


The DtMin Protocol: Implementing Data Minimization Principles in Medical Information Sharing

Abstract
1. Introduction
1.1. Problem Identification
1.2. Objectives and Methods
- Data Classification System: Attributes are classified into six categories based on sensitivity (ciphertext/plaintext), patient consent/non-consent, and EHR request/non-request, applying different encryption methods to each level.
- Multiple Encryption: Different encryption methods are used according to the type of attribute.
- Hybrid Encryption: Shared key generation is performed via a key exchange method.
- Multi-Layer Encryption Process:
- First Encryption: Encrypts using the doctor’s private key/public key based on the patient’s consent/non-consent.
- Second Encryption: Further encrypts with the HCP’s secret key.
- Decryption: Decrypts with HCP’s secret key only for the attributes which EHRP requested to be shared.
- Re-Encryption: Re-encrypts with a sharing key for the sensitive attributes in ciphertext.
1.3. Contributions
- Attributes are classified based on six criteria: sensitivity (ciphertext/plaintext), patient consent/non-consent, and EHR request/non-request, using different encryption methods for each. This forms the basis for implementing a selective sharing mechanism, achieving fine cryptographic access control (Fine CAC) that enables fine-grained access control.
- This protocol is designed to practically implement the data minimization principle emphasized in modern privacy regulations such as GDPR, meeting the regulatory requirements and privacy principles that must be adhered to during information sharing in healthcare.
- By integrating attribute-based encryption (ABE) with the data minimization principle, an encryption infrastructure is established that inherently enforces minimal data disclosure. Traditional healthcare information sharing systems handle data in an “All-or-Nothing” manner. In contrast, DtMin selectively shares only the intersection of attributes consented to by the patient and requested by the EHRP.
- Quantitative performance evaluation and theoretical security analysis are provided; the performance of the proposed protocol is actually measured and analyzed based on varying data sizes and numbers of patients (see Section 6), and formal security proofs are used to rigorously analyze the security of the protocol (see Section 5).
- As a result, efficiency is improved: (1) the amount of data to be processed is reduced, lowering computational costs; (2) system efficiency is enhanced due to reduced storage and transmission requirements; and (3) the security overhead is reduced by limiting the range of data requiring security management.
- Consequently, DtMin ensures minimal information sharing based on patient consent and data sensitivity, drastically reducing unnecessary data exposure.
- This approach becomes a practical solution that can significantly reduce the risk of privacy breaches and regulatory non-compliance in real healthcare environments.
- As future enhancements, we explore strategies to apply advanced cryptographic techniques to DtMin in complex, diverse, and large-scale healthcare environments to adhere to the principle of data minimization.
