
SARS-CoV-2 Infection Is an Independent Risk Factor for Decompensation in Cirrhosis Patients

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Inclusion and Exclusion Criteria
3. Results
3.1. Baseline Characterestics
3.2. Outcomes
4. Discussion
4.1. Cirrhosis and Immune Dysfunction
4.2. Mechanism of SARS-CoV-2-Induced Liver Injury
4.3. SARS-CoV-2 Drug-Induced Liver Injury
4.4. SARS-CoV-2 and Underlying Liver Disease
4.5. Decompensation of Cirrhosis
4.6. Prognosis of SARS-CoV-2 in Patients with Cirrhosis
4.7. Strengths and Weaknesses
4.8. Summary
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kapuria, D.; Gangu, K.; Chourasia, P.; Boba, A.; Nguyen, A.; Ryu, M.; Peicher, M.; Flores, M.; Chela, H.K.; Daglilar, E.S.; et al. COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database. Trop. Med. Infect. Dis. 2022, 7, 421. [Google Scholar] [CrossRef]
- Chela, H.K.; Tallon, E.M.; Baskett, W.; Gangu, K.; Tahan, V.; Shyu, C.R.; Daglilar, E. Liver injury on admission linked to worse outcomes in COVID-19: An analysis of 14,138 patients. Transl. Gastroenterol. Hepatol. 2023, 8, 4. [Google Scholar] [CrossRef] [PubMed]
- Noor, M.T.; Manoria, P. Immune Dysfunction in Cirrhosis. J. Clin. Transl. Hepatol. 2017, 5, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Sipeki, N.; Antal-Szalmas, P.; Lakatos, P.L.; Papp, M. Immune dysfunction in cirrhosis. World J. Gastroenterol. 2014, 20, 2564–2577. [Google Scholar] [CrossRef] [PubMed]
- Holdstock, G.; Leslie, B.; Hill, S.; Tanner, A.R.; Wright, R. Monocyte function in cirrhosis. J. Clin. Pathol. 1982, 35, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Antoniades, C.G.; Wendon, J.; Vergani, D. Paralysed monocytes in acute on chronic liver disease. J. Hepatol. 2005, 42, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, V.; Mookerjee, R.P.; Wright, G.A.; Davies, N.A.; Jürgens, G.; Hallström, S.; Jalan, R. Role of Toll-like receptors 2, 4 and 9 in mediating neutrophil dysfunction in alcoholic hepatitis. Am. J. Physiol. Liver Physiol. 2009, 296, G15–G22. [Google Scholar] [CrossRef]
- Dousari, A.S.; Hosseininasab, S.S.; Dousari, F.S.; Fuladvandi, M.; Satarzadeh, N. The impact of COVID-19 on liver injury in various age. World J. Virol. 2023, 12, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Márquez, M.; Fernández-Gutiérrez, C.; Montes-de-Oca, M.; Blanco, M.J.; Brun, F.; Rodríguez-Ramos, C.; Girón-González, J.A. Chronic antigenic stimuli as a possible explanation for the immunodepression caused by liver cirrhosis. Clin. Exp. Immunol. 2009, 158, 219–229. [Google Scholar] [CrossRef]
- Van de Wiel, A.; Schuurman, H.J.; Kater, L. Alcoholic liver disease: An IgA-associated disorder. Scand. J. Gastroenterol. 1987, 22, 1025–1030. [Google Scholar] [CrossRef]
- Serum Bactericidal and Opsonic Activities in Patients with Non-Alcoholic Cirrhosis—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/3901076/ (accessed on 3 February 2024).
