Meta-Analysis on the Effectiveness of Virtual Reality Cognitive Training (VRCT) and Computer-Based Cognitive Training (CBCT) for Individuals with Mild Cognitive Impairment (MCI)

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Appraisal of Study Quality
2.5. Analytical Approach
3. Results
3.1. Search Results
3.2. Data Extraction and Analysis
3.3. Cohort Characteristics
Country of Origin
3.4. Individuals Characteristics
Age and Gender
3.5. Compliance and Attrition Factors
3.6. Intervention Outcomes
3.7. Correlation between the Five Cognitive Domains
3.8. Comparison between CBCT and VRCT
Cognitive Measurements Used
3.9. Intervention Results
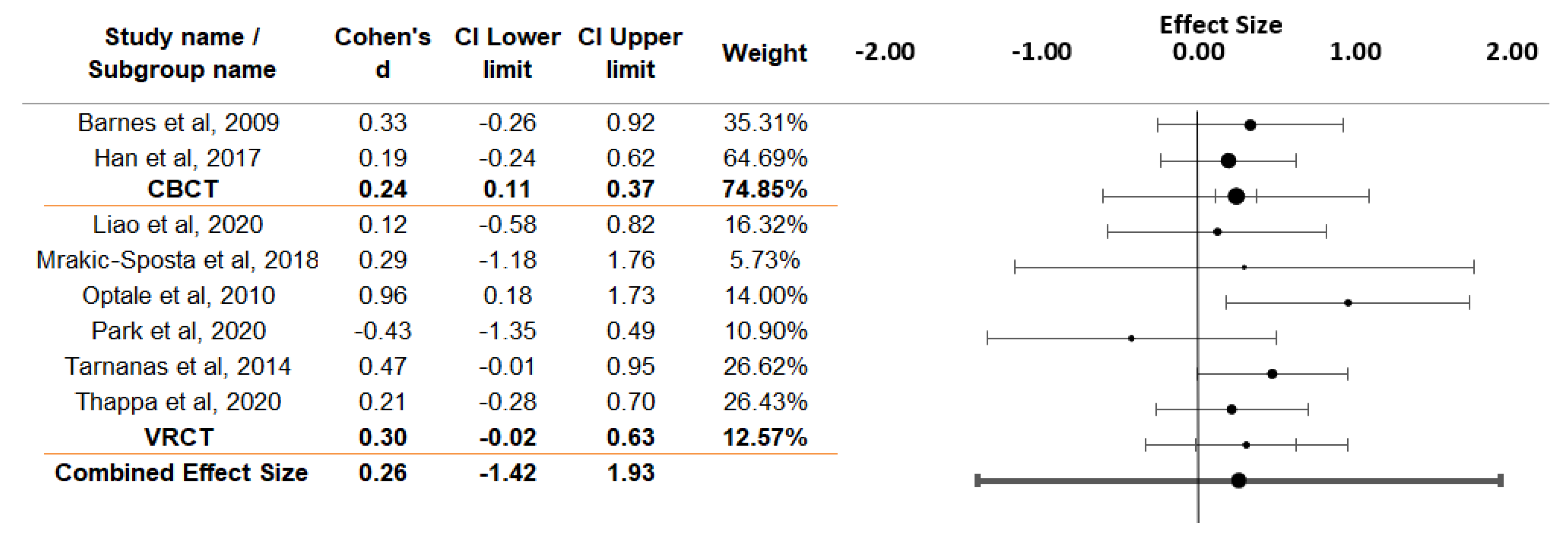
3.10. Overall Analysis
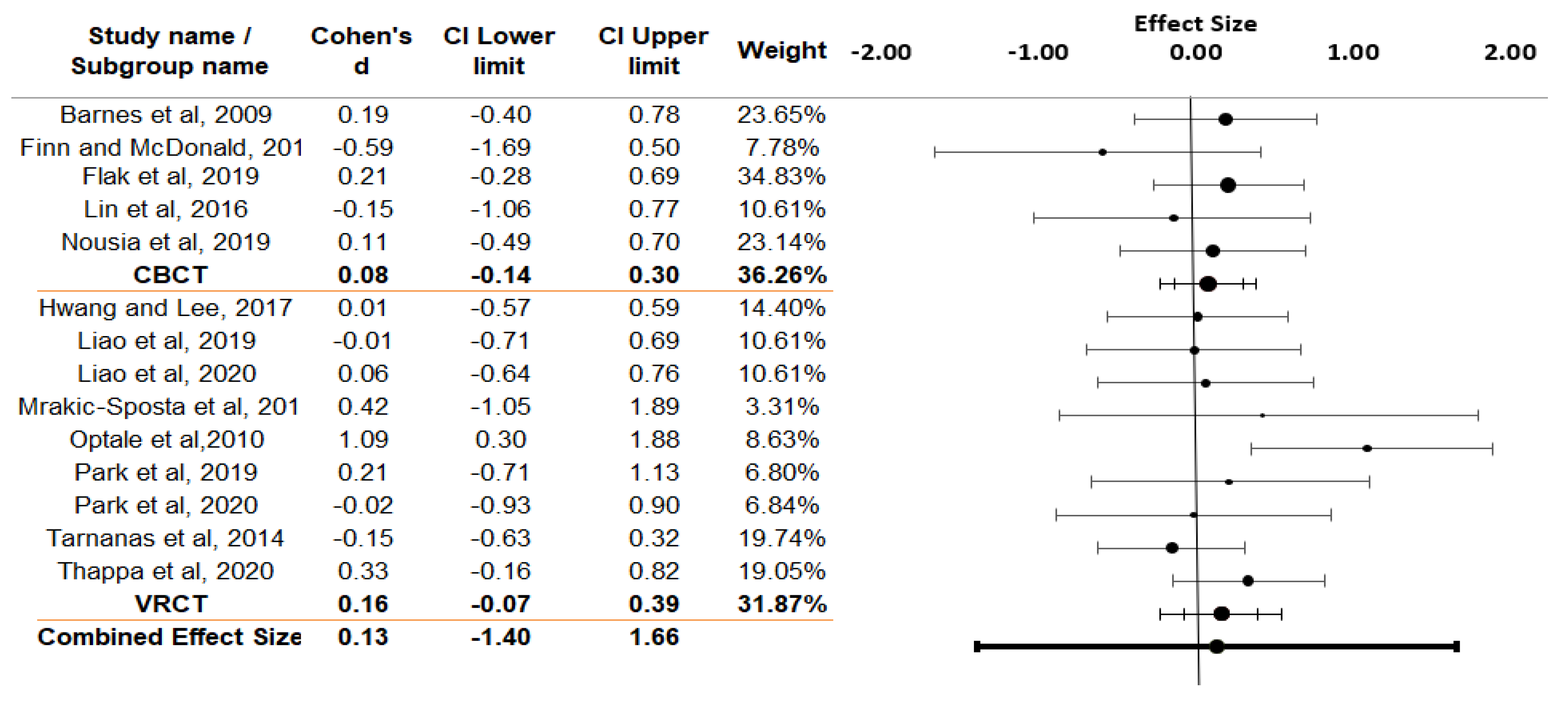
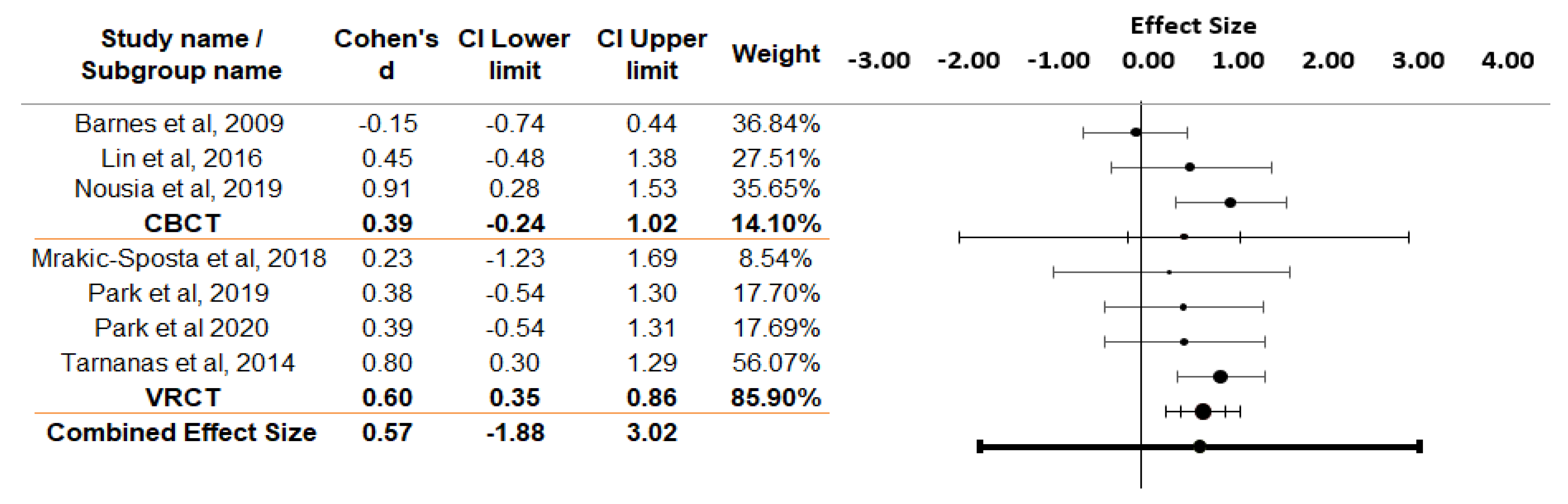
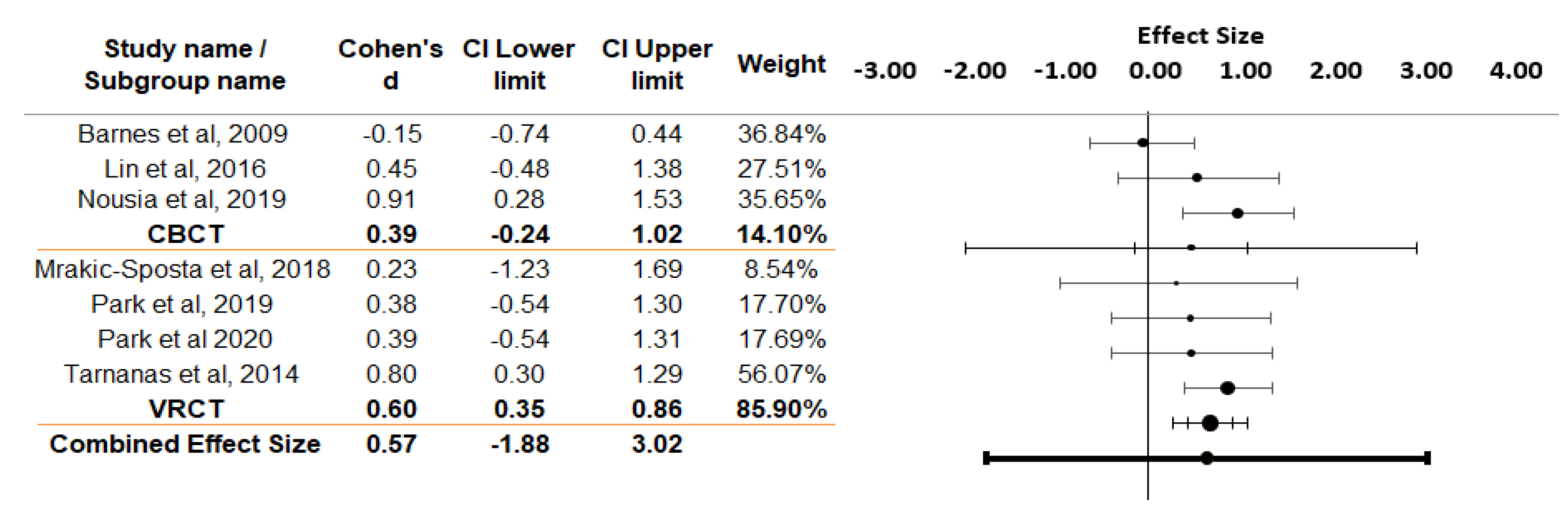
3.11. Effect Sizes According to Different Cognitive Domains
4. Discussions
4.1. Effectiveness of CBCT and VRCT
4.2. Trend of Rehabilitation
4.3. Advantages of CBCT
4.4. Limitations of CBCT
4.5. Advantages of VRCT
4.6. Limitations of VRCT
4.7. Comparison between CBCT and VRCT
Advantages of VRCT over CBCT
4.8. Common Limitations of CBCT and VRCT
4.9. Compliance and Attrition Factor
4.10. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 29 April 2020).
