Affordable and Faster Transradial Prosthetic Socket Production Using Photogrammetry and 3D Printing


 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
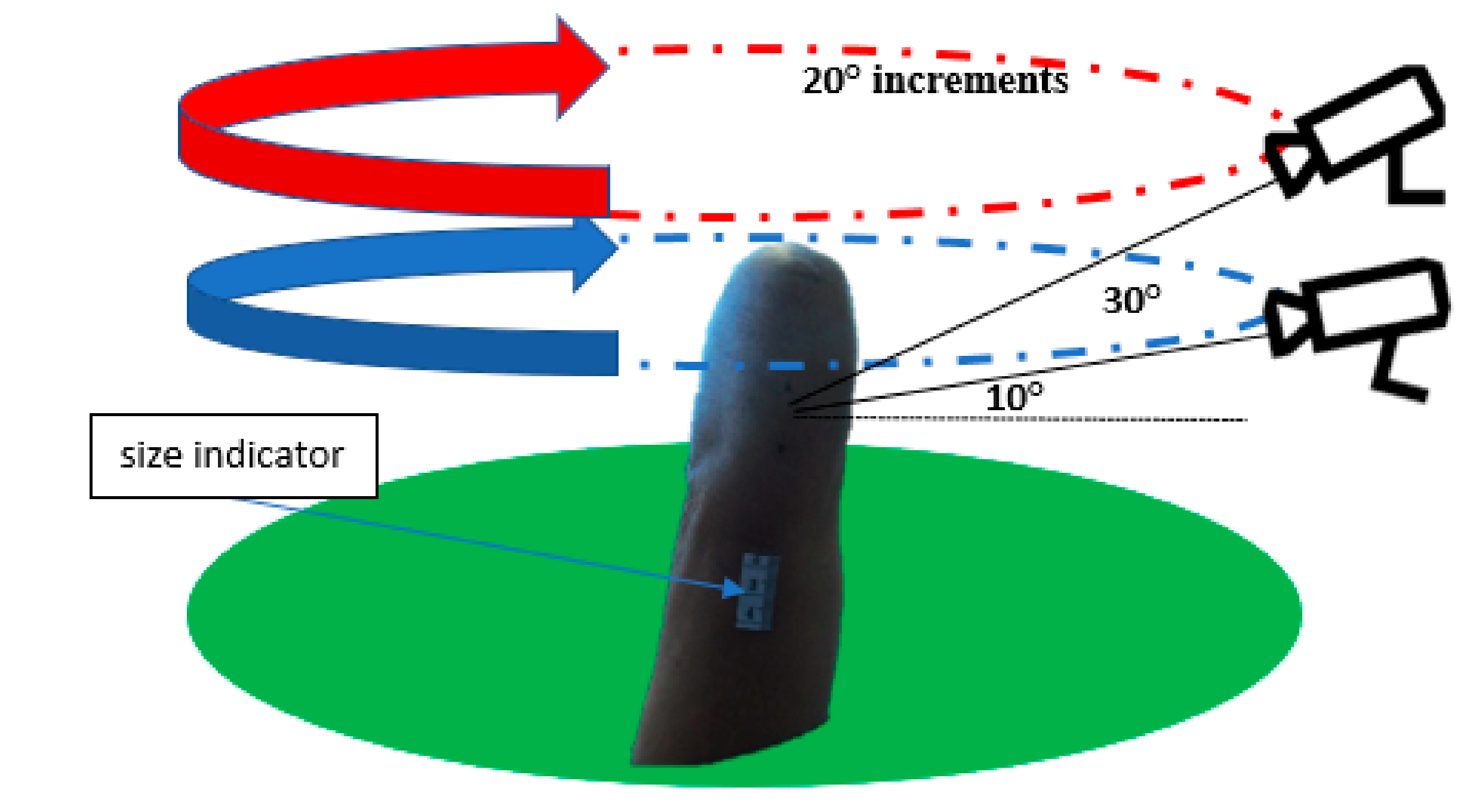
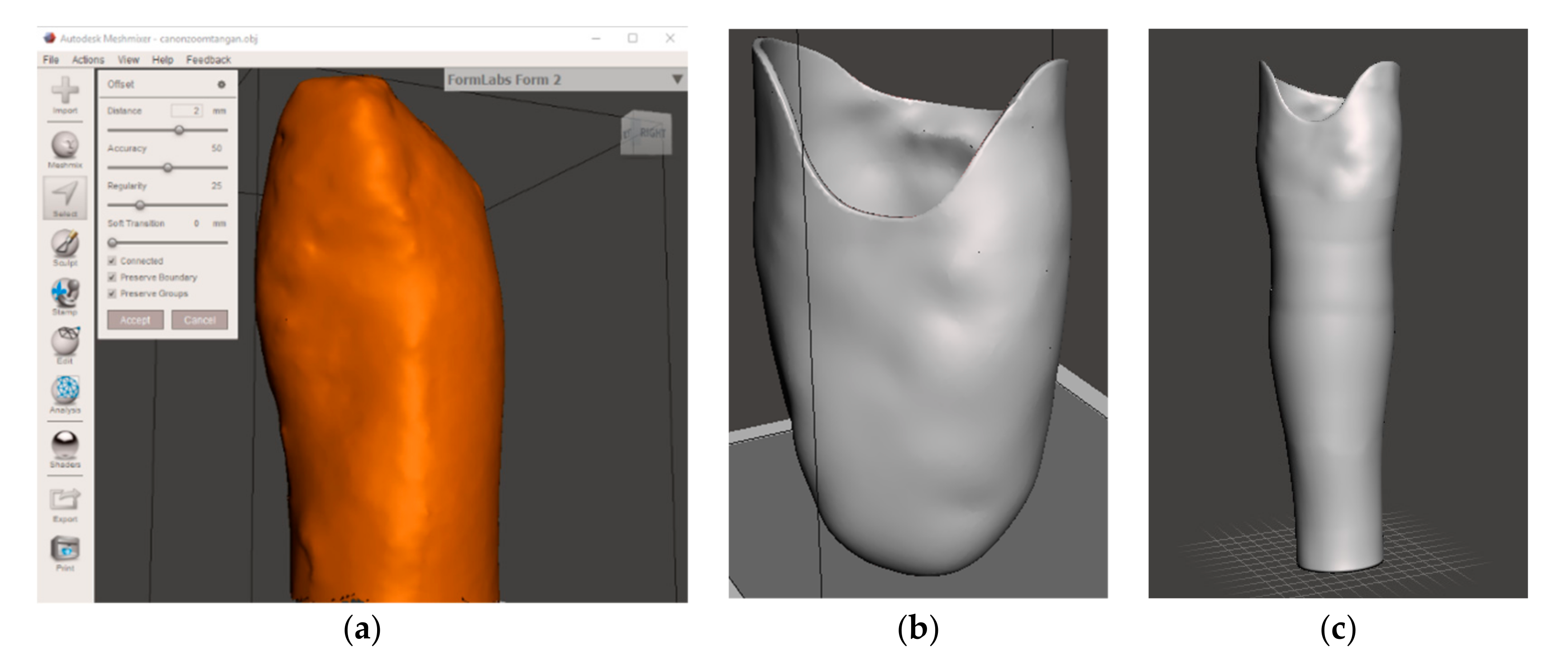
2.1. Photogrammetry Socket Fabrication Method
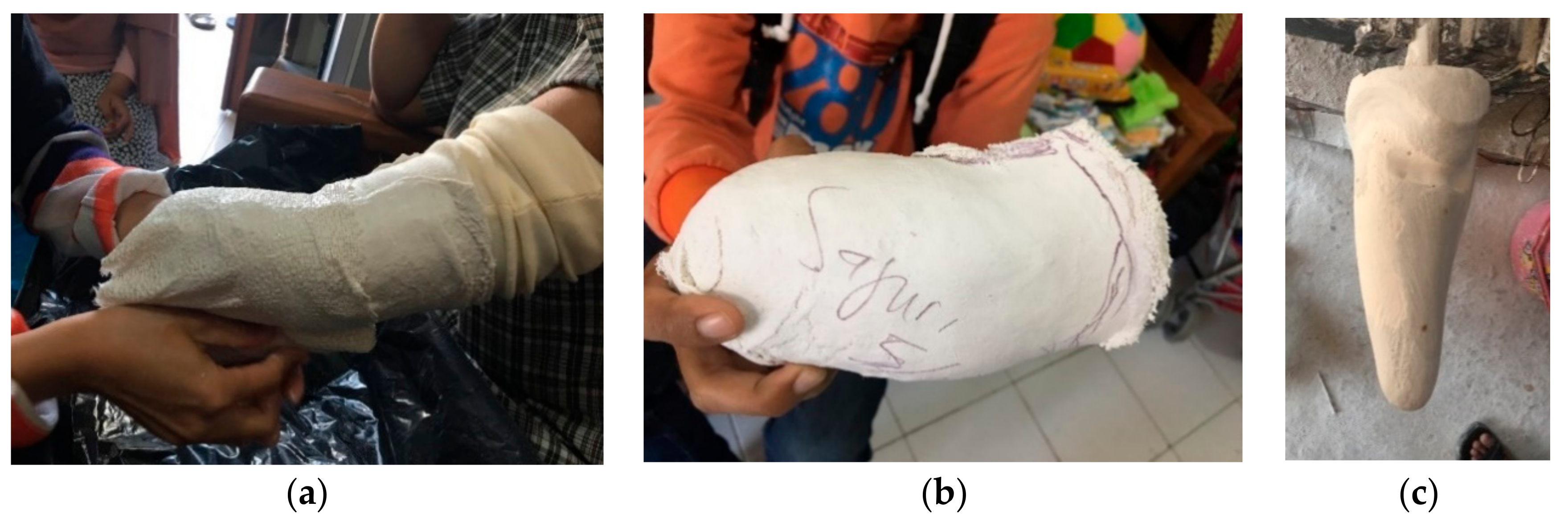
2.2. Casting Socket Fabrication Method
2.3. Usability Test
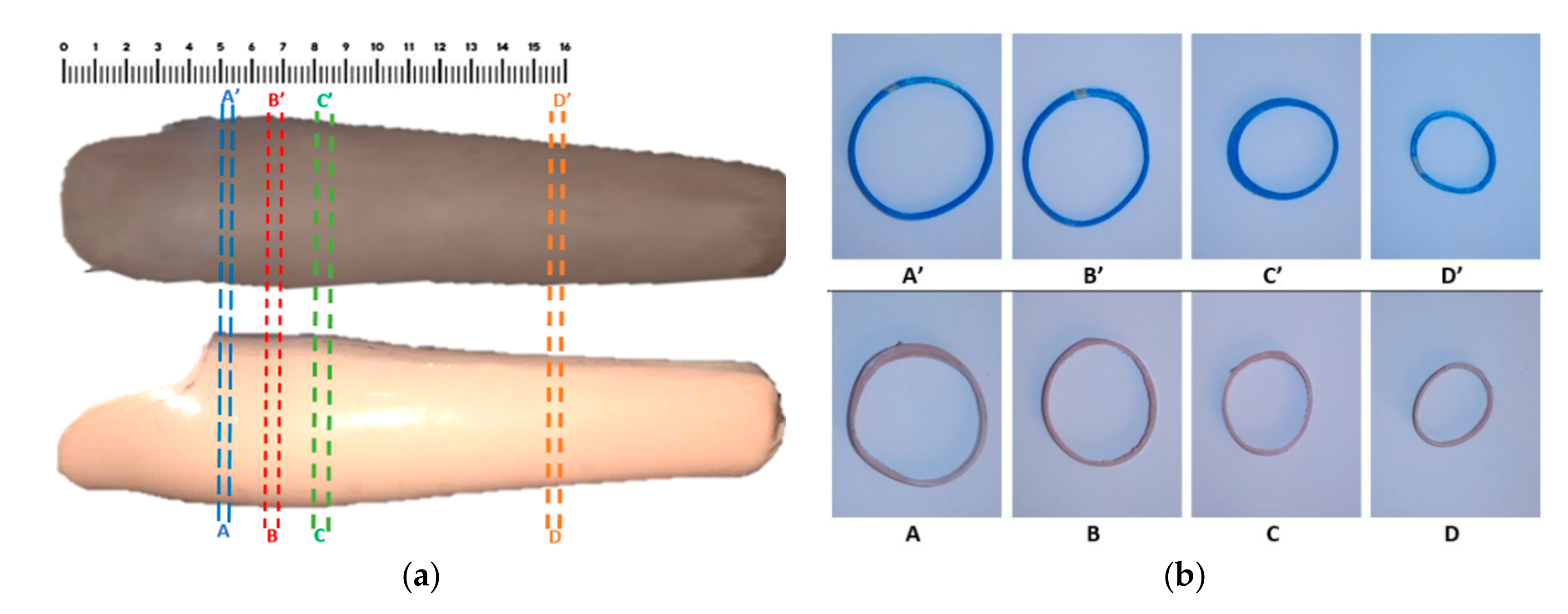
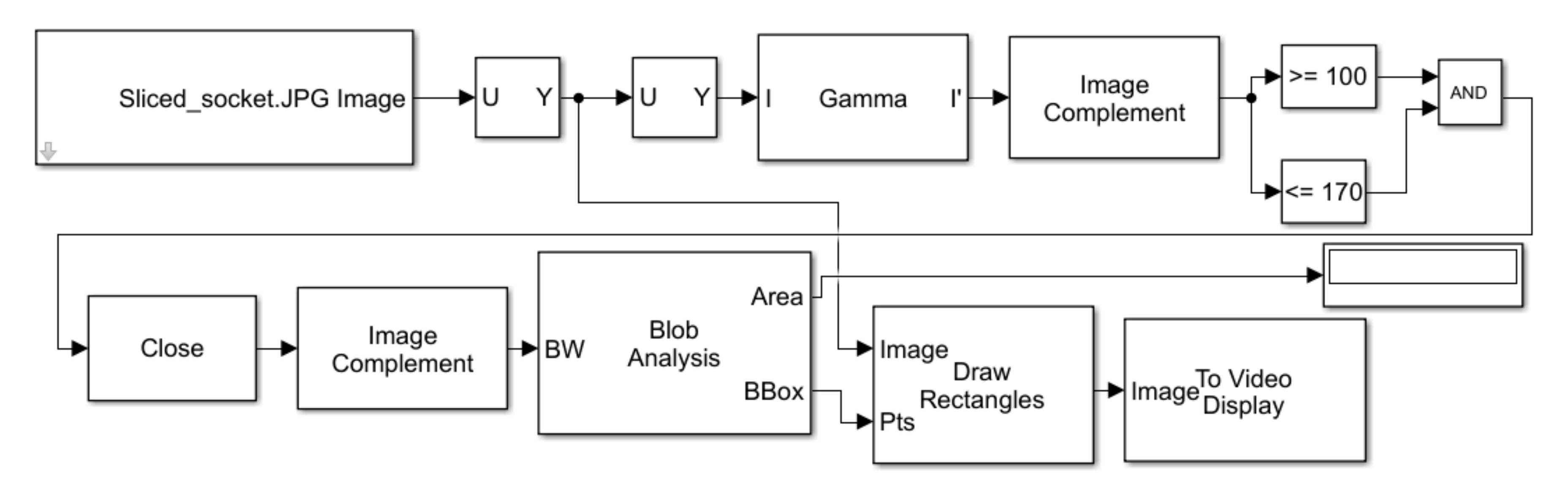
2.4. Segments Area Conformity Analysis
3. Result and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organisation (WHO). International Society for Prosthetics and Orthotics (ISPO) Guidelines for Training Personnel in Developing Countries for Prosthetics and Orthotics Services; WHO: Geneva, Switzerland, 2005; pp. 1–57. [Google Scholar]
- Junianto, A.D.; Kuswanto, D. Desain kaki palsu untuk membantu aktivitas berjalan pada tuna daksa transtibial dengan menggunakan rapid prototyping dan reverse engineering. J. Sains dan Seni ITS 2018, 7, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Sang, Y.; Li, X.; Luo, Y. Biomechanical design considerations for transradial prosthetic interface: A review. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2016, 230, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.K.; Jin, Y.; Wensman, J.; Shih, A. Additive manufacturing of custom orthoses and prostheses—A review. Addit. Manuf. 