
Spatial Analysis of Schistosomiasis in Hunan and Jiangxi Provinces in the People’s Republic of China

 ,
,  ,
,  , , ,
, , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Ethics
2.3. Data Sources
2.4. Statistical Analysis
2.5. Geospatial Analysis
2.6. Spatial Prediction
3. Results
3.1. Prevalence of Schistosomiasis at the Province and Village Levels
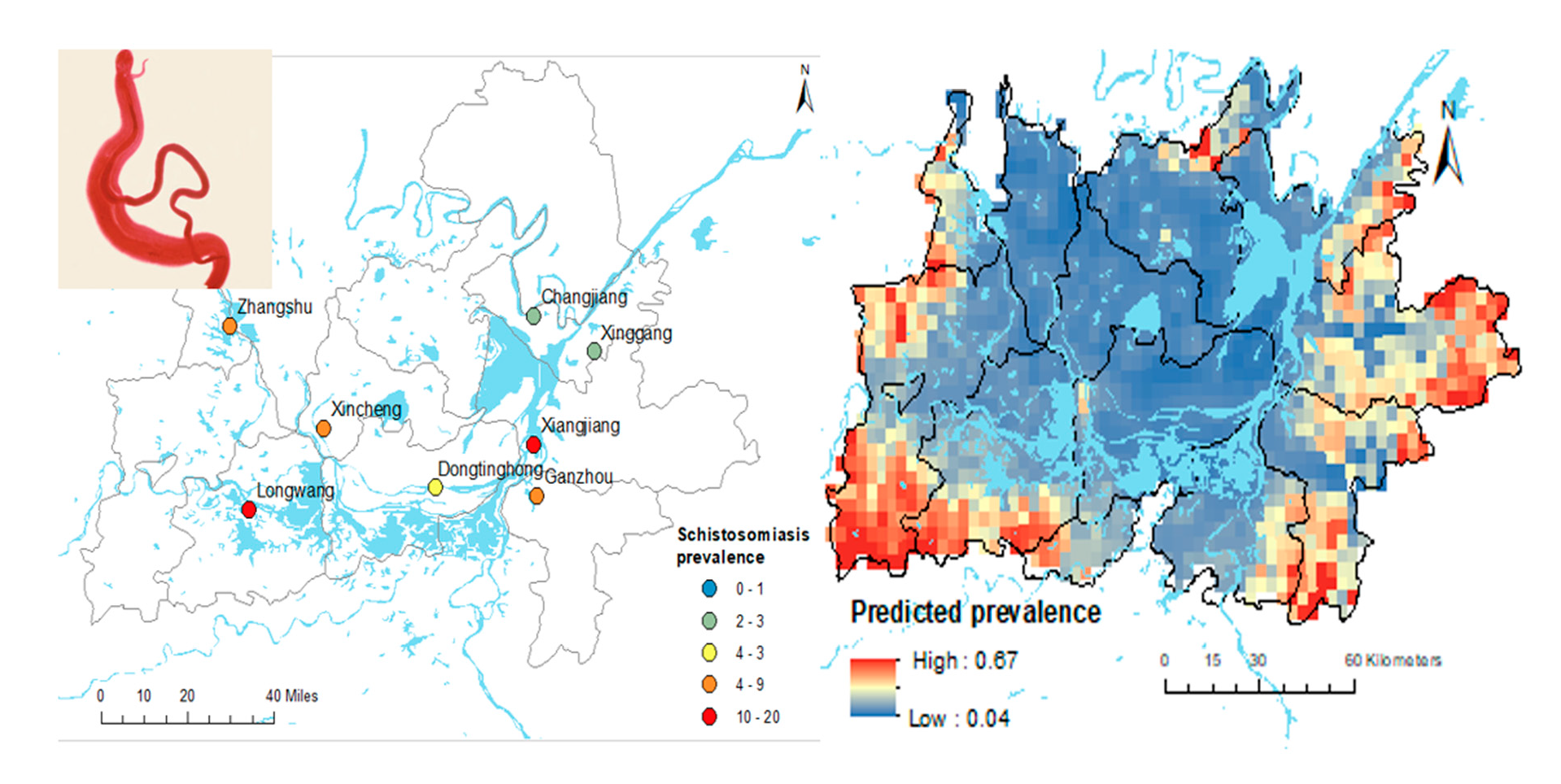
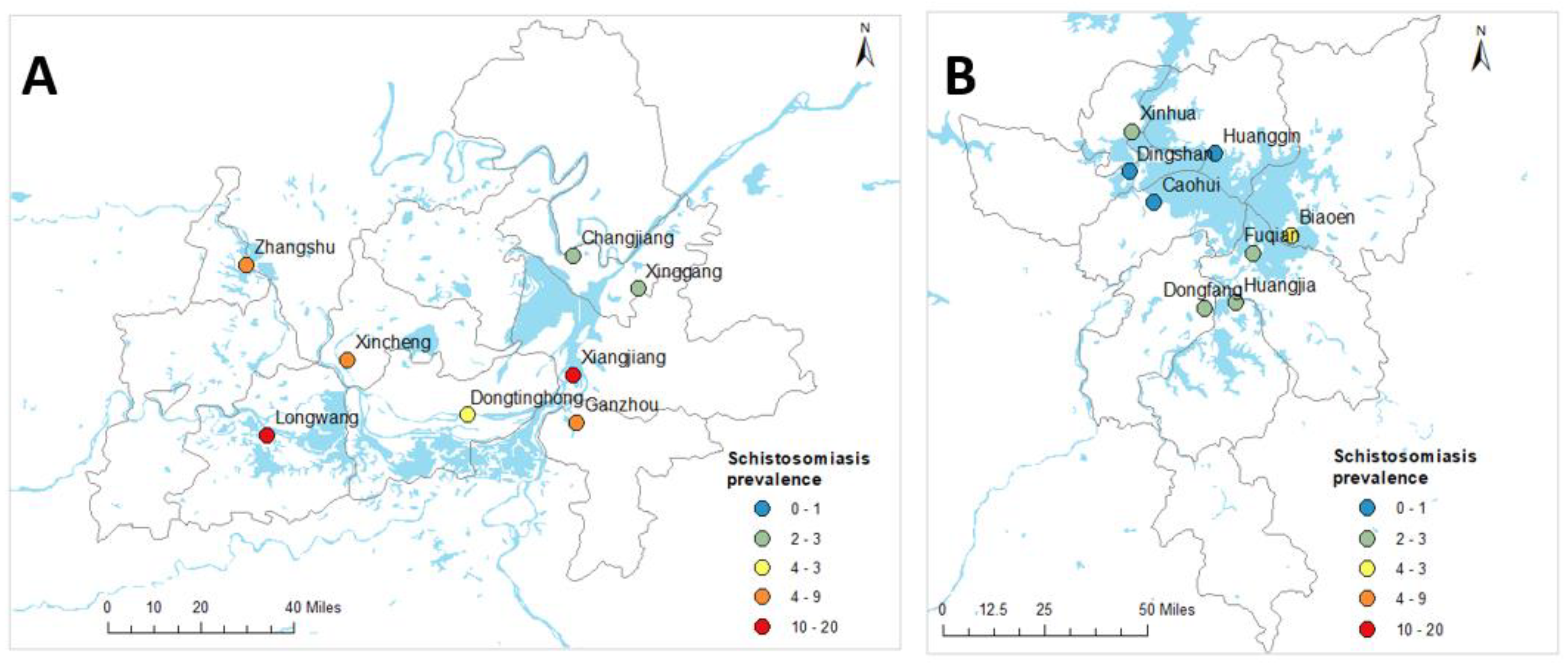
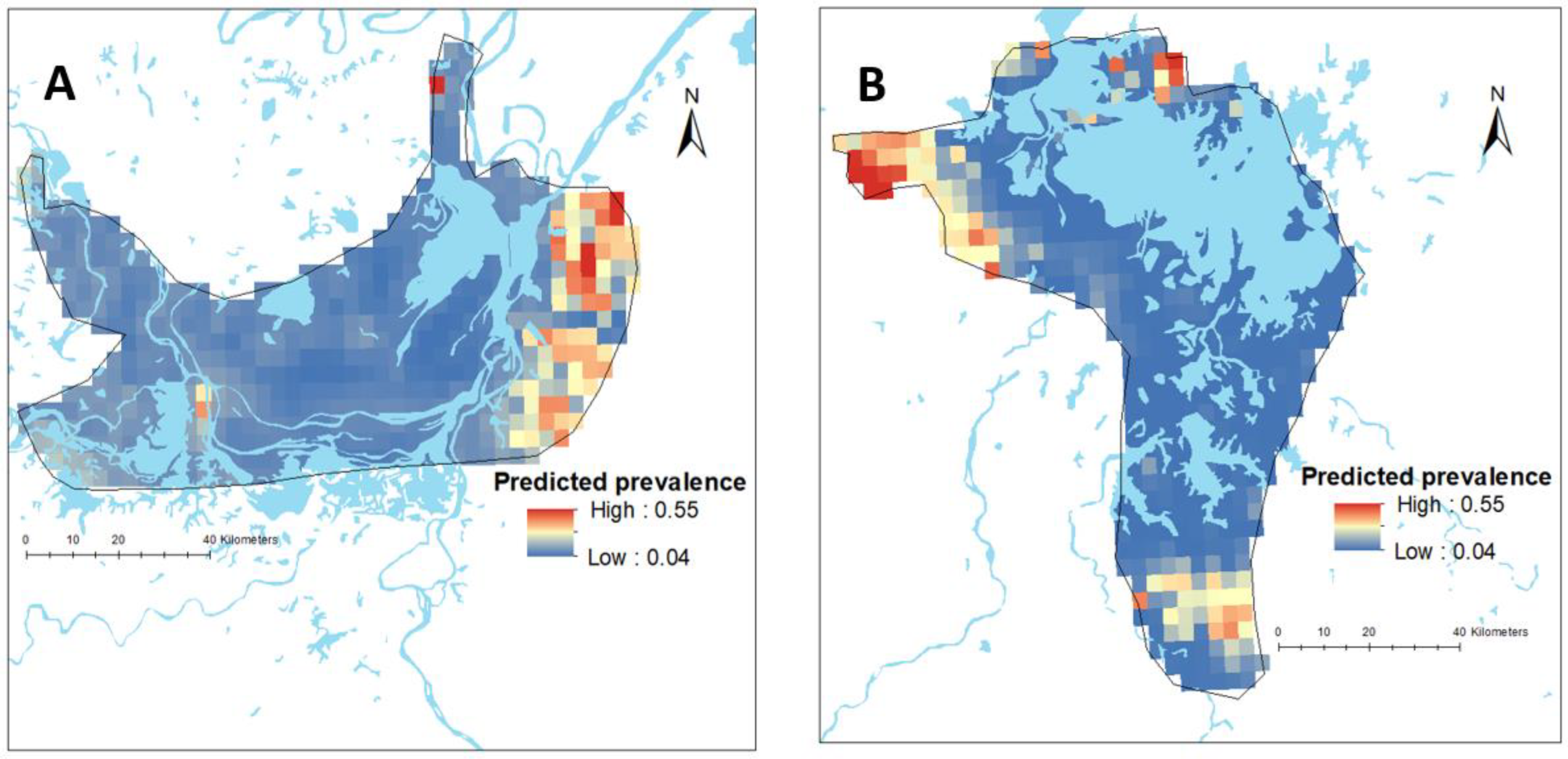
3.2. Spatial Distribution of Schistosomiasis
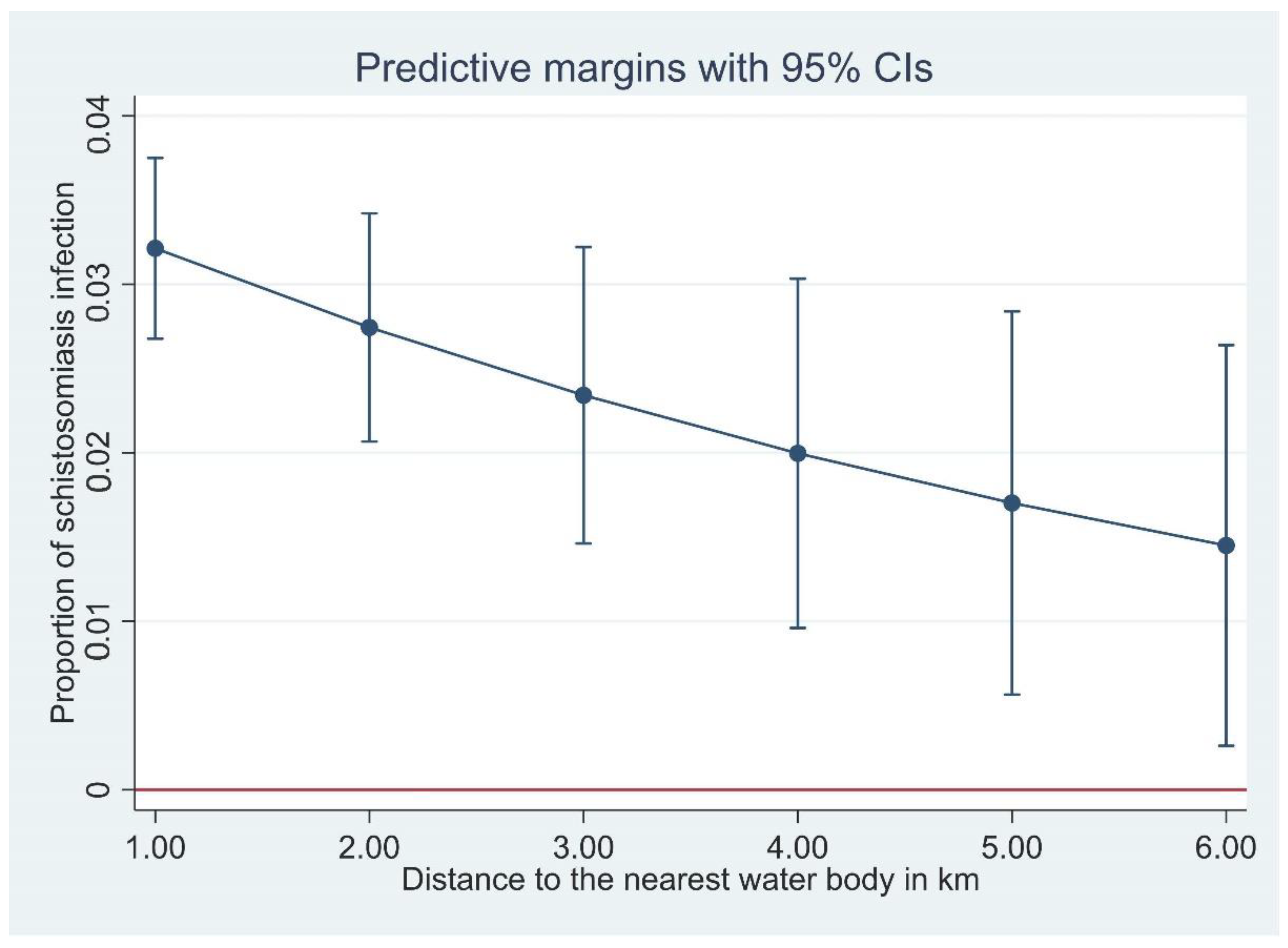
3.3. Ecological-Level Factors Associated with the Spatial Distribution of Schistosomiasis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gryseels, B.; Polman, K.; Clerinx, J.; Kestens, L. Human schistosomiasis. Lancet 2006, 368, 1106–1118. [Google Scholar] [CrossRef]
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Lai, Y.-S.; Biedermann, P.; Ekpo, U.F.; Garba, A.; Mathieu, E.; Midzi, N.; Mwinzi, P.; N’Goran, E.K.; Raso, G.; Assaré, R.K. Spatial distribution of schistosomiasis and treatment needs in sub-Saharan Africa: A systematic review and geostatistical analysis. Lancet Infect. Dis. 2015, 15, 927–940. [Google Scholar] [CrossRef]
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef]
- Assaré, R.K.; Lai, Y.-S.; Yapi, A.; Tian-Bi, Y.-N.T.; Ouattara, M.; Yao, P.K.; Knopp, S.; Vounatsou, P.; Utzinger, J.; N’Goran, E.K. The spatial distribution of Schistosoma mansoni infection in four regions of western Côte d’Ivoire. Geospat. Health 2015, 10, 345. [Google Scholar] [CrossRef][Green Version]
- Gordon, C.A.; Williams, G.M.; Gray, D.J.; Clements, A.C.; Zhou, X.-N.; Li, Y.; Utzinger, J.; Kurscheid, J.; Forsyth, S.; Alene, K.A. Schistosomiasis in the People’s Republic of China—Down but not out. Parasitology 2022, 149, 218–233. [Google Scholar] [CrossRef]