- Prince, M.; Ali, G.-C.; Guerchet, M.; Prina, A.M.; Albanese, E.; Wu, Y.-T. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimers Res. Ther. 2016, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Saunders, N.L.; Summers, M.J. Longitudinal deficits to attention, executive, and working memory in subtypes of mild cognitive impairment. Neuropsychologia 2011, 25, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Storandt, M.; Grant, E.; Miller, J.; Morris, J. Longitudinal course and neuropathological outcomes in original versus revised MCI and in PreMCI. Neurology 2006, 67, 467–473. [Google Scholar] [CrossRef]
- Ge, S.; Zhu, Z.; Wu, B.; McConnell, E.S. Technology-based cognitive training and rehabilitation interventions for individuals with mild cognitive impairment: A systematic review. BMC Geriatr. 2018, 18, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchoł, Ł.; Kędziora-Kornatowska, K.; Araszkiewicz, A.; Izdebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: A pretest-posttest design pilot study. BMC Res. Notes 2019, 12, 776–778. [Google Scholar] [CrossRef]
- Kim, O.; Pang, Y.; Kim, J.-H. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry 2019, 19, 219. [Google Scholar] [CrossRef]
- Manera, V.; Chapoulie, E.; Bourgeois, J.; Guerchouche, R.; David, R.; Ondrej, J.; Drettakis, G.; Robert, P. A feasibility study with image-based rendered virtual reality in patients with mild cognitive impairment and dementia. PLoS ONE 2016, 11, e0151487. [Google Scholar] [CrossRef]
- Coyle, H.; Traynor, V.; Solowij, N. Computerized and virtual reality cognitive training for individuals at high risk of cognitive decline: Systematic review of the literature. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2014, 23. [Google Scholar] [CrossRef]
- Gates, N.J.; Sachdev, P.S.; Fiatarone Singh, M.A.; Valenzuela, M. Cognitive and memory training in adults at risk of dementia: A systematic review. BMC Geriatr. 2011, 11, 55. [Google Scholar] [CrossRef]
- Lampit, A.; Hallock, H.; Valenzuela, M. Computerized cognitive training in cognitively healthy older adults: A systematic review and meta-analysis of effect modifiers. PLoS Med. 2014, 11, e1001756. [Google Scholar] [CrossRef]
- Kurz, A.; Leucht, S.; Lautenschlager, N. The clinical significance of cognition-focused interventions for cognitively impaired older adults: A systematic review of randomized controlled trials. Int. Psychogeriatr. IPA 2011, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Schofield, D. Cognitive Deficits. 2018. Available online: https://emedicine.medscape.com/article/917629-overview (accessed on 2 May 2020).
