyte to monocyte ratio in stage IV colorectal cancer. J. Surg. Res. 2015, 199, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Stotz, M.; Pichler, M.; Absenger, G.; Szkandera, J.; Arminger, F.; Schaberl-Moser, R.; Samonigg, H.; Stojakovic, T.; Gerger, A. The preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Br. J. Cancer 2014, 110, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-J.; Lin, Y.-X.; Ye, H.; Li, F.-Y.; Xiong, X.-Z.; Cheng, N.-S. Lymphocyte to monocyte ratio and prognostic nutritional index predict survival outcomes of hepatitis B virus-associated hepatocellular carcinoma patients after curative hepatectomy. J. Surg. Oncol. 2016, 114, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.-X.; Ruan, D.-Y.; Li, Y.; Wu, D.-H.; Ma, X.-K.; Chen, J.; Chen, Z.-H.; Li, X.; Wang, T.-T.; Lin, Q.; et al. Lymphocyte-to-monocyte ratio predicts survival of patients with hepatocellular carcinoma after curative resection. World J. Gastroenterol. 2015, 21, 10898–10906. [Google Scholar] [CrossRef] [PubMed]
- Minici, R.; Siciliano, M.A.; Ammendola, M.; Santoro, R.C.; Barbieri, V.; Ranieri, G.; Laganà, D. Prognostic Role of Neutrophil-to-Lymphocyte Ratio (NLR), Lymphocyte-to-Monocyte Ratio (LMR), Platelet-to-Lymphocyte Ratio (PLR) and Lymphocyte-to-C Reactive Protein Ratio (LCR) in Patients with Hepatocellular Carcinoma (HCC) undergoing Chemoembolizations (TACE) of the Liver: The Unexplored Corner Linking Tumor Microenvironment, Biomarkers and Interventional Radiology. Cancers 2022, 15, 257. [Google Scholar] [CrossRef] [PubMed]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Lucatelli, P.; Burrel, M.; Guiu, B.; de Rubeis, G.; van Delden, O.; Helmberger, T. CIRSE Standards of Practice on Hepatic Transarterial Chemoembolisation. Cardiovasc. Interv. Radiol. 2021, 44, 1851–1867. [Google Scholar] [CrossRef]
- Gaba, R.C.; Lokken, R.P.; Hickey, R.M.; Lipnik, A.J.; Lewandowski, R.J.; Salem, R.; Brown, D.B.; Walker, T.G.; Silberzweig, J.E.; Baerlocher, M.O.; et al. Quality Improvement Guidelines for Transarterial Chemoembolization and Embolization of Hepatic Malignancy. J. Vasc. Interv. Radiol. 2017, 28, 1210–1223.e3. [Google Scholar] [CrossRef]
- Lencioni, R.; de Baere, T.; Burrel, M.; Caridi, J.G.; Lammer, J.; Malagari, K.; Martin, R.C.G.; O’Grady, E.; Real, M.I.; Vogl, T.G.; et al. Transcatheter Treatment of Hepatocellular Carcinoma with Doxorubicin-loaded DC Bead (DEBDOX): Technical Recommendations. Cardiovasc. Interv. Radiol. 2012, 35, 980–985. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef]
- Lammer, J.; Malagari, K.; Vogl, T.; Pilleul, F.; Denys, A.; Watkinson, A.; Pitton, M.; Sergent, G.; Pfammatter, T.; Terraz, S.; et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: Results of the PRECISION V study. Cardiovasc. Interv. Radiol. 2010, 33, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, M.; Chen, M.; Mei, J.; Xu, L.; Guo, R.; Lin, X.; Li, J.; Peng, Z. Association of Sustained Response Duration With Survival After Conventional Transarterial Chemoembolization in Patients With Hepatocellular Carcinoma. JAMA Netw. Open 2018, 1, e183213. [Google Scholar] [CrossRef]