- Chadeka, E.A.; Nagi, S.; Sunahara, T.; Cheruiyot, N.B.; Bahati, F.; Ozeki, Y.; Inoue, M.; Osada-Oka, M.; Okabe, M.; Hirayama, Y. Spatial distribution and risk factors of Schistosoma haematobium and hookworm infections among schoolchildren in Kwale, Kenya. PLoS Negl. Trop. Dis. 2017, 11, e0005872. [Google Scholar] [CrossRef]
- da Paz, W.S.; Duthie, M.S.; de Jesus, A.R.; de Araújo, K.C.G.M.; Dos Santos, A.D.; Bezerra-Santos, M. Population-based, spatiotemporal modeling of social risk factors and mortality from schistosomiasis in Brazil between 1999 and 2018. Acta Trop. 2021, 218, 105897. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-Y.; Huang, X.-B.; Xiao, Y.; Jiang, Y.; Shan, X.-W.; Zhang, J.; Cai, S.-X.; Liu, J.-B. Spatial analysis of schistosomiasis in Hubei Province, China: A GIS-based analysis of schistosomiasis from 2009 to 2013. PLoS ONE 2015, 10, e0118362. [Google Scholar]
- Hu, Y.; Zhang, Z.; Chen, Y.; Wang, Z.; Gao, J.; Tao, B.; Jiang, Q.; Jiang, Q. Spatial pattern of schistosomiasis in Xingzi, Jiangxi Province, China: The effects of environmental factors. Parasit. Vectors 2013, 6, 214. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Cai, S.-X.; Liu, J.-B.; Tu, Z.-W.; Xia, J.; Shan, X.-W.; Qiu, J.; Jiang, Y.; Xiao, Y.; Tang, L. A spatial analysis of human Schistosoma japonicum infections in Hubei, China, during 2009–2014. Parasit. Vectors 2016, 9, 529. [Google Scholar] [CrossRef]
- Zhou, Y.-B.; Liang, S.; Chen, G.-X.; Rea, C.; Han, S.-M.; He, Z.-G.; Li, Y.-P.; Wei, J.-G.; Zhao, G.-M.; Jiang, Q.-W. Spatial-temporal variations of Schistosoma japonicum distribution after an integrated national control strategy: A cohort in a marshland area of China. BMC Public Health 2013, 13, 297. [Google Scholar] [CrossRef] [PubMed]
