
Chloroquine and Hydroxychloroquine in the Treatment of Dry Eye Disease


 , , ,
, , , 
Abstract
1. Introduction

| Aqueous-Deficient Dry Eye Disease | Evaporative Dry Eye Disease |
|---|---|
| Sjögren’s-syndrome-related dry eye disease [3,45] | Meibomian Gland Dysfunction [3] |
| Non-Sjögren’s-syndrome-related dry eye disease, including inflammatory lacrimal gland infiltration, or lacrimal gland obstruction [3,45] | Ocular surface related evaporative dry eye disease [3] |
| Other conditions, including diabetes mellitus [3] | Disorders of the lid aperture [3] |
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
- P (Population): patients with dry eye disease;
- I (Intervention): treatment with CQ or HCQ;
- C (Comparison): efficacy at the last follow-up, comparison with placebo or artificial tears (control group);
- O (Outcomes): Tear breakup time; Schirmer I test, corneal staining, Ocular Surface Disease Index.
2.3. Selection and Data Collection
2.4. Assessment of the Study Risk of Bias
2.5. Synthesis Methods
3. Results
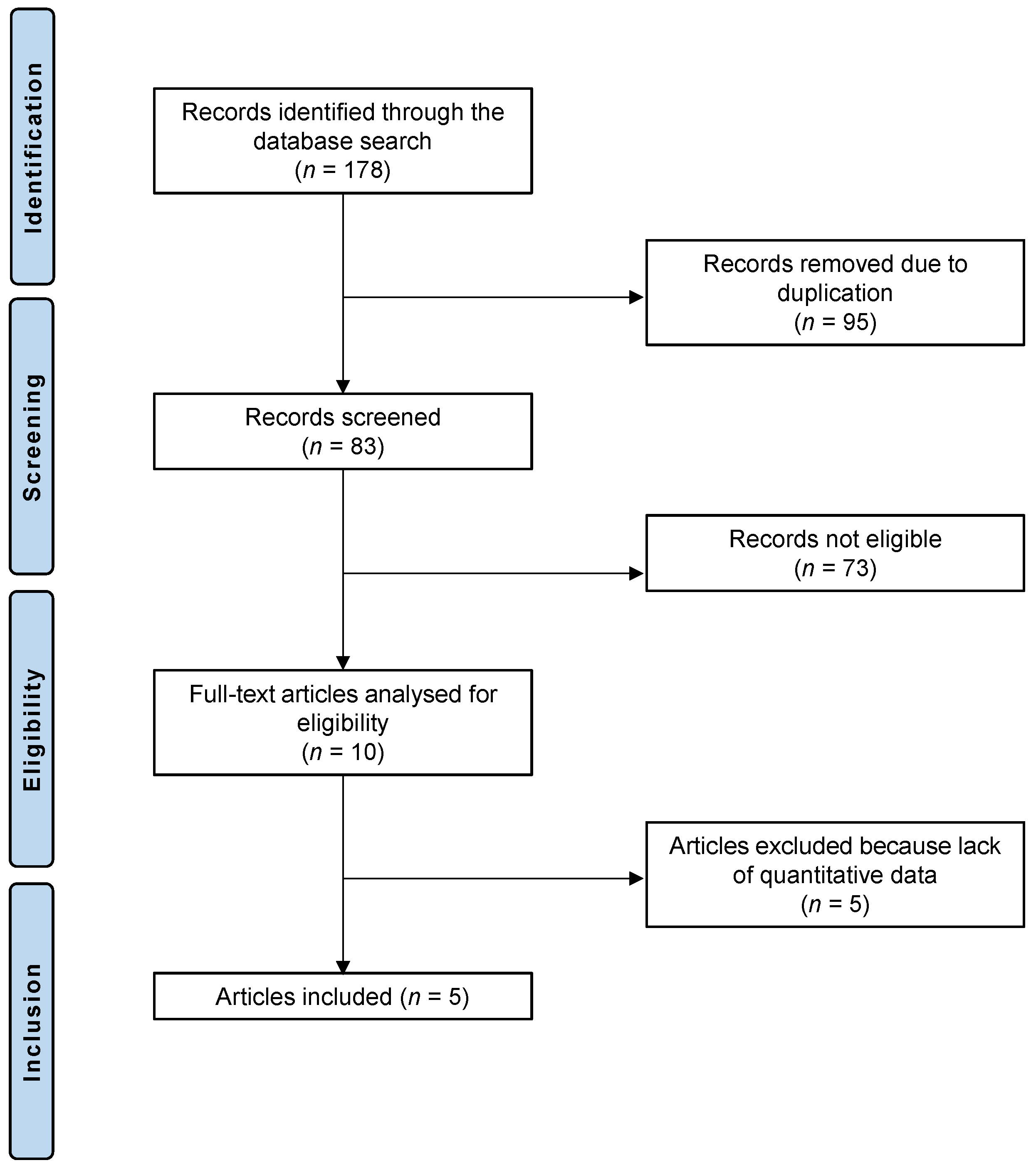
3.1. Study Selection
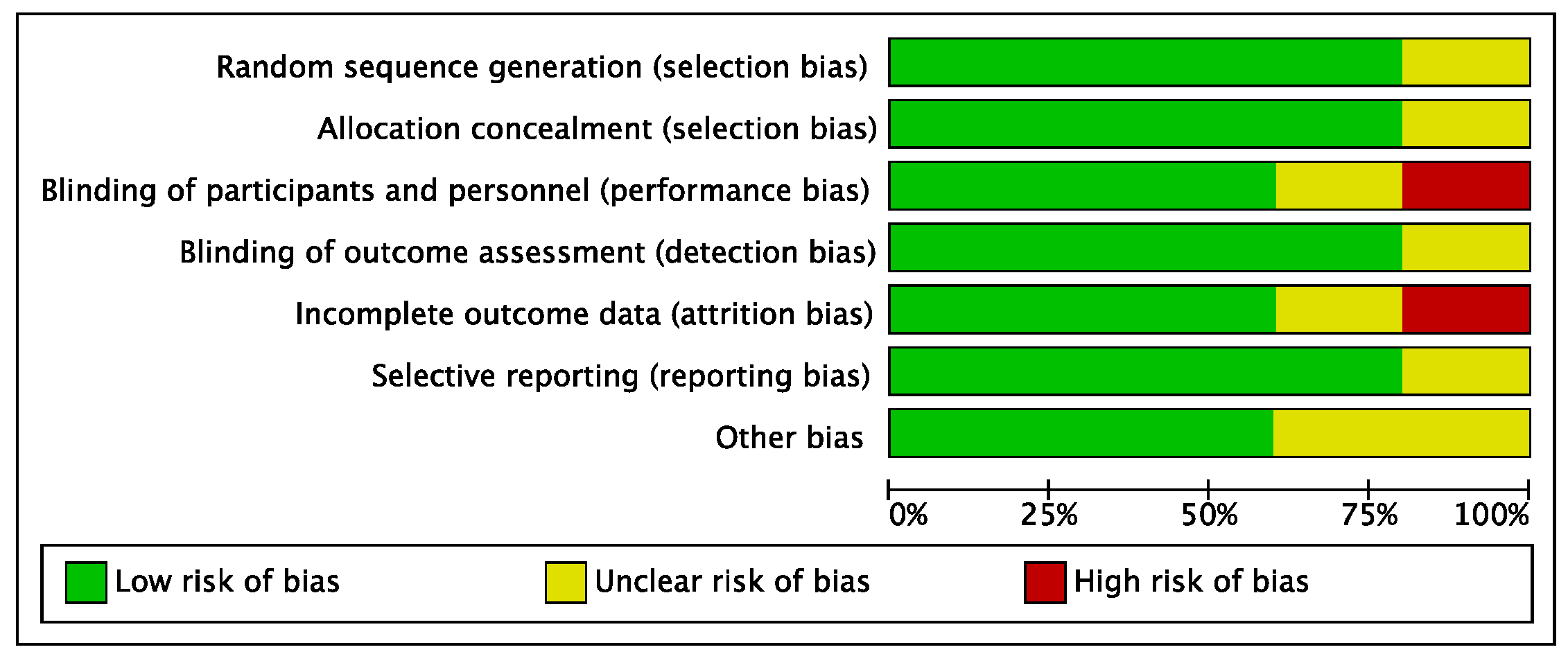
3.2. Risk of Bias Evaluation
3.3. Study Characteristics and Results of Studies
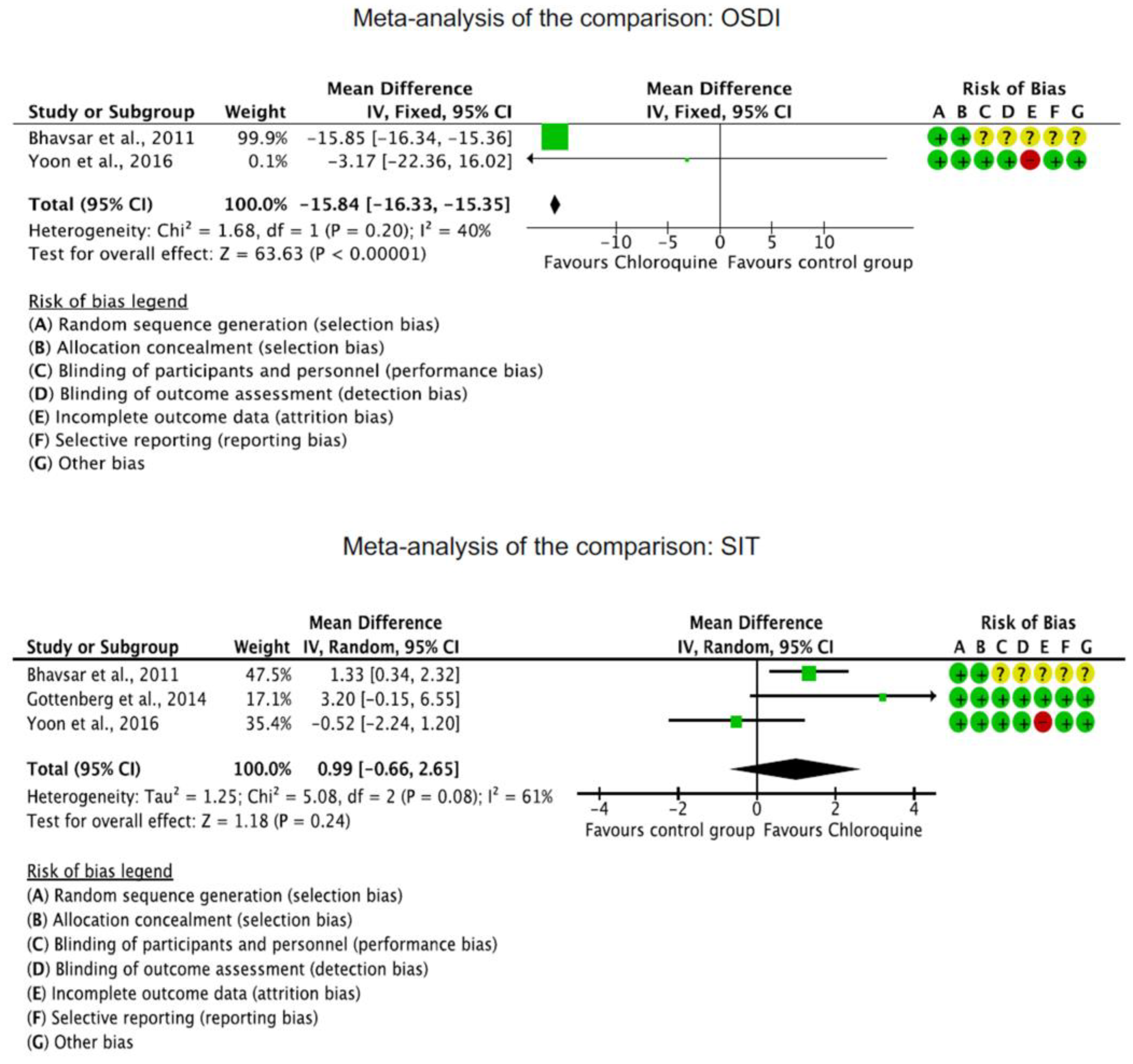
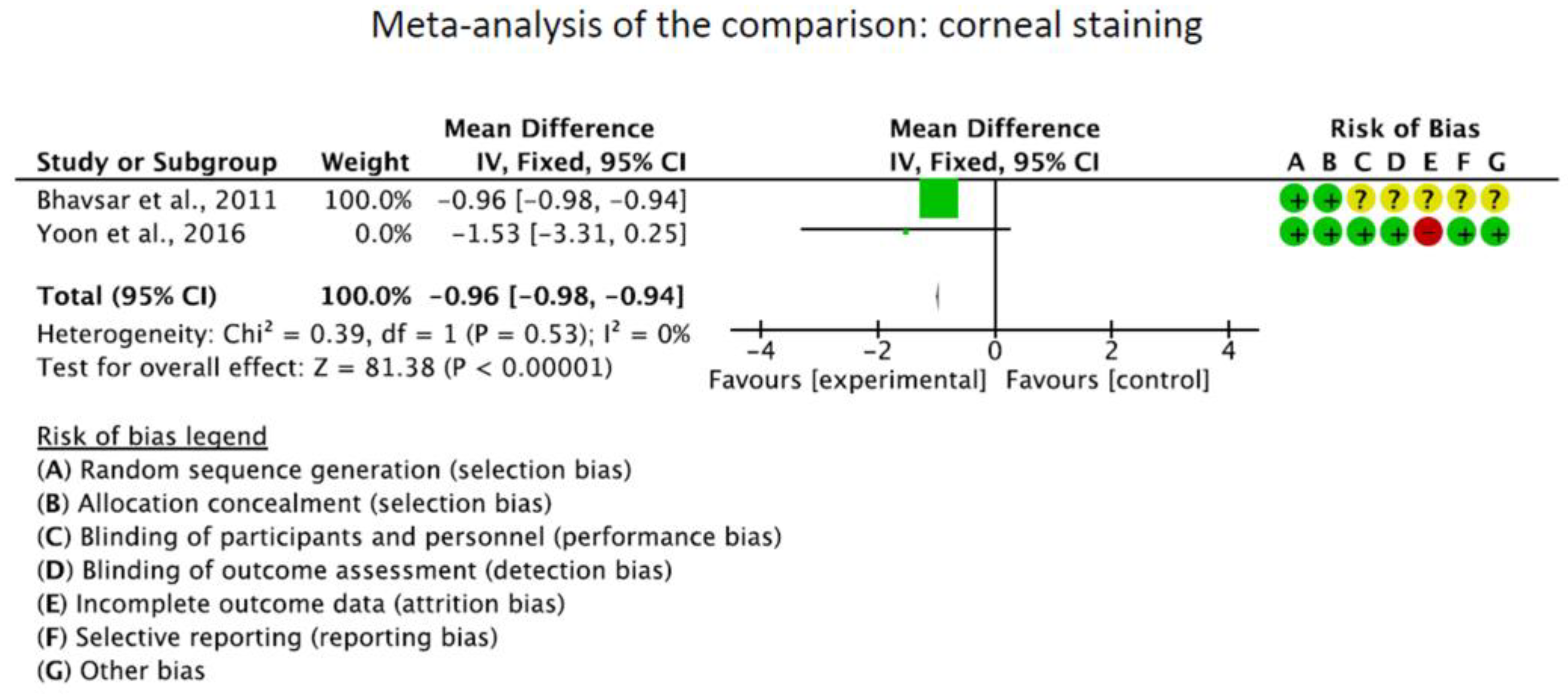
3.4. Efficacy of CQ and HCQ
3.5. CQ and HCQ Compared to Other Treatments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, F.; Alves, M.; Bunya, V.Y.; Jalbert, I.; Lekhanont, K.; Malet, F.; Na, K.S.; Schaumberg, D.; Uchino, M.; Vehof, J.; et al. TFOS DEWS II Epidemiology Report. Ocul. Surf. 2017, 15, 334–365. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II pathophysiology report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef]
