
The Menace of Candida auris Epidemic Amidst the COVID-19 Pandemic: A Systematic Review

 ,
,
Abstract
:1. Introduction
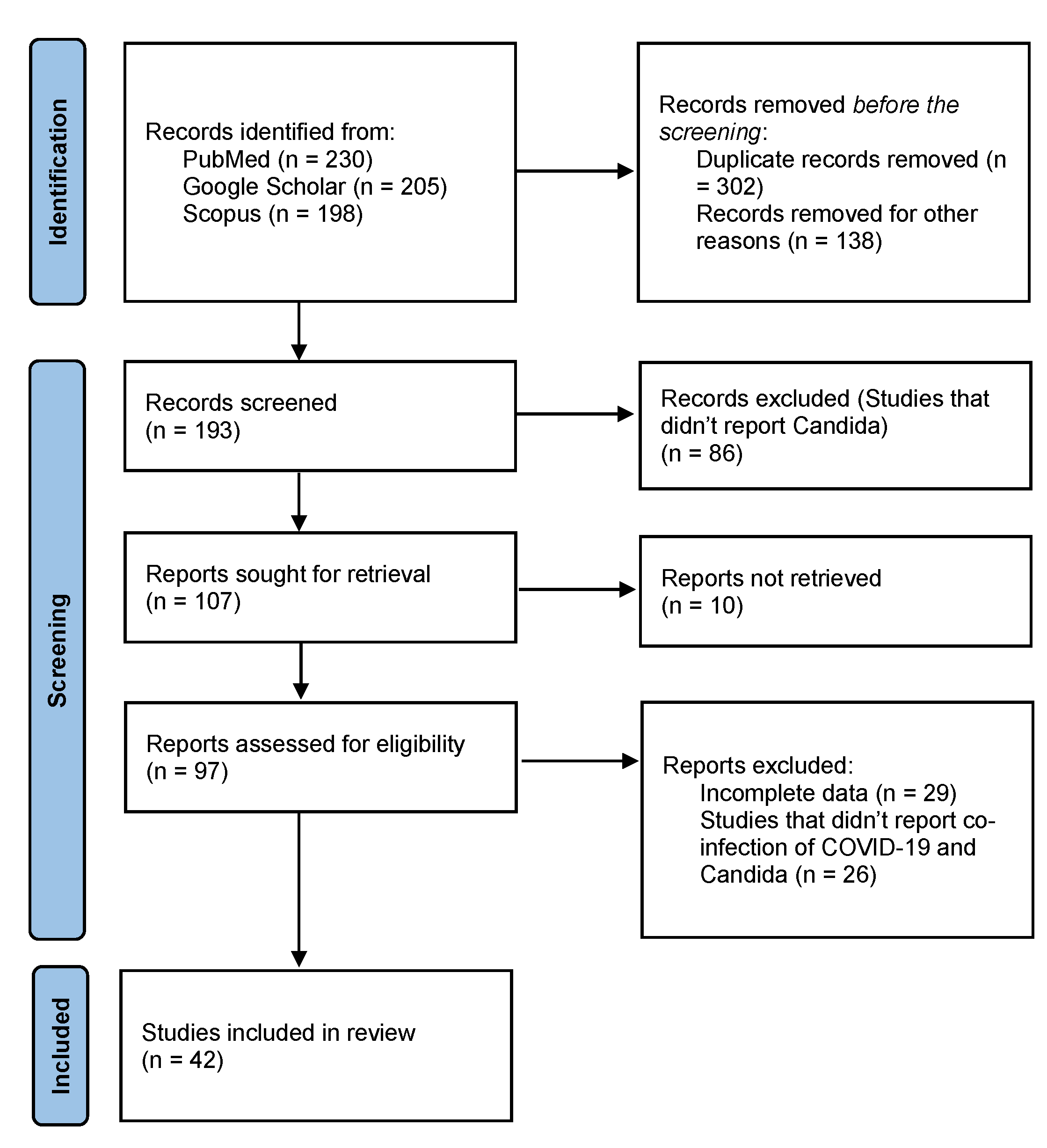
2. Methods
3. Results
4. COVID and Co-Infections
5. Types of Invasive Mycoses
6. Epidemiology
7. Pathophysiology
7.1. Pathophysiology of SARS-CoV-2
7.2. Pathophysiology of Candida auris
8. Risk Factors
9. Clinical Presentation and Complications
10. Diagnosis
11. Treatment and Prevention
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Meis, J.F.; Chowdhary, A. Candida auris: A global fungal public health threat. Lancet Infect. Dis. 2018, 18, 1298–1299. [Google Scholar] [CrossRef]
- Superinfections and Coinfections in COVID-19. Available online: https://www.medpagetoday.com/infectiousdisease/covid19/86192 (accessed on 24 May 2022).