- M’Bra, R.K.; Kone, B.; Yapi, Y.G.; Silué, K.D.; Sy, I.; Vienneau, D.; Soro, N.; Cissé, G.; Utzinger, J. Risk factors for schistosomiasis in an urban area in northern Côte d’Ivoire. Infec. Dis. Pov. 2018, 7, 47. [Google Scholar] [CrossRef]
- Clements, A.C.A.; Lwambo, N.J.S.; Blair, L.; Nyandindi, U.; Kaatano, G.; Kinung’hi, S.; Webster, J.P.; Fenwick, A.; Brooker, S. Bayesian spatial analysis and disease mapping: Tools to enhance planning and implementation of a schistosomiasis control programme in Tanzania. Trop. Med. Int. Health 2006, 11, 490–503. [Google Scholar] [CrossRef]
- WHO. WHO Guideline on Control and Elimination of Human Schistosomiasis; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Sokolow, S.H.; Wood, C.L.; Jones, I.J.; Lafferty, K.D.; Kuris, A.M.; Hsieh, M.H.; De Leo, G.A. To reduce the global burden of human schistosomiasis, use ‘old fashioned’ snail control. Trends Parasitol. 2018, 34, 23–40. [Google Scholar] [CrossRef]
- Kokaliaris, C.; Garba, A.; Matuska, M.; Bronzan, R.N.; Colley, D.G.; Dorkenoo, A.M.; Ekpo, U.F.; Fleming, F.M.; French, M.D.; Kabore, A. Effect of preventive chemotherapy with praziquantel on schistosomiasis among school-aged children in sub-Saharan Africa: A spatiotemporal modelling study. Lancet Infect. Dis. 2022, 22, 136–149. [Google Scholar] [CrossRef]
- Deol, A.K.; Fleming, F.M.; Calvo-Urbano, B.; Walker, M.; Bucumi, V.; Gnandou, I.; Tukahebwa, E.M.; Jemu, S.; Mwingira, U.J.; Alkohlani, A. Schistosomiasis—Assessing progress toward the 2020 and 2025 global goals. N. Engl. J. Med. 2019, 381, 2519–2528. [Google Scholar] [CrossRef]
- Li, Q.; Xu, J.; Li, S.; Utzinger, J.; McManus, D.P.; Zhou, X. Short-, mid-, and long term epidemiological and economic effects of the World Bank Loan Project on schistosomiasis control in the People’s Republic of China. Diseases 2022, 10, 84. [Google Scholar] [CrossRef]
