

The COVID-19 Experience in Adolescents: Emotional and Behavioral Recall at the End of the Pandemic

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Participants and Methods
2.1. Research Design, Procedure, and Participants
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Smith, A.J.; Moreno-López, L.; Davidson, E.; Dauvermann, M.; Orellana, S.; Soneson, E.; Ioannidis, K.; Kaser, M.; van Harmelen, A.L. REACT study protocol: Resilience after the COVID-19 threat (REACT) in adolescents. BMJ 2021, 11, e042824. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Meade, J. Mental Health Effects of the COVID-19 Pandemic on Children and Adolescents: A Review of the Current Research. Pediatr. Clin. N. Am. 2021, 6, 945–959. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent-child discussion. J. Affect. Disord. 2021, 279, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Shao, X.; Wang, Y.; Huang, Y.; Miao, J.; Yang, X.; Zhu, G. An investigation of mental health status of children and adolescents in China during the outbreak of COVID-19. J. Affect. Disord. 2020, 275, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Gibbs, B.B.; Kline, C.E.; Stoner, L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Hanifah, L.; Nasrulloh, N.; Sufyan, D.L. Sedentary Behavior and Lack of Physical Activity among Children in Indonesia. Children 2023, 10, 1283. [Google Scholar] [CrossRef]
- Paterson, D.C.; Ramage, K.; Moore, S.A.; Riazi, N.; Tremblay, M.S.; Faulkner, G. Exploring the impact of COVID-19 on the movement behaviors of children and youth: A scoping review of evidence after the first year. J. Sport Health Sci. 2021, 10, 675–689. [Google Scholar] [CrossRef]
- Ten Velde, G.; Lubrecht, J.; Arayess, L.; van Loo, C.; Hesselink, M.; Reijnders, D.; Vreugdenhil, A. Physical activity behavior and screen time in Dutch children during the COVID-19 pandemic: Pre-, during- and post-school closures. Pediatr. Obes. 2021, 16, e12779. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- An, R. Projecting the impact of the coronavirus disease-2019 pandemic on childhood obesity in the United States: A microsimulation model. J. Sport Health Sci. 2020, 9, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, I.; Delle Cave, F.; Guarracino, C.; De Filippo, M.; Votto, M.; Licari, A.; Pistone, C.; Tondina, E. Obesity and COVID-19 in children and adolescents: A double pandemic. Acta Biomed. 2022, 93 (Suppl. 3), e2022195. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef] [PubMed]
- Zaccagni, L.; Toselli, S.; Barbieri, D. Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6416. [Google Scholar] [CrossRef] [PubMed]
- Montanari, M. La scuola ai tempi del Coronavirus: Esperienze, narrazioni, emozioni, riflessioni. J. Health Care Educ. Pract. 2021, 3, 99–104. [Google Scholar]
- IRCCS-Gaslini. Impatto Psicologico e Comportamentale sui Bambini delle Famiglie in Italia. 2020. Available online: https://www.gaslini.org/wp-content/uploads/2020/06/Indagine-Irccs-Gaslini.pdf (accessed on 20 February 2024).
- Dallavalle, G.; Pezzotti, E.; Provenzi, L.; Toni, F.; Carpani, A.; Borgatti, R. Migraine symptoms improvement during the COVID-19 lockdown in a cohort of children and adolescents. Front. Neurol. 2020, 11, 579047. [Google Scholar] [CrossRef] [PubMed]
- Camera dei Deputati. Le Misure Adottate a Seguito Dell’emergenza Coronavirus (COVID-19) per il Mondo Dell’istruzione (Scuola, Istruzione e Formazione Professionale, Università, Istituzioni AFAM). 2022. Available online: https://temi.camera.it/leg18/temi/le-misure-adottate-a-seguito-dell-emergenza-coronavirus-covid-19-per-il-mondo-dell-istruzione-scuola-istruzione-e-formazione-professionale-universit-istituzioni-afam.html#:~:text=A%20seguito%20dell’emergenza%20da,quelle%20relative%20all’anno%20accademico (accessed on 19 February 2024).
