
Long COVID and Physical Therapy: A Systematic Review

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Protocol
2.2. Eligibility Criteria
2.3. Sources of Information
2.4. Search Strategy
2.5. Data Extraction Process
2.6. Data Collection Process and Data Collected
2.7. Methodological Quality Assessment
2.8. Risk of Bias in Individual Studies
2.9. Synthesis of Results
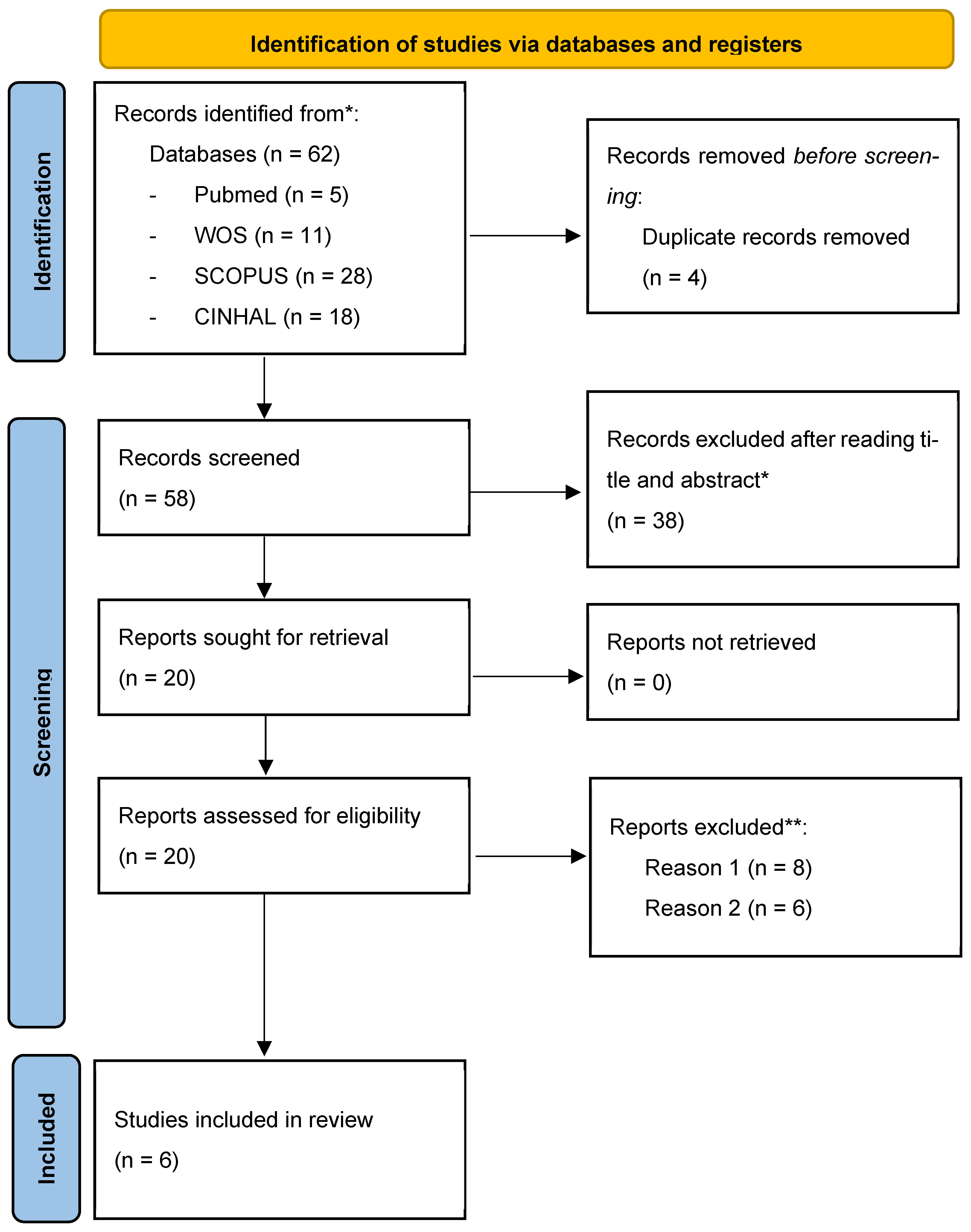
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Institute for Health and Care Excellence (NICE); Scottish Intercollegiate Guidelines Network (SIGN); Royal College of General Practitioners (RCGP) (Eds.) COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; Version 1; NICE: London, UK, 2022. [Google Scholar]
- Townsend, L.; Dyer, A.H.; McCluskey, P.; O’Brien, K.; Dowds, J.; Laird, E.; Bannan, C.; Bourke, N.M.; Ní Cheallaigh, C.; Byrne, D.G.; et al. Investigating the Relationship between Vitamin D and Persistent Symptoms Following SARS-CoV-2 Infection. Nutrients 2021, 13, 2430. [Google Scholar] [CrossRef] [PubMed]
- Pancera, S.; Bianchi, L.N.C.; Porta, R.; Galeri, S.; Carrozza, M.C.; Villafañe, J.H. Feasibility of Subacute Rehabilitation for Mechanically Ventilated Patients with COVID-19 Disease: A Retrospective Case Series. Int. J. Rehabil. Res. 2021, 44, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, A.; Piekorz, Z.; Sarwińska, J.; Siedlaczek, M. Long-Term Trends in Changes in Physical and Motor Development Observed among Physiotherapy Students from Bydgoszcz in 2011–2020. Int. J. Environ. Res. Public Health 2022, 19, 14444. [Google Scholar] [CrossRef]
- Certain Curi, A.C.; Antunes Ferreira, A.P.; Calazans Nogueira, L.A.; Meziat Filho, N.A.M.; Sá Ferreira, A. Osteopathy and Physiotherapy Compared to Physiotherapy Alone on Fatigue in Long COVID: Study Protocol for a Pragmatic Randomized Controlled Superiority Trial. Int. J. Osteopath. Med. 2022, 44, 22–28. [Google Scholar] [CrossRef]
- Wagner, B.; Steiner, M.; Markovic, L.; Crevenna, R. Successful Application of Pulsed Electromagnetic Fields in a Patient with Post-COVID-19 Fatigue: A Case Report. Wien. Med. Wochenschr. 2022, 172, 227–232. [Google Scholar] [CrossRef]
- Dean, E.; Söderlund, A.; Gosselink, R.; Jones, A.Y.M.; Yu, H.P.-M.; Skinner, M. Immuno-Modulation with Lifestyle Behaviour Change to Reduce SARS-CoV-2 Susceptibility and COVID-19 Severity: Goals Consistent with Contemporary Physiotherapy Practice. Physiotherapy 2022, 114, 63–67. [Google Scholar] [CrossRef]