- Ohashi, Y.; Ishida, R.; Kojima, T.; Goto, E.; Matsumoto, Y.; Watanabe, K.; Ishida, N.; Nakata, K.; Takeuchi, T.; Tsubota, K. Abnormal protein profiles in tears with dry eye syndrome. Am. J. Ophthalmol. 2003, 136, 291–299. [Google Scholar] [CrossRef]
- Javadi, M.A.; Feizi, S. Dry eye syndrome. J. Ophthalmic Vis. Res. 2011, 6, 192–198. [Google Scholar]
- Alves, M.; Novaes, P.; Morraye Mde, A.; Reinach, P.S.; Rocha, E.M. Is dry eye an environmental disease? Arq. Bras. Oftalmol. 2014, 77, 193–200. [Google Scholar] [CrossRef]
- Seen, S.; Tong, L. Dry eye disease and oxidative stress. Acta Ophthalmol. 2018, 96, e412–e420. [Google Scholar] [CrossRef]
- Kanellopoulos, A.J.; Asimellis, G. In pursuit of objective dry eye screening clinical techniques. Eye Vis. 2016, 3, 1. [Google Scholar] [CrossRef]
- Lemp, M.A.; Foulks, G.N. The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 75–92. [Google Scholar] [CrossRef]
- Sullivan, B.D.; Crews, L.A.; Messmer, E.M.; Foulks, G.N.; Nichols, K.K.; Baenninger, P.; Geerling, G.; Figueiredo, F.; Lemp, M.A. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: Clinical implications. Acta Ophthalmol. 2014, 92, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Li, D.Q.; Doshi, A.; Farley, W.; Corrales, R.M.; Pflugfelder, S.C. Experimental dry eye stimulates production of inflammatory cytokines and MMP-9 and activates MAPK signaling pathways on the ocular surface. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4293–4301. [Google Scholar] [CrossRef]
- Na, K.S.; Mok, J.W.; Kim, J.Y.; Rho, C.R.; Joo, C.K. Correlations between tear cytokines, chemokines, and soluble receptors and clinical severity of dry eye disease. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5443–5450. [Google Scholar] [CrossRef]
- Zoukhri, D. Effect of inflammation on lacrimal gland function. Exp. Eye Res. 2006, 82, 885–898. [Google Scholar] [CrossRef]