- Garcia-Tsao, G.; Wiest, R. Gut microflora in the pathogenesis of the complications of cirrhosis. Best Pract. Res. Clin. Gastroenterol. 2004, 18, 353–372. [Google Scholar] [CrossRef]
- Wiest, R.; Garcia-Tsao, G. Bacterial translocation (BT) in cirrhosis. Hepatology 2005, 41, 422–433. [Google Scholar] [CrossRef]
- Aldersley, M.A.; Howdle, P.D. Intestinal permeability and liver disease. Eur. J. Gastroenterol. Hepatol. 1999, 11, 401–404. [Google Scholar] [CrossRef]
- Hunt, R.H.; East, J.E.; Lanas, A.; Malfertheiner, P.; Satsangi, J.; Scarpignato, C.; Webb, G.J. COVID-19 and Gastrointestinal Disease: Implications for the Gastroenterologist. Dig. Dis. 2021, 39, 119–139. [Google Scholar] [CrossRef]
- Choudhary, N.S.; Dhampalwar, S.; Saraf, N.; Soin, A.S. Outcomes of COVID-19 in Patients with Cirrhosis or Liver Transplantation. J. Clin. Exp. Hepatol. 2021, 11, 713–719. [Google Scholar] [CrossRef]
- Iavarone, M.; D’Ambrosio, R.; Soria, A.; Triolo, M.; Pugliese, N.; Del Poggio, P.; Perricone, G.; Massironi, S.; Spinetti, A.; Buscarini, E.; et al. High rates of 30-day mortality in patients with cirrhosis and COVID-19. J. Hepatol. 2020, 73, 1063–1071. [Google Scholar] [CrossRef]
- Boettler, T.; Newsome, P.N.; Mondelli, M.U.; Maticic, M.; Cordero, E.; Cornberg, M.; Berg, T. Care of patients with liver disease during the COVID-19 pandemic: EASL-ESCMID position paper. JHEP Rep. 2020, 2, 100113. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S., 4th; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Dufour, J.F.; Marjot, T.; Becchetti, C.; Tilg, H. COVID-19 and liver disease. Gut 2022, 71, 2350–2362. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Prichett, L.; Tao, X.; Alqahtani, S.A.; Hamilton, J.P.; Mezey, E.; Strauss, A.T.; Kim, A.; Potter, J.J.; Chen, P.H.; et al. Abnormal liver chemistries as a predictor of COVID-19 severity and clinical outcomes in hospitalized patients. World J. Gastroenterol. 2022, 28, 570–587. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Lozano-Sepulveda, S.A.; Galan-Huerta, K.; Martínez-Acuña, N.; Arellanos-Soto, D.; Rivas-Estilla, A.M. SARS-CoV-2 another kind of liver aggressor, how does it do that? Ann. Hepatol. 2020, 19, 592–596. [Google Scholar] [CrossRef]
- Nardo, A.D.; Schneeweiss-Gleixner, M.; Bakail, M.; Dixon, E.D.; Lax, S.F.; Trauner, M. Pathophysiological mechanisms of liver injury in COVID-19. Liver Int. 2021, 41, 20–32. [Google Scholar] [CrossRef]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 Expression in Pancreas May Cause Pancreatic Damage after SARS-CoV-2 Infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef]
- Ozkurt, Z.; Tanrıverdi, E.Ç. COVID-19: Gastrointestinal manifestations, liver injury and recommendations. World J. Clin. Cases 2022, 10, 1140–1163. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Cai, Y.; Ye, L.P.; Song, Y.Q.; Mao, X.L.; Wang, L.; Jiang, Y.Z.; Que, W.T.; Li, S.W. Liver injury in COVID-19: Detection, pathogenesis, and treatment. World J. Gastroenterol. 2021, 27, 3022–3036. [Google Scholar] [CrossRef]
- Spiezia, L.; Boscolo, A.; Poletto, F.; Cerruti, L.; Tiberio, I.; Campello, E.; Navalesi, P.; Simioni, P. COVID-19-Related Severe Hypercoagulability in Patients Admitted to Intensive Care Unit for Acute Respiratory Failure. Thromb. Haemost. 2020, 120, 998–1000. [Google Scholar] [CrossRef]
- Rampotas, A.; Pavord, S. Platelet aggregates, a marker of severe COVID-19 disease. J. Clin. Pathol. 2021, 74, 750–751. [Google Scholar] [CrossRef]
- El-Hady, H.A.; Mahmoud Abd-Elwahab, E.S.; Mostafa-Hedeab, G.; Elfarargy, M.S. Portal vein thrombosis in patients with COVID-19: A systematic review. Asian J. Surg. 2023, 46, 3017–3026. [Google Scholar] [CrossRef] [PubMed]