- Kristoffersen, A.E.; Jong, M.C.; Nordberg, J.H.; van der Werf, E.T.; Stub, T. Safety and Use of Complementary and Alternative Medicine in Norway during the First Wave of the COVID-19 Pandemic Using an Adapted Version of the I-CAM-Q; a Cross-Sectional Survey. BMC Complement. Med. Ther. 2022, 22, 234. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.v. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Rosman, L.; Mazzella, A.J.; Gehi, A.; Liu, Y.; Li, Q.; Salmoirago-Blotcher, E.; Lampert, R.; Burg, M.M. Immediate and Long-term Effects of the COVID-19 Pandemic and Lockdown on Physical Activity in Patients with Implanted Cardiac Devices. Pacing Clin. Electrophysiol. 2022, 45, 111–123. [Google Scholar] [CrossRef]
- Scheiber, B.; Spiegl, C.; Wiederin, C.; Schifferegger, E.; Schiefermeier-Mach, N. Post-COVID-19 Rehabilitation: Perception and Experience of Austrian Physiotherapists and Physiotherapy Students. Int. J. Environ. Res. Public Health 2021, 18, 8730. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.; Yáñez, A.M.; Bennasar-Veny, M.; Navarro, C.; Salva, J.; Ibarra, O.; Gomez-Juanes, R.; Serrano-Ripoll, M.J.; Oliván, B.; Gili, M.; et al. Efficacy of an Adjuvant Non-Face-to-Face Multimodal Lifestyle Modification Program for Patients with Treatment-Resistant Major Depression: A Randomized Controlled Trial. Psychiatry Res. 2023, 319, 114975. [Google Scholar] [CrossRef] [PubMed]
- Estebanez-Pérez, M.-J.; Pastora-Bernal, J.-M.; Martín-Valero, R. The Effectiveness of a Four-Week Digital Physiotherapy Intervention to Improve Functional Capacity and Adherence to Intervention in Patients with Long COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 9566. [Google Scholar] [CrossRef] [PubMed]
- Palau, P.; Domínguez, E.; Gonzalez, C.; Bondía, E.; Albiach, C.; Sastre, C.; Martínez, M.L.; Núñez, J.; López, L. Effect of a Home-Based Inspiratory Muscle Training Programme on Functional Capacity in Postdischarged Patients with Long COVID: The InsCOVID Trial. BMJ Open Respir. Res. 2022, 9, e001439. [Google Scholar] [CrossRef]
- Chang, Y.; Li, K.M.C.; Chien, L.; Lee, E.Y.; Hong, S.A.; Coca, K.P. Associations between Breastfeeding Intention, Breastfeeding Practices and Post-natal Depression during the COVID-19 Pandemic: A Multi-country Cross-sectional Study. Matern. Child Nutr. 2023, 19, e13450. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- The University of Sidney Physiotherapy Evidence Database-PEDro. Available online: https://pedro.org.au/ (accessed on 30 January 2023).