- Lehner, B.; Döll, P. Development and validation of a global database of lakes, reservoirs and wetlands. J. Hydrol. 2004, 296, 1–22. [Google Scholar] [CrossRef]
- Balen, J.; Liu, Z.-C.; McManus, D.P.; Raso, G.; Utzinger, J.; Xiao, S.-Y.; Yu, D.-B.; Zhao, Z.-Y.; Li, Y.-S. Health access livelihood framework reveals potential barriers in the control of Schistosomiasis in the Dongting Lake Area of Hunan Province, China. PLoS Negl. Trop. Dis. 2013, 7, e2350. [Google Scholar] [CrossRef]
- Banerjee, S. On geodetic distance computations in spatial modeling. Biometrics 2005, 61, 617–625. [Google Scholar] [CrossRef]
- Fick, S.E.; Hijmans, R.J. WorldClim 2: New 1 km spatial resolution climate surfaces for global land areas. Int. J. Climatol. 2017, 37, 4302–4315. [Google Scholar] [CrossRef]
- Farr, T.G.; Kobrick, M. Shuttle Radar Topography Mission produces a wealth of data. Eos Trans. Am. Geophys. Union 2000, 81, 583–585. [Google Scholar] [CrossRef]
- Hijmans, R.J.; Guarino, L.; Bussink, C.; Mathur, P.; Cruz, M.; Barrentes, I.; Rojas, E. Diva-gis Manual Version 5.0. 2004. Available online: http://www.diva-gis.org (accessed on 8 August 2022).
- Weiss, D.; Nelson, A.; Vargas-Ruiz, C.; Gligorić, K.; Bavadekar, S.; Gabrilovich, E.; Bertozzi-Villa, A.; Rozier, J.; Gibson, H.; Shekel, T. Global maps of travel time to healthcare facilities. Nat. Med. 2020, 26, 1835–1838. [Google Scholar] [CrossRef]
- Areas, G.A. GADM Database of Global Administrative Areas, version 2.8.; University of California: Berkeley, CA, USA, 2015. Available online: http://www.gadm.org2018 (accessed on 5 May 2021).
- Diggle, P.J.; Tawn, J.A.; Moyeed, R. Model-based geostatistics. J. R. Stat. Soc. Ser. C Appl. Stat. 1998, 47, 299–350. [Google Scholar] [CrossRef]
- Rue, H.; Martino, S.; Chopin, N. Approximate Bayesian inference for latent Gaussian models by using integrated nested Laplace approximations. J. R. Stat. Soc. Ser. B Stat. Methodol. 2009, 71, 319–392. [Google Scholar] [CrossRef]