- Chowdhary, A.; Sharma, A. The lurking scourge of multi-drug resistant Candida auris in times of COVID-19 pandemic. J. Glob. Antimicrob. Resist. 2020, 22, 175. [Google Scholar] [CrossRef]
- Chowdhary, A.; Tarai, B.; Singh, A.; Sharma, A. Multidrug-resistant Candida auris infections in critically ill coronavirus disease patients, India, April–July 2020. Emerg. Infect. Dis. 2020, 26, 2694. [Google Scholar] [CrossRef] [PubMed]
- Ostrowsky, B.; Greenko, J.; Adams, E.; Quinn, M.; O’Brien, B.; Chaturvedi, V.; Berkow, E.; Vallabhaneni, S.; Forsberg, K.; Chaturvedi, S.; et al. Candida auris isolates resistant to three classes of antifungal medications—New York, 2019. Morb. Mortal. Wkly. Rep. 2020, 69, 6. [Google Scholar] [CrossRef]
- Rodríguez, J.Y.; Morales-López, S.E.; Rodríguez, G.J.; Álvarez-Moreno, C.A.; Esquea, K.; Pinzon, H.; Ramirez, L.R.; Moreno, L.; Ocampo, W.; Cepeda, M.L. Case series study of melioidosis, Colombia. Emerg. Infect. Dis. 2019, 25, 1531. [Google Scholar] [CrossRef]
- Schauwvlieghe, A.F.; Rijnders, B.J.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Villanueva-Lozano, H.; Treviño-Rangel, R.D.J.; González, G.M.; Ramírez-Elizondo, M.T.; Lara-Medrano, R.; Aleman-Bocanegra, M.C.; Guajardo-Lara, C.E.; Gaona-Chávez, N.; Castilleja-Leal, F.; Torre-Amione, G.; et al. Outbreak of Candida auris infection in a COVID-19 hospital in Mexico. Clin. Microbiol. Infect. 2021, 27, 813–816. [Google Scholar] [CrossRef]
- Alvarado, M.; Bartolomé Álvarez, J.; Lockhart, S.R.; Valentín, E.; Ruiz-Gaitán, A.C.; Eraso, E.; de Groot, P.W. Identification of Candida auris and related species by multiplex PCR based on unique GPI protein-encoding genes. Mycoses 2021, 64, 194–202. [Google Scholar] [CrossRef]
- Hernando-Ortiz, A.; Mateo, E.; Perez-Rodriguez, A.; De Groot, P.W.; Quindós, G.; Eraso, E. Virulence of Candida auris from different clinical origins in Caenorhabditis elegans and Galleria mellonella host models. Virulence 2021, 12, 1063–1075. [Google Scholar] [CrossRef]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A.; Rose, L.J.; Litvintseva, A.P. Survival, persistence, and isolation of the emerging multidrug-resistant pathogenic yeast Candida auris on a plastic health care surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Khan, Z.; Al-Sweih, N.; Alfouzan, W.; Joseph, L. Candida auris in various hospitals across Kuwait and their susceptibility and molecular basis of resistance to antifungal drugs. Mycoses 2020, 63, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 21, 339. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Parrill, A.; Tsao, T.; Dong, V.; Huy, N.T. SARS-CoV-2-induced immunodysregulation and the need for higher clinical suspicion for co-infection and secondary infection in COVID-19 patients. J. Microbiol. Immunol. Infect. 2021, 54, 105–108. [Google Scholar] [CrossRef]
- Chen, X.; Liao, B.; Cheng, L.; Peng, X.; Xu, X.; Li, Y.; Hu, T.; Li, J.; Zhou, X.; Ren, B. The microbial co-infection in COVID-19. Appl. Microbiol. Biotechnol. 2020, 11, 7777–7785. [Google Scholar] [CrossRef]
- Saeed, N.K.; Al-Khawaja, S.; Alsalman, J.; Almusawi, S.; Albalooshi, N.A.; Al-Biltagi, M. Bacterial co-infection in patients with SARS-CoV-2 in the Kingdom of Bahrain. World J. Virol. 2021, 10, 168. [Google Scholar] [CrossRef]
- Ramos-Martinez, A.; Fernández-Cruz, A.; Domínguez, F.; Forteza, A.; Cobo, M.; Sánchez-Romero, I.; Asensio, A. Hospital-acquired infective endocarditis during COVID-19 pandemic. Infect. Prev. Pract. 2020, 2, 100080. [Google Scholar] [CrossRef]
- Lima, W.G.; Brito, J.C.; da Cruz Nizer, W.S. Ventilator-associated pneumonia (V.A.P.) caused by carbapenem-resistant Acinetobacter baumannii in patients with COVID-19: Two problems, one solution? Med. Hypotheses 2020, 144, 110139. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, M.A.; Kaur, J.; Wani, F.; Kichloo, A.; Bhanot, R. Renal transplant recipient with concurrent COVID-19 and Stenotrophomonas maltophilia pneumonia treated with trimethoprim/sulfamethoxazole leading to acute kidney injury: A therapeutic dilemma. Am. J. Case Rep. 2020, 21, e926464-1. [Google Scholar] [CrossRef]
- Nori, P.; Cowman, K.; Chen, V.; Bartash, R.; Szymczak, W.; Madaline, T.; Katiyar, C.P.; Jain, R.; Aldrich, M.; Weston, G.; et al. Bacterial and fungal co-infections in COVID-19 patients hospitalized during the New York City pandemic surge. Infect. Control Hosp. Epidemiol. 2021, 42, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Senok, A.; Alfaresi, M.; Khansaheb, H.; Nassar, R.; Hachim, M.; Al Suwaidi, H.; Almansoori, M.; Alqaydi, F.; Afaneh, Z.; Mohamed, A.; et al. Coinfections in Patients Hospitalized with COVID-19: A Descriptive Study from the United Arab Emirates. Infect. Drug Resist. 2021, 14, 2289–2296. [Google Scholar] [CrossRef] [PubMed]
- Peci, A.; Tran, V.; Guthrie, J.L.; Li, Y.; Nelson, P.; Schwartz, K.L.; Eshaghi, A.; Buchan, S.A.; Gubbay, J.B. Prevalence of co-infections with respiratory viruses in individuals investigated for SARS-CoV-2 in Ontario, Canada. Viruses 2021, 13, 130. [Google Scholar] [CrossRef]
- Chen, T.; Song, J.; Liu, H.; Zheng, H.; Chen, C. Positive Epstein–Barr virus detection in coronavirus disease 2019 (COVID-19) patients. Sci. Rep. 2021, 11, 10902. [Google Scholar] [CrossRef] [PubMed]
- Kula, B.E.; Clancy, C.J.; Nguyen, M.H.; Schwartz, I.S. Invasive mould disease in fatal COVID-19: A systematic review of autopsies. Lancet Microbe 2021, 2, e405–e414. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef]
- Hashemi, S.A.; Safamanesh, S.; Ghasemzadeh-moghaddam, H.; Ghafouri, M.; Azimian, A. High prevalence of SARS-CoV-2 and influenza A virus (H1N1) co-infection in dead patients in Northeastern Iran. J. Med Virol. 2021, 93, 1008–1012. [Google Scholar] [CrossRef]
- Salehi, M.; Ahmadikia, K.; Mahmoudi, S.; Kalantari, S.; Jamalimoghadamsiahkali, S.; Izadi, A.; Kord, M.; Dehghan Manshadi, S.A.; Seifi, A.; Ghiasvand, F.; et al. Oropharyngeal candidiasis in hospitalized COVID-19 patients from Iran: Species identification and antifungal susceptibility pattern. Mycoses 2020, 63, 771–778. [Google Scholar] [CrossRef]
- Mulet Bayona, J.V.; Tormo Palop, N.; Salvador García, C.; Fuster Escrivá, B.; Chanzá Aviñó, M.; Ortega García, P.; Gimeno Cardona, C. Impact of the SARS-CoV-2 Pandemic in Candidaemia, Invasive Aspergillosis and Antifungal Consumption in a Tertiary Hospital. J. Fungi 2021, 7, 440. [Google Scholar] [CrossRef] [PubMed]
- Wee, L.E.; Ko, K.K.; Ho, W.Q.; Kwek, G.T.; Tan, T.T.; Wijaya, L. Community-acquired viral respiratory infections amongst hospitalized inpatients during a COVID-19 outbreak in Singapore: Co-infection and clinical outcomes. J. Clin. Virol. 2020, 128, 104436. [Google Scholar] [CrossRef] [PubMed]
- Hazra, A.; Collison, M.; Pisano, J.; Kumar, M.; Oehler, C.; Ridgway, J.P. Co-infections with SARS-CoV-2 and other respiratory pathogens. Infect. Control Hosp. Epidemiol. 2020, 41, 1228–1229. [Google Scholar] [CrossRef] [PubMed]
- Tadolini, M.; Codecasa, L.R.; García-García, J.M.; Blanc, F.X.; Borisov, S.; Alffenaar, J.W.; Andréjak, C.; Bachez, P.; Bart, P.A.; Belilovski, E.; et al. Active tuberculosis, sequelae and COVID-19 co-infection: First cohort of 49 cases. Eur. Respir. J. 2020, 56, 2001398. [Google Scholar] [CrossRef]
- Pemán, J.; Ruiz-Gaitán, A.; García-Vidal, C.; Salavert, M.; Ramírez, P.; Puchades, F.; García-Hita, M.; Alastruey-Izquierdo, A.; Quindós, G. Fungal co-infection in COVID-19 patients: Should we be concerned? Rev. Iberoam. De Micol. 2020, 37, 41–46. [Google Scholar] [CrossRef]
- Song, G.; Liang, G.; Liu, W. Fungal co-infections associated with global COVID-19 pandemic: A clinical and diagnostic perspective from China. Mycopathologia 2020, 31, 1–8. [Google Scholar] [CrossRef]
- Fungal Diseases and COVID-19|CDC, Cdc.gov. 2021. Available online: https://www.cdc.gov/fungal/covid-fungal.html (accessed on 26 August 2021).