- RobotReviewer. Available online: https://www.robotreviewer.net/ (accessed on 17 January 2023).
- Jimeno-Almazán, A.; Buendía-Romero, Á.; Martínez-Cava, A.; Franco-López, F.; Sánchez-Alcaraz, B.J.; Courel-Ibáñez, J.; Pallarés, J.G. Effects of a Concurrent Training, Respiratory Muscle Exercise, and Self-Management Recommendations on Recovery from Post-COVID-19 Conditions: The RECOVE Trial. J. Appl. Physiol. 2023, 134, 95–104. [Google Scholar] [CrossRef]
- Jimeno-Almazán, A.; Franco-López, F.; Buendía-Romero, Á.; Martínez-Cava, A.; Sánchez-Agar, J.A.; Sánchez-Alcaraz Martínez, B.J.; Courel-Ibáñez, J.; Pallarés, J.G. Rehabilitation for Post-COVID-19 Condition through a Supervised Exercise Intervention: A Randomized Controlled Trial. Scand. J. Med. Sci. Sports 2022, 32, 1791–1801. [Google Scholar] [CrossRef]
- McNarry, M.A.; Berg, R.M.G.; Shelley, J.; Hudson, J.; Saynor, Z.L.; Duckers, J.; Lewis, K.; Davies, G.A.; Mackintosh, K.A. Inspiratory Muscle Training Enhances Recovery Post-COVID-19: A Randomised Controlled Trial. Eur. Respir. J. 2022, 60, 2103101. [Google Scholar] [CrossRef]
- Philip, K.E.J.; Owles, H.; McVey, S.; Pagnuco, T.; Bruce, K.; Brunjes, H.; Banya, W.; Mollica, J.; Lound, A.; Zumpe, S.; et al. An Online Breathing and Wellbeing Programme (ENO Breathe) for People with Persistent Symptoms Following COVID-19: A Parallel-Group, Single-Blind, Randomised Controlled Trial. Lancet Respir. Med. 2022, 10, 851–862. [Google Scholar] [CrossRef]
- Sharma, P.; Goswami, S.K. Pulmonary Tele-Rehabilitation in Patients (Post COVID-19) With Respiratory Complications: A Randomized Controlled Trial. Indian J. Physiother. Occup. Ther.-Int. J. 2022, 16, 182–189. [Google Scholar] [CrossRef]
- Vickory, F.; Ridgeway, K.; Falvey, J.; Houwer, B.; Gunlikson, J.; Payne, K.; Niehaus, W. Safety, Feasibility, and Outcomes of Frequent, Long-Duration Rehabilitation in an Inpatient Rehabilitation Facility After Prolonged Hospitalization for Severe COVID-19: An Observational Study. Phys. Ther. 2021, 101, pzab208. [Google Scholar] [CrossRef] [PubMed]
- Kashif, M.; Ahmad, A.; Ashraf, A.; Imtiaz, Z.; Albalwi, A.; Hussain, M.N. Physical Therapists’ Knowledge and Implementation of Best Practices in the Outpatient Physiotherapy Department during the COVID-19 Pandemic: A Cross-Sectional Study. Work 2022, 71, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Yu, P.; Yang, M.; Xie, W.; Huang, L.; He, C.; Gosselink, R.; Wei, Q.; Jones, A.Y.M. Physical Therapist Management of COVID-19 in the Intensive Care Unit: The West China Hospital Experience. Phys. Ther. 2021, 101, pzaa198. [Google Scholar] [CrossRef]
- Plekhanova, T.; Rowlands, A.V.; Evans, R.A.; Edwardson, C.L.; Bishop, N.C.; Bolton, C.E.; Chalmers, J.D.; Davies, M.J.; Daynes, E.; Dempsey, P.C.; et al. Device-Assessed Sleep and Physical Activity in Individuals Recovering from a Hospital Admission for COVID-19: A Multicentre Study. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 94. [Google Scholar] [CrossRef]
- Saliba-Gustafsson, E.A.; Miller-Kuhlmann, R.; Kling, S.M.R.; Garvert, D.W.; Brown-Johnson, C.G.; Lestoquoy, A.S.; Verano, M.-R.; Yang, L.; Falco-Walter, J.; Shaw, J.G.; et al. Rapid Implementation of Video Visits in Neurology During COVID-19: Mixed Methods Evaluation. J. Med. Internet Res. 2020, 22, e24328. [Google Scholar] [CrossRef]
- Mirabzadeh, A.; Forouzan, A.S.; Falahat, K.; Chinehkesh, A.; Banazadeh, Z.; Eftekhari, M.B. Help Seeking Behaviors during Covid 19 Pandemic in Iran: A Qualitative Study. Evid. Based Care J. 2022, 12, 17–23. [Google Scholar] [CrossRef]