- Samant, H.; Asafo-Agyei, K.O.; Garfield, K. Portal Vein Thrombosis; Springer Nature: Berlin, Germany, 2022; pp. 1–171. [Google Scholar] [CrossRef]
- García, L.F. Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Front. Immunol. 2020, 11, 1441. [Google Scholar] [CrossRef]
- Costela-Ruiz, V.J.; Illescas-Montes, R.; Puerta-Puerta, J.M.; Ruiz, C.; Melguizo-Rodríguez, L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020, 54, 62–75. [Google Scholar] [CrossRef]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56e1. [Google Scholar] [CrossRef]
- Portincasa, P.; Krawczyk, M.; Machill, A.; Lammert, F.; Di Ciaula, A. Hepatic consequences of COVID-19 infection. Lapping or biting? Eur. J. Intern. Med. 2020, 77, 18–24. [Google Scholar] [CrossRef]
- Zhai, G.; Li, M.; Wang, Y.; Wu, J. Drug-Induced Liver Disturbance During the Treatment of COVID-19. Front. Pharmacol. 2021, 12, 719308. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Kumar, P.; Tevethia, H.V.; Premkumar, M.; Arab, J.P.; Candia, R.; Talukdar, R.; Sharma, M.; Qi, X.; Rao, P.N.; et al. Systematic review with meta-analysis: Liver manifestations and outcomes in COVID-19. Aliment. Pharmacol. Ther. 2020, 52, 584–599. [Google Scholar] [CrossRef]
- Hasona, N.; Morsi, A. Grape Seed Extract Alleviates Dexamethasone-Induced Hyperlipidemia, Lipid Peroxidation, and Hematological Alteration in Rats. Indian J. Clin. Biochem. 2019, 34, 213–218. [Google Scholar] [CrossRef]
- [Fatal Liver Failure after Corticosteroid Treatment of a Hepatitis B Virus Carrier]—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/10394348/ (accessed on 2 February 2024).
- Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B.; et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Gordon, C.J.; Tchesnokov, E.P.; Woolner, E.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; Götte, M. Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency. J. Biol. Chem. 2020, 295, 6785–6797. [Google Scholar] [CrossRef]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 383, 1827–1837. [Google Scholar] [CrossRef]
- Hundt, M.A.; Deng, Y.; Ciarleglio, M.M.; Nathanson, M.H.; Lim, J.K. Abnormal Liver Tests in COVID-19: A Retrospective Observational Cohort Study of 1827 Patients in a Major U.S. Hospital Network. Hepatology 2020, 72, 1169–1176. [Google Scholar] [CrossRef]
- Van Laar, S.A.; de Boer, M.G.J.; Gombert-Handoko, K.B.; Guchelaar, H.; Zwaveling, J. Liver and kidney function in patients with Covid-19 treated with remdesivir. Br. J. Clin. Pharmacol. 2021, 87, 4450–4454. [Google Scholar] [CrossRef]
- COVID-19 Treatments and Medications|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/treatments-for-severe-illness.html (accessed on 23 January 2024).
- “Ritonavir”, LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2017. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548301/ (accessed on 2 February 2024).
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- “Imatinib”, LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK547959/ (accessed on 2 February 2024).
- Tonyali, O.; Coskun, U.; Yildiz, R.; Karakan, T.; Demirci, U.; Akyurek, N.; Benekli, M.; Buyukberber, S. Imatinib mesylate-induced acute liver failure in a patient with gastrointestinal stromal tumors. Med. Oncol. 2010, 27, 768–773. [Google Scholar] [CrossRef]
- Ridruejo, E.; Cacchione, R.; Villamil, A.G.; Marciano, S.; Gadano, A.C.; Mandó, O.G. Imatinib-induced fatal acute liver failure. World J. Gastroenterol. 2007, 13, 6608–6611. [Google Scholar] [CrossRef]
- “Baricitinib”, LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548012/ (accessed on 2 February 2024).