- Greenspan, J.S.; Daniels, T.E.; Talal, N.; Sylvester, R.A. The histopathology of Sjögren’s syndrome in labial salivary gland biopsies. Oral. Surg. Oral. Med. Oral. Pathol. 1974, 37, 217–229. [Google Scholar] [CrossRef]
- Cho, P.; Yap, M. Schirmer test. I. A review. Optom. Vis. Sci. 1993, 70, 152–156. [Google Scholar] [CrossRef]
- Cho, P.; Leung, L.; Lam, A.; Choi, A. Tear break-up time: Clinical procedures and their effects. Ophthalmic Physiol. Opt. 1998, 18, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Nichols, K.K.; Baldwin, E.K. Current patterns in the use of diagnostic tests in dry eye evaluation. Cornea 2008, 27, 656–662. [Google Scholar] [CrossRef]
- Yang, Y.J.; Lee, W.Y.; Kim, Y.J.; Hong, Y.P. A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2383. [Google Scholar] [CrossRef] [PubMed]
- Bhavsar, A.S.; Bhavsar, S.G.; Jain, S.M. Evaluation of the Effects of Chloroquine Phosphate Eye Drops in Patients with Dry Eye Syndrome. Int. J. Biomed. Adv. Res. 2011, 2, 198–214. [Google Scholar] [CrossRef]
- Kallab, M.; Szegedi, S.; Hommer, N.; Stegmann, H.; Kaya, S.; Werkmeister, R.M.; Schmidl, D.; Schmetterer, L.; Garhofer, G. Topical Low Dose Preservative-Free Hydrocortisone Reduces Signs and Symptoms in Patients with Chronic Dry Eye: A Randomized Clinical Trial. Adv. Ther. 2020, 37, 329–341. [Google Scholar] [CrossRef]
- Prinz, J.; Maffulli, N.; Fuest, M.; Walter, P.; Bell, A.; Migliorini, F. Efficacy of Topical Administration of Corticosteroids for the Management of Dry Eye Disease: Systematic Review and Meta-Analysis. Life 2022, 12, 1932. [Google Scholar] [CrossRef] [PubMed]
- Coursey, T.G.; de Paiva, C.S. Managing Sjögren’s Syndrome and non-Sjögren Syndrome dry eye with anti-inflammatory therapy. Clin. Ophthalmol. 2014, 8, 1447–1458. [Google Scholar] [CrossRef] [PubMed]