- Lai, K.S.P.; Watt, C.; Ionson, E.; Baruss, I.; Forchuk, C.; Sukhera, J.; Burhan, A.M.; Vasudev, A. Breath Regulation and Yogic Exercise An Online Therapy for Calm and Happiness (BREATH) for Frontline Hospital and Long-Term Care Home Staff Managing the COVID-19 Pandemic: A Structured Summary of a Study Protocol for a Feasibility Study for a Randomised Controlled Trial. Trials 2020, 21, 648. [Google Scholar] [CrossRef]
- Cahalan, R.; Meade, C.; Mockler, S. SingStrong—A Singing and Breathing Retraining Intervention for Respiratory and Other Common Symptoms of Long COVID: A Pilot Study. Can. J. Respir. Ther. 2022, 58, 20–27. [Google Scholar] [CrossRef]
- Gothe, N.P.; Erlenbach, E. Feasibility of a Yoga, Aerobic and Stretching-Toning Exercise Program for Adult Cancer Survivors: The STAYFit Trial. J. Cancer Surviv. 2022, 16, 1107–1116. [Google Scholar] [CrossRef]


{kind=link}
| Sources | Search Strategy | Filters | Limits | Date of Search | Items |
|---|---|---|---|---|---|
| SCOPUS | (TITLE-ABS-KEY-AUTH (long AND covid) AND TITLE-ABS-KEY (physical AND therapy AND modalities) AND NOT TITLE-ABS-KEY (child *)) AND (LIMIT-TO (DOCTYPE, “ar”)) | RCT research | 2019- | 14 January 2023 | 28 |
| PUBMED | ((LONG COVID[Title/Abstract]) AND (“physical therapy modalities” [MeSH Terms])) AND (Therapy/Broad[filter]) | RCT Full text | 2019- | 10 January 2023 | 5 |
| WOS | long COVID (Topic) and physical therapy (Topic) | Document types: Clinical trial. MeSH Qualifiers: Therapy. MesH Headings: Humans | 2019- | 8 January 2023 | 11 |
| CINAHL | long COVID OR post-acute COVID-19 syndrome AND (physical therapy or physiotherapy or rehabilitation) | Limits—Full text; Refereed publications; Human; Age groups: Adult: 19–44 years, Middle Aged: 45–64 years Enlargers—Apply Equivalent Subjects Search Modes—Boolean/Phrase | 2019- | 15 January 2023 | 18 |
| Reference | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | P10 | P11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Jimeno-Almazán et al., 2023 [20] | + | - | + | - | - | - | + | + | + | + | 6/10 |
| Jimeno-Almazán et al., 2022 [21] | + | - | + | - | - | - | + | + | + | + | 6/10 |
| Mcnarry et al., 2022 [22] | + | - | - | - | - | - | + | + | + | + | 5/10 |
| Palau et al., 2022 [15] | + | - | + | - | - | + | + | + | + | + | 7/10 |
| Philip et al., 2022 [23] | + | - | + | + | - | - | + | + | + | + | 7/10 |
| Sharma et al., 2022 [24] | + | - | - | + | + | - | + | - | + | + | 6/10 |
| Rate of compliance | 100% | 0% | 67% | 33% | 17% | 17% | 100% | 83% | 100% | 100% |
| Trial | Design | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment |
|---|---|---|---|---|---|
| Palau et al., 2022 [15] | RCT | + | + | ? | + |
| Sharma et al., 2022 [24] | RCT | ? | ? | ? | + |
| Jimeno-Almazán et al., 2023 [20] | RCT | + | ? | ? | ? |
| Jimeno-Almazán et al., 2022 [21] | RCT | + | ? | ? | ? |
| Philip et al., 2022 [23] | RCT | + | + | ? | + |
| Mcnarry et al., 2022 [22] | RCT | + | + | ? | ? |
| Author | Participants | Interventions | Outcomes | Conclusion | Finding |
|---|---|---|---|---|---|
| Palau et al., 2022 [15] | 26 post-discharged patients with long COVID | They assessed a 12-week home-based IMT program in 26 post-discharge COVID-19 patients | At 12 weeks, the mean pp-peakVO2 was higher in the IMT group compared to controls | IMT significantly increased pp-peakVO2 in post-COVID patients versus controls | ↑ sig increase |
| Sharma et al., 2022 [24] | 30 post-COVID patients with respiratory complications and chronic COVID | They evaluated a pulmonary tele-rehabilitation program including breathing exercises and therapeutic exercises in 30 post-COVID patients with respiratory complications and chronic COVID compared to conventional care | Patients receiving tele-rehabilitation showed significant improvement in dyspnea, fatigue, and ability to rehabilitate at home versus conventional care | Pulmonary tele-rehabilitation was a valuable service for post-COVID patients with respiratory complications | ↑ sig increase |