- Brinley, J.F.; Jovick, T.J.; McLaughlin, L.M. Age, reasoning, and memory in adults. J. Gerontol. 1974, 29, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Finn, M.; McDonald, S. Computerised cognitive training for older persons with mild cognitive impairment: A pilot study using a randomised controlled trial design. Brain Impair. 2012, 12, 187–199. [Google Scholar] [CrossRef]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Faria, C.D.A.; Alves, H.V.D.; Charchat-Fichman, H. The most frequently used tests for assessing executive functions in aging. Dement. Neuropsychol. 2015, 9, 149–155. [Google Scholar] [CrossRef]
- Maseda, A.; Fernández, L.L.; Lorenzo-López, L.; Núñez-Naveira, L.; Balo, A.; Calenti, J.M. Verbal fluency, naming and verbal comprehension: Three aspects of language as predictors of cognitive impairment. Aging Ment. Health 2014, 18, 1–9. [Google Scholar] [CrossRef]
- Llorente, M.D. Dementia: Comprehensive principles and practice. J. Nerv. Ment. Dis. 2015, 203, 978. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- van Rhee, H.; Suurmond, R.; Hak, T. User manual for meta-essentials: Workbooks for meta-analysis. Erasmus Res. Inst. Manag. 2015. [Google Scholar] [CrossRef]
- Flak, M.M.; Hol, H.R.; Hernes, S.S.; Chang, L.; Engvig, A.; Bjuland, K.J.; Pripp, A.; Madsen, B.O.; Knapskog, A.B.; Ulstein, I.; et al. Adaptive computerized working memory training in patients with mild cognitive impairment. A randomized double-blind active controlled trial. Front. Psychol. 2019, 10, 807. [Google Scholar] [CrossRef]
- Man, D.W.; Chung, J.C.; Lee, G.Y. Evaluation of a virtual reality-based memory training programme for Hong Kong Chinese older adults with questionable dementia: A pilot study. Int. J. Geriatr. Psychiatry 2012, 27, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Thapa, N.; Park, H.J.; Yang, J.G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The effect of a virtual reality-based intervention program on cognition in older adults with mild cognitive impairment: A randomized control trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef] [PubMed]
- Nousia, A.; Martzoukou, M.; Siokas, V.; Aretouli, E.; Aloizou, A.M.; Folia, V.; Peristeri, E.; Messinis, L.; Nasios, G.; Dardiotis, E. Beneficial effect of computer-based multidomain cognitive training in patients with mild cognitive impairment. Appl. Neuropsychol. Adult 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Herrera, C.; Chambon, C.; Michel, B.F.; Paban, V.; Alescio-Lautier, B. Positive effects of computer-based cognitive training in adults with mild cognitive impairment. Neuropsychologia 2012, 50, 1871–1881. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Lee, S. The effect of virtual reality program on the cognitive function and balance of the people with mild cognitive impairment. J. Phys. Ther. Sci. 2017, 29, 1283–1286. [Google Scholar] [CrossRef]
- Optale, G.; Urgesi, C.; Busato, V.; Marin, S.; Piron, L.; Priftis, K.; Gamberini, L.; Capodieci, S.; Bordin, A. Controlling memory impairment in elderly adults using virtual reality memory training: A randomized controlled pilot study. Neurorehabil. Neural Repair 2010, 24, 348–357. [Google Scholar] [CrossRef]
- Park, E.; Yun, B.-J.; Min, Y.-S.; Lee, Y.-S.; Moon, S.-J.; Huh, J.-W.; Cha, H.; Chang, Y.; Jung, T.-D. Effects of a mixed reality-based cognitive training system compared to a conventional computer-assisted cognitive training system on mild cognitive impairment: A pilot study. Cognit. Behav. Neurol. 2019, 32, 172–178. [Google Scholar] [CrossRef]
- Park, J.-H.; Liao, Y.; Kim, D.R.; Song, S.; Lim, J.H.; Park, H.; Lee, Y.; Park, K.W. Feasibility and Tolerability of a Culture-Based Virtual Reality (VR) Training program in patients with mild cognitive impairment: A randomized controlled pilot study. Int. J. Environ. Res. Public Health 2020, 17, 3030. [Google Scholar] [CrossRef]