2016, 12, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Baumann, F.; Roller, D. Additive Manufacturing, Cloud-Based 3D Printing and Associated Services—Overview. J. Manuf. Mater. Process. 2017, 1, 15. [Google Scholar] [CrossRef] [Green Version]
- Berman, B. 3-D printing: The new industrial revolution. Bus. Horiz. 2012, 55, 155–162. [Google Scholar] [CrossRef]
- Cho, H.; Jammalamadaka, U.; Tappa, K. Nanogels for pharmaceutical and biomedical applications and their fabrication using 3D printing technologies. Materials 2018, 11, 302. [Google Scholar] [CrossRef] [Green Version]
- Taqriban, R.B.; Ismail, R.; Ariyanto, M.; Putra, A.F.Y.S. 3D Model of Photogrammetry Technique for Transtibial Prosthetic Socket Design Development. In Proceedings of the 2019 2nd International Seminar on Research of Information Technology and Intelligent Systems (ISRITI), Yogyakarta, Indonesia, 5–6 December 2019; pp. 456–461. [Google Scholar] [CrossRef]
- Said, S.; Boulkaibet, I.; Sheikh, M.; Karar, A.S.; Alkork, S.; Nait-Ali, A. Machine-Learning-Based Muscle Control of a 3D-Printed Bionic Arm. Sensors 2020, 20, 3144. [Google Scholar] [CrossRef]
- Van der Riet, D.; Stopforth, R.; Bright, G.; Perumall, P.; Diegel, O. The Low Cost Design of a 3D Printed Multi-Fingered Myoelectric Prosthetic Hand; Nova Science Publishers, Inc.: New York, NY, USA, 2015; ISBN 9781634828543. [Google Scholar]