- Lindgren, F.; Rue, H.; Lindström, J. An explicit link between Gaussian fields and Gaussian Markov random fields: The stochastic partial differential equation approach. J. R. Stat. Soc. Ser. B Stat. Methodol. 2011, 73, 423–498. [Google Scholar] [CrossRef]
- Fuglstad, G.-A.; Simpson, D.; Lindgren, F.; Rue, H. Constructing priors that penalize the complexity of Gaussian random fields. J. Am. Stat. Assoc. 2019, 114, 445–452. [Google Scholar] [CrossRef]
- Thomas, A.; Best, N.; Lunn, D.; Arnold, R.; Spiegelhalter, D. GeoBUGS User Manual; Medical Research Council Biostatistics Unit: Cambridge, UK, 2004. [Google Scholar]
- Lei, Z.L.; Zheng, H.; Zhang, L.J.; Zhu, R.; Xu, Z.M.; Xu, J.; Fu, Q.; Wang, Q.; Li, S.Z.; Zhou, X.N. Endemic status of schistosomiasis in People’s Republic of China in 2013. Chin. J. Schistosomiasis Control 2014, 26, 591–597. [Google Scholar]
- WHO. Progress Report 2001–2011 and Strategic Plan 2012–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Yang, G.-J.; Liu, L.; Zhu, H.-R.; Griffiths, S.M.; Tanner, M.; Bergquist, R.; Utzinger, J.; Zhou, X.-N. China’s sustained drive to eliminate neglected tropical diseases. Lancet Infect. Dis. 2014, 14, 881–892. [Google Scholar] [CrossRef]
- Li, F.-Y.; Hou, X.-Y.; Tan, H.-Z.; Williams, G.M.; Gray, D.J.; Gordon, C.A.; Kurscheid, J.; Clements, A.C.A.; Li, Y.-S.; McManus, D.P. Current status of schistosomiasis control and prospects for elimination in the Dongting lake region of the People’s Republic of China. Front. Immunol. 2020, 11, 574136. [Google Scholar] [CrossRef]
- Guangping, L.; Xinling, Y.; Xiang, W.; Zhengyuan, Z.; Chamon; Yi, D.; Jie, Z.; Zhenhua, L.; Qiong, J.; Jun, W. Epidemiological analysis of national schistosomiasis surveillance sites in Hunan Province from 2015 to 2019. Chin. J. Schistosomiasis Control 2020, 32, 242–247. [Google Scholar]