- Barnes, D.E.; Yaffe, K.; Belfor, N.; Jagust, W.J.; DeCarli, C.; Reed, B.R.; Kramer, J.H. Computer-based cognitive training for mild cognitive impairment: Results from a pilot randomized, controlled trial. Alzheimer Dis. Assoc. Disord. 2009, 23, 205–210. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Chen, I.H.; Lin, Y.J.; Chen, Y.; Hsu, W.C. Effects of virtual reality-based physical and cognitive training on executive function and dual-task gait performance in older adults with mild cognitive impairment: A randomized control trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Mrakic-Sposta, S.; Di Santo, S.G.; Franchini, F.; Arlati, S.; Zangiacomi, A.; Greci, L.; Moretti, S.; Jesuthasan, N.; Marzorati, M.; Rizzo, G.; et al. Effects of combined physical and cognitive virtual reality-based training on cognitive impairment and oxidative stress in MCI patients: A pilot study. Front. Aging Neurosci. 2018, 10, 282. [Google Scholar] [CrossRef] [PubMed]
- Tarnanas, I.; Tsolakis, A.; Tsolaki, M. Assessing virtual reality environments as cognitive stimulation method for patients with MCI. Stud. Comput. Intell. 2014, 536, 39–74. [Google Scholar] [CrossRef]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Kokmen, E.; Tangelos, E.G. Aging, memory, and mild cognitive impairment. Int. Psychogeriatr. 1997, 9, 65–69. [Google Scholar] [CrossRef]
- Smith, G.; Housen, P.; Yaffe, K.; Ruff, R.; Kennison, R.; Mahncke, H.; Zelinski, E. A cognitive training program based on principles of brain plasticity: Results from the Improvement in Memory with Plasticity-based Adaptive Cognitive Training (IMPACT) Study. J. Am. Geriatr. Soc. 2009, 57, 594–603. [Google Scholar] [CrossRef]
- Chang, Y.-L.; Jacobson, M.; Fennema-Notestine, C.; Hagler, D.; Jennings, R.; Dale, A.; McEvoy, L. Level of executive function influences verbal memory in amnestic mild cognitive impairment and predicts prefrontal and posterior cingulate thickness. Cereb. Cortex (N.Y. 1991) 2009, 20, 1305–1313. [Google Scholar] [CrossRef]
- Emery, V.O.B. Language impairment in dementia of the alzheimer type: A hierarchical decline? Int. J. Psychiatry Med. 2000, 30, 145–164. [Google Scholar] [CrossRef]
- Taylor, J.R.; Olichney, J.M. From amnesia to dementia: ERP studies of memory and language. Clin. EEG Neurosci. 2007, 38, 8–17. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.; Rettinger, D.; Shah, P.; Hegarty, M. How are visuospatial working memory, executive functioning, and spatial abilities related? A latent-variable analyses. J. Exp. Psychol. Gen. 2001, 130, 621–640. [Google Scholar] [CrossRef]
- Vazou, S.; Smiley-Oyen, A. Moving and academic learning are not antagonists: Acute effects on executive function and enjoyment. J. Sport Exerc. Psychol. 2014, 36, 474–485. [Google Scholar] [CrossRef]
- Duff, K.; Schoenberg, M.R.; Scott, J.G.; Adams, R.L. The relationship between executive functioning and verbal and visual learning and memory. Arch. Clin. Neuropsychol. 2005, 20, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Kueider, A.M.; Parisi, J.M.; Gross, A.L.; Rebok, G.W. Computerized cognitive training with older adults: A systematic review. PLoS ONE 2012, 7, e40588. [Google Scholar] [CrossRef] [PubMed]
- Han, J.W.; Son, K.L.; Byun, H.J.; Ko, J.W.; Kim, K.; Hong, J.W.; Kim, T.H.; Kim, K.W. Efficacy of the Ubiquitous Spaced retrieval-based Memory Advancement and Rehabilitation Training (USMART) program among patients with mild cognitive impairment: A randomized controlled crossover trial. Alzheimers Res. Ther. 2017, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.; Heffner, K.L.; Ren, P.; Tivarus, M.E.; Brasch, J.; Chen, D.G.; Mapstone, M.; Porsteinsson, A.P.; Tadin, D. Cognitive and Neural effects of vision-based speed-of-processing training in older adults with amnestic mild cognitive impairment: A pilot study. J. Am. Geriatr. Soc. 2016, 64, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.; Weinborn, M.; Verdile, G.; Sohrabi, H.; Martins, R. Enhancing cognitive functioning in healthly older adults: A systematic review of the clinical significance of commercially available computerized cognitive training in preventing cognitive decline. Neuropsychol. Rev. 2017, 27, 62–80. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cognitive Domains | Cognitive Measurements Used | |