- Dougados, M.; van der Heijde, D.; Chen, Y.C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; de la Torre, I.; Gaich, C.; et al. Extended report: Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: Results from the RA-BUILD study. Ann. Rheum. Dis. 2017, 76, 88–95. [Google Scholar] [CrossRef]
- Bacharier, L.B.; Guilbert, T.W.; Mauger, D.T.; Boehmer, S.; Beigelman, A.; Fitzpatrick, A.M.; Jackson, D.J.; Baxi, S.N.; Benson, M.; Burnham, C.D.; et al. Early Administration of Azithromycin and Prevention of Severe Lower Respiratory Tract Illnesses in Preschool Children with a History of Such Illnesses: A Randomized Clinical Trial. JAMA 2015, 314, 2034–2044. [Google Scholar] [CrossRef]
- Wahab, S.; Ahmad, M.F.; Hussain, A.; Usmani, S.; Shoaib, A.; Ahmad, W. Effectiveness of Azithromycin as Add-on Therapy in COVID-19 Management. Mini Rev. Med. Chem. 2021, 21, 2860–2873. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Alexopoulos, H.; Politou, M.; Paraskevis, D.; Scorilas, A.; Kastritis, E.; Andreakos, E.; Dimopoulos, M.A. Adverse effects of COVID-19 mRNA vaccines: The spike hypothesis. Trends Mol. Med. 2022, 28, 542–554. [Google Scholar] [CrossRef]
- Cascaval, R.I.; Lancaster, D.J. Hypersensitivity syndrome associated with azithromycin. Am. J. Med. 2001, 110, 330–331. [Google Scholar] [CrossRef]
- “Azithromycin”, LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548434/ (accessed on 2 February 2024).
- Azithromycin-Induced Intrahepatic Cholestasis—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/9217574/ (accessed on 2 February 2024).
- Ellison, C.A.; Blackwell, S.B. Acute Hepatocellular Injury Associated With Azithromycin. J. Pharm. Pr. 2021, 34, 493–496. [Google Scholar] [CrossRef]
- National Instite of Diabetes en Digestive and Kidney Diseases. “Acetaminophen”, LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548162/ (accessed on 23 January 2024).
- Mantovani, A.; Beatrice, G.; Dalbeni, A. Coronavirus disease 2019 and prevalence of chronic liver disease: A meta-analysis. Liver Int. 2020, 40, 1316–1320. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.M.; Webb, G.J.; Aloman, C.; Armstrong, M.J.; Cargill, T.; Dhanasekaran, R.; Genescà, J.; Gill, U.S.; James, T.W.; Jones, P.D.; et al. High mortality rates for SARS-CoV-2 infection in patients with pre-existing chronic liver disease and cirrhosis: Preliminary results from an international registry. J. Hepatol. 2020, 73, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Runyon, B.A. Management of adult patients with ascites due to cirrhosis: An update. Hepatology 2009, 49, 2087–2107. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Parikh, C.R.; Viola, A. Acute kidney injury in cirrhosis. Hepatology 2008, 48, 2064–2077. [Google Scholar] [CrossRef]
- Alleway, R.; Butt, A.; Ellis, D.; Freeth, H.; Jarman, D.; Joy, S.; Majid, W.; Nwosu, E.; Protopapa, K.; Shotton, H. Measuring the Units Measuring the Units A Review of Patients Who Died with Alcohol-Related Liver Disease; National Confidential Enquiry into Patient Outcome and Death: London, UK, 2013. [Google Scholar]
- Tripathi, D.; Stanley, A.J.; Hayes, P.C.; Patch, D.; Millson, C.; Mehrzad, H.; Austin, A.; Ferguson, J.W.; Olliff, S.P.; Hudson, M.; et al. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut 2015, 64, 1680–1704. [Google Scholar] [CrossRef] [PubMed]
- Acute Upper Gastrointestinal Bleeding in Over 16 s: Management. 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554919/ (accessed on 2 February 2024).