- Singh, A.K.; Singh, R.; Joshi, S.R.; Misra, A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef]
- White, P.L.; Dhillon, R.; Cordey, A.; Hughes, H.; Faggian, F.; Soni, S.; Pandey, M.; Whitaker, H.; May, A.; Morgan, M.; et al. A national strategy to diagnose coronavirus disease 2019–associated invasive fungal disease in the intensive care unit. Clin. Infect. Dis. 2020, 73, e1634–e1644. [Google Scholar] [CrossRef]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2021, 64, 132–143. [Google Scholar] [CrossRef]
- Rabagliati, R.; Rodríguez, N.; Núñez, C.; Huete, A.; Bravo, S.; Garcia, P. COVID-19–Associated Mold Infection in Critically Ill Patients, Chile. Emerg. Infect. Dis. 2021, 27, 1454. [Google Scholar] [CrossRef]
- Martins, A.C.; Psaltikidis, E.M.; de Lima, T.C.; Fagnani, R.; Schreiber, A.Z.; de Oliveira Conterno, L.; Kamei, K.; Watanabe, A.; Trabasso, P.; Resende, M.R.; et al. COVID-19 and invasive fungal co-infections: A case series at a Brazilian referral hospital. J. Med Mycol. 2021, 31, 101175. [Google Scholar] [CrossRef] [PubMed]
- Cafardi, J.; Haas, D.; Lamarre, T.; Feinberg, J. Opportunistic fungal infection associated with COVID-19. In InOpen Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2021. [Google Scholar]
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol. Immunol. 2009, 53, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Bing, J.; Hu, T.; Ennis, C.L.; Nobile, C.J.; Huang, G. Candida auris: Epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020, 16, e1008921. [Google Scholar] [CrossRef] [PubMed]
- De Cássia Orlandi Sardi, J.; Silva, D.R.; Soares Mendes Giannini, M.J.; Rosalen, P.L. Candida auris: Epidemiology, risk factors, virulence, resistance, and therapeutic options. Microb. Pathog. 2018, 125, 116–121. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 64, 134–140. [Google Scholar] [CrossRef]
- Mathur, P.; Hasan, F.; Singh, P.K.; Malhotra, R.; Walia, K.; Chowdhary, A. Five-year profile of candidaemia at an Indian trauma centre: High rates of Candida auris blood stream infections. Mycoses 2018, 61, 674–680. [Google Scholar] [CrossRef]
- Eyre, D.W.; Sheppard, A.E.; Madder, H.; Moir, I.; Moroney, R.; Quan, T.P.; Jeffery, K.J. A Candida auris outbreak and its control in an intensive care setting. N. Engl. J. Med. 2018, 379, 1322–1331. [Google Scholar] [CrossRef]
- Allaw, F.; Kara Zahreddine, N.; Ibrahim, A.; Tannous, J.; Taleb, H.; Bizri, A.R.; Dbaibo, G.; Kanj, S.S. First Candida auris Outbreak during a COVID-19 Pandemic in a Tertiary-Care Center in Lebanon. Pathogens 2021, 10, 157. [Google Scholar] [CrossRef]
- Mason, R.J. Pathogenesis of COVID-19 from a Cell Biology Perspective. Eur. Respir. J. 2020, 55, 2000607. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. N. Eng. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and multiorgan response. Curr. Probl. Cardiol. 2020, 45, 100618. [Google Scholar] [CrossRef] [PubMed]
- Leisman, D.E.; Deutschman, C.S.; Legrand, M. Facing COVID-19 in the I.C.U.: Vascular dysfunction, thrombosis, and dysregulated inflammation. Intensive Care Med. 2020, 46, 1105–1108. [Google Scholar] [CrossRef] [PubMed]
- Teuwen, L.A.; Geldhof, V.; Pasut, A.; Carmeliet, P. Author Correction: COVID-19: The vasculature unleashed. Nat. Rev. Immunol. 2020, 20, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Jeffery-Smith, A.; Taori, S.K.; Schelenz, S.; Jeffery, K.; Johnson, E.M.; Borman, A. Candida auris Incident Management Team; Manuel, R.; Brown CS. Candida auris: A review of the literature. Clin. Microbiol. Rev. 2018, 31, e00029-17. [Google Scholar] [CrossRef]
- Day, A.M.; McNiff, M.M.; da Silva Dantas, A.; Gow, N.A.; Quinn, J. Hog1 regulates stress tolerance and virulence in the emerging fungal pathogen Candida auris. MSphere 2018, 3, e00506-18. [Google Scholar] [CrossRef]
- Pathirana, R.U.; Friedman, J.; Norris, H.L.; Salvatori, O.; McCall, A.D.; Kay, J.; Edgerton, M. Fluconazole-resistant Candida auris is susceptible to salivary histatin 5 killing and to intrinsic host defenses. Antimicrob. Agents Chemother. 2018, 62, e01872-17. [Google Scholar] [CrossRef]
- Spivak, E.S.; Hanson, K.E. Candida auris: An emerging fungal pathogen. J. Clin. Microbiol. 2018, 56, e01588-17. [Google Scholar] [CrossRef]
- Abastabar, M.; Haghani, I.; Ahangarkani, F.; Rezai, M.S.; Taghizadeh Armaki, M.; Roodgari, S.; Kiakojuri, K.; Al-Hatmi, A.M.S.; Meis, J.F.; Badali, H. Candida auris otomycosis in Iran and review of recent literature. Mycoses 2019, 62, 101–105. [Google Scholar] [CrossRef]
- Mirhendi, H.; Charsizadeh, A.; Aboutalebian, S.; Mohammadpour, M.; Nikmanesh, B.; de Groot, T.; Meis, J.F.; Badali, H. South Asian (Clade I) Candida auris meningitis in a pediatric patient in Iran with a review of the literature. Mycoses 2022, 65, 134–139. [Google Scholar] [CrossRef]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control 2016, 5, 35. [Google Scholar] [CrossRef] [Green Version]
- Fakhim, H.; Vaezi, A.; Dannaoui, E.; Chowdhary, A.; Nasiry, D.; Faeli, L.; Meis, J.F.; Badali, H. Comparative virulence of Candida auris with Candida haemulonii, Candida glabrata and Candida albicans in a murine model. Mycoses 2018, 61, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Alampalli, S.V.; Nageshan, R.K.; Chettiar, S.T.; Joshi, S.; Tatu, U.S. Draft genome of a commonly misdiagnosed multi-drug resistant pathogen Candida auris. BMC Genom. 2015, 16, 686. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Banerjee, T.; Pratap, C.B.; Tilak, R. Itraconazole-resistant Candida auris with phospholipase, proteinase and hemolysin activity from a case of vulvovaginitis. J. Infect. Dev. Ctries. 2015, 9, 435–437. [Google Scholar] [CrossRef] [PubMed]