- ISS. Apertura delle Scuole e Andamento dei Casi Confermati di SARS-CoV-2: La Situazione in Italia. 30 December 2020. Available online: https://www.iss.it/documents/20126/0/Rapporto+ISS+COVID-19+n.+63_2020.pdf/7b3d3626-3982-f7a1-86ef-1ede83e170a4?t=1609758939391 (accessed on 19 February 2024).
- Harris, E. WHO Declares End of COVID-19 Global Health Emergency. JAMA 2023, 329, 1817. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. COVID-19: WHO declares end of global health emergency. BMJ 2023, 381, 1041. [Google Scholar] [CrossRef]
- Okuyama, J.; Seto, S.; Fukuda, Y.; Funakoshi, S.; Amae, S.; Onobe, J.; Izumi, S.; Ito, K.; Imamura, F. Mental Health and Physical Activity among Children and Adolescents during the COVID-19 Pandemic. Tohoku J. Exp. Med. 2021, 253, 203–215. [Google Scholar] [CrossRef]
- Ladouceur, C.D. COVID-19 Adolescent Symptom & Psychological Experience (CASPE) Questionnaire. 2020. Available online: https://www.phenxtoolkit.org/toolkit_content/PDF/CASPE_Parent_Emotional.pdf (accessed on 19 February 2024).
- CRISIS. The Coronavirus Health Impact Survey. Available online: http://www.crisissurvey.org/ (accessed on 19 February 2024).
- Gualdi-Russo, E.; Rinaldo, N.; Mazzoni, G.; Mandini, S.; Masotti, S.; Toselli, S.; Zaccagni, L. Age at Menarche, Growth Velocity, and Adiposity Indices in Italian Girls Aged 10 to 14. Children 2022, 9, 1928. [Google Scholar] [CrossRef]
- Zaccagni, L.; Rosa, L.; Toselli, S.; Gualdi-Russo, E. Sports Practice, Body Image Perception, and Factors Involved in Sporting Activity in Italian Schoolchildren. Children 2023, 10, 1850. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C. Sample Size and its Importance in Research. Indian J. Psychol. Med. 2020, 42, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- Gualdi Russo, E. Metodi Antropometrici: Generalità e principali caratteri antropometrici. In Manuale di Antropologia. Evoluzione e Biodiversità Umana; Sineo, L., Moggi Cecchi, J., Eds.; UTET: Torino, Italy, 2022; pp. 55–75. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- Silk, J.S.; Scott, L.N.; Hutchinson, E.A.; Lu, C.; Sequeira, S.L.; McKone, K.M.P.; Do, Q.B.; Ladouceur, C.D. Storm Clouds and Silver Linings: Day-to-Day Life in COVID-19 Lockdown and Emotional Health in Adolescent Girls. J. Pediatr. Psychol. 2022, 47, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle Changes and Determinants of Children’s and Adolescents’ Body Weight Increase during the First COVID-19 Lockdown in Greece: The COV-EAT Study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef] [PubMed]