- Prinz, J.; Maffulli, N.; Fuest, M.; Walter, P.; Hildebrand, F.; Migliorini, F. Placebo administration for dry eye disease: A level I evidence based systematic review and meta-analysis. Int. J. Clin. Pharm. 2022, 44, 1087–1101. [Google Scholar] [CrossRef]
- Jones, L.; Downie, L.E.; Korb, D.; Benitez-Del-Castillo, J.M.; Dana, R.; Deng, S.X.; Dong, P.N.; Geerling, G.; Hida, R.Y.; Liu, Y.; et al. TFOS DEWS II Management and Therapy Report. Ocul. Surf. 2017, 15, 575–628. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.Y.; Li, Y.H. A survey on treatment of dry eye by traditional chinese medicine and integrative chinese and Western medicine. Chin. J. Integr. Med. 2006, 12, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Prinz, J.; Maffulli, N.; Fuest, M.; Walter, P.; Hildebrand, F.; Migliorini, F. Honey-Related Treatment Strategies in Dry Eye Disease. Pharmaceuticals 2023, 16, 762. [Google Scholar] [CrossRef]
- Prinz, J.; Maffulli, N.; Fuest, M.; Walter, P.; Hildebrand, F.; Migliorini, F. Acupuncture for the management of dry eye disease. Front. Med. 2022, 16, 975–983. [Google Scholar] [CrossRef]
- Mittal, R.; Patel, S.; Galor, A. Alternative therapies for dry eye disease. Curr. Opin. Ophthalmol. 2021, 32, 348–361. [Google Scholar] [CrossRef]
- Yusuf, I.H.; Sharma, S.; Luqmani, R.; Downes, S.M. Hydroxychloroquine retinopathy. Eye 2017, 31, 828–845. [Google Scholar] [CrossRef]
- Karres, I.; Kremer, J.P.; Dietl, I.; Steckholzer, U.; Jochum, M.; Ertel, W. Chloroquine inhibits proinflammatory cytokine release into human whole blood. Am. J. Physiol. 1998, 274, R1058–R1064. [Google Scholar] [CrossRef]
- Meinão, I.M.; Sato, E.I.; Andrade, L.E.; Ferraz, M.B.; Atra, E. Controlled trial with chloroquine diphosphate in systemic lupus erythematosus. Lupus 1996, 5, 237–241. [Google Scholar] [CrossRef]