- Buzzi, M.; Colombo, G.; Facoetti, G.; Gabbiadini, S.; Rizzi, C. 3D modelling and knowledge: Tools to automate prosthesis development process. Int. J. Interact. Des. Manuf. 2012, 6, 41–53. [Google Scholar] [CrossRef]
- Lee, J.J.; Kim, D.H.; Noh, K. A technique for transferring the contours of a functional impression to the polished surfaces of digitally fabricated removable complete dentures. J. Prosthet. Dent. 2019, 124, 153–156. [Google Scholar] [CrossRef]
- Evin, A.; Souter, T.; Hulme-Beaman, A.; Ameen, C.; Allen, R.; Viacava, P.; Larson, G.; Cucchi, T.; Dobney, K. The use of close-range photogrammetry in zooarchaeology: Creating accurate 3D models of wolf crania to study dog domestication. J. Archaeol. Sci. Reports 2016, 9, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-gonz, E.; Agüera-vega, F.; Carvajal-ram, F.; Mart, P. UAV Photogrammetry Accuracy Assessment for Corridor Mapping Based on the Number and Distribution of Ground Control Points. Remote Sens. 2020, 12, 2447. [Google Scholar] [CrossRef]
- Vitale, V. The case of the middle valley of the Sinni (Southern Basilicata). Methods of archaeological and architectural documentation: 3D photomodelling techniques and use of RPAS. Digit. Appl. Archaeol. Cult. Herit. 2018, 11, e00084. [Google Scholar] [CrossRef]