- Yuan, M.; Li, Y.; Lv, S.; Hu, F.; Hang, C.; Chen, Z.; Lin, D.; Dang, H.; Lv, S. Endemic status of schistosomiasis in national surveillance sites in Jiangxi Province from 2015 to 2018. Chin. J. Parasitol. Parasit. Dis. 2019, 37, 652–657. [Google Scholar]
- Raso, G.; Li, Y.S.; Zhao, Z.Y.; Balen, J.; Williams, G.M.; McManus, D.P. Spatial distribution of human Schistosoma japonicum infections in the Dongting Lake Region, China. PLoS ONE 2009, 4, e6947. [Google Scholar] [CrossRef]
- WHO. Expert Consultation to Accelerate Elimination of Asian Schistosomiasis; Meeting Report WHO; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- McManus, D.P.; Gray, D.J.; Li, Y.; Feng, Z.; Williams, G.M.; Stewart, D.; Rey-Ladino, J.; Ross, A.G. Schistosomiasis in the People’s Republic of China: The era of the three gorges dam. Clin. Microbiol. Rev. 2010, 23, 442–466. [Google Scholar] [CrossRef]
- Zhou, X.N.; Bergquist, R.; Leonardo, L.; Yang, G.J.; Yang, K.; Sudomo, M.; Olveda, R. Schistosomiasis japonica control and research needs. Adv. Parasitol. 2010, 72, 145–178. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Hunan Province | Jiangxi Province | Total |
|---|---|---|---|
| Total number of households with GPS coordinates | 1099 | 1250 | 2349 |
| Number of administrative villages | 8 | 8 | 16 |
| Number of household members | 4367 | 5657 | 10,024 |
| Number with Schistosoma japonicum infection | 141 | 33 | 174 |
| Number of male participants | 989 | 1061 | 2050 |
| Number of female participants | 916 | 958 | 1874 |
| Age of the survey participants (year), mean (SD) | 46.4 (10.5) | 47.8 (6.9) | 47.2 (12.3) |
| Distance from household to nearest waterbody (km), mean (SD) | 1.22 (1.55) | 0.73 (0.94) | 0.96 (1.28) |
| Walking distance to health facilities (min), mean (SD) | 108 (108) | 143 (107) | 126 (109) |