2. Related Works
2.1. Characteristics of Medical Information
2.2. Sharing of Medical Information
2.3. Data Minimization Principle
2.3.1. Regulation
2.3.2. Research Papers Emphasizing the Importance of the Principle of Minimization
3. Preliminaries
3.1. Application Scenario and Participants
3.1.1. Participants
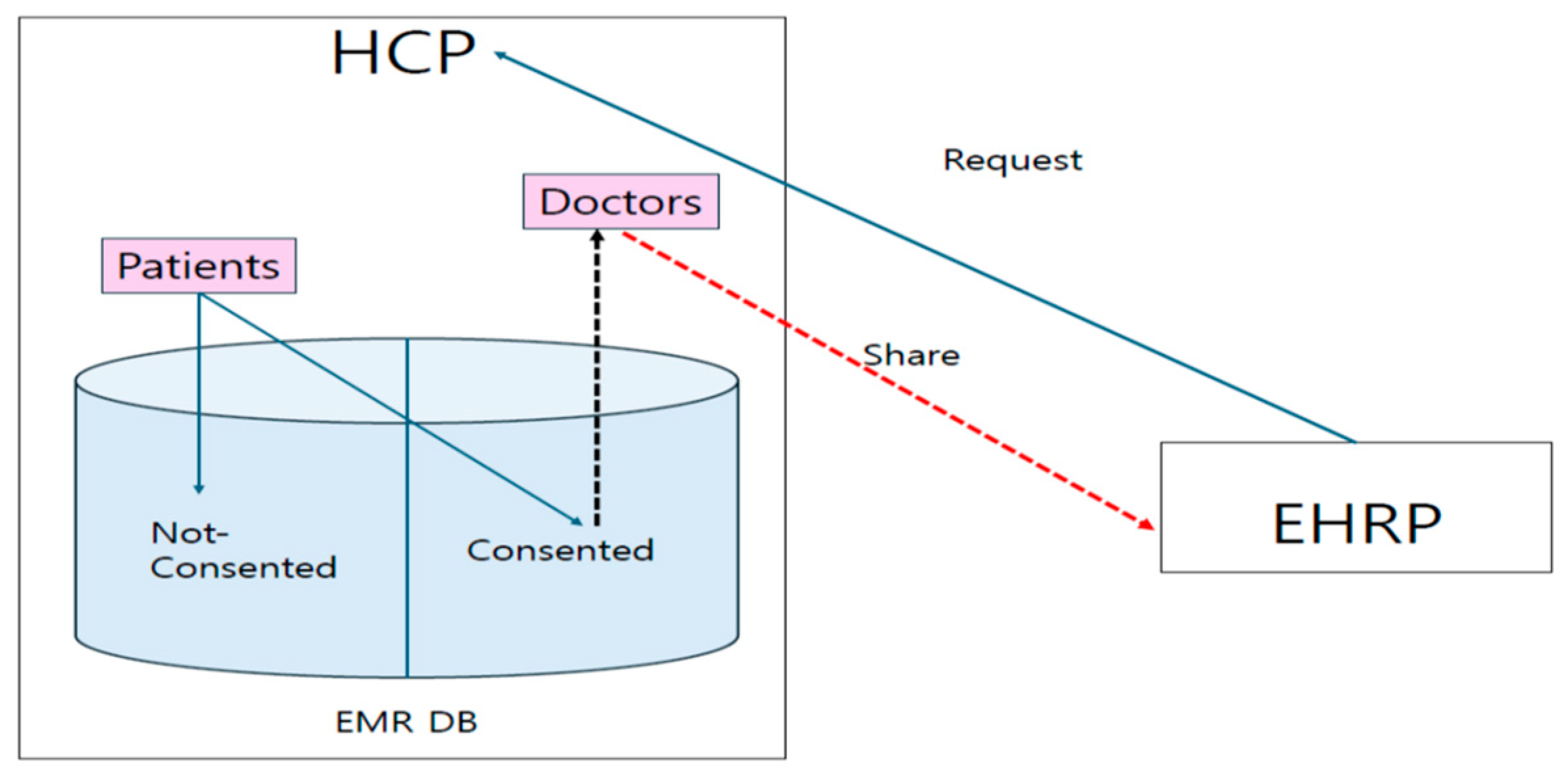
- HCP (HealthCare Provider): This is an institution that provides medical services, such as hospitals, clinics, and public health centers. HCPs use an electronic medical record (EMR) system.
- EHRP (EHR Provider): This is an entity that uses an electronic health record (EHR) system, such as insurance companies and government health agencies.
- Patients and Doctor: These are individuals registered with the HCP. The doctor makes the final decision on whether to share only the information the patient has consented to share.
- Server Administrator: This is the HCP’s server manager responsible for managing patient data.
3.1.2. Application Scenario
3.2. Notation
- : pseudorandom function for symmetric encryption
- : reverse function of , in other words, decryption function of
- : asymmetric encryption/decryption function
- : encryption functions f and E for message M with the encryption key K
- : re-encryption with a sharing key for all attributes
- : doctor’s private/public key
- : ID and password of EHRP
- sk: HCP server’s secret key for symmetric encryption
- : random number generated for every session j
- : sharing key between HCP and EHRP
- : consented/non-consented attributes
- : authentication polynomial
- : share-requested attributes of user i
- At_t: t-th attributes
- : requested sharing attributes in the consented/non-consented attributes of user i
- : non-requested sharing attributes in the consented/non-consented attributes of user i
3.3. Security Building Blocks
- -
- Encryption: A message (M) is encrypted using the public key () to produce a ciphertext (C). This process can be mathematically represented as C = E(, M), where (E) denotes the encryption function.
- -
- Decryption: The ciphertext (C) is decrypted using the private key () to retrieve the original message (M). Mathematically, this is represented as M = D(, C), where (D) denotes the decryption function [9].
- -
- In this study, we use RSA as a public key cryptography:
- such that Where, e is a public key, and d is a private key.
- Encryption: Decryption: (M is a message).
- RSA’s security is based on the intractability of the Integer Factorization Problem (IFP) for sufficiently large integers. RSA operates within the multiplicative group of integers modulo n, denoted as , [23].
3.4. Algorithms
- SysPrm () → λ: The parameter-generating algorithm SysPrm takes a security parameter s as input and generates a set of system parameters λ.
- KGenRg () → Pr, Pu, sk, ID, PW: Given λ as input, the key generation and registration algorithm KGenRg generates a public key Pu and a private key Pr for each participant and a secret key for HCP, and ID/PW for each participant.