- Zurita-Hernandez, J.; Ayuso-Montero, R.; Cuartero-Balana, M.; Willaert, E.; Martinez-Gomis, J. Relationship between unilateral posterior crossbite and human static body posture. Int. J. Environ. Res. Public Health 2020, 17, 5303. [Google Scholar] [CrossRef] [PubMed]
- Prado, E.; Rodr, A.; Cobo, A.; Pilar, R. 3D Fine-scale Terrain Variables from Underwater Photogrammetry: A New Approach to Benthic Microhabitat Modeling in a Circalittoral Rocky Shelf. Remote Sens. 2020, 12, 2466. [Google Scholar] [CrossRef]
- Patias, P. Medical imaging challenges photogrammetry. ISPRS J. Photogramm. Remote Sens. 2002, 56, 295–310. [Google Scholar] [CrossRef]
- Luhmann, T. Close range photogrammetry for industrial applications. ISPRS J. Photogramm. Remote Sens. 2010, 65, 558–569. [Google Scholar] [CrossRef]
- Barbero-García, I.; Cabrelles, M.; Lerma, J.L.; Marqués-Mateu, Á. Smartphone-based close-range photogrammetric assessment of spherical objects. Photogramm. Rec. 2018, 33, 283–299. [Google Scholar] [CrossRef] [Green Version]
- Kahmen, O.; Rofallski, R.; Luhmann, T. Impact of stereo camera calibration to object accuracy in multimedia photogrammetry. Remote Sens. 2020, 12, 2057. [Google Scholar] [CrossRef]
- Ariyanto, M.; Ismail, R.; Setiawan, J.D.; Yuandi, E.P. Anthropomorphic transradial myoelectric hand using tendon-spring mechanism. Telkomnika Telecommunication Comput. Electron. Control. 2019, 17, 537–548. [Google Scholar] [CrossRef]