|---|---|---|
| CBCT | VRCT | |
| GCF | RBANS total score (5 RBANS index score), Dementia Rating Scale-2 (DRS-2), Mini-Mental State Examination (MMSE), Cambridge Neuropsychological Test Automated Battery (CANTAB). | Montreal Cognitive Assessment (MoCA), Mental Status in Neurology, Mini-Mental State Examination (MMSE), Korean Version of Mini Mental Status Examination (MMSE-K), Mini-Mental State Examination for Dementia Screening (MMSE-DS). |
| Mem | Immediate and delayed recall: Repeatable Battery for Assessment of Cognitive Status (RBANS), California Verbal Learning Test (CVLT-II), Word-List Mem Test (WLMT), Word List Recall Test (WLRT), Word List Recognition Test (WLRcT), Immediate word recall, Delayed word Mem test. Mem in everyday living: The Measurement of Everyday Cognition (ECOG), CANTAB- MFQ (Mem Functioning Questionnaire), Subjective Mem Complaints Questionnaire (SMCQ). Visual Mem: CANTAB- PAL (Paired Associates Learning), CANTAB- PRM (Pattern recognition Mem), Rey Complex Figure Test and Recognition Trial (RCFT), Wechsler Mem Scale WMS-III Faces I and II, visual recognition subtest from the Doors and People Mem battery, Delayed Matching-to-Sample Task 48 (DMS48). Verbal Mem: Logical Mem II Delayed recall, CVLT-II Long delay free recall, CVLT Total hits, Digit Span Test, 12-word-list recall from BEM-144 Mem battery, the 16-item free and cued reminding test (16-FR/CR test), sub-score recall of the MMSE. | Immediate and delayed recall: Fuld Object Mem Evaluation (FOME), the Word List Recall Test, the Word List Recognition Test. Mem in everyday living: Multifactorial Mem Questionnaire (MMQ). Visual Mem: Visual Span Test (VST). Verbal Mem: Chinese version of the Verbal Learning Test (CVVLT), The Rey Auditory Verbal Learning Test (RAVLT), Digit Span Test, Verbal Story Recall Test (VSR), Word List Learning Test. |
| EF | Attention: Repeatable Battery for Assessment of Neuropsychological Status (RBANS) attention subtest, Rapid visual information processing (RVP), Digit Span Forward (DSF), Digit Span Backward (DSB). Mental flexibility: Set shifting and flanker tasks from Executive Abilities: Measures and Instruments for Neurobehavioral Evaluation and Research (EXAMINER), Intra-/extra-dimensional set shifting (IED), Trail Making Test (TMT-A and TMT-B), Design fluency test. Inhibitory control: Delis–Kaplan EF System (D-KEFS) Working Mem: Digit Span Forward (DSF), Digit Span Backward (DSB) test, Spatial span test, Wechsler Mem Scale- Letter Number Sequencing, Dot counting and 1-back. Speed of processing: Trail Making Test (TMT-A and TMT-B). | Attention: Word Color Test (WCT), Digit Span Forward (DSF), Digit Span Backward (DSB) test. Mental flexibility: Trail making test (TMT-A, TMT-B), Dual Task Performance (DTP) test, Letter fluency test. Inhibitory control: Stroop test, Symbol Digit Modalities Test, The Stroop Color and Word Test (SCWT), Stroop interference test. Working Mem: Cognitive Estimation Test (CET), Digit Span Forward (DSF), Digit Span Backward (DSB) test. Speed of processing: Trail making test (TMT-A, TMT-B) test. Overall EF: Frontal Assessment Battery (FAB), The Executive Interview 25 (EXIT-25). |
| Lang | Verbal fluency: Controlled Oral Word Association Test (COWAT), Semantic Fluency (SF), phonemic and categorical task from Executive Abilities: Measures and Instruments for Neurobehavioral Evaluation and Research (EXAMINER), semantic fluency task from Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). Naming: The Boston Naming Test (BNT), picture naming task from Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). | Verbal fluency: Verbal Fluency Test (VF), Word Fluency Test (category and letter fluency), Category fluency tasks. Naming: 15-items short-form of the Boston Naming Test, the Korean version of Boston Naming Test. |
| VS | Repeatable Battery for Assessment of Cognitive Status (RBANS) visuospatial subtest, Clock Drawing Test, Rey–Osterrieth Complex Figure. | Rey-Osterrieth Complex Figure Test (ROCFT), Clock Drawing Test, the Attentional Matrices Test (AM), the Trail Making Test A (TMT-A), Constructional Praxis Test, Constructional Recall Test. |