- Rossi, R.; Talarico, M.; Pascale, A.; Pascale, V.; Minici, R.; Boriani, G. Low Levels of Vitamin D and Silent Myocardial Ischemia in Type 2 Diabetes: Clinical Correlations and Prognostic Significance. Diagnostics 2022, 12, 2572. [Google Scholar] [CrossRef] [PubMed]
- Minici, R.; Serra, R.; Ierardi, A.M.; Petullà, M.; Bracale, U.M.; Carrafiello, G.; Laganà, D. Thoracic endovascular repair for blunt traumatic thoracic aortic injury: Long-term results. Vascular 2022, 32, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Bracale, U.M.; Peluso, A.; Panagrosso, M.; Cecere, F.; DEL Guercio, L.; Minici, R.; Giannotta, N.; Ielapi, N.; Licastro, N.; Serraino, G.F.; et al. Ankle-Brachial Index evaluation in totally percutaneous approach vs. femoral artery cutdown for endovascular aortic repair of abdominal aortic aneurysms. Chirurgia 2022, 35, 349–354. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; Giurdanella, M.; Talarico, M.; Siciliano, M.A.; Carrafiello, G.; Laganà, D. Efficacy and Safety of Distal Radial Access for Transcatheter Arterial Chemoembolization (TACE) of the Liver. J. Pers. Med. 2023, 13, 640. [Google Scholar] [CrossRef]
- Minici, R.; Venturini, M.; Fontana, F.; Guzzardi, G.; Pingitore, A.; Piacentino, F.; Serra, R.; Coppola, A.; Santoro, R.; Laganà, D. Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study. Medicina 2023, 59, 710. [Google Scholar] [CrossRef]
- Minici, R.; Fontana, F.; Venturini, M.; Guzzardi, G.; Siciliano, A.; Piacentino, F.; Serra, R.; Coppola, A.; Guerriero, P.; Apollonio, B.; et al. Transcatheter Arterial Embolization (TAE) in the Management of Bleeding in the COVID-19 Patient. Medicina 2023, 59, 1062. [Google Scholar] [CrossRef]
- Zhu, Z.-F.; Zhuang, L.-P.; Zhang, C.-Y.; Ning, Z.-Y.; Wang, D.; Sheng, J.; Hua, Y.-Q.; Xie, J.; Xu, L.-T.; Meng, Z.-Q. Predictive role of the monocyte-to-lymphocyte ratio in advanced hepatocellular carcinoma patients receiving anti-PD-1 therapy. Transl. Cancer Res. 2022, 11, 160–170. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; De Rosi, N.; Ciranni, S.; Talarico, M.; Petullà, M.; Guzzardi, G.; Fontana, F.; Laganà, D. Endovascular treatment of femoro-popliteal occlusions with retrograde tibial access after failure of the antegrade approach. Catheter. Cardiovasc. Interv. 2023, 101, 1108–1119. [Google Scholar] [CrossRef] [PubMed]
- Cernigliaro, M.; Stanca, C.; Galbiati, A.; Spinetta, M.; Coda, C.; Negroni, D.; Laganà, D.; Minici, R.; Airoldi, C.; Carriero, A.; et al. Innovation in Acute Ischemic Stroke Patients over 80 y/o—A Retrospective Monocentric Study on Mechanical Thrombectomy of Consecutive Patients: Is Age an Adequate Selection Criterion? J. Clin. Med. 2023, 12, 3688. [Google Scholar] [CrossRef] [PubMed]