- Ariyanto, M.; Munadi Haryadi, G.D.; Ismail, R.; Pakpahan, J.A.; Mustaqim, K.A. A low cost anthropomorphic prosthetic hand using DC micro metal gear motor. In Proceedings of the 2016 3rd International Conference on Information Technology, Computer, and Electrical Engineering, ICITACEE 2016, Semarang, Indonesia, 18–20 October 2016; pp. 42–46. [Google Scholar] [CrossRef] [Green Version]
- Kusumanto, R.D.; Tompunu, A.N. Pengolahan citra digital untuk mendeteksi obyek menggunakan pengolahan warna model normalisasi rgb. In Proceedings of the Seminar Nasional Teknologi Informasi dan Komunikasi Terapan, Semarang, Jawa Tengah, Indonesia, 16 April 2011; Volume 1. [Google Scholar]
- Zalud, K.H.L. Image Processing on Raspberry Pi for Mobile Robotics. Int. J. Signal Process. Syst. 2016, 494–498. [Google Scholar] [CrossRef]
- Wang, C.S.; Yang, W.R.; Chung, C.Y.; Chang, W.L. Application of Image Processing to Wafer Probe Mark Area Calculation. In Proceedings of the 2010 5th IEEE Conference on Industrial Electronics and Applications, ICIEA 2010, Taichung, Taiwan, 15–17 June 2010; pp. 414–419. [Google Scholar]
- Kumar, T.; Verma, K. A Theory Based on Conversion of RGB image to Gray image. Int. J. Comput. Appl. 2010, 7, 5–12. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Segment | Area (mm2) | Area Error (%) | |
|---|---|---|---|
| 3D Print | Casting | ||
| A–A′ | 2907 | 2619 | 10.99 |