| Cognitive Domains | Citation | Sub-Domains | CBCT/VRCT | Cognitive Measurement Used | Statistically Significant Improvement (p < 0.05) | Effect Size | Remarks/Comments |
|---|---|---|---|---|---|---|---|
| GCF | Barnes et al., 2009 | N.A. | CBCT | RBANS total score | Yes | d = 0.33 | |
| Chandler et al., 2017 | N.A. | CBCT | DRS-2 | Yes | N.A. | ||
| Han et al., 2017 | N.A. | CBCT | MMSE | No | d = 0.19 | ||
| Liao et al., 2020 | N.A. | VRCT | MoCA | Yes | d = 0.12 | ||
| Mrakic-Sposta et al., 2018 | N.A. | VRCT | MMSE | Yes | d = 0.29 | ||
| Optale et al., 2010 | N.A. | VRCT | MMSE | Yes | d = 1.40 | ||
| N.A. | VRCT | Mental Status of Neurology | Yes | d = 0.51 | |||
| Park et al., 2020 | N.A. | VRCT | K-MMSE | No | d = −0.43 | K-MMSE scores did not change significantly in either groups after 12 weeks | |
| Tarnanas et al., 2014 | N.A. | VRCT | MMSE | No | d = 0.47 | ||
| Thapa et al., 2020 | N.A. | VRCT | MMSE-DS | No | d = 0.21 | ||
| Mem | Barnes et al., 2009 | Immediate and delayed recall | CBCT | RBANS delayed Mem | Yes | d = 0.53 | |
| Chandler et al., 2017 | Mem Activities of Daily Living | CBCT | ECOG | No | d = 0.54 | ||
| Finn and McDonald, 2012 | Overall Mem | CBCT | PAL errors | No | d = −1.15 | ||
| Flak et al., 2019 | Visual Mem | CBCT | RCFT Delayed Recall | No | d = 0.29 | The training group tended to perform better on both learning (encoding) and delayed recall (retrieval) on a word list task. | |
| Verbal Mem | CBCT | CVLT-II Long delay free recall | No | d = 0.20 | The training group tended to perform better on both learning (encoding) and delayed recall (retrieval) on a word list task. | ||
| Herrera et al., 2012 | Immediate and delayed recall | CBCT | BEM-14412-word-list recall test | Yes | d = 1.45 | The training group improved at both post-test and 6-month follow up, indicating training improved recall. | |
| Man et al., 2012 | Immediate and delayed recall | VRCT | FOME score in total retrieval | Yes | d = 1.25 | Improvement in immediate recall of episodic Mem. | |
| Mem in everyday living | VRCT | MMQ-strategy | Yes | d = 0.70 | There was significant impact in subjective perception of Mem function and use of Mem strategies. | ||
| Hwang and Lee, 2017 | Visual Mem | VRCT | Visual span | Yes | d = 0.67 | ||
| Optale et al., 2010 | Verbal Mem | VRCT | VSR | Yes | d = 1.12 | ||
| Tarnanas et al., 2014 | Verbal Mem | VRCT | RAVLT | Yes | d = 0.133 | ||
| Liao et al., 2020 | Verbal Mem Immediate and delayed recall | VRCT | CVVLT | Yes | Immediate recall: d = 0.21 Delayed recall: d = 0.19 | ||
| Mrakic-Sposta et al., 2018 | Verbal Mem | VRCT | RAVLT_I | No | d = 0.61 | The training group showed a greater improvement than control group in the Mem functions and the study was limited by relatively small number of individuals, i.e., 10 in total. | |
| Park et al., 2019 | Immediate and delayed recall | VRCT | WLRT | No | d = 0.06 | ||
| EF | Finn and McDonald, 2012 | Visual sustained attention | CBCT | RVP A mean scores | Yes | d = 1.12 | There is a combined effect of gains in the treatment group following training, and a decline in the waitlist group’s RVP A scores, leading to a significant effect on visual sustained attention. |
| Lin et al., 2016 | Processing speed | CBCT | CEN connectivity | Yes | d = 0.12 | ||
| Working Mem | CBCT | Dot counting and 1-back | Yes | d = 0.28 | |||
| Nousia et al. 2019 | Mental flexibility | CBCT | TMT-A | Yes | d = 0.54 | Even though EF scores were still low before and after the training, the training group improved significantly when compared to the control group. | |
| Barnes et al., 2009 | Attention | CBCT | RBANS attention | No | d = 0.04 | There was no consistent pattern for measures of attention or EF. | |
| Flak et al., 2019 | Overall EF | CBCT | D-KEFS | No | d = 0.21 | No significant differences in training effects on composite scores of EF. | |