- Nahm, F.S. Receiver operating characteristic curve: Overview and practical use for clinicians. Korean J. Anesthesiol. 2022, 75, 25. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Li, L.; Chen, G.; Zhang, Y.; Gao, Q. The lymphocyte-to-monocyte ratio could predict the efficacy of PD-1 inhibitors in patients with advanced cancer. Transl. Cancer Res. 2020, 9, 4111–4120. [Google Scholar] [CrossRef] [PubMed]
- Väyrynen, J.P.; Tuomisto, A.; Klintrup, K.; Mäkelä, J.; Karttunen, T.J.; Mäkinen, M.J. Detailed analysis of inflammatory cell infiltration in colorectal cancer. Br. J. Cancer 2013, 109, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Labani-Motlagh, A.; Ashja-Mahdavi, M.; Loskog, A. The Tumor Microenvironment: A Milieu Hindering and Obstructing Antitumor Immune Responses. Front. Immunol. 2020, 11, 940. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Chanmee, T.; Ontong, P.; Konno, K.; Itano, N. Tumor-associated macrophages as major players in the tumor microenvironment. Cancers 2014, 6, 1670–1690. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, S.; Yasuda, K.; Suzuki, K.; Tahara, K.; Higashi, H.; Era, S. Macrophage infiltration and its prognostic implications in breast cancer: The relationship with VEGF expression and microvessel density. Oncol. Rep. 2005, 14, 425–431. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef]
- Itoh, S.; Yugawa, K.; Shimokawa, M.; Yoshiya, S.; Mano, Y.; Takeishi, K.; Toshima, T.; Maehara, Y.; Mori, M.; Yoshizumi, T. Prognostic significance of inflammatory biomarkers in hepatocellular carcinoma following hepatic resection. BJS Open 2019, 3, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Qiao, W.; Liu, B.; Li, J.; Yuan, C.; Long, J.; Hu, C.; Zang, C.; Zheng, J.; Zhang, Y. The monocyte to lymphocyte ratio not only at baseline but also at relapse predicts poor outcomes in patients with hepatocellular carcinoma receiving locoregional therapy. BMC Gastroenterol. 2022, 22, 98. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Wang, H.; Chen, X.; Li, W.; Chen, J. Prognostic significance of lymphocyte-to-monocyte ratio and platelet-to-lymphocyte ratio in patients with hepatocellular carcinoma undergoing transcatheter arterial chemoembolization and radiofrequency ablation. Onco Targets Ther. 2019, 12, 7129–7137. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Shi, M.; Chen, S.; Wan, W.; Shen, L.; Shen, B.; Qi, H.; Cao, F.; Wu, Y.; Huang, T.; et al. Intermediate stage hepatocellular carcinoma: Comparison of the value of inflammation-based scores in predicting progression-free survival of patients receiving transarterial chemoembolization. J. Cancer Res. Ther. 2021, 17, 740–748. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, W.; Niu, R.; Li, Y.; Zhou, X.; Han, X. A combination of the preoperative neutrophil-to-lymphocyte and lymphocyte-to-monocyte ratios as a useful predictor of survival outcomes following the transarterial chemoembolization of huge hepatocellular carcinoma. Saudi Med. J. 2020, 41, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Unitt, E.; Marshall, A.; Gelson, W.; Rushbrook, S.M.; Davies, S.; Vowler, S.L.; Morris, L.S.; Coleman, N.; Alexander, G.J. Tumour lymphocytic infiltrate and recurrence of hepatocellular carcinoma following liver transplantation. J. Hepatol. 2006, 45, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.-D.; Zhang, J.-B.; Zhuang, P.-Y.; Zhu, H.-G.; Zhang, W.; Xiong, Y.-Q.; Wu, W.-Z.; Wang, L.; Tang, Z.-Y.; Sun, H.-C. High expression of macrophage colony-stimulating factor in peritumoral liver tissue is associated with poor survival after curative resection of hepatocellular carcinoma. J. Clin. Oncol. 2008, 26, 2707–2716. [Google Scholar] [CrossRef]
- Yang, Y.-T.; Jiang, J.-H.; Yang, H.-J.; Wu, Z.; Xiao, Z.-M.; Xiang, B.-D. The lymphocyte-to-monocyte ratio is a superior predictor of overall survival compared to established biomarkers in HCC patients undergoing liver resection. Sci. Rep. 2018, 8, 2535. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | All Patients (n = 109) | |||
|---|---|---|---|---|
| Group 1 Low LMR (n = 35) | Group 2 High LMR (n = 74) | p Value | ||
| Age (years) | 57.1 (±13.7) | 54.4 (±14.2) | 58.4 (±13.4) | 0.124 |
| Sex (F) | 32 (29.4%) | 14 (40%) | 18 (24.3%) | 0.093 |
| Hepatitis B virus | 15 (13.8%) | 4 (11.4%) | 11 (14.9%) | 0.627 |
| Hepatitis C virus | 47 (43.1%) | 7 (20%) | 40 (54.1%) | 0.001 |
| Non-alcoholic fatty liver disease | 9 (8.3%) | 5 (14.3%) | 4 (5.4%) | 0.116 |
| Alcoholic liver disease | 45 (41.3%) | 18 (51.4%) | 27 (36.5%) | 0.139 |
| α-Fetoprotein (ng/mL) | 236.5 (±225.8) | 311.9 (±286.7) | 200.8 (±182.1) | 0.110 |
| Carbohydrate antigen 19-9 (U/mL) | 11.4 (±13.6) | 12.3 (±13.7) | 10.9 (±13.6) | 0.803 |
| γ-Glutamyltransferase (U/L) | 88.7 (±56.8) | 91.8 (±71.5) | 87.2 (±48.9) | 0.953 |
| Alkaline phosphatase (U/L) | 52.4 (±21.9) | 54.3 (±21) | 51.5 (±22.4) | 0.285 |
| Aspartate transaminase (U/L) | 64.1 (±28.7) | 57.7 (±29.3) | 67.1 (±28.1) | 0.296 |
| Alanine transaminase (U/L) | 68.5 (±25.1) | 70.3 (±25.8) | 67.6 (±24.9) | 0.422 |
| Albumin (g/L) | 30.1 (±2.7) | 29.5 (±2.4) | 30.4 (±2.8) | 0.116 |
| Total bilirubin (mg/dL) | 1.12 (±0.4) | 1.05 (±0.37) | 1.15 (±0.42) | 0.165 |
| Prothrombin time (seconds prolonged) | 6.4 (±1.4) | 6.3 (±1.4) | 6.5 (±1.4) | 0.329 |
| Ascites | 0 (0%) | 0 (0%) | 0 (0%) | NA |
| Child–Pugh score, A6/B7/B8/B9 | 5 (4.6%)/37 (33.9%)/65 (59.6%)/2 (1.8%) | 0 (0%)/13 (37.1%)/21 (60%)/1 (2.9%) | 5 (6.8%)/24 (32.4%)/44 (59.5%)/1 (1.4%) | 0.421 |
| Cirrhosis | 107 (98.2%) | 34 (97.1%) | 73 (98.6%) | 0.584 |
| Platelet count (No. ×103/μL) | 135.1 (±51) | 128.5 (±43.2) | 138.2 (±54.3) | 0.597 |
| Hemoglobin (g/dL) | 11.5 (±1.43) | 11.8 (±1.48) | 11.4 (±1.40) | 0.241 |
| White blood cell count (per μL) | 4642 (±825.6) | 4771 (±722.7) | 4580 (±868) | 0.136 |