- EnCDB (Pr, Pu, sk, ) → 1st and 2nd Enc.: The inputs for DB Encryption algorithm EnCDB are {Pr, Pu, sk, The outputs are 1st and 2nd Encryptions. The first one is that and are encrypted with different keys. The second one on top of that is encrypted with the HCP’s secret key.
- MuAuth (vrfinf, ) → Verified or Fail: Given verifiable information vrfinf and random number , the mutual authentication algorithm MuAuth outputs Verified or Fail.
- ShKGen (Verified, , Pr, ) → ShKey: If the verification is successful, the sharing key generation algorithm ShKGen produces the sharing key ShKey between HCP and EHRP.
- ShRq ( This sharing request algorithm ShRq takes as an input and HCP decrypts the requested attributes.
- ReEnC (ShKey The re-encryption algorithm ReEnC encrypts for all attributes again with the sharing key.
- Dec (ShKey, Pu): The decryption algorithm Dec decrypts all attributes with the shaing key ShKey first, then secondly decrypts with the public key. The result is the requested attributes in plaintext and others in ciphertext.
3.5. Attribute Types of Database
3.6. Authentication Polynomial (AP)
4. Construction of DtMin Encryption Protocol
4.1. System Setting and Registration
4.1.1. SysPrm ()
- 1.
- Input: s (security parameter)
- 2.
- Output: λ (system parameters’ set) = {}
4.1.2. KGenRg ()
- 3.
- Input:
- 4.
- Output: Pr (private key), Pu (public key), sk (symmetric key), ID, PW
4.1.3. EnCDB (Pr, Pu, sk, )
- 5.
- Input: Pr, Pu, sk,
- 6.
- Output: 1st and 2nd Enc.
- ○
- 1st Encryption:
- ○
- 2nd Encryption:
4.2. Log-In by Authentication
MuAuth (vrfinf, )
- 7.
- Input: vrfinf (verifiable information),
- 8.
- Output: Verified or Fail
- The process for mutual authentication is as follows:
- ○
- EHRP sends its verifiable information:
- -
- , where is a randomly generated number for this session. The encryption key is HCP’s public key and the message is encrypted by RSA.
- ○
- HCP deceypts: Here, the decryption key is HCP’s private key and the above ciphertext is decrypted by RSA.
- ○
- HCP authenticates the subject of the received information using polynomials
- -
- If 1 (Successful)
- -
- (first, compute and then compute:
4.3. Key Sharing
ShKGen (1, , Pr, )
- 9.
- Input: 1, , ,
- 10.
- Output: ShKey =
- ○
- HCP generates the sharing key with EHRP:
- ○
- HCP sends EHRP the encryption of the shaing key:
- ○
- EHRP decrypts the received ciphertext with the random number : . The resulte is HCP’s public key and the sharing key .
- ○
- EHRP decrypts again for the result() with HCP’s public key: ) = .
- ○
- Then, EHRP checks whether the result is the same as , which was sent from EHRP to HCP for authentication.
4.4. Information Shring
4.4.1. ShRq (
- 11.
- Input:
- 12.
- Output: All attributes for 2nd Decryption
- ○
- EHRP requests the attributes of user i they wish to share from HCP:
- -
- . The attributes EHRP wants to share are encrypted with their sharing key and sent to HCP.
- ○
- HCP decrypts:
- -
- 1st Decryption with Sharing Key: . With the decryption key , the received ciphertext is decrypted. The result is the attributes which EHRP wants to share
- -
- 2nd Decryption (only for the requested attributes): . The only requested ciphertexts are decrypted with the HCP’s symmetric secret key sk
4.4.2. ReEnC (ShKey
- 13.
- Input: ShKey, all attributes
- 14.
- Output: ReE
- ○
- HCP re-encrypts the encrypted attributes of user i with sharing key:
- ○
- HCP sends EHRP the re-encrypted attributes including .
4.4.3. Dec (ShKey, Pu):
- 15.
- Input: , ReE
- 16.
- Output: Final 2nd Decryption
- ○
- 1st Decryption: EHRP decrypts the received encryption with their sharing key:
- Here, is the RSA encryption, which encrypts the with the Dr’s private key . is encrypted twice. The first is encrypted with RSA using the doctor’s private key as the encryption key for , and the second is encrypted with PRF f using sk_s as the encryption key, for the first encryption. is the RSA encrypted with the doctor’s public key for . is also encrypted twice. For , it is first RSA encrypted with and, second, encrypted with PRF f using sk_s. The result is the same as in Section 4.4.1.