| Hwang and Lee, 2017 | Attention | VRCT | WCT | Yes | d = 0.05 | ||
| Liao et al., 2019 | Inhibitory control | VRCT | SCWT | Yes | d = 0.01 | ||
| Mental flexibility | VRCT | TMT-A | Yes | d = 0.07 | |||
| Optale et al., 2010 | Mental flexibility | VRCT | DTP | Yes | d = 1.08 | ||
| Tarnanas et al., 2014 | Mental flexibility | VRCT | TMT-B | Yes | d = 2.11 | Significantly improved at the 5-month follow-up. | |
| Thapa et al., 2020 | Mental flexibility | VRCT | TMT-B | Yes | d = −0.48 | Both groups showed improved EF but significant within group effects were only noted for the VR group. | |
| Liao et al., 2020 | Overall EF | VRCT | EXIT-25 | Yes | d = 0.65 | ||
| Mrakic-Sposta et al., 2018 | Overall EF | VRCT | FAB | No | d = 0.42 | Weak effect of treatment on EF was observed. | |
| Park et al., 2019 | Mental flexibility | VRCT | TMT-B | No | d = 0.42 | ||
| Park et al., 2020 | Inhibitory control | VRCT | Stroop test | No | d = −0.45 | ||
| Lang | Nousia et al., 2019 | Naming | CBCT | Boston Naming Test | Yes | d = 0.93 | |
| Verbal fluency | CBCT | Semantic Fluency | Yes | d = 0.88 | |||
| Barnes et al., 2009 | Verbal fluency | CBCT | Verbal fluency | No | d = −0.22 | The effect size tended to favor control conditions, which included listening to books. | |
| Naming | CBCT | Boston Naming Test | No | d = −0.23 | The effect size tended to favor control conditions, which included listening to books. | ||
| Lin et al., 2016 | Verbal fluency | CBCT | Verbal fluency | No | d = 0.45 | ||
| Mrakic-Sposta et al., 2018 | Verbal fluency | VRCT | Verbal fluency | No | d = 0.23 | Intervention group showed a greater improvement in Lang measures than the control group. | |
| Tarnanas et al., 2014 | Verbal fluency | VRCT | Category fluency | No | d = 0.04 | ||
| VS | Barnes et. al, 2009 | N.A. | CBCT | RBANS visuospatial | Yes | d = −0.51 | |
| Nousia et al., 2019 | N.A. | CBCT | Clock drawing test | Yes | d = −1.58 | CDT requires constructional praxis abilities. The ability may not be tested adequately for possible improvement in spatial orientation. | |
| Herrera et al., 2012 | N.A. | CBCT | ROCFT | No | d = 0.06 | ||
| Tarnanas et al., 2014 | N.A. | VRCT | ROCFT copy and immediate recall | Yes | d = 0.58 | The immediate recall in the ROCFT was improved significantly at the 5-month follow-up. | |
| Park et al., 2019 | N.A. | VRCT | Constructional Recall Test | Yes | d = 0.94 | ||
| Optale et al., 2010 | N.A. | VRCT | Clock drawing test | No | d = 0.83 | ||
| Mrakic-Sposta et al., 2018 | N.A. | VRCT | ROCFT | No | d = 0.19 | Weak effect of the treatment on visuo-constructive abilities was observed. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, S.C.-w.; Ho, A.Y.-n.; Lai, I.H.-w.; Lee, C.S.-w.; Pong, A.S.-k.; Lai, F.H.-y. Meta-Analysis on the Effectiveness of Virtual Reality Cognitive Training (VRCT) and Computer-Based Cognitive Training (CBCT) for Individuals with Mild Cognitive Impairment (MCI). Electronics 2020, 9, 2185. https://doi.org/10.3390/electronics9122185
Hung SC-w, Ho AY-n, Lai IH-w, Lee CS-w, Pong AS-k, Lai FH-y. Meta-Analysis on the Effectiveness of Virtual Reality Cognitive Training (VRCT) and Computer-Based Cognitive Training (CBCT) for Individuals with Mild Cognitive Impairment (MCI). Electronics. 2020; 9(12):2185. https://doi.org/10.3390/electronics9122185
Chicago/Turabian StyleHung, Sarah Chui-wai, Annie Yin-ni Ho, Idy Hiu-wai Lai, Carol Sze-wing Lee, Angela Shuk-kwan Pong, and Frank Ho-yin Lai. 2020. "Meta-Analysis on the Effectiveness of Virtual Reality Cognitive Training (VRCT) and Computer-Based Cognitive Training (CBCT) for Individuals with Mild Cognitive Impairment (MCI)" Electronics 9, no. 12: 2185. https://doi.org/10.3390/electronics9122185
APA StyleHung, S. C.-w., Ho, A. Y.-n., Lai, I. H.-w., Lee, C. S.-w., Pong, A. S.-k., & Lai, F. H.-y. (2020). Meta-Analysis on the Effectiveness of Virtual Reality Cognitive Training (VRCT) and Computer-Based Cognitive Training (CBCT) for Individuals with Mild Cognitive Impairment (MCI). Electronics, 9(12), 2185. https://doi.org/10.3390/electronics9122185