| Neutrophil count (per μL) | 3332 (±776.2) | 3604.9 (±747.9) | 3203 (±760.7) | 0.011 |
| Lymphocyte count (per μL) | 901.8 (±322.4) | 710.8 (±287.6) | 992.2 (±299.1) | <0.001 |
| Monocyte count (per μL) | 245.8 (±81.4) | 277.1 (±79.2) | 231.1 (±78.7) | 0.003 |
| Lymphocyte-to-monocyte ratio (LMR) | 4.25 (±2.29) | 2.82 (±1.58) | 4.92 (±2.26) | <0.001 |
| Number of tumors, 1/2/3 | 42 (38.5%)/34 (31.2%)/33 (30.3%) | 12 (34.3%)/11 (31.4%)/12 (34.3%) | 30 (40.5%)/23 (31.1%)/21 (28.4%) | 0.773 |
| Maximum tumour size (cm) | 4.50 (±1.13) | 4.42 (±1.10) | 4.54 (±1.15) | 0.651 |
| Bilobar disease | 46 (42.2%) | 15 (42.9%) | 31 (41.9%) | 0.924 |
| Capsule | 56 (51.4%) | 20 (57.1%) | 36 (48.6%) | 0.407 |
| Variables | All Patients (n = 109) | |||
|---|---|---|---|---|
| Group 1 Low LMR (n = 35) | Group 2 High LMR (n = 74) | p Value | ||
| Technical success | 109 (100%) | 35 (100%) | 74 (100%) | NA |
| Tumour response | 0.017 | |||
| CR | 11 (10.1%) | 0 (0%) | 11 (14.9%) | |
| PR | 26 (23.9%) | 5 (14.3%) | 21 (28.4%) | |
| SD | 49 (45%) | 20 (57.1%) | 29 (39.2%) | |
| PD | 23 (21.1%) | 10 (28.6%) | 13 (17.6%) | |
| Complete response | 11 (10.1%) | 0 (0%) | 11 (14.9%) | 0.016 |
| Objective response (CR + PR) | 37 (33.9%) | 5 (14.3%) | 32 (43.2%) | 0.003 |
| Sustained response duration ≥ 6 months | 57 (52.3%) | 19 (54.3%) | 38 (51.4%) | 0.775 |
| Overall survival at 6 months | 109 (100%) | 35 (100%) | 74 (100%) | NA |
| Progression-free survival at 6 months | 72 (66.1%) | 16 (45.7%) | 56 (75.7%) | 0.002 |
| Successful downstaging at 6 months | 12 (11%) | 0 (0%) | 12 (16.2%) | 0.012 |
| Post-procedural clinical complications (CIRSE classification) | 33 (30.3%) | 12 (34.3%) | 21 (28.4%) | 0.340 |
| Grade 1 | 28 (25.7%) | 11 (31.4%) | 17 (23%) | |
| Grade 2 | 0 (0%) | 0 (0%) | 0 (0%) | |
| Grade 3 | 5 (4.6%) | 1 (2.9%) | 4 (5.4%) | |
| Grade ≥ 4 | 0 (0%) | 0 (0%) | 0 (0%) | |
| Adverse Events (CTCAE classification) | 50 (45.9%) | 10 (28.6%) | 40 (54.1%) | 0.013 |
| Grade 1 | 29 (26.6%) | 3 (8.6%) | 26 (35.1%) | |
| Grade 2 | 16 (14.7%) | 6 (17.1%) | 10 (13.5%) | |
| Grade 3 | 5 (4.6%) | 1 (2.9%) | 4 (5.4%) | |
| Grade 4 | 0 (0%) | 0 (0%) | 0 (0%) |
| Predictors | Coeff. | Std. Err. | Wald | p > |z| |
|---|---|---|---|---|
| Age (years) | 0.530/0.071 | 0.02/0.02 | 9.093/8.653 | 0.003/0.003 |
| Sex | −0.172 | 0.45 | 0.147 | 0.702 |
| Hepatitis C virus | −0.860/−2.367 | 0.43/0.68 | 4.001/12.086 | 0.045–0.001 |
| α-Fetoprotein (ng/mL) | −0.004/−0.004 | <0.01/<0.01 | 7.178/4.833 | 0.007–0.028 |
| Albumin (g/L) | 0.047 | 0.74 | 0.404 | 0.525 |
| White blood cell count (per μL) | 0 | 0 | 0.112 | 0.738 |
| Neutrophil count (per μL) | 0 | 0 | 0.468 | 0.494 |
| Lymphocyte count (per μL) | 0.003/0.002 | <0.01/<0.01 | 13.897/4.054 | <0.001/0.044 |
| Monocyte count (per μL) | −0.005 | <0.01 | 3.274 | 0.070 |
| Lymphocyte-to-monocyte ratio (LMR) | 0.325/0.247 | 0.10/0.18 | 11.283/1.792 | 0.001/0.181 |