- Augustijns, P.; Geusens, P.; Verbeke, N. Chloroquine levels in blood during chronic treatment of patients with rheumatoid arthritis. Eur. J. Clin. Pharmacol. 1992, 42, 429–433. [Google Scholar] [CrossRef]
- Ben-Zvi, I.; Kivity, S.; Langevitz, P.; Shoenfeld, Y. Hydroxychloroquine: From malaria to autoimmunity. Clin. Rev. Allergy Immunol. 2012, 42, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Rainsford, K.D.; Parke, A.L.; Clifford-Rashotte, M.; Kean, W.F. Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases. Inflammopharmacology 2015, 23, 231–269. [Google Scholar] [CrossRef]
- Goodman, S.M. Rheumatoid arthritis: Perioperative management of biologics and DMARDs. Semin. Arthritis Rheum. 2015, 44, 627–632. [Google Scholar] [CrossRef]
- Mariette, X.; Gottenberg, J.E. Pathogenesis of Sjögren’s syndrome and therapeutic consequences. Curr. Opin. Rheumatol. 2010, 22, 471–477. [Google Scholar] [CrossRef]
- Kuznik, A.; Bencina, M.; Svajger, U.; Jeras, M.; Rozman, B.; Jerala, R. Mechanism of endosomal TLR inhibition by antimalarial drugs and imidazoquinolines. J. Immunol. 2011, 186, 4794–4804. [Google Scholar] [CrossRef] [PubMed]
- Lesiak, A.; Narbutt, J.; Sysa-Jedrzejowska, A.; Lukamowicz, J.; McCauliffe, D.P.; Wózniacka, A. Effect of chloroquine phosphate treatment on serum MMP-9 and TIMP-1 levels in patients with systemic lupus erythematosus. Lupus 2010, 19, 683–688. [Google Scholar] [CrossRef]
- Weber, S.M.; Chen, J.M.; Levitz. S.M. Inhibition of mitogen-activated protein kinase signaling by chloroquine. J. Immunol. 2002, 168, 5303–5309. [Google Scholar] [CrossRef] [PubMed]
- Yoon, C.H.; Lee, H.J.; Lee, E.Y.; Lee, E.B.; Lee, W.W.; Kim, M.K.; Wee, W.R. Effect of Hydroxychloroquine Treatment on Dry Eyes in Subjects with Primary Sjogren’s Syndrome: A Double-Blind Randomized Control Study. J. Korean Med. Sci. 2016, 31, 1127–1135. [Google Scholar] [CrossRef]
