
Association between COVID-19 Infection and Miscarriages, What We Really Know?

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Miscarriage Rates and COVID-19 Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, R.; Yin, T.; Fang, F.; Li, Q.; Chen, J.; Wang, Y.; Hao, Y.; Wu, G.; Duan, P.; Wang, Y.; et al. Potential risks of SARS-CoV-2 infection on reproductive health. Reprod. Biomed. Online 2020, 41, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Sharma, I.; Kumari, P.; Sharma, A.; Saha, S.C. SARS-CoV-2 and the reproductive system: Known and the unknown!! Middle East Fertil. Soc. J. 2021, 26, 1. [Google Scholar] [CrossRef]
- Kanmaz, A.G.; Inan, A.H.; Beyan, E.; Budak, A. The effects of threatened abortions on pregnancy outcomes. Ginekol. Pol. 2019, 90, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Zinaman, M.J.; Clegg, E.D.; Brown, C.C.; O’Connor, J.; Selevan, S.G. Estimates of human fertility and pregnancy loss. Fertil. Steril. 1996, 65, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, A.J.; Weinberg, C.R.; O’Connor, J.F.; Baird, D.D.; Schlatterer, J.P.; Canfield, R.E.; Armstrong, E.G.; Nisula, B.C. Incidence of early loss of pregnancy. N. Engl. J. Med. 1988, 319, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Hajialiakbari, N.; Schwartz, D.; Javaheri, A.; Karimi-Zarchi, M.; Golshan-Tafti, M.; Dastgheib, S.A.; Bahrami, R.; Zanbagh, L.; Neamatzadeh, H. A Meta-Analysis for Frequency of Miscarriage in Pregnant Women with COVID-19. World J. Peri Neonatol. 2022, 4, 104–114. [Google Scholar] [CrossRef]
- Cavalcante, M.B.; de Melo Bezerra Cavalcante, C.T.; Cavalcante, A.N.M.; Sarno, M.; Barini, R.; Kwak-Kim, J. COVID-19 and miscarriage: From immunopathological mechanisms to actual clinical evidence. J. Reprod. Immunol. 2021, 148, 103382. [Google Scholar] [CrossRef]
- Batiha, O.; Al-Deeb, T.; Al-Zoubi, E.; Alsharu, E. Impact of COVID-19 and other viruses on reproductive health. Andrologia 2020, 52, e13791. [Google Scholar] [CrossRef]
- Liu, C.; Mu, C.; Zhang, Q.; Yang, X.; Yan, H.; Jiao, H. Effects of Infection with SARS-CoV-2 on the Male and Female Reproductive Systems: A Review. Med. Sci. Monit. 2021, 27, e930168. [Google Scholar] [CrossRef]
- Lee, W.Y.; Mok, A.; Chung, J.P.W. Potential effects of COVID-19 on reproductive systems and fertility; assisted reproductive technology guidelines and considerations: A review. Hong Kong Med. J. 2021, 27, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Carneiro Gomes, P.R.; Rodrigues da Rocha, M.D.; da Rocha Coelho, F.A.; Sousa Pinho de Lira, J.A.; de Sousa Carmo, R.R.; Silva Nascimento, H.M.; Marques de Oliveira, S.; Rodrigues da Silva, W.; Galdino Medeiros, R.; Pereira Alves, E.H.; et al. Alterations of the male and female reproductive systems induced by COVID-19. Wien. Klin. Wochenschr. 