| Average monthly temperature (°C), mean (SD) | 17.2 (0.1) | 17.6 (0.1) | 17.4 (0.2) |
| Average monthly precipitation (mm), mean (SD) | 107.6 (3.1) | 129.4 (3.7) | 119.2 (11.4) |
| Average monthly solar radiation (kJ m−2 day−1), mean (SD) | 13,629 (87) | 14,703 (93) | 14,201 (544) |
| Elevation (m), mean (SD) | 34.3 (5.7) | 19.8 (17.5) | 26.6 (15.2) |
| Total Number | Number Positive | Percentage Positive | 95% CI * | ||
|---|---|---|---|---|---|
| Province | Hunan | 1099 | 141 | 12.8 | 10.8–14.8 |
| Jiangxi | 1250 | 33 | 2.6 | 1.8–3.5 | |
| Combined | 2349 | 174 | 7.4 | 6.3–7.4 | |
| Hunan | Changjiang | 98 | 7 | 7.1 | 2.0–12. |
| Dongtinghong | 175 | 8 | 4.6 | 1.4–7.7 | |
| Ganzhou | 197 | 23 | 11.7 | 7.2–16.2 | |
| Longwang | 104 | 29 | 27.9 | 19.1–36.6 | |
| Xiangjiang | 61 | 24 | 39.3 | 26.7–52.0 | |
| Xincheng | 173 | 23 | 13.3 | 8.2–18.4 | |
| Xinggang | 118 | 6 | 5.1 | 1.1–9.1 | |
| Zhangshu | 173 | 21 | 12.1 | 7.2–17.1 | |
| Jiangxi | Biaoen | 146 | 8 | 5.5 | 1.7–9.2 |
| Caohui | 118 | 3 | 2.5 | 0–5.4 | |
| Dingshan | 132 | 0 | 0.0 | na | |
| Dongfang | 183 | 7 | 3.8 | 1.0–6.6 | |
| Fuqian | 156 | 4 | 2.6 | 0–5.1 | |
| Huanggin | 172 | 2 | 1.2 | 0–2.8 | |
| Huangjia | 222 | 6 | 2.7 | 0.6–4.9 | |
| Xinhua | 121 | 3 | 2.5 | 0–5.3 |
| Variable | Hunan Province | Jiangxi Province |
|---|---|---|
| Regression Coefficients (95% CrI) | Regression Coefficients (95% CrI) | |
| Distance to waterbody | −2.367 (−4.217, −0.697) | −5.471 (−11.332, −0.507) |
| Distance to health facilities | −0.424 (−0.637, −0.236) | −0.056 (−0.415, 0.269) |
| Altitude | −4.947 (−7.228, −2.727) | 5.537 (−0.996, 10.014) |
| Temperature | −0.127 (−0.448, 0.198) | 2.664 (0.964, 4.360) |
| Intercept | −4.789 (−6.077, −3.667) | −6.405 (−10.387, −3.203) |
| Variable | Hunan Province | Jiangxi Province |
|---|---|---|