- ○
- 2nd Decryption: EHRP decrypts the first decryption with doctor’s public key
4.5. The Whole Flow of Protocol Data
5. Security Analysis
5.1. Proof of Security
5.2. Discussion About Security
5.2.1. Confidentiality
5.2.2. Mutual Authentication
5.2.3. Intractability of Replay or Reflection
5.2.4. Self-Regulation for Privacy
5.2.5. Limited Access Control
5.2.6. Data Minimization
6. Efficiency Analysis
6.1. Time Complexity
- SysPrm: O(m + n)
- The generation of system parameters is a constant-time operation, denoted as O(1). In this, the classification of attributes in the database takes time proportional to the number of attributes (m), resulting in a time complexity of O(m). Generating the authentication polynomial takes time proportional to the number of registered EHRPs (n), leading to a time complexity of O(n). Therefore, the final time complexity for this algorithm becomes O(1 + m + n). We can simplify this to O(m + n). The dominant factors in determining the runtime are the number of attributes (m) and the number of registered EHRPs (n).
- KGenRg: O(1)
- This step involves generating various cryptographic keys (for EHRP, doctor, HCP). The number of keys is fixed and does not scale with the input data size. Therefore, the time taken is considered constant, represented by O(1).
- EnCDB: O(m)
- This stage encrypts the database. The encryption process iterates through each of the ‘m’ attributes in the database, performing encryption operations on each one. The time taken is directly proportional to the number of attributes; hence, the time complexity is O(m).
- MuAuth and ShKGen: O(1)
- Mutual authentication involves verifying identities and generating a sharing key. These operations are assumed to have a constant-time complexity, independent of the database size or the number of attributes. Thus, the time complexity is O(1).
- ShRq: O(1)
- The EHRP requests specific attributes. This involves a single encryption operation using the sharing key. Since it is a fixed number of operations, regardless of the database size, the time complexity is O(1).
- ReEnC: O(r)
- This step re-encrypts the selected attributes. The number of attributes being re-encrypted is represented by ’r’. The time taken is directly proportional to ’r’, giving us a time complexity of O(r).
- Dec: O(r)
- The final decryption step decrypts the re-encrypted attributes. Similar to re-encryption, the time complexity is directly proportional to the number of attributes being decrypted (‘r’), resulting in O(r).
6.2. Performance Analysis
6.2.1. Implementation and Experimental Setup
6.2.2. Performance Measurement of Key Algorithms
6.3. Data Minimization as a Key Efficiency Metric
- Intersection of Consented and Requested Attributes: The protocol cleverly ensures that only the intersection of the patient’s consented attributes and the EHRP’s requested attributes are shared, in other words, selective sharing. This minimizes data exposure, enhances security, and directly implements data minimization. Only absolutely necessary information is exchanged, reducing storage, processing, and transmission overheads.
- Reduced Storage and Processing Requirements: By only sharing the minimal necessary data, the system reduces storage requirements for both the HCP and the EHRP. Having fewer data also means less processing overhead for tasks like queries, analysis, and reporting.
- Improved Data Quality: Data minimization often leads to improved data quality as well. Focusing on essential data simplifies data management, reducing the chance of errors or inconsistencies. This indirectly improves efficiency by avoiding the need for extensive data cleaning or correction.
- Enhanced Compliance: Data minimization aligns with data protection regulations and reduces the risk of non-compliance. This indirect efficiency is vital; it avoids potential penalties, legal issues, and reputational damage that could significantly hamper the system’s operational efficiency.
- Streamlined Security Measures: Protecting fewer data inherently simplifies security measures. Fewer data points to secure make monitoring, auditing, and responding to potential security threats more manageable and efficient.
7. Analysis Comparing DtMin to Existing Systems
7.1. Comparative Analysis Framework
- Security and Privacy: How well does the system protect sensitive medical data?
- Data Minimization: Does the system adhere to the principle of collecting, processing, and storing only the minimum necessary data?
- Efficiency: What are the computational and operational efficiencies of the system?
- Scalability: How does the system perform with increasing data volumes and user numbers?
- Interoperability: Can the system integrate with other healthcare systems?
- User Control: To what extent does the system empower users with control over their data?
7.2. Comparison with Existing Systems
7.2.1. Security and Privacy
- DtMin:
- -
- Utilizes a multi-layered encryption approach, leveraging attribute-based encryption (ABE) and a hybrid encryption technique that incorporates decisional Diffie–Hellman (DDH) assumption, pseudorandom generators (PRGs), and pseudorandom functions (PRFs).
- -
- Formal security analysis under ICR-DB and ICR-IS security games, proving security based on the hardness of established cryptographic assumptions.
- -
- Provides granular control over data access based on attribute sensitivity levels and user consent, minimizing data exposure.