- Gottenberg, J.E.; Ravaud, P.; Puechal, X.; Le Guern, V.; Sibilia, J.; Goeb, V.; Larroche, C.; Dubost, J.J.; Rist, S.; Saraux, A.; et al. Effects of hydroxychloroquine on symptomatic improvement in primary Sjogren syndrome: The JOQUER randomized clinical trial. JAMA 2014, 312, 249–258. [Google Scholar] [CrossRef]
- Kruize, A.A.; Hené, R.J.; Kallenberg, C.G.; van Bijsterveld, O.P.; van der Heide, A.; Kater, L.; Bijlsma, J.W. Hydroxychloroquine treatment for primary Sjögren’s syndrome: A two year double blind crossover trial. Ann. Rheum. Dis. 1993, 52, 360–364. [Google Scholar] [CrossRef]
- Bodewes, I.L.A.; Gottenberg, J.E.; van Helden-Meeuwsen, C.G.; Mariette, X.; Versnel, M.A. Hydroxychloroquine treatment downregulates systemic interferon activation in primary Sjogren’s syndrome in the JOQUER randomized trial. Rheumatology 2020, 59, 107–111. [Google Scholar] [CrossRef]
- Tyagi, P.; Sharma, V.; Chugh, J.P.; Chauhan, R.S.; Rathi, A. A comparative study of efficacy of chloroquine phosphate 0.03% and sodiumcarboxymethylcellulose 1% in dry eye. Indian J. Clin. Exp. Ophthalmol. 2021, 7, 302–307. [Google Scholar]
- Findlay, Q.; Reid, K. Dry eye disease: When to treat and when to refer. Aust. Prescr. 2018, 41, 160–163. [Google Scholar] [CrossRef]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Carl Heneghan Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; Hodgkinson, M. The 2011 Oxford CEBM Levels of Evidence. Oxf. Cent. Evid.-Based Med. 2011. Available online: https://www.cebm.net/index.aspx?o=5653 (accessed on 5 May 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Walt, J.G.; Rowe, M.M.; Stern, K. Evaluating the functional impact of dry eye: The Ocular Surface Disease Index. Drug. Inf. J. 1997, 31, b5. [Google Scholar]