| LMR Groups (<2.24; ≥2.24) | 1.520/1.578 | 0.54/0.74 | 8.009/4.488 | 0.005–0.034 |
| Predictors | Coeff. | Std. Err. | Wald | p > |z| |
|---|---|---|---|---|
| Age (years) | −0.014 | 0.01 | 0.804 | 0.370 |
| Sex | 0.222 | 0.44 | 0.255 | 0.614 |
| Hepatitis C virus | −0.174 | 0.41 | 0.182 | 0.669 |
| α-Fetoprotein (ng/mL) | −0.002 | <0.01 | 3.305 | 0.069 |
| Albumin (g/L) | −0.009 | 0.07 | 0.014 | 0.906 |
| White blood cell count (per μL) | 0 | 0 | 2.344 | 0.126 |
| Neutrophil count (per μL) | −0.001/0/0 | 0/0/0 | 4.629/0.202/2.393 | 0.031/0.653/0.122 |
| Lymphocyte count (per μL) | 0.003/0.003 | <0.01/<0.01 | 15.125/3.431 | <0.001/0.064 |
| Monocyte count (per μL) | −0.017/−0.017 | <0.01/<0.01 | 20.299/5.261 | <0.001/0.022 |
| Lymphocyte-to-monocyte ratio (LMR) | 0.777/0.200 | 0.17/0.41 | 20.873/0.234 | <0.001/0.629 |
| LMR Groups (<2.24; ≥2.24) | 1.307/0.326/1.162 | 0.43/0.58/0.45 | 9.058/0.319/6.798 | 0.003/0.572/0.009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minici, R.; Venturini, M.; Guzzardi, G.; Fontana, F.; Coppola, A.; Piacentino, F.; Torre, F.; Spinetta, M.; Maglio, P.; Guerriero, P.; et al. Prognostic Role of Lymphocyte-to-Monocyte Ratio (LMR) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations (DEM-TACE or cTACE) of the Liver: Exploring the Link between Tumor Microenvironment and Interventional Radiology. Diseases 2024, 12, 137. https://doi.org/10.3390/diseases12070137
Minici R, Venturini M, Guzzardi G, Fontana F, Coppola A, Piacentino F, Torre F, Spinetta M, Maglio P, Guerriero P, et al. Prognostic Role of Lymphocyte-to-Monocyte Ratio (LMR) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations (DEM-TACE or cTACE) of the Liver: Exploring the Link between Tumor Microenvironment and Interventional Radiology. Diseases. 2024; 12(7):137. https://doi.org/10.3390/diseases12070137
Chicago/Turabian StyleMinici, Roberto, Massimo Venturini, Giuseppe Guzzardi, Federico Fontana, Andrea Coppola, Filippo Piacentino, Federico Torre, Marco Spinetta, Pietro Maglio, Pasquale Guerriero, and et al. 2024. "Prognostic Role of Lymphocyte-to-Monocyte Ratio (LMR) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations (DEM-TACE or cTACE) of the Liver: Exploring the Link between Tumor Microenvironment and Interventional Radiology" Diseases 12, no. 7: 137. https://doi.org/10.3390/diseases12070137
APA StyleMinici, R., Venturini, M., Guzzardi, G., Fontana, F., Coppola, A., Piacentino, F., Torre, F., Spinetta, M., Maglio, P., Guerriero, P., Ammendola, M., MGJR Research Team, Brunese, L., & Laganà, D. (2024). Prognostic Role of Lymphocyte-to-Monocyte Ratio (LMR) in Patients with Intermediate-Stage Hepatocellular Carcinoma (HCC) Undergoing Chemoembolizations (DEM-TACE or cTACE) of the Liver: Exploring the Link between Tumor Microenvironment and Interventional Radiology. Diseases, 12(7), 137. https://doi.org/10.3390/diseases12070137