- Amo-Setién, F.J.; Leal-Costa, C.; Abajas-Bustillo, R.; González-Lamuño, D.; Redondo-Figuero, C. Factors associated with grip strength among adolescents: An observational study. J. Hand Ther. 2020, 33, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.S.; Skrondal, A. The Cambridge Dictionary of Statistics; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Berchtold, A. Test-retest: Agreement or reliability? Methodol. Innov. 2016, 9, 1–7. [Google Scholar] [CrossRef]
- Gualdi-Russo, E.; Rinaldo, N.; Toselli, S.; Zaccagni, L. Associations of Physical Activity and Sedentary Behaviour Assessed by Accelerometer with Body Composition among Children and Adolescents: A Scoping Review. Sustainability 2021, 13, 335. [Google Scholar] [CrossRef]
- Toselli, S.; Grigoletto, A.; Zaccagni, L.; Rinaldo, N.; Badicu, G.; Grosz, W.R.; Campa, F. Body image perception and body composition in early adolescents: A longitudinal study of an Italian cohort. BMC Public Health 2021, 21, 1381. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: A pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet 2024, 403, 1027–1050. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.N.; Yoshida-Montezuma, Y.; Dewart, N.; Jalil, E.; Khattar, J.; De Rubeis, V.; Carsley, S.; Griffith, L.E.; Mbuagbaw, L. Obesity and weight change during the COVID-19 pandemic in children and adults: A systematic review and meta-analysis. Obes. Rev. 2023, 24, e13550. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Chourdakis, M. Impact of the first COVID-19 lockdown 341 on body weight: A combined systematic review and a meta-analysis. Clin. Nutr. 2022, 41, 3046–3054. [Google Scholar] [CrossRef] [PubMed]
- Daniel, M.M.; Liboredo, J.C.; Anastácio, L.R.; Souza, T.C.M.; Oliveira, L.A.; Della Lucia, C.M.; Ferreira, L.G. Incidence and Associated Factors of Weight Gain During the Covid-19 Pandemic. Front. Nutr. 2022, 9, 818632. [Google Scholar] [CrossRef]
- Jenssen, B.P.; Kelly, M.K.; Powell, M.; Bouchelle, Z.; Mayne, S.L.; Fiks, A.G. COVID-19 and Changes in Child Obesity. Pediatrics 2021, 147, e2021050123. [Google Scholar] [CrossRef] [PubMed]
- Bacaro, V.; Gavriloff, D.; Lombardo, C.; Baglioni, C. Sleep Characteristics in the Italian Pediatric Population: A Systematic Review. Clin. Neuropsychiatry 2021, 18, 119–136. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Maslowsky, J.; Hamilton, A.; Schulenberg, J. The great sleep recession: Changes in sleep duration among US adolescents, 1991–2012. Pediatrics 2015, 135, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Dvorsky, M.R.; Breaux, R.; Cusick, C.N.; Taylor, K.P.; Langberg, J.M. Prospective examination of adolescent sleep patterns and behaviors before and during COVID-19. Sleep 2021, 44, zsab054. [Google Scholar] [CrossRef]