- Wang, S.Q.; Zhang, L.W.; Wei, P.; Hua, H. Is hydroxychloroquine effective in treating primary Sjogren’s syndrome: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 186. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, S.; Asfuroğlu, E.; Bicakcigil, M.; Toker, E. Hydroxychloroquine improves dry eye symptoms of patients with primary Sjogren’s syndrome. Rheumatol. Int. 2011, 31, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Cankaya, H.; Alpöz, E.; Karabulut, G.; Güneri, P.; Boyacioglu, H.; Kabasakal, Y. Effects of hydroxychloroquine on salivary flow rates and oral complaints of Sjögren patients: A prospective sample study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2010, 110, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Yam, J.C.; Kwok, A.K. Ocular toxicity of hydroxychloroquine. Hong Kong Med. J. 2006, 12, 294–304. [Google Scholar] [PubMed]
- Fiehn, C.; Ness, T.; Weseloh, C.; Specker, C.; Hadjiski, D.; Detert, J.; Krüger, K. Safety management in treatment with antimalarials in rheumatology. Interdisciplinary recommendations on the basis of a systematic literature review. Z. Rheumatol. 2021, 80, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Blignaut, M.; Espach, Y.; van Vuuren, M.; Dhanabalan, K.; Huisamen, B. Revisiting the cardiotoxic effect of chloroquine. Cardiovasc. Drugs Ther. 2019, 33, 1–11. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Journal | Follow-Up (Weeks) | Patients (n) | Treatment | Dose | Mean Age | Women (%) |
|---|---|---|---|---|---|---|---|
| Bhavsar et al., 2011 [19] | Int. J. Biomed. Adv. Res. | 4 | 82 | CQ (eye drops) | 0.03% | 53.4 | 71 |
| 85 | Control group (artificial tears) | 53.4 | 71 | ||||
| Bodewes et al., 2020 [43] | Rheumatology (Oxford) | 24 | 37 | HCQ (oral) | 400 mg daily | ||
| 40 | Control group (placebo) | ||||||
| Gottenberg et al., 2014 [41] | J. Am. Med. Ass. | 48 | 44 | HCQ (oral) | 400 mg daily | 56.3 | 89 |