- Existing Systems:
- -
- EHRs, HIEs, and Clinical Trial Management Systems often rely on simpler access control mechanisms, which might not offer the same level of granular control or formal security analysis.
- -
- Some systems use blockchain technology for security, but they might not prioritize data minimization or provide the same level of user control over data sharing.
7.2.2. Data Minimization
- DtMin:
- -
- Explicitly designed to minimize the amount of data shared, ensuring only the necessary information is released based on user consent and data sensitivity.
- -
- Implements selective sharing, where only the intersection of consented and requested attributes is shared, reducing data exposure and enhancing security.
- Existing Systems:
- -
- Many systems do not prioritize data minimization, leading to the collection and storage of more data than necessary, increasing the risk of data breaches and non-compliance with privacy regulations.
7.2.3. Efficiency
- DtMin:
- -
- Performance analysis demonstrates efficiency across various data volumes and patient numbers, with a time complexity of O(m + n + r), where m is the number of attributes, n is the number of registered EHRPs, and r is the number of attributes being shared.
- -
- Reduces storage and processing requirements by minimizing data sharing, leading to improved data quality and streamlined security measures.
- Existing Systems:
- -
- Systems like EHRs and HIEs might face scalability issues due to the volume of data they handle, potentially leading to higher computational costs and slower performance.
7.2.4. Scalability
- DtMin:
- -
- While the multi-layered encryption and ABE mechanisms might present scalability challenges, the strategies like distributed computing, efficient data sharding, and optimized database design can mitigate these issues.
- Existing Systems:
- -
- Scalability is often a concern, especially with large datasets and numerous users. Systems like blockchain-based HIEs might struggle with scalability due to the inherent limitations of blockchain technology.
7.2.5. Interoperability
- DtMin:
- -
- Designed with interoperability in mind, DtMin can integrate with existing healthcare systems through standardized data formats and protocols.
- Existing Systems:
- -
- Interoperability remains a significant challenge due to the lack of standardization in data formats and communication protocols across different healthcare systems.
7.2.6. User Control
- DtMin:
- -
- Empowers users with control over their data through a tiered approach to data handling, allowing patients to decide which information to share publicly.
- Existing Systems:
- -
- User control is often limited, with systems primarily managed by healthcare providers or third parties, reducing patient autonomy over their data.
7.3. Strengths and Weaknesses
7.3.1. Strenghths
7.3.2. Weaknesses
8. Future Enhancements: Integration with Advanced Cryptographic Techniques for Data Sizes of over 100,000 in Real Environments
8.1. Integration with Advanced Cryptographic Techniques
8.1.1. Applying Lattice-Based ABE
- RLWE (Ring Learning With Errors)-based KP-ABE: RLWE-based KP-ABE is more efficient than LWE-based variants. It has a complexity that depends only on the depth of the policy circuit, rather than its size [34].
- GPU acceleration: According to implementation research [34], encryption operations can be accelerated using Graphics Processing Units (GPUs). This demonstrates that public key and ciphertext evaluation tasks can be performed within a reasonably short time.
- Use of Small Secret Keys: Lattice-based ABE has the advantage that the secret key is much smaller than those in similar constructions, which are proportional to the size of the policy circuit [34].
8.1.2. Adoption of Lightweight ABE Variants
- Utilization of Optimized Data Structures: As proposed in the ABE Squared benchmarking framework, ABE implementations can be optimized using efficient data structures [35].
- ABE Library for Android Devices: As mentioned in [36], the ABE library for the Android operating system, AndrABEn, can be implemented with satisfactory performance using ABE on Android smartphones and similar devices.
- Minimization of Input Data Size: Medical data, such as ECG (electrocardiogram) signals, can be significantly reduced in size using DTW (Dynamic Time Warping) compression, which can help lower encryption costs [36].
8.2. Analysis of Integration Strategies with Existing Medical Information Systems
8.2.1. Analysis of the Current Medical Information Standards Environment
- -
- HL7 FHIR (Fast Healthcare Interoperability Resources): A framework for standardized representation and exchange of healthcare data. FHIR focuses on increasing the interoperability of healthcare information by facilitating data sharing between various healthcare systems [37].
- -
- HL7 v2.x: A set of standards for exchanging health information electronically. It is widely used in healthcare for messaging between different systems, such as hospitals, laboratories, and pharmacies. HL7 v2.x supports various types of messages, including patient demographics, orders, results, and billing information [38].
- -
- DICOM (Digital Imaging and Communications in Medicine): A standard for handling, storing, printing, and transmitting medical imaging information. It includes a file format definition and a network communications protocol, ensuring interoperability among different medical imaging devices and systems [39].