- Leise, M.D.; Poterucha, J.J.; Kamath, P.S.; Kim, W.R. Management of Hepatic Encephalopathy in the Hospital. Mayo Clin. Proc. 2014, 89, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. OpenSAFELY: Factors associated with COVID-19 death in 17 million patients. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.W.; Wu, X.X.; Jiang, X.G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Li, S.B.; Wang, H.Y.; Zhang, S.; Gao, H.N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-CoV-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m606. [Google Scholar] [CrossRef]
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Non-alcoholic fatty liver diseases in patients with COVID-19: A retrospective study. J. Hepatol. 2020, 73, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Tarar, Z.I.; Farooq, U.; Saleem, S.; Chela, H.K.; Daglilar, E. The COVID-19 Infection Resulted Delayed Esophagogastroduodenoscopy in Patients Admitted with Variceal Bleeding: Hospital-Based Outcomes of a National Database. Diseases 2023, 11, 75. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SARS-CoV-2-Positive and SARS-CoV-2-Negative counts before and after propensity score matching | ||||||
| Cohort | Patient count before PSM matching | Patient count after PSM matching | ||||
| SARS-CoV-2-Positive | 8367 | 5092 | ||||
| SARS-CoV-2-Negative | 8150 | 5092 | ||||
| Propensity score density function—before and after matching (SARS-CoV-2-positive—purple, SARS-CoV-2-negative—green) | ||||||
 |  | |||||
| Before PSM | After PSM | |||||
| SARS-CoV-2-Positive (n = 69,057) | SARS-CoV-2-Negative (n = 183,574) | p-value | SARS-CoV-2-Positive (n = 61,963) | SARS-CoV-2-Negative (n = 61,963) | p-value | |
| Demographics | ||||||
| 54.3 ± 11.2 | 51.4 ± 11.1 | <0.001 | 53.6 ± 11.4 | 53.2 ± 11 | 0.08 |
| 43.9% | 40.6% | <0.001 | 43.3% | 43.7% | 0.14 |
| 73.5% | 51.5% | <0.001 | 71.7% | 70.3% | 0.07 |
| Comorbidities | ||||||
| 14.5% | 4.9% | <0.001 | 10.4% | 10.6% | 0.33 |
| 15.7% | 4.8% | <0.001 | 11.1% | 11.2% | 0.54 |