| 48 | Control group (placebo) | 55.6 | 94 | ||||
| Tyagi et al., 2021 [44] | Ind. J. Clin. Exp. Ophthalm | 12 | 50 | CQ (eye drops) | 0.03% | 51.0 | |
| 50 | Control group (artificial tears) | 51.0 | |||||
| Yoon et al., 2016 [40] | J. Korean. Med. Sci. | 12 | 11 | HCQ (oral) | 300 mg daily | 59.4 | 100 |
| 15 | Control group (placebo) | 55.0 | 100 |
| Endpoint | Baseline | Last FU | MD | SE | 95% CI | T Value | p |
|---|---|---|---|---|---|---|---|
| Tear breakup time | 4.6 ± 1.6 | 6.9 ± 6.6 | 2.3 | 0.453 | 1.40 to 3.19 | 5.077 | <0.0001 |
| OSDI | 57.8 ± 5.2 | 22.2 ± 7.8 | −35.6 | 0.621 | −36.81 to −34.38 | −57.357 | <0.0001 |
| Schirmer I test | 7.4 ± 3.9 | 10.0 ± 5.1 | 2.6 | 0.424 | 1.76 to 3.43 | 6.128 | <0.0001 |
| Corneal staining | 3.2 ± 0.02 | 1.5 ± 1.5 | −1.7 | 0.1 | −1.89 to −1.50 | −16.96 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prinz, J.; Maffulli, N.; Fuest, M.; Walter, P.; Hildebrand, F.; Migliorini, F. Chloroquine and Hydroxychloroquine in the Treatment of Dry Eye Disease. Diseases 2023, 11, 85. https://doi.org/10.3390/diseases11020085
Prinz J, Maffulli N, Fuest M, Walter P, Hildebrand F, Migliorini F. Chloroquine and Hydroxychloroquine in the Treatment of Dry Eye Disease. Diseases. 2023; 11(2):85. https://doi.org/10.3390/diseases11020085
Chicago/Turabian StylePrinz, Julia, Nicola Maffulli, Matthias Fuest, Peter Walter, Frank Hildebrand, and Filippo Migliorini. 2023. "Chloroquine and Hydroxychloroquine in the Treatment of Dry Eye Disease" Diseases 11, no. 2: 85. https://doi.org/10.3390/diseases11020085
APA StylePrinz, J., Maffulli, N., Fuest, M., Walter, P., Hildebrand, F., & Migliorini, F. (2023). Chloroquine and Hydroxychloroquine in the Treatment of Dry Eye Disease. Diseases, 11(2), 85. https://doi.org/10.3390/diseases11020085