- Rabinowitz, A.R.; Arnett, P.A. Positive psychology perspective on traumatic brain injury recovery and rehabilitation. Appl. Neuropsychol. Adult 2008, 25, 295–303. [Google Scholar] [CrossRef]
- Ashour, R.; Halstead, E.J.; Mangar, S.; Lin, V.K.Q.; Azhari, A.; Carollo, A.; Esposito, G.; Threadgold, L.; Dimitriou, D. Childhood experiences and sleep problems: A cross-sectional study on the indirect relationship mediated by stress, resilience and anxiety. PLoS ONE 2024, 19, e0299057. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Blendermann, M.; Ebalu, T.I.; Obisie-Orlu, I.C.; Fried, E.I.; Hallion, L.S. A narrative systematic review of changes in mental health symptoms from before to during the COVID-19 pandemic. Psychol. Med. 2024, 54, 43–66. [Google Scholar] [CrossRef] [PubMed]
- Araujo, C.P.; Piva, J.; Vettoretti Nicoladeli, A.; Paniz Hartwig, J.; Vieira, A.P.R.; Sica Rocha, N.; Rocha, T.S. Lifestyle and quality of life in children and adolescents during the covid-19 social distancing period. J. Pediatr. 2024, 100, 53–59. [Google Scholar] [CrossRef]
- Adams, E.L.; Caccavale, L.J.; Smith, D.; Bean, M.K. Food Insecurity, the Home Food Environment, and Parent Feeding Practices in the Era of COVID-19. Obesity 2020, 28, 2056–2063. [Google Scholar] [CrossRef]

{kind=link}
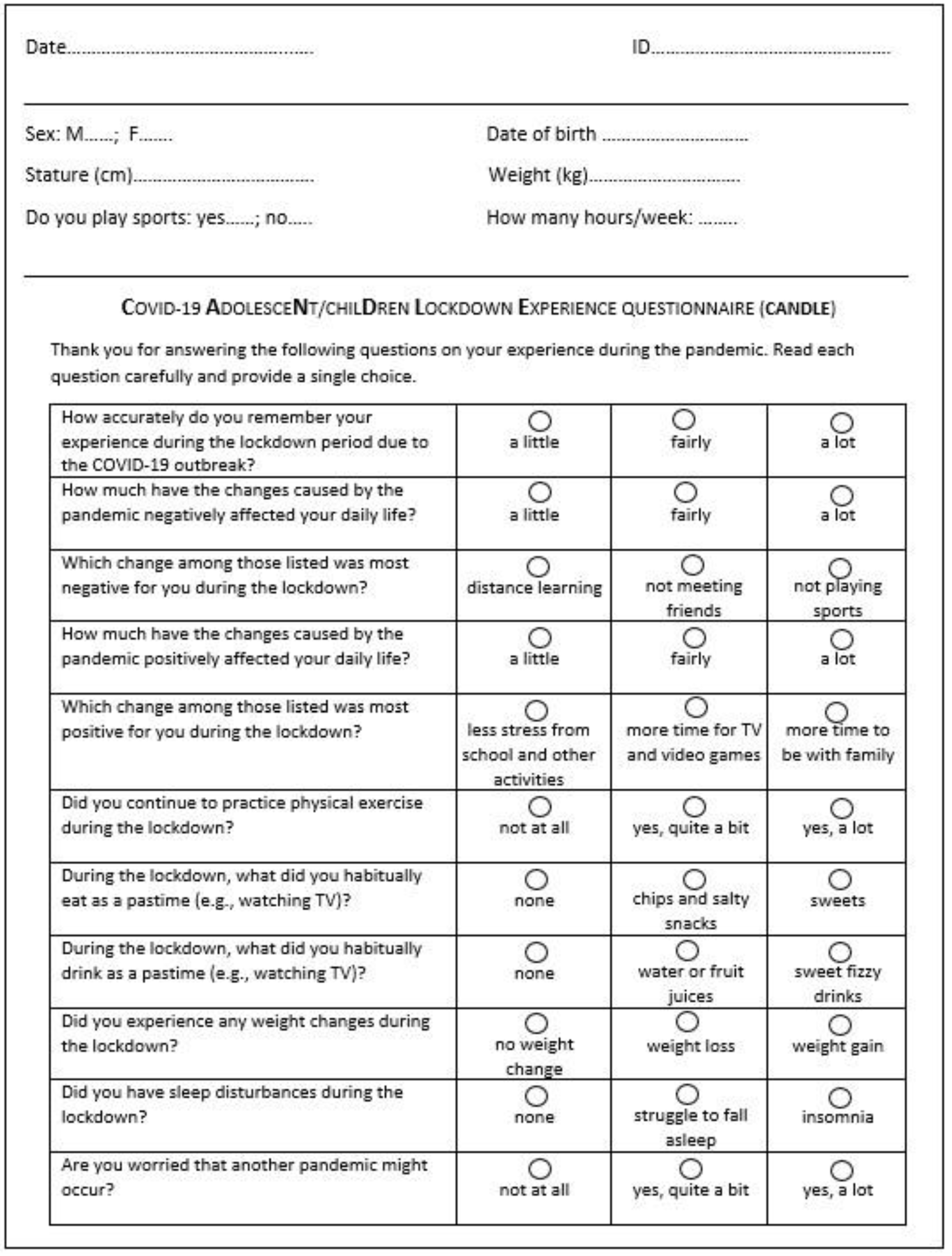
| Question | Answer 1 | Answer 2 | Answer 3 |
|---|---|---|---|
| Q1. How accurately do you remember your experience during the lockdown period due to the COVID-19 outbreak? | a little | fairly | a lot |
| Q2. How much have the changes caused by the pandemic negatively affected your daily life? | a little | fairly | a lot |
| Q3. Which change among those listed was most negative for you during the lockdown? | distance learning | not meeting friends | not playing sports |
| Q4. How much have the changes caused by the pandemic positively affected your daily life? | a little | fairly | a lot |
| Q5. Which change among those listed was most positive for you during the lockdown? | less stress from school and other activities | more time for TV and video games | more time to be with family |
| Q6. Did you continue to practice physical exercise during the lockdown? | not at all | yes, quite a bit | yes, a lot |