- Larkin, E.; Hager, C.; Chandra, J.; Mukherjee, P.K.; Retuerto, M.; Salem, I.; Long, L.; Isham, N.; Kovanda, L.; Borroto-Esoda, K.; et al. The emerging pathogen Candida auris: Growth phenotype, virulence factors, activity of antifungals, and effect of SCY-078, a novel glucan synthesis inhibitor, on growth morphology and biofilm formation. Antimicrob. Agents Chemother. 2017, 61, e02396-16. [Google Scholar] [CrossRef]
- Sherry, L.; Ramage, G.; Kean, R.; Borman, A.; Johnson, E.M.; Richardson, M.D.; Rautemaa-Richardson, R. Biofilm-forming capability of highly virulent, multidrug-resistant Candida auris. Emerg. Infect. Dis. 2017, 23, 328. [Google Scholar] [CrossRef]
- Borman, A.M.; Szekely, A.; Johnson, E.M. Comparative pathogenicity of United Kingdom isolates of the emerging pathogen Candida auris and other key pathogenic Candida species. MSphere 2016, 1, e00189-16. [Google Scholar] [CrossRef]
- Samudrala, P.K.; Kumar, P.; Choudhary, K.; Thakur, N.; Wadekar, G.S.; Dayaramani, R.; Agrawal, M.; Alexander, A. Virology, pathogenesis, diagnosis and in-line treatment of COVID-19. Eur. J. Pharmacol. 2020, 883, 173375. [Google Scholar] [CrossRef]
- Nucci, M.; Barreiros, G.; Guimarães, L.F.; Deriquehem, V.A.; Castiñeiras, A.C.; Nouér, S.A. Increased incidence of candidemia in a tertiary care hospital with the COVID-19 pandemic. Mycoses 2021, 64, 152–156. Available online: https://pubmed.ncbi.nlm.nih.gov/33275821/ (accessed on 12 July 2021). [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; Li, W.; Tong, Q.; Yi, J.; Zhao, L.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine 2020, 55, 102763. [Google Scholar] [CrossRef]
- Xu, X.; Ong, Y.K.; Wang, Y. Role of adjunctive treatment strategies in COVID-19 and a review of international and national clinical guidelines. Mil. Med. Res. 2020, 7, 22. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef] [PubMed]
- Antinori, S.; Bonazzetti, C.; Gubertini, G.; Capetti, A.; Pagani, C.; Morena, V.; Rimoldi, S.; Galimberti, L.; Sarzi-Puttini, P.; Ridolfo, A.L. Tocilizumab for cytokine storm syndrome in COVID-19 pneumonia: An increased risk for candidemia? Autoimmun. Rev. 2020, 19, 102564. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Ahmadikia, K.; Badali, H.; Khodavaisy, S. Opportunistic Fungal Infections in the Epidemic Area of COVID-19: A Clinical and Diagnostic Perspective from Iran. Mycopathologia 2020, 185, 607–611. Available online: /pmc/articles/PMC7393345/ (accessed on 7 June 2021). [CrossRef]
- Medeiros, M.A.P.; Melo, A.P.V.; Bento, A.O.; Souza, L.B.F.C.; Neto, F.A.B.; Garcia, J.B.; Zuza-Alves, D.L.; Francisco, E.C.; Melo, A.S.A.; Chaves, G.M. Epidemiology and prognostic factors of nosocomial candidemia in Northeast Brazil: A six-year retrospective study. PLoS ONE 2019, 14, e0221033. [Google Scholar] [CrossRef] [PubMed]
- Kenters, N.; Kiernan, M.; Chowdhary, A.; Denning, D.W.; Pemán, J.; Saris, K.; Schelenz, S.; Tartari, E.; Widmer, A.; Meis, J.F.; et al. Control of Candida auris in healthcare institutions: Outcome of an International Society for Antimicrobial Chemotherapy expert meeting. Int. J. Antimicrob. Agents 2019, 54, 400–406. [Google Scholar] [CrossRef]
- Görkem, A.; Hafize, S.A.V.; Özge, K.A.A.N.; Esma, E.R.E.N. Coronavirus disease and candidemia infection: A case report. J. Mycol. Med. 2021, 31. Available online: https://pubmed.ncbi.nlm.nih.gov/34146997/ (accessed on 12 July 2021). [CrossRef] [PubMed]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.B.; CMMID Working Group; Jombart, T.; Procter, S.R.; Knight, G. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- Nobrega de Almeida, J., Jr.; Brandão, I.B.; Francisco, E.C.; de Almeida, S.L.R.; de Oliveira Dias, P.; Pereira, F.M.; Santos Ferreira, F.; de Andrade, T.S.; de Miranda Costa, M.M.; de Souza Jordão, R.T.; et al. Axillary Digital Thermometers uplifted a multidrug-susceptible Candida auris outbreak among COVID-19 patients in Brazil. Mycoses 2021, 35, e00094-21. [Google Scholar] [CrossRef]
- Rodriguez, J.Y.; Le Pape, P.; Lopez, O.; Esquea, K.; Labiosa, A.L.; Alvarez-Moreno, C. Candida auris: A latent threat to critically ill patients with COVID-19. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 73, ciaa1595, Advance online publication. [Google Scholar] [CrossRef]
- Baccolini, V.; Migliara, G.; Isonne, C.; Dorelli, B.; Barone, L.C.; Giannini, D.; Marotta, D.; Marte, M.; Mazzalai, E.; Alessandri, F.; et al. The impact of the COVID-19 pandemic on healthcare-associated infections in intensive care unit patients: A retrospective cohort study. Antimicrob. Resist. Infect. Control 2021, 10, 87. [Google Scholar] [CrossRef]
- Gorospe-Sarasúa, L.; Gallego-Rivera, J.I.; Muñoz-Molina, G.M.; Mirambeaux-Villalona, R.M.; Ajuria-Illarramendi, O.; González-García, A.; Barbolla-Díaz, I. Delayed Candida Costochondritis and Spondylitis in a Post-COVID-19 Patient Previously Treated With Corticosteroids, Antibiotics, and Tocilizumab. Costocondritis y espondilitis diferidas por Candida en paciente post-COVID-19 tratado previamente con corticoides, antibióticos y tocilizumab. Arch. Bronconeumol. 2021, 57 (Suppl. S2), 48–50. [Google Scholar] [CrossRef] [PubMed]