2021, 133, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Cornish, E.F.; McDonnell, T.; Williams, D.J. Chronic Inflammatory Placental Disorders Associated With Recurrent Adverse Pregnancy Outcome. Front. Immunol. 2022, 13, 825075. [Google Scholar] [CrossRef] [PubMed]
- Litman, E.A.; Yin, Y.; Nelson, S.J.; Capbarat, E.; Kerchner, D.; Ahmadzia, H.K. Adverse perinatal outcomes in a large United States birth cohort during the COVID-19 pandemic. Am. J. Obstet. Gynecol. MFM 2022, 4, 100577. [Google Scholar] [CrossRef]
- Aho Glele, L.S.; Simon, E.; Bouit, C.; Serrand, M.; Filipuzzi, L.; Astruc, K.; Kadhel, P.; Sagot, P. Association between SARS-CoV-2 infection during pregnancy and adverse pregnancy outcomes: A re-analysis of the data reported by Wei et al. (2021). Infect. Dis. Now 2022, 52, 123–128. [Google Scholar] [CrossRef]
- Kazemi, S.N.; Hajikhani, B.; Didar, H.; Hosseini, S.S.; Haddadi, S.; Khalili, F.; Mirsaeidi, M.; Nasiri, M.J. COVID-19 and cause of pregnancy loss during the pandemic: A systematic review. PLoS ONE 2021, 16, e0255994. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women With and Without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef] [PubMed]
- La Cour Freiesleben, N.; Egerup, P.; Hviid, K.V.R.; Severinsen, E.R.; Kolte, A.M.; Westergaard, D.; Fich Olsen, L.; Praetorius, L.; Zedeler, A.; Christiansen, A.H.; et al. SARS-CoV-2 in first trimester pregnancy: A cohort study. Hum. Reprod. 2021, 36, 40–47. [Google Scholar] [CrossRef]
- Rotshenker-Olshinka, K.; Volodarsky-Perel, A.; Steiner, N.; Rubenfeld, E.; Dahan, M.H. COVID-19 pandemic effect on early pregnancy: Are miscarriage rates altered, in asymptomatic women? Arch. Gynecol. Obstet. 2021, 303, 839–845. [Google Scholar] [CrossRef]
- Alberca, R.W.; Pereira, N.Z.; Oliveira, L.; Gozzi-Silva, S.C.; Sato, M.N. Pregnancy, Viral Infection, and COVID-19. Front. Immunol. 2020, 11, 1672. [Google Scholar] [CrossRef]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E.; Pomar, L. Second-Trimester Miscarriage in a Pregnant Woman With SARS-CoV-2 Infection. JAMA 2020, 323, 2198–2200. [Google Scholar] [CrossRef]
- Shanes, E.D.; Mithal, L.B.; Otero, S.; Azad, H.A.; Miller, E.S.; Goldstein, J.A. Placental Pathology in COVID-19. Am. J. Clin. Pathol. 2020, 154, 23–32. [Google Scholar] [CrossRef]
- Weiner, E.; Feldstein, O.; Tamayev, L.; Grinstein, E.; Barber, E.; Bar, J.; Schreiber, L.; Kovo, M. Placental histopathological lesions in correlation with neonatal outcome in preeclampsia with and without severe features. Pregnancy Hypertens. 2018, 12, 6–10. [Google Scholar] [CrossRef]