- -
- IHE (Integrating the Healthcare Enterprise): A framework that integrates various healthcare systems to ensure interoperability. It provides a set of standards and guidelines to facilitate the sharing of patient information across different healthcare systems [40].
8.2.2. Adaptation Strategy to Integrate DtMin into Current Healthcare Information Systems
- FHIR Resource Mapping: Map DtMin’s attribute-based classification to FHIR resources and extensions.
- API Gateway: Mediate requests between DtMin and EHR systems while handling authentication and authorization.
- Transformation Service: Handle data transformation between the DtMin protocol and standard healthcare data formats.
8.2.3. Case-by-Case Integration Patterns
- ESB (Enterprise Service Bus) Integration: Utilize existing ESB to integrate DtMin services into the organization’s service mesh.
- API Management Platform: Manage DtMin APIs via existing API gateways.
- Phased Implementation: Gradually expand, starting from specific departments or data types.
- Cloud-Based Integration: Minimize integration complexity with DtMin services offered as a SaaS model.
- Standard Connectors: Provide pre-built connectors for common EHR systems.
- Simplified Configuration: Interfaces configurable with minimal technical knowledge
- IHE Profile Compliance: Extend IHE XDS (Cross-Enterprise Document Sharing) profiles to integrate DtMin capabilities.
- Common Data Model: Map HIE’s common data model with DtMin’s attribute classification.
- Interoperability Gateway: Integrate DtMin capabilities into HIE gateways to apply data minimization principles to all exchanged data.
8.3. Integrated Strategy Analysis for Large-Scale Environments Processing More than 100,000 Big Data
8.3.1. Data Partitioning and Parallel Processing
8.3.2. Improved Authentication Polynomial
8.3.3. Multi-Level Architecture
8.3.4. Incremental Updates
9. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.; Kim, S.; Lee, I. A Study on Diffie Hellman-Private Set Intersection Protocol for Sharing of Medical Data. In Proceedings of the Korea Multimedia Society Spring Conference, Seoul, Republic of Korea, 16–18 May 2024; p. 27. [Google Scholar]
- Zhou, X.; Liu, J.; Wu, Q.; Zhang, Z. Privacy Preservation for Outsourced Medical Data with Flexible Access Control. IEEE Access 2018, 6, 14827–14841. [Google Scholar] [CrossRef]
- Miyaji, A.; Nakasho, K.; Nishida, S. Privacy-Preserving Integration of Medical Data. Trans. Process. Syst. 2017, 41, 37. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-A. Secure Information Sharing System for Online Patient Networks. J. Secur. Commun. Netw. 2019, 2019, 7541269. [Google Scholar] [CrossRef]
- Pan, H.; Zhang, Y.; Si, X.; Yao, Z.; Zhao, L. MDS2-C3PF: A Medical Data Sharing Scheme with Cloud-Chain Cooperation and Policy Fusion in IoT. Symmetry 2022, 14, 2479. [Google Scholar] [CrossRef]
- Elvas, L.B.; Ferreira, J.C.; Dias, M.S.; Rosário, L.B. Health Data Sharing towards Knowledge Creation. Systems 2023, 11, 435. [Google Scholar] [CrossRef]
- Hu, M.; Ren, Y.; Chen, C. Privacy-Preserving Medical Data-Sharing System with Symmetric Encryption Based on Blockchain. Symmetry 2023, 15, 1010. [Google Scholar] [CrossRef]
- Walid, R.; Joshi, K.P.; Choi, S.G. Comparison of attribute-based encryption schemes in securing healthcare systems. Sci. Rep. 2024, 14, 7147. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Son, S.; Kwon, D.; Kim, M.; Park, Y.; Park, Y. Design of Secure and Privacy-Preserving Data Sharing Scheme Based on Key Aggregation and Private Set Intersection in Medical Information System. Mathematics 2024, 12, 1717. [Google Scholar] [CrossRef]
- Mao, X.; Li, C.; Zhang, Y.; Zhang, G.; Xing, C. Efficient and Secure Management of Medical Data Sharing Based on Blockchain Technology. Appl. Sci. 2024, 14, 6816. [Google Scholar] [CrossRef]
- Official EU GDPR. Article 5—Principles Relating to Processing of Personal Data. Available online: https://gdpr.eu/ (accessed on 12 February 2025).
- U.S. Department of Health & Human Services HIPAA Page. Available online: https://www.hhs.gov/programs/hipaa/index.html (accessed on 12 February 2025).