- Di Pilato, V.; Codda, G.; Ball, L.; Giacobbe, D.R.; Willison, E.; Mikulska, M.; Magnasco, L.; Crea, F.; Vena, A.; Pelosi, P.; et al. Molecular Epidemiological Investigation of a Nosocomial Cluster of C. auris: Evidence of Recent Emergence in Italy and Ease of Transmission during the COVID-19 Pandemic. J. Fungi 2021, 7, 140. [Google Scholar] [CrossRef] [PubMed]
- Majumder, J.; Minko, T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J. 2021, 23, 14. [Google Scholar] [CrossRef]
- Bhatt, K.; Agolli, A.; Patel, M.H.; Garimella, R.; Devi, M.; Garcia, E.; Amin, H.; Domingue, C.; Del Castillo, R.G.; Sanchez-Gonzalez, M. High mortality co-infections of COVID-19 patients: Mucormycosis and other fungal infections. Discoveries 2021, 9, e126. [Google Scholar] [CrossRef] [PubMed]
- Arastehfar, A.; Shaban, T.; Zarrinfar, H.; Roudbary, M.; Ghazanfari, M.; Hedayati, M.T.; Sedaghat, A.; Ilkit, M.; Najafzadeh, M.J.; Perlin, D.S. Candidemia among iranian patients with severe COVID-19 admitted to I.C.U.s. J. Fungi 2021, 7, 280. [Google Scholar] [CrossRef]
- Alashqar, M.B.; Alabdan, L.; Khan, M.; Almakadma, A.H.; Almustanyir, S. A Case Report of a Candida auris Infection in Saudi Arabia. Cureus 2021, 13, 15240. [Google Scholar] [CrossRef]
- Almeida, J.N.; Francisco, E.C.; Hagen, F.; Brandão, I.B.; Pereira, F.M.; Presta Dias, P.H.; de Miranda Costa, M.M.; de Souza Jordão, R.T.; de Groot, T.; Colombo, A.L. Emergence of Candida auris in Brazil in a COVID-19 intensive care unit. J. Fungi 2021, 7, 220. [Google Scholar] [CrossRef]
- Invasive Candidiasis|Candidiasis|Types of Fungal Diseases|Fungal Diseases|CDC [Internet]. Available online: https://www.cdc.gov/fungal/diseases/candidiasis/invasive/index.html (accessed on 12 July 2021).
- Candida Auris: Symptoms, Causes, Diagnosis, Treatment. Available online: https://www.verywellhealth.com/candida-auris-4692475 (accessed on 12 July 2021).
- Breazzano, M.P.; Tooley, A.A.; Godfrey, K.J.; Iacob, C.E.; Yannuzzi, N.A.; Flynn, H.W. Candida auris and endogenous panophthalmitis: Clinical and histopathological features. Am. J. Ophthalmol. Case Rep. 2020, 19, 100738. [Google Scholar] [CrossRef]
- Shenoy, V.; Ballenberger, M.; Prince, A.; Maslak, S. Panophthalmitis from Candida auris. Ann. Intern. Med. 2019, 171, 941–943. [Google Scholar] [CrossRef]
- Supreeth, S.; Al Ghafri, K.A.; Jayachandra, R.K.; Al Balushi, Z.Y. First Report of Candida auris Spondylodiscitis in Oman: A Rare Presentation. World Neurosurg. 2020, 135, 335–338. [Google Scholar] [CrossRef]
- Choi, H.I.; An, J.; Hwang, J.J.; Moon, S.Y.; Son, J.S. Otomastoiditis caused by Candida auris: Case report and literature review. Mycoses 2017, 60, 488–492. [Google Scholar] [CrossRef] [PubMed]
- Dewaele, K.; Frans, J.; Smismans, A.; Ho, E.; Tollens, T.; Lagrou, K. First case of Candida auris infection in Belgium in a surgical patient from Kuwait. Acta Clin. Belg. 2018, 73, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Sarma, S.; Upadhyay, S. Current perspective on emergence, diagnosis and drug resistance in Candida auris. Infect. Drug Resist. 2017, 10, 155. [Google Scholar] [CrossRef] [PubMed]
- Procedure for collection of patient swabs for Candida auris. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-patient-swab.html (accessed on 12 July 2021).
- Arastehfar, A.; Carvalho, A.; Nguyen, M.H.; Hedayati, M.T.; Netea, M.G.; Perlin, D.S.; Hoenigl, M. COVID-19-associated candidiasis (C.A.C.): An underestimated complication in the absence of immunological predispositions? J. Fungi 2020, 6, 211. [Google Scholar] [CrossRef] [PubMed]
- Osei Sekyere, J. Candida auris: A systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen 2018, 7, e00578. [Google Scholar] [CrossRef]
- Identification of Candida auris|Candida auris|Fungal Diseases|CDC [Internet]. Available online: https://www.cdc.gov/fungal/candida-auris/identification.html (accessed on 12 July 2021).
- Fasciana, T.; Cortegiani, A.; Ippolito, M.; Giarratano, A.; Di Quattro, O.; Lipari, D.; Graceffa, D.; Giammanco, A. Candida auris: An overview of how to screen, detect, test and control this emerging pathogen. Antibiotics 2020, 9, 778. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Chakrabarti, A.; Paul, R.A.; Sood, P.; Kaur, H.; Capoor, M.R.; Kindo, A.J.; Marak, R.S.; Arora, A.; Sardana, R.; et al. Candida auris candidaemia in Indian I.C.U.s: Analysis of risk factors. J. Antimicrob. Chemother. 2017, 72, 1794–1801. [Google Scholar] [CrossRef]
- Lai, C.C.; Wang, C.Y.; Hsueh, P.R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Zuo, T.; Zhan, H.; Zhang, F.; Liu, Q.; Tso, E.Y.; Lui, G.C.; Chen, N.; Li, A.; Lu, W.; Chan, F.K.; et al. Alterations in fecal fungal microbiome of patients with COVID-19 during time of hospitalization until discharge. Gastroenterology 2020, 159, 1302–1310. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2015, 62, e1–e50. [Google Scholar] [CrossRef] [Green Version]
- Treatment and Management of Infections and Colonization|Candida auris|Fungal Diseases|CDC, Cdc.gov. 2021. Available online: https://www.cdc.gov/fungal/candida-Auris/c-Auris-treatment.html (accessed on 27 August 2021).