| Jimeno-Almazán et al., 2023 [20] | 80 non-hospitalized adults with post-COVID-19 conditions | They compared two 8-week exercise programs in 80 non-hospitalized adults with post-COVID conditions: (1) multicomponent exercise with concurrent resistance and endurance training versus (2) a program combining inspiratory muscle training, physical exercise and self-management | The multicomponent exercise program elicited significant improvement in fatigue, depression, fitness, quality of life, symptoms, dyspnea, strength, and severity versus the other program | Multicomponent exercise with concurrent training showed more effectiveness than the other program in post-COVID conditions | ↑ sig increase |
| Jimeno-Almazán et al., 2022 [21] | 39 patients | They compared 10 weeks of tailored supervised therapeutic exercise versus self-management recommendations in the WHO rehabilitation leaflet in 39 patients with post-COVID conditions | Supervised exercise showed significantly better cardiovascular fitness, strength, quality of life, fatigue, depression, and functional status than self-management controls | Supervised therapeutic exercise was a more effective intervention than self-management in post-COVID conditions | ↑ sig increase |
| Philip et al., 2022 [23] | 192 people with long COVID | They assessed a 6-week online breathing and well-being program developed for 192 people with long COVID experiencing breathlessness | The online breathing program improved the mental component of HRQoL and breathlessness VAS while running versus controls | The online breathing program improved mental HRQoL and breathlessness in people with persisting post-COVID symptoms | ↑ sig increase |
| Mcnarry et al., 2022 [22] | 281 adults recovering from self-reported COVID-19 | They compared IMT versus control in 281 adults recovering from self-reported COVID-19 | No difference between groups in KBILD total score but clinically meaningful IMT improvements in breathlessness, chest symptoms, and respiratory muscle strength | IMT may represent an important home-based post-COVID rehabilitation strategy, improving breathlessness, chest symptoms, respiratory muscle strength and estimated aerobic fitness | ↓ sig decrease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-García, J.C.; Reinoso-Cobo, A.; Piqueras-Sola, B.; Cortés-Martín, J.; Menor-Rodríguez, M.J.; Alabau-Dasi, R.; Rodríguez-Blanque, R. Long COVID and Physical Therapy: A Systematic Review. Diseases 2023, 11, 163. https://doi.org/10.3390/diseases11040163
Sánchez-García JC, Reinoso-Cobo A, Piqueras-Sola B, Cortés-Martín J, Menor-Rodríguez MJ, Alabau-Dasi R, Rodríguez-Blanque R. Long COVID and Physical Therapy: A Systematic Review. Diseases. 2023; 11(4):163. https://doi.org/10.3390/diseases11040163
Chicago/Turabian StyleSánchez-García, Juan Carlos, Andrés Reinoso-Cobo, Beatriz Piqueras-Sola, Jonathan Cortés-Martín, María José Menor-Rodríguez, Raquel Alabau-Dasi, and Raquel Rodríguez-Blanque. 2023. "Long COVID and Physical Therapy: A Systematic Review" Diseases 11, no. 4: 163. https://doi.org/10.3390/diseases11040163
APA StyleSánchez-García, J. C., Reinoso-Cobo, A., Piqueras-Sola, B., Cortés-Martín, J., Menor-Rodríguez, M. J., Alabau-Dasi, R., & Rodríguez-Blanque, R. (2023). Long COVID and Physical Therapy: A Systematic Review. Diseases, 11(4), 163. https://doi.org/10.3390/diseases11040163