- Park, H. Security and privacy model of electronic medical record systems. Int. J. Healthc. Technol. Manag. 2022, 19, 303–323. [Google Scholar]
- Xu, Z.; Zheng, E.; Han, H.; Dong, X.; Dang, X.; Wang, Z. A secure healthcare data sharing scheme based on two-dimensional chaotic mapping and blockchain. Sci. Rep. 2024, 14, 23470. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Zheng, J.; Wu, W.; Gao, D.; Gu, X. Research on healthcare data sharing in the context of digital platforms considering the risks of data breaches. Front. Public Health 2024, 12, 1438579. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Park, J.; Woo, H.; Yun, H.; Lee, M.; Hong, D. Safe Utilization and Sharing of Genomic Data: Amendment to the Health and Medical Data Utilization Guidelines of South Korea. Cancer Res. Treat. 2024, 7, 1027–1039. [Google Scholar]
- Barker, W.; Chang, W.; Everson, J.; Gabriel, M.; Patel, V.; Richwine, C.; Strawley, C. The Evolution of Health Information Technology for Enhanced Patient-Centric Care in the United States: Data-Driven Descriptive Study. J. Med. Internet Res. 2024, 26, e59791. [Google Scholar] [PubMed]
- Personal Information Protection Act, Amendment in 2022; Legislature of Republic of Korea: Seoul, Republic of Korea, 2022.
- Mukta, R.; Paik, H.; Lu, Q.; Kanhere, S. A survey of data minimisation techniques in blockchain-based healthcare. Comput. Netw. 2022, 205, 108766. [Google Scholar] [CrossRef]
- Conte, R.; Sansone, F.; Tonacci, A.; Pala, A. Privacy-by-Design and Minimization within a Small Electronic Health Record: The Health360 Case Study. Appl. Sci. 2022, 12, 8441. [Google Scholar] [CrossRef]
- Bargh, M.; Meijer, R.; Braak, S.; Latenko, A.; Vink, M.; Sunil, C. Embedding Personal Data Minimization Technologies in Organizations: Needs, Vision and Artifacts. In Proceedings of the 14th International Conference on Theory and Practice of Electronic Governance, Athens, Greece, 6–8 October 2021. [Google Scholar]
- Senarath, A.; Arachchilage, N. A Data Minimization Model for Embedding Privacy into Software Systems. Comput. Secur. 2019, 87, 101605. [Google Scholar]
- Menezes, A.J.; Oorschot, P.C.; Vanstone, S.A. Handbook of Applied Cryptography, 1st ed.; CRC Press: Boca Raton, FL, USA, 1996. [Google Scholar]
- Song, D.X.; Wagner, D.; Perrig, A. Practical techniques for searches on encrypted data. In Proceedings of the IEEE Symposium on Security and Privacy, Berkeley, CA, USA, 14–17 May 2000; pp. 44–55. [Google Scholar]
- Schneier, B. Applied Cryptography, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1996. [Google Scholar]
- Goldreich, O. Foundations of Cryptography, Volume 1, Basic Tools; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- Katz, J.; Lindell, Y. Introduction to Modern Cryptography; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Bellare, M.; Rogaway, P. The Security of Triple Encryption and a Framework for Code-Based Game-Playing Proofs. In Proceedings of the 2005 International Conference on the Theory and Application of Cryptographic Techniques, Aarhus, Denmark, 22–26 May 2005. [Google Scholar]
- Stallings, W.; Brown, L. Computer Security: Principles and Practice, 4th ed.; Pearson: London, UK, 2018. [Google Scholar]
- Stallings, W. Cryptography and Network Security: Principles and Practice, 7th ed.; Pearson: London, UK, 2016. [Google Scholar]
- Stallings, W. Network Security Essentials: Applications and Standards, 6th ed.; Pearson: London, UK, 2016. [Google Scholar]
- IBM Security Website. Cost of a Data Breach Report 2022. Available online: https://www.ibm.com/security/data-breach (accessed on 12 February 2025).
- Accenture’s Healthcare Industry Insights Page. Health/Digital-Health-Technology-Vision-2022. Available online: https://www.accenture.com/us-en/insights (accessed on 12 February 2025).
- Dai, W.; Doroz, Y.; Polyakov, Y.; Rohloff, K.; Sajjadpour, H.; Savas, E.; Sunar, B. Implementation and Evaluation of a Lattice-Based Key-Policy ABE Scheme. IEEE Trans. Inf. Forensics Secur. 2018, 13, 1169–1184. [Google Scholar]
- Piedra1, A.; Venema, M.; Alpár, G. ABE Squared: Accurately Benchmarking Efficiency of Attribute-Based Encryption. IACR Trans. Cryptogr. Hardw. Embed. Syst. 2022, 2022, 192–239. [Google Scholar]
- Krinah, A.; Challal, Y.; Omar, M.; Nouali, O. Using ABE for Medical Data Protection in Fog Computing. In Proceedings of the 21st International Conference on Enterprise Information Systems, Heraklion, Greece, 3–5 May 2019; pp. 155–161. [Google Scholar]
- HL7 FHIR Documentation. Exchanging Resources. Available online: https://www.hl7.org/fhir/documentation.html (accessed on 12 February 2025).