| Q7. During the lockdown, what did you habitually eat as a pastime (e.g., watching TV)? | none | chips and salty snacks | sweets |
| Q8. During the lockdown, what did you habitually drink as a pastime (e.g., watching TV)? | none | water or fruit juices | sweet fizzy drinks |
| Q9. Did you experience any weight change during the lockdown? | no weight change | weight loss | weight gain |
| Q10. Did you have sleep disturbances during the lockdown? | none | struggle to fall asleep | insomnia |
| Q11. Are you worried that another pandemic might occur? | not at all | yes, quite a bit | yes, a lot |
| Question | Correlation Value | p-Value |
|---|---|---|
| Q1 | 0.884 | <0.001 |
| Q2 | 0.695 | <0.001 |
| Q3 | 0.821 | <0.001 |
| Q4 | 0.738 | <0.001 |
| Q5 | 0.800 | <0.001 |
| Q6 | 0.646 | 0.001 |
| Q7 | 0.856 | <0.001 |
| Q8 | 0.536 | 0.010 |
| Q9 | 0.965 | <0.001 |
| Q10 | 0.659 | <0.001 |
| Q11 | 0.766 | <0.001 |
| Variable | Overall n = 233 | Boys n = 143 | Girls n = 90 | p-Value |
|---|---|---|---|---|
| Age (years) | 12.4 (0.9) | 12.4 (0.9) | 12.3 (0.8) | 0.2268 a |
| Weight (kg) | 48.8 (11.5) | 48.7 (12.1) | 49.0 (10.5) | 0.8317 a |
| Stature (cm) | 155.3 (9.1) | 155.6 (10.1) | 154.9 (7.3) | 0.5799 a |
| BMI (kg/m2) | 20.1 (3.6) | 19.9 (3.6) | 20.3 (3.6) | 0.4050 a |
| Sports practice (%) | 67.8 | 72.7 | 60.0 | 0.0429 a |
| Amount of sports practice (h/week) | 4.3 (2.7) | 4.5 (2.5) | 3.8 (3.2) | 0.1139 a |
| Weight status: | 0.8834 b | |||
| Underweight | 13 (5.6%) | 8 (5.6%) | 5 (5.6%) | |
| Normal weight | 155 (66.5%) | 96 (67.1%) | 59 (65.6%) | |
| Overweight | 52 (22.3%) | 30 (21.0%) | 22 (24.4%) | |
| Obese | 13 (5.6%) | 9 (6.3%) | 4 (4.4%) |
| Question | Overall (n = 233) | Boys (n = 143) | Girls (n = 90) | p-Value b | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| A1 | A2 | A3 | A1 | A2 | A3 | A1 | A2 | A3 | ||
| Q1. How accurately do you remember your experience during the lockdown period due to the COVID-19 outbreak? | 19.4 | 52.6 | 28.0 | 17.6 | 54.2 | 28.2 | 22.2 | 50.0 | 27.8 | 0.6719 |
| Q2. How much have the changes caused by the pandemic negatively affected your daily life? | 57.3 | 37.9 | 4.7 | 61.3 | 35.9 | 2.8 | 51.1 | 41.1 | 7.8 | 0.1199 |
| Q3. Which change among those listed was most negative for you during the lockdown? | 17.4 | 48.7 | 33.9 | 15.0 | 45.7 | 39.3 | 21.1 | 53.3 | 25.6 | 0.0874 |
| Q4. How much have the changes caused by the pandemic positively affected your daily life? | 53.0 | 38.8 | 8.2 | 52.8 | 38.7 | 8.5 | 53.3 | 38.9 | 7.8 | 0.9834 |