- Khosa, F.; Naeem, M.; Sultan, Z.; Rizwan, A.S.; Sher, S.J.; Ali, N. Impacts of COVID-19 Pandemic on the Early Trimester Pregnancies. Pak. J. Med. Health Sci. 2021, 15, 2508–2511. [Google Scholar] [CrossRef]
- Balachandren, N.; Davies, M.C.; Hall, J.A.; Stephenson, J.M.; David, A.L.; Barrett, G.; O’Neill, H.C.; Ploubidis, G.B.; Yasmin, E.; Mavrelos, D. SARS-CoV-2 infection in the first trimester and the risk of early miscarriage: A UK population-based prospective cohort study of 3041 pregnancies conceived during the pandemic. Hum. Reprod. 2022, 37, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, B.H.; Bandarian, F.; Bandarian, M. Maternal and neonatal outcomes of pregnancies of infertile women during the COVID-19 pandemic: A real world evidence. JBRA Assist. Reprod. 2022, 26, 594–598. [Google Scholar] [CrossRef]
- Arican, C.D. The Relationship between the COVID-19 Pandemic and Early Pregnancy Abortions. Eur. J. Med. Health Sci. 2022, 4, 84–86. [Google Scholar] [CrossRef]
- Afrooz, N.; Mahmoudi, S.K.; Yazdizadeh, M.; Jahanshahiafshar, Z.; Sabernia, N.; Rohaninasab, M. The evaluation of COVID-19 effect on pregnancy loss; a molecular and diagnostic approach. Immunopathol. Persa 2022, e30332. [Google Scholar] [CrossRef]
- Bilal, M.Y.; Katara, G.; Dambaeva, S.; Kwak-Kim, J.; Gilman-Sachs, A.; Beaman, K.D. Clinical molecular genetics evaluation in women with reproductive failures. Am. J. Reprod. Immunol. 2021, 85, e13313. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Run-Qian, L.; Hao-Ran, W.; Hao-Ran, C.; Ya-Bin, L.; Yang, G.; Fei, C. Potential influence of COVID-19/ACE2 on the female reproductive system. Mol. Hum. Reprod. 2020, 26, 367–373. [Google Scholar] [CrossRef]
- Muyayalo, K.P.; Huang, D.H.; Zhao, S.J.; Xie, T.; Mor, G.; Liao, A.H. COVID-19 and Treg/Th17 imbalance: Potential relationship to pregnancy outcomes. Am. J. Reprod. Immunol. 2020, 84, e13304. [Google Scholar] [CrossRef] [PubMed]
- Nateghi, R.; Ghashghaei, S.H.; Shokoohian, B.; Hezavehei, M.; Ebrahimi, B.; Shahverdi, A.H.; Mashayekhi, M.; Shpichka, A.; Timashev, P.; Nasr-Esfahani, M.H.; et al. Female Reproductive Health in SARS-CoV-2 Pandemic Era. Int. J. Fertil. Steril. 2021, 15, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Saadedine, M.; El Sabeh, M.; Borahay, M.A.; Daoud, G. The influence of COVID-19 infection-associated immune response on the female reproductive systemdagger. Biol. Reprod. 2023, 108, 172–182. [Google Scholar] [CrossRef] [PubMed]