| B–B′ | 5887 | 5314 | 10.78 |
| C–C′ | 4892 | 4110 | 19.03 |
| D–D′ | 1804 | 1710 | 5.50 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ismail, R.; Taqriban, R.B.; Ariyanto, M.; Atmaja, A.T.; Sugiyanto; Caesarendra, W.; Glowacz, A.; Irfan, M.; Glowacz, W. Affordable and Faster Transradial Prosthetic Socket Production Using Photogrammetry and 3D Printing. Electronics 2020, 9, 1456. https://doi.org/10.3390/electronics9091456
Ismail R, Taqriban RB, Ariyanto M, Atmaja AT, Sugiyanto, Caesarendra W, Glowacz A, Irfan M, Glowacz W. Affordable and Faster Transradial Prosthetic Socket Production Using Photogrammetry and 3D Printing. Electronics. 2020; 9(9):1456. https://doi.org/10.3390/electronics9091456
Chicago/Turabian StyleIsmail, Rifky, Rilo Berdin Taqriban, Mochammad Ariyanto, Ali Tri Atmaja, Sugiyanto, Wahyu Caesarendra, Adam Glowacz, Muhammad Irfan, and Witold Glowacz. 2020. "Affordable and Faster Transradial Prosthetic Socket Production Using Photogrammetry and 3D Printing" Electronics 9, no. 9: 1456. https://doi.org/10.3390/electronics9091456
APA StyleIsmail, R., Taqriban, R. B., Ariyanto, M., Atmaja, A. T., Sugiyanto, Caesarendra, W., Glowacz, A., Irfan, M., & Glowacz, W. (2020). Affordable and Faster Transradial Prosthetic Socket Production Using Photogrammetry and 3D Printing. Electronics, 9(9), 1456. https://doi.org/10.3390/electronics9091456