- Ademe, M.; Girma, F. Candida auris: From Multidrug Resistance to Pan-Resistant Strains. Infect. Drug Resist. 2020, 13, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Magnasco, L.; Mikulska, M.; Giacobbe, D.; Taramasso, L.; Vena, A.; Dentone, C.; Dettori, S.; Tutino, S.; Labate, L.; Di Pilato, V.; et al. Spread of Carbapenem-Resistant Gram-Negatives and Candida auris during the COVID-19 Pandemic in Critically Ill Patients: One Step Back in Antimicrobial Stewardship? Microorganisms 2021, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Pristov, K.; Ghannoum, M. Resistance of Candida to azoles and echinocandins worldwide. Clin. Microbiol. Infect. 2019, 25, 792–798. [Google Scholar] [CrossRef]
- Chow, N.A.; Muñoz, J.F.; Gade, L.; Berkow, E.L.; Li, X.; Welsh, R.M.; Forsberg, K.; Lockhart, S.R.; Adam, R.; Alanio, A.; et al. Tracing the Evolutionary History and Global Expansion of Candida auris Using Population Genomic Analyses. mBio 2020, 11, e03364-19. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, T.; Alkhazraji, S.; Alqarihi, A.; Jeon, H.H.; Gu, Y.; Kapoor, M.; Shaw, K.J.; Ibrahim, A.S. APX001 Is Effective in the Treatment of Murine Invasive Pulmonary Aspergillosis. Antimicrob. Agents Chemother. 2019, 63, e01715-18. [Google Scholar] [CrossRef]
- Wring, S.; Borroto-Esoda, K.; Solon, E.; Angulo, D. SCY-078, a Novel Fungicidal Agent, Demonstrates Distribution to Tissues Associated with Fungal Infections during Mass Balance Studies with Intravenous and Oral [14C] SCY-078 in Albino and Pigmented Rats. Antimicrob. Agents Chemother. 2019, 63, e02119-18. [Google Scholar] [CrossRef]
- Ham, Y.; Lewis, J.; Thompson, G. Rezafungin: A novel antifungal for the treatment of invasive candidiasis. Future Microbiol. 2021, 16, 27–36. [Google Scholar] [CrossRef]
- Infection Prevention and Control for Candida auris|Candida auris|Fungal Diseases|CDC, Cdc.gov. 2021. Available online: https://www.cdc.gov/fungal/candida-Auris/c-Auris-infection-control.html (accessed on 27 August 2021).


{kind=link}
| Title | Study Type | Study Period | Region | Prevalence (% or Number) | Clinical Presentation | Diagnostic Technique | Mortality |
|---|---|---|---|---|---|---|---|
| Outbreak of Candida auris infection in a COVID-19 hospital in Mexico | Letter | April to May 2021 | Mexico | 12 | Mechanical ventilation | Matrix-assisted laser desorption/ionization time-of-flight | 83.30% |
| Peripherally inserted central lines (PICCs) | Mass spectrometry | ||||||
| Urinary catheters | Confirmed by multilocus sequence typing | ||||||
| Prolonged hospital stay (20–70 days). | |||||||
| Emergence of Candida auris in Brazil in a COVID-19 Intensive Care Unit | Original A | 1 December 2021 | Brazil | 2 | Case 1: fever subsided | CVCt culture identified by Vitek 2 automated system | - |
| Case 2: hemodialysis catheter exit showed inflammatory signs, | |||||||
| catheter-related bloodstream infections | |||||||
| Candida auris Outbreak in a COVID-19 Specialty Care Unit-Florida, July–August 2020 | Case report | July to August 2020 | USA | 67 | Invasive infection | Clinical cultures | 40% |
| The lurking scourge of multidrug-resistant Candida auris in times of COVID-19 pandemic | Letter | - | - | 4 | 30% to 72% | ||
| First Candida auris Outbreak during a COVID-19 Pandemic in a Tertiary-Care Center in Lebanon | Case report | October to December 2020 | Lebanon | 14 | Pneumonia and respiratory failure | MS-VITEK matrix-assisted laser desorption ionization time of flight mass spectrometry | 35% |
| five patients expired | |||||||
| Multidrug-Resistant Candida auris Infections in Critically Ill Coronavirus Disease Patients, India, April–July 2020 | case report | April to July 2020 | India | 15 | Cultured from blood and urine samples | 60% | |
| Spread of Carbapenem-Resistant Gram-Negatives and Candida auris during the COVID-19 Pandemic in Critically Ill Patients: One Step Back in Antimicrobial Stewardship? | Original Article | February to May 2020 | Italy | 4 | two out of four patients expired | using Vitek2 system | 50% |
| Axillary Digital Thermometers uplifted a multidrug-susceptible Candida auris outbreak among COVID-19 patients in Brazil | Original Article | Brazil | 66 | Body swabs Central venous catheter tip (CVC-tip) Blood cultures Urine Culture | 33.3% | ||
| Genomic Characterizations of Clade III Lineage of Candida auris, California, USA | Case report | September 2019–September 2020 | USA | 6 | Swab samplesPCR | - | |
| Molecular Epidemiological Investigation of a Nosocomial Cluster of C. auris: Evidence of Recent Emergence in Italy and Ease of Transmission during the COVID-19 Pandemic | Original Article | July 2019 to May 2020 | Italy | 10 | Matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS | 50% | |
| confirmed by PCR amplification | |||||||
| Increased incidence of candidemia in a tertiary care hospital with the COVID-19 pandemic | Original Article | January 2019 to February 2020 (period 1) | Brazil | Period 1 incidence of candidemia (per 1000 admissions): 1.54 and | Diarrhea Nausea abdominal pain vomiting | 61.00% | |
| March to September 2020 (period 2). | Period 2: 7.44 | ||||||
| Oropharyngeal candidiasis in hospitalized COVID-19 Patients from Iran: Species identification and antifungal susceptibility pattern | Original Article | 20-Jun | Iran | 65 | LymLeucopeniaLeucopaenia, Leucocytosis, Prolonged fever, Respiratory distress | train identification was performed by PCR sequencing of the internal transcribed spacer region | - |
| The impact of the COVID-19 pandemic on healthcare-associated infections in intensive care unit patients: a retrospective cohort study | Retrospective Cohort | March to April 2020 | Italy | 59 | 2019: 10 patients expired | ||
| 2020: 35 patients expired | |||||||
| Prevalence of candidiasis and oral candidiasis in COVID-19 patients: a cross-sectional pilot study from the patients’ registry in a large health center | Observational | 21-July | 106 and 14 | - | |||