| Regression Coefficients (95% CrI) | Regression Coefficients (95% CrI) | |
| Distance to waterbody | −1.158 (−2.104, −0.116) | 2.821 (−3.508, 8.722) |
| Distance to health facilities | −0.079 (−0.301, 0.101) | 0.291 (−0.011, 0.621) |
| Altitude | 2.712 (−7.542, 11.409) | 15.888 (−12.109, 41.995) |
| Temperature | 0.320 (−0.477, 0.901) | −4.359 (−9.641, −0.055) |
| Intercept | −1.597 (−8.544, 3.860) | 4.383 (−9.716, 17.014) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alene, K.A.; Gordon, C.A.; Clements, A.C.A.; Williams, G.M.; Gray, D.J.; Zhou, X.-N.; Li, Y.; Utzinger, J.; Kurscheid, J.; Forsyth, S.; et al. Spatial Analysis of Schistosomiasis in Hunan and Jiangxi Provinces in the People’s Republic of China. Diseases 2022, 10, 93. https://doi.org/10.3390/diseases10040093
Alene KA, Gordon CA, Clements ACA, Williams GM, Gray DJ, Zhou X-N, Li Y, Utzinger J, Kurscheid J, Forsyth S, et al. Spatial Analysis of Schistosomiasis in Hunan and Jiangxi Provinces in the People’s Republic of China. Diseases. 2022; 10(4):93. https://doi.org/10.3390/diseases10040093
Chicago/Turabian StyleAlene, Kefyalew Addis, Catherine A. Gordon, Archie C. A. Clements, Gail M. Williams, Darren J. Gray, Xiao-Nong Zhou, Yuesheng Li, Jürg Utzinger, Johanna Kurscheid, Simon Forsyth, and et al. 2022. "Spatial Analysis of Schistosomiasis in Hunan and Jiangxi Provinces in the People’s Republic of China" Diseases 10, no. 4: 93. https://doi.org/10.3390/diseases10040093
APA StyleAlene, K. A., Gordon, C. A., Clements, A. C. A., Williams, G. M., Gray, D. J., Zhou, X.-N., Li, Y., Utzinger, J., Kurscheid, J., Forsyth, S., Zhou, J., Li, Z., Li, G., Lin, D., Lou, Z., Li, S., Ge, J., Xu, J., Yu, X., ... McManus, D. P. (2022). Spatial Analysis of Schistosomiasis in Hunan and Jiangxi Provinces in the People’s Republic of China. Diseases, 10(4), 93. https://doi.org/10.3390/diseases10040093