- Sandulescu, M.S.; Vaduva, C.C.; Siminel, M.A.; Dijmarescu, A.L.; Vrabie, S.C.; Camen, I.V.; Tache, D.E.; Neamtu, S.D.; Nagy, R.D.; Carp-Veliscu, A.; et al. Impact of COVID-19 on fertility and assisted reproductive technology (ART): A systematic review. Rom. J. Morphol. Embryol. 2022, 63, 503–510. [Google Scholar] [CrossRef]
- Sills, E.S.; Wood, S.H. An Experimental Model for Peri-conceptual COVID-19 Pregnancy Loss and Proposed Interventions to Optimize Outcomes. Int. J. Mol. Cell. Med. 2020, 9, 180–187. [Google Scholar] [CrossRef]
- Vesce, F.; Battisti, C.; Crudo, M. The Inflammatory Cytokine Imbalance for Miscarriage, Pregnancy Loss and COVID-19 Pneumonia. Front. Immunol. 2022, 13, 861245. [Google Scholar] [CrossRef]

{kind=link}
| Study | Year | Study Design | Main Outcome |
|---|---|---|---|
| Afrooz N et al. [28] | 2022 | Review | Immune system suppression disrupts the pregnancy process by affecting the profiles of cytokines, coagulation systems (D-dimer), and hormones |
| Aho Glele L.S. et al. [15] | 2022 | Meta-analysis | COVID-19 infection is associated with preterm birth, and may be associated with preeclampsia |
| Alberca R.W. et al. [20] | 2020 | Review | A single case involving a second trimester miscarriage |
| Allotey J et al. [2] | 2020 | Systematic review and meta-analysis/435 studies | Pregnant women with COVID-19 have increased risk for preterm delivery, maternal death, and ICU admission. |
| Arican C.D. et al. [27] | 2022 | Article | Significant vascular changes in the placentas of infected pregnant women |
| Balachandren N. et al. [25] | 2022 | Prospective cohort study/3041 pregnancies | COVID-19 infection in the first trimester may have a higher risk of miscarriage |
| Batiha O. et al. [9] | 2020 | Review | Miscarriages were only reported in SARS infections. Preterm birth, preeclampsia, and caesarean delivery were more common in COVID-19-infected mothers |
| Baud D. et al. [21] | 2020 | Case report | One case of miscarriage during the second trimester of pregnancy related to placental infection |
| Bilal M.Y. et al. [29] | 2021 | Article | Infection by COVID-19 can lead to miscarriage, respiratory distress, and preterm delivery |
| Carneiro Gomes P.R. et al. [12] | 2021 | Review | Infection in the primordial germ cells causes a malfunction of the reproductive glands and a possible alteration in the gametes |
| Cavalcante M.B. et al. [8] | 2021 | Systematic review (17 studies)/meta-analysis (10 studies—223 cases) | Miscarriage rates in pregnant women with COVID-19 were 15.3% (95% CI 10.94–20.59) and 23.1% (95% CI 13.17–34.95) using fixed and random effect models, respectively |