| High mortality co-infections of COVID-19 patients: mucormycosis and other fungal infections | Original Article | 1 October | USA | 6 | clinical cultures | 100% | |
| COVID-19-Associated Candidiasis (CAC): An Underestimated Complication in the Absence of Immunological Predispositions? | Original Article | 20 October | clinical cultures | ||||
| Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections | Original Article | March to May 2020 | Spain | blood cultures were obtained > 48 h after admission. | |||
| ICU-acquired bloodstream infections in critically ill patients with COVID-19 | Observational | March to May 2020 | Greece | 7 | blood culture | ||
| C. auris and non-C. auris candidemia in hospitalized adult and pediatric COVID-19 patients; single center data from Pakistan | Observational | April–December 2020 | Pakistan | 26 | blood cultures | 67% | |
| The landscape of candidemia during the COVID-19 pandemic | Observational | April–August 2020 | USA | 64 | culture | 20.30% | |
| Incidence and Risk Factors for COVID-19 Associated Candidemia (CAC) in ICU Patients | Observational | August 2020 to August 2021 | Turkey | 63 | bacteremia | Isolated blood culture, urine, deep tracheal aspirate, VitekMS (bioMerieux) device, and MALDI-TOF MS method | 77.80% |
| Clinical characteristics and risk factors for COVID-19-associated Candidemia | Observational | March 2020 and April 2021 | Qatar | 80 | blood culture | 72.60% | |
| Candida auris Invasive Infections during a COVID-19 Case Surge | Case Report | USA | 12 | matrix-assisted laser desorption/ionization-time of flight (MALDI-ToF) | |||
| Candidemia in COVID-19 treated with corticosteroids and tocilizumab | Case Report | Obesity, fever (38.6 °C), a saturation of percutaneous oxygen of 92%, respiratory rate of 24/min | blood culture | ||||
| Candidemia among Iranian Patients with Severe COVID-19 Admitted to ICUs | Original Article | November 2020 to January 2021 | Iran | 7 | PCR, blood cultures, DNA Extraction, and Species Identification | 100% | |
| The challenge of preventing and containing outbreaks of multidrug-resistant organisms and Candida auris during the coronavirus disease 2019 pandemic: report of a carbapenem-resistant Acinetobacter baumannii outbreak and a systematic review of the literature | Systematic Review | September to early December | |||||
| COVID-19 and invasive fungal coinfections: A case series at a Brazilian referral hospital | Observational | February to December 2020 | Brazil | 4 | clinical cultures | 100% | |
| Impact of the SARS-CoV-2 Pandemic in Candidaemia, Invasive Aspergillosis, and Antifungal Consumption in a Tertiary Hospital | Retrospective | April 2019 to March 2021 | Spain | 152 | clinical cultures | 27.9% and 57.7% in 2020 and 2021 | |
| COVID-19 and Candida duobushaemulonii superinfection: A case report | Case Report | Lebanon | acute respiratory distress syndrome (ARDS) | clinical cultures | |||
| First Case of COVID-19 Positive Candida auris Fungemia in Turkey | Case Report | October 20 | Turkey | 1 | acute respiratory distress syndrome (ARDS) and viral pneumonia | clinical cultures, VITEK MALDI TOF MS | 100% |
| confirmed by sequencing. | |||||||
| Ominous combination: COVID-19 disease and Candida auris fungemia-Case report and review of the literature. | Case Report | - | - | 1 | fever, cough, and progressive shortness of breath, cytokine storm, liver, and acute kidney injury, new radiological infiltrates and worse condition | Blood culture obtained from central and peripheral lines | 100% |
| Fungemia in COVID-19 ICU patients, a single medical center experience | Retrospective | March 2020–June 2020 | USA | 24 | Prolonged mechanical ventilation support | Blood culture system | 38% |
| matrix-assisted laser desorption ionization time-of-flight mass spectrometry. | |||||||
| Laboratory-based surveillance of Candida auris in Colombia, 2016–2020. | Original Article | March 2016 to December 2020. | Columbia | 122 | bloodstream infections, sepsis | Culture from skin, genito-urinary site. Biotyper MALDI-TOF | - |
| The Influence of Infection and Colonization on Outcomes in Inpatients With COVID-19: Are We Forgetting Something? | Observational | 27 February 2020–26 February 2021 | Spain | 14 | - | MALDI-TOF mass spectrometry, antimicrobial susceptibility tests | 30.80% |
| Molecular Epidemiological Investigation of a Nosocomial Cluster of C. auris: Evidence of Recent Emergence in Italy and Ease of Transmission during the COVID-19 Pandemic | Original Article | July 2019 to May 2020 | Italy | 10 | bloodstream infections and colonization | matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) and PCR amplification of the species-specific GPI protein-encoding genes | - |
| Axillary Digital Thermometers uplifted a multidrug-susceptible Candida auris outbreak among COVID-19 patients in Brazil | Case Report | 1 December 20 | Brazil | 8 | acute respiratory distress syndrome related to SARS-CoV-2 infection at admission. | Vitek 2 system, Culture, MALDI-TOF mass spectrometry | 33.30% |
| Three Candida auris Case Reports from Istanbul, Turkey | Case Report | November 2020–January 2021 | Turkey | 1 | Shortness of breathpneumoniaacute renal failure. | Catheter tip cultures MALDI-TOF Microflex LT/SH Smart MS confirmed by conventional and DNA methods. | 33.30% |
| A High Frequency of Candida auris Blood Stream Infections in Coronavirus Disease 2019 Patients Admitted to Intensive Care Units, Northwestern India: A Case Control Study | Case Control Study | August 2020–January 2021 | India | 33 | MALDI-TOF Bruker Biotyper. confirmed by amplification and sequencing of DNA. | ||
| Candidemia in Coronavirus Disease 2019 (COVID-19) Patients: Incidence and Characteristics in a Prospective Cohort Compared With Historical Non–COVID-19 Controls | Observational | 15 February 2020–30 June 2020 | Italy | 21 | severe acute respiratory distress syndrome | 57.10% | |