| Q5. Which change among those listed was most positive for you during the lockdown? | 37.5 | 16.4 | 46.1 | 39.9 | 16.8 | 43.4 | 33.3 | 15.7 | 50.0 | 0.5465 |
| Q6. Did you continue to practice physical exercise during the lockdown? | 33.2 | 48.7 | 18.1 | 30.3 | 46.5 | 23.2 | 37.8 | 52.2 | 10.0 | 0.0362 |
| Q7. During the lockdown, what did you habitually eat as a pastime (e.g., watching TV)? | 37.7 | 52.8 | 9.5 | 41.5 | 52.8 | 5.6 | 31.5 | 52.8 | 15.7 | 0.0255 |
| Q8. During the lockdown, what did you habitually drink as a pastime (e.g., watching TV)? | 10.0 | 76.6 | 13.4 | 9.9 | 74.5 | 15.6 | 10.0 | 80.0 | 10.0 | 0.4713 |
| Q9. Did you experience any weight change during the lockdown? | 49.1 | 18.5 | 32.3 | 49.0 | 17.5 | 33.6 | 49.4 | 20.2 | 30.3 | 0.8178 |
| Q10. Did you have sleep disturbances during the lockdown? | 73.8 | 19.3 | 6.9 | 76.2 | 18.9 | 4.9 | 70.0 | 20.0 | 10.0 | 0.2979 |
| Q11. Are you worried that another pandemic might occur? | 41.6 | 46.6 | 11.8 | 51.5 | 39.0 | 9.6 | 25.9 | 58.8 | 15.3 | 0.0009 |
| Variables | Boys | Girls | ||||
|---|---|---|---|---|---|---|
| β | p-Value | VIF | β | p-Value | VIF | |
| Q7 (no eating as a pastime) | −0.1790 | 0.0415 | 1.0000 | |||
| Q10 (no sleep problems) | −0.3610 | 0.0025 | 1.3156 | |||
| Amount of sports practice (h/week) | −0.2446 | 0.0420 | 1.3848 | |||
| R2 | 0.0321 | 0.3468 | ||||
| R2 adjusted | 0.0245 | 0.1860 | ||||
| p-value | 0.0415 | 0.0156 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaccagni, L.; De Luca, F.; Rinaldo, N.; Mazzoni, G.; Mandini, S.; Gualdi-Russo, E. The COVID-19 Experience in Adolescents: Emotional and Behavioral Recall at the End of the Pandemic. Diseases 2024, 12, 116. https://doi.org/10.3390/diseases12060116
Zaccagni L, De Luca F, Rinaldo N, Mazzoni G, Mandini S, Gualdi-Russo E. The COVID-19 Experience in Adolescents: Emotional and Behavioral Recall at the End of the Pandemic. Diseases. 2024; 12(6):116. https://doi.org/10.3390/diseases12060116
Chicago/Turabian StyleZaccagni, Luciana, Federica De Luca, Natascia Rinaldo, Gianni Mazzoni, Simona Mandini, and Emanuela Gualdi-Russo. 2024. "The COVID-19 Experience in Adolescents: Emotional and Behavioral Recall at the End of the Pandemic" Diseases 12, no. 6: 116. https://doi.org/10.3390/diseases12060116
APA StyleZaccagni, L., De Luca, F., Rinaldo, N., Mazzoni, G., Mandini, S., & Gualdi-Russo, E. (2024). The COVID-19 Experience in Adolescents: Emotional and Behavioral Recall at the End of the Pandemic. Diseases, 12(6), 116. https://doi.org/10.3390/diseases12060116