| Cornish E.F. et al. [13] | 2022 | Review | A systematic analysis of placental pathology in 1008 pregnant women with COVID-19 infection found chronic inflammatory pathology (including chronic villitis) in 26% of cases and increased perivillous fibrin in 33% of cases |
| Hajialiakbari N, S.D. et al. [7] | 2022 | Meta-analysis (22 studies/8591 infected pregnant women, 141 abortions) | Miscarriage incidence was 3.9% (95% CI 0.023–0.063) in infected women with COVID-19 |
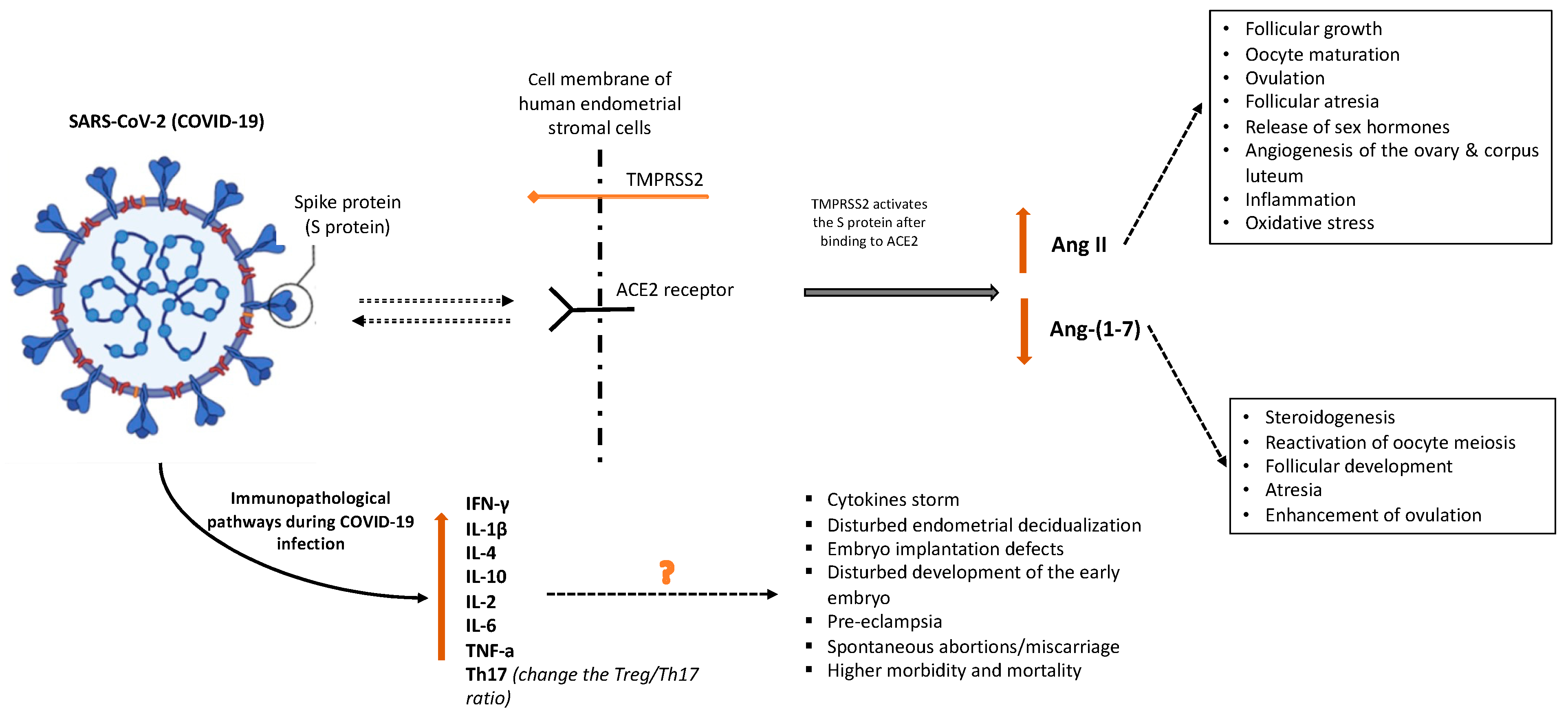
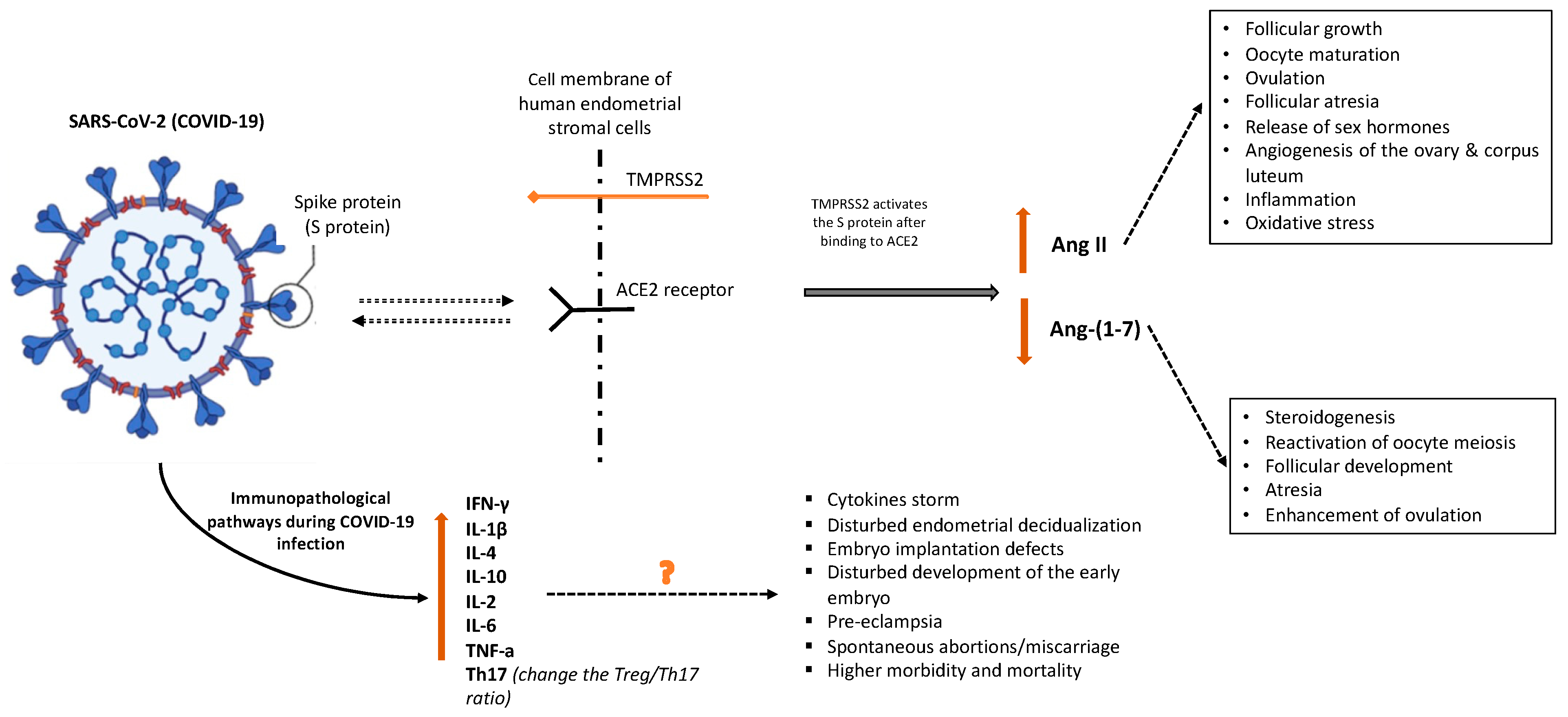
| Jing Y. et al. [30] | 2020 | Review | Pregnancy-related hypertension, preeclampsia, and eclampsia may be associated with the abnormal expression of Ang II, ACE2, and Ang-(1–7) in COVID-19 infection |
| Kazami F.N. et al. [16] | 2021 | Systematic Review | Increased risk of miscarriage in COVID-19-positive women Placental inflammation may result in fetal growth retardation and induce abortion |
| Khosa S.N. et al. [24] | 2021 | Case series/76 women | Of 76 pregnant women, 41 (54%) had a miscarriage with positive COVID-19 tests and 24 (31.6%) had spouses who had COVID-19 positive tests |
| La Cour Freiesleben N. et al. [18] | 2021 | Cohort study/1019 women | Maternal COVID-19 infection in first trimester does not increase the risk of miscarriage |
| Lee W.Y. et al. [11] | 2021 | Review | SARS-CoV-2 infection, via ACE2 receptor, may disrupt ovarian function and oocyte quality |
| Li R. et al. [1] | 2020 | Review | COVID-19 affects the epithelial cell function in the endometrium and interferes with early embryo implantation COVID-19 can affect ovarian tissue potency and granulosa cell function and reduce oocyte quality |
| Litman E.A. et al. [14] | 2022 | Cohort study | There was no significant difference in the prevalence of stillbirths between women with and without COVID-19 (0.6% vs. 0.5%) |
| Liu C. et al. [10] | 2021 | Review | COVID-19 can affect the follicular membrane and granulosa cells of the ovary, reduce the quality of oocytes, and lead to miscarriages |
| Muyayalo K.P. et al. [31] | 2020 | Review | The increased IL-7/IL-7R signaling pathway has been associated with fetal miscarriage |
| Nateghi R. et al. [32] | 2021 | Review of literature | The higher levels of inflammatory cytokines such as TNF-α, IFN-γ, IL-2, and IL-6 in COVID-19 disease may affect early embryo development |
| Rashidi B.H. et al. [26] | 2022 | Case series/38 women | No correlation in neonatal morbidity during pregnancy in pregnancies with COVID-19 infection |
| Rotshenker-Olshinka K. et al. [19] | 2021 | Cohort study/285 women | No correlation in first trimester miscarriages and ongoing pregnancies |