| ICU-acquired Candidemia in COVID-19 Patients: An Experience from a Tertiary Care Hospital in Kerala, South India | Letter | July 5, 2020, to February 28, 2021 | India | 1 | 100% | ||
| Candida auris: A Latent Threat to Critically Ill Patients With Coronavirus Disease 2019 | Letter | June to September 2020 | Colombia | 6 | severe acute respiratory distress syndrome | matrix-assisted laser desorption/ionization time-of-flight mass spectrometry | 100% |
| Microbial Species | Name of Organisms | Co-Infection |
|---|---|---|
| GRAM-POSITIVE BACTERIA | Staphylococcus aureus Streptococcus pneumoniae Enterococcus faecium Enterococcus faecalis Coagulase negative-S.aureus | Causes community/ventilator-associated pneumonia, necrotizing/cavitating pneumonia, sepsis shock, and Infective endocarditis [17,19,21,27]. Causes Hospital-acquired pneumonia [17]. Causes intra-abdominal infection, concurrent urinary tract infection, and bacteremia [17]. Causes urinary tract infection, intra-abdominal infection, and infective endocarditis in COVID 19 patients [17,21]. Causes bacteremia and sepsis [17,19]. |
| GRAM-NEGATIVE BACTERIA | Pseudomonas aeruginosa Klebsiella pneumoniae Escherichia coli Acinetobacter baumannii Stenotrophomonas maltophilia Haemophilus influenzae | Causes hospital/ventilator-associated pneumonia, bacteremia, urinary tract infection, and lower respiratory tract infection with bronchiectasis in severely ill COVID patients [17]. Causes ventilator-associated pneumonia and concurrent urinary tract infection [17]. Causes bacteremia, concurrent urinary tract infection, and intra-abdominal infection with E. faecalis and E. faecium [17]. Causes ventilator-associated pneumonia in patients with comorbidities like diabetes, and increased stay in ICU [17,22]. Causes ventilator-associated pneumonia and nosocomial infection in immunosuppressed COVID patients [17,23]. Causes community-acquired pneumonia [17]. |
| ATYPICAL BACTERIA | Mycoplasma pneumoniae Moraxella catarrhalis Mycobacterium tuberculosis | Causes interstitial pneumonia and exacerbation COVID symptoms [17]. Community-acquired interstitial pneumonia [17].Causes caseating granulomas and activation of latent T.B. due to immune dysfunction in COVID infection [35]. |
| FUNGI | Candida auris | Persistent fungemia in immunocompromised individuals, urinary tract infection Eye, ear, and nose infections associated with COVID patients having co-morbidities [31,32]. |
| Candida albicans Candida dubliniensis Candida glabrata Candida krusei Candida parapsilosis | Causes oropharyngeal candidiasis, oropharyngeal thrush with erythematous inflammation, and infective endocarditis. Invasive in immunocompromised individuals causing infection in the blood; candidemia. Associated with ventilation, intubation and urine catheterization [21,31,32]. | |
| Aspergillus fumigatus Aspergillus flavus | Causes tracheobronchitis, necrotizing pneumonia, and bronchial wall ulceration in COVID 19 patients on the ventilator [32]. | |
| VIRUSES | Respiratory Syncytial virus Influenza A/B virus Human metapneumovirus rhino/enterovirus Parainfluenza Epstein-Barr virus | Causes cold/ flu-like symptoms (cough, sore throat, fever, rhinorrhea, and dyspnea) but can exacerbate COVID symptoms causing acute respiratory distress syndrome [33,34]. Causes Infectious Mononucleosis (I.M.) and splenomegaly [27]. |
| H.I.V. Hepatitis B/C virus | Leads to a decrease in CD4+ T cells and immunosuppression in COVID patients [19]. Causes liver impairment and systemic inflammation [19]. |
| Invasive Fungal Infection | Fungi Species | Name of Organism |
|---|---|---|
| Invasive candidiasis | Candida spp. | Candida albicans Candida tropicalis Candida parapsilosis [36,40,41,42,43,44]. |
| COVID-associated pulmonary aspergillosis [CAPA] | Aspergillus spp. | Aspergillus niger Aspergillus fumigatus Aspergillus lentulus Aspergillus terreus Aspergillus trinoterreus [36,37,38,39,40,41,42,43,44] |
| Mucormycosis | Rhizopus spp. | Rhizopus stolonifera Rhizopus microspores [42] |
| Cryptococcosis | Cryptococcus spp. | Cryptococcus neoformans [44] |
| Histoplasmosis | Histoplasmosis spp. | Histoplasmosis capsulatum [44] |
| Clinical Risk Factors | Non-Clinical Risk Factors | Medication-Related Risk Factors |
|---|---|---|
| Diabetes Mellitus [4,9,71,81,82,83] | Prolonged ICU stay [51,71] | Corticosteroids [5,9,51,71,81,82,83,84] |
| Renal Failure [81] | Age > 60 [78] | Catheter venous, Foley catheter [5,9,81,84] |
| Chronic Kidney Disease [4,9,82] | Male sex [78] | Mechanical Ventilation and/or intubation [5,9,71,84,85] |
| Ventilator-associated pneumonia [71] | Obesity [83] | Incorrect use of PPE [82] |
| Hypertension [71] | Broad spectrum antibiotics [5,9,51,71,81,84) | |
| Invasive hemodynamic monitoring | Interleukin-6 receptor inhibitors [71] | |
| Lymphopenia [71] | Tocilizumab [85] | |
| Cardiovascular diseases [71,83] | Colonized digital thermometers [5] | |
| Urinary tract infections [71] | Dialysis [84] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najeeb, H.; Siddiqui, S.A.; Anas, Z.; Ali, S.H.; Usmani, S.U.R.; Jawed, F.; Jatoi, H.N. The Menace of Candida auris Epidemic Amidst the COVID-19 Pandemic: A Systematic Review. Diseases 2022, 10, 58. https://doi.org/10.3390/diseases10030058
Najeeb H, Siddiqui SA, Anas Z, Ali SH, Usmani SUR, Jawed F, Jatoi HN. The Menace of Candida auris Epidemic Amidst the COVID-19 Pandemic: A Systematic Review. Diseases. 2022; 10(3):58. https://doi.org/10.3390/diseases10030058
Chicago/Turabian StyleNajeeb, Hala, Sarush Ahmed Siddiqui, Zahra Anas, Syed Hasan Ali, Shajie Ur Rehman Usmani, Fareeha Jawed, and Hafsa Nazir Jatoi. 2022. "The Menace of Candida auris Epidemic Amidst the COVID-19 Pandemic: A Systematic Review" Diseases 10, no. 3: 58. https://doi.org/10.3390/diseases10030058
APA StyleNajeeb, H., Siddiqui, S. A., Anas, Z., Ali, S. H., Usmani, S. U. R., Jawed, F., & Jatoi, H. N. (2022). The Menace of Candida auris Epidemic Amidst the COVID-19 Pandemic: A Systematic Review. Diseases, 10(3), 58. https://doi.org/10.3390/diseases10030058