| 14.3% | 4.7% | <0.001 | 10.2% | 10.3% | 0.41 |
| 55.7% | 24.5% | <0.001 | 50.7% | 51.8% | 0.09 |
| 33.8% | 15.1% | <0.001 | 29.2% | 30.6% | 0.1 |
| Outcomes at 1 Month | Outcomes at 3 Months | |||||||
|---|---|---|---|---|---|---|---|---|
| SARS-CoV-2-Positive (61,963) | SARS-CoV-2-Negative (61,963) | OR | p-Value | SARS-CoV-2-Positive (61,963) | SARS-CoV-2-Negative (61,963) | OR | p-Value | |
| Decompensation | 4.4% | 1.9% | 2.4 | <0.0001 | 6% | 2.6% | 2.4 | <0.0001 |
| Jaundice | 0.7% | 0.6% | 1.1 | 0.08 | 0.9% | 0.8% | 1.1 | 0.03 |
| Ascites | 2.6% | 0.4% | 6 | <0.0001 | 3.5% | 0.7% | 5.4 | <0.0001 |
| SBP | 0.1% | 0.02% | 4.7 | <0.0001 | 0.17% | 0.03% | 5 | <0.0001 |
| HE | 1.9% | 0.9% | 2.2 | <0.0001 | 2.5% | 1.2% | 2.2 | <0.0001 |
| HRS | 0.2% | 0.05% | 4.3 | <0.0001 | 0.27% | 0.07% | 4 | <0.0001 |
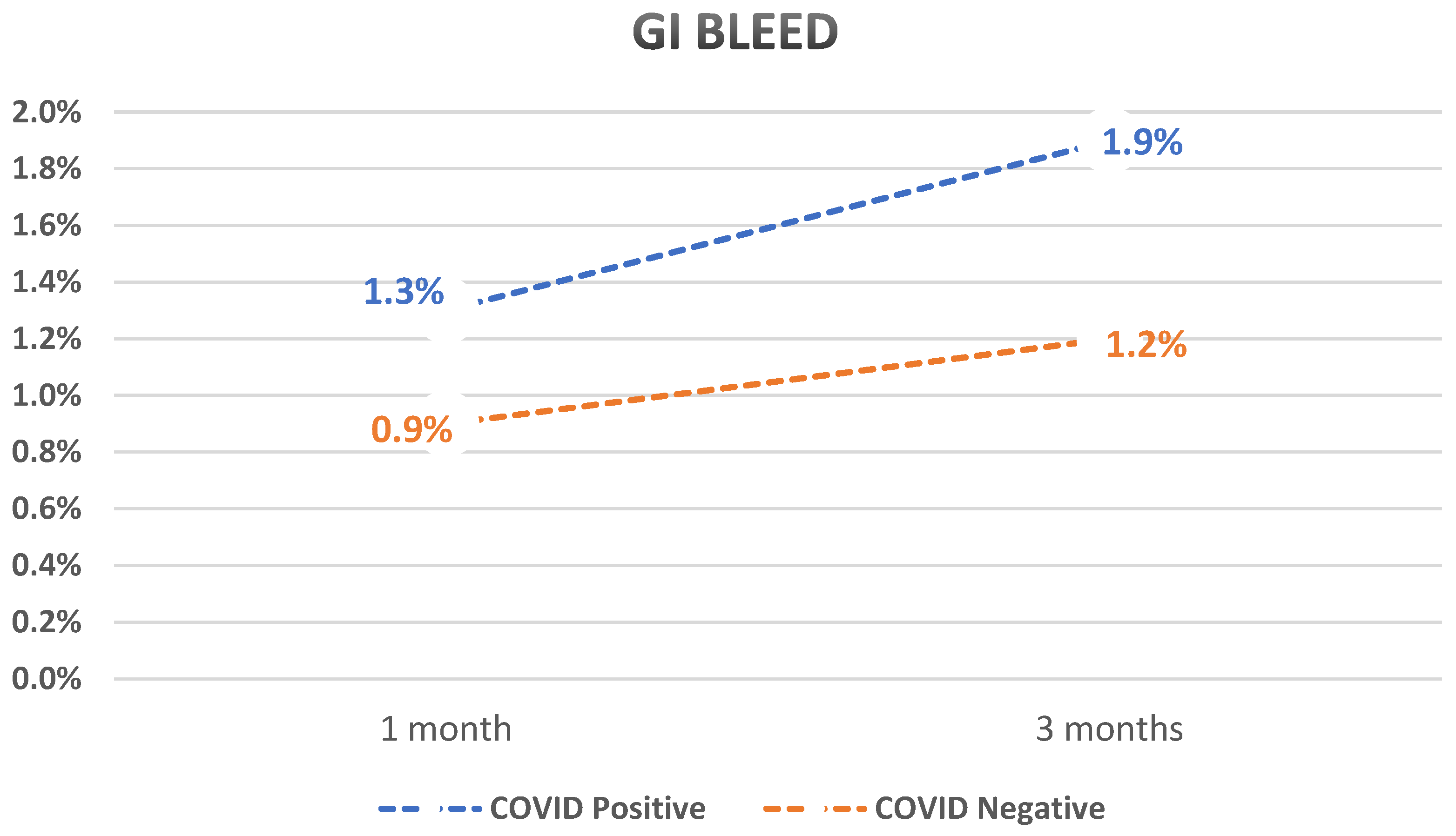
| GI bleed | 1.3% | 0.9% | 1.5 | <0.0001 | 1.9% | 1.2% | 1.6 | <0.0001 |
| Mortality | 2.5% | 1.7% | 1.5 | <0.0001 | 3.6% | 2.7% | 1.3 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayoub, M.; Tomanguillo, J.; Faris, C.; Anwar, N.; Chela, H.; Daglilar, E. SARS-CoV-2 Infection Is an Independent Risk Factor for Decompensation in Cirrhosis Patients. Diseases 2024, 12, 46. https://doi.org/10.3390/diseases12030046
Ayoub M, Tomanguillo J, Faris C, Anwar N, Chela H, Daglilar E. SARS-CoV-2 Infection Is an Independent Risk Factor for Decompensation in Cirrhosis Patients. Diseases. 2024; 12(3):46. https://doi.org/10.3390/diseases12030046
Chicago/Turabian StyleAyoub, Mark, Julton Tomanguillo, Carol Faris, Nadeem Anwar, Harleen Chela, and Ebubekir Daglilar. 2024. "SARS-CoV-2 Infection Is an Independent Risk Factor for Decompensation in Cirrhosis Patients" Diseases 12, no. 3: 46. https://doi.org/10.3390/diseases12030046
APA StyleAyoub, M., Tomanguillo, J., Faris, C., Anwar, N., Chela, H., & Daglilar, E. (2024). SARS-CoV-2 Infection Is an Independent Risk Factor for Decompensation in Cirrhosis Patients. Diseases, 12(3), 46. https://doi.org/10.3390/diseases12030046