| Saadedine M. et al. [33] | 2023 | Review | A severe COVID-19 infection may raise Th17 cells and change the Treg/Th17 ratio, leading to uncontrolled systemic inflammation that affects pregnancy outcomes |
| Sandulescu M.S. et al. [34] | 2022 | Review | COVID-19 infection interferes with ACE2 receptors found at the endometrium and negatively affects embryo implantation and/or fetal distress in pregnant patients |
| Shanes E.D. et al. [22] | 2020 | Article | Higher incidence of maternal vascular malperfusion (MVM), with decidual arteriopathy in COVID-19 pregnancies |
| Sharma I. et al. [3] | 2021 | Review | COVID-19 affects granulosa cells and ovarian tissue and increases the risk of miscarriage and infertility |
| Sills E.S. et al. [35] | 2020 | Review | In COVID-19, preferential Th1 immunity stimulation is induced and may affect embryo implantation |
| Vesce F. et al. [36] | 2022 | Review | Miscarriages in COVID-19 patients, at immunopathological levels, might result from thromboembolic events, pro-inflammatory maternal immunological responses, or direct viral activity in the uterine environment |
| Villar J. et al. [17] | 2021 | Cohort study/2130 women | COVID-19 infection in pregnancy was associated with increased risk for neonatal complications |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrysanthopoulos, I.; Potiris, A.; Drakaki, E.; Mavrogianni, D.; Machairiotis, N.; Zarogoulidis, P.; Karampitsakos, T.; Machairoudias, P.; Vrachnis, D.; Panagopoulos, P.; et al. Association between COVID-19 Infection and Miscarriages, What We Really Know? Diseases 2023, 11, 173. https://doi.org/10.3390/diseases11040173
Chrysanthopoulos I, Potiris A, Drakaki E, Mavrogianni D, Machairiotis N, Zarogoulidis P, Karampitsakos T, Machairoudias P, Vrachnis D, Panagopoulos P, et al. Association between COVID-19 Infection and Miscarriages, What We Really Know? Diseases. 2023; 11(4):173. https://doi.org/10.3390/diseases11040173
Chicago/Turabian StyleChrysanthopoulos, Ioannis, Anastasios Potiris, Eirini Drakaki, Despoina Mavrogianni, Nikolaos Machairiotis, Paul Zarogoulidis, Theodoros Karampitsakos, Pavlos Machairoudias, Dionysios Vrachnis, Periklis Panagopoulos, and et al. 2023. "Association between COVID-19 Infection and Miscarriages, What We Really Know?" Diseases 11, no. 4: 173. https://doi.org/10.3390/diseases11040173
APA StyleChrysanthopoulos, I., Potiris, A., Drakaki, E., Mavrogianni, D., Machairiotis, N., Zarogoulidis, P., Karampitsakos, T., Machairoudias, P., Vrachnis, D., Panagopoulos, P., Drakakis, P., & Stavros, S. (2023). Association between COVID-19 Infection and Miscarriages, What We Really Know? Diseases, 11(4), 173. https://doi.org/10.3390/diseases11040173