- HL7 Official Website. HL7 v2.x. Available online: https://www.hl7.org/ (accessed on 12 February 2025).
- DICOM Official Website. Standard, DICOM Part 7: Message Exchange. Available online: https://www.dicomstandard.org/ (accessed on 12 February 2025).
- IHE Official Website. IHE Technical Framework Documents for Public Comment. Available online: https://www.ihe.net/ (accessed on 12 February 2025).
- Kim, S.; Chung, M.; Lee, T.; Won, J. Implementation of Medical Data-Based Big Data Analytics Service. In Proceedings of the Korean Institute of Information Scientists and Engineers 2015, Busan, Republic of Korea, 20–22 September 2015; pp. 157–159. [Google Scholar]
- What-Is-Distributed-Data-Processing. Available online: https://www.purestorage.com/kr/knowledge (accessed on 12 February 2025).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HCP | EHRP |
|---|---|
| 4.1. System Setting and Registration 4.1.1. SysPrm 4.1.2. KGenRg 4.1.3. EnCDB | |
4.2. Log-In by Authentication: MuAuth
| |
| 4.3. Key Sharing: ShKGen | |
| 4.4. Information Shring 4.4.1. ShRq | |
| 4.4.2. ReEnC | |
| 4.4.3. Dec | |
| Hardware | CPU | 11th Gen Intel(R) Core™ i5-1155G7 @ 2.50 GHz |
| Memory | 16 G | |
| Disk | 1 TB | |
| System type | 64-bit operating system, ×64-based processor | |
| OS | Windows 11 Home | |
| Language | Python 3.13 | |
| Cryptographic Parameters and Libraries | |
|---|---|
| Pseudorandom Function f | AES 128 bits |
| Asymmetric Encryption Function | RSA 4096 bits |
| Pseudorandom Generator | AES-CTR 256 bits |
| Group parameter | cyclic group |
| Modulus p | 2048 bits |
| Order q | 256 bits |
| Generator g | 2048 bits |
| Crypto library | PyCryptodome, cryptography |
| Python library | Numpy, Sympy, os, string, random |
| Time measurement function | timeit.default_timer() |
| Total Number of Polynomial Terms | Running Time (Second) |
|---|---|
| 250 | 0.138386 |
| 500 | 0.504379 |
| 1000 | 2.051452 |
| 1500 | 4.488000 |
| 2000 | 8.305066 |
| Attribute Size | Running Time (Second) |
|---|---|
| 1 KB | 0.001666 |
| 10 KB | 0.003509 |
| 100 KB | 0.023096 |
| 1 MB | 0.224033 |
| 10 MB | 3.598605 |
| 100 MB | 44.010283 |
| ReEnC | Dec | |
|---|---|---|
| 1 KB | 0.000963 | 0.000464 |
| 10 KB | 0.000936 | 0.000932 |
| 100 KB | 0.006014 | 0.004883 |
| 1 MB | 0.093270 | 0.072731 |
| 10 MB | 0.775543 | 0.965413 |
| Criteria | DtMin Protocol | Existing Systems |
|---|---|---|
| Security and Privacy | Multi-layered encryption, formal security analysis under ICR-DB and ICR-IS | Simpler access control mechanisms, less rigorous security analysis |
| Data Minimization | Explicitly designed to minimize data shared based on user consent and sensitivity | Do not prioritize data minimization, often collect and store excess data |
| Efficiency | Efficient with O(m + n + r) complexity, reduces storage and processing requirements | Potential scalability issues with large datasets, higher computational costs |
| Scalability | Scalability challenges mitigated through distributed computing and data sharding | Limited scalability due to inherent system constraints |
| Interoperability | Designed for interoperability with standardized data formats and protocols | Interoperability challenges due to lack of standardization |
| User Control | Empowers users with granular control over data sharing | Limited user control, primarily managed by providers or third parties |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-A. The DtMin Protocol: Implementing Data Minimization Principles in Medical Information Sharing. Electronics 2025, 14, 1501. https://doi.org/10.3390/electronics14081501
Park H-A. The DtMin Protocol: Implementing Data Minimization Principles in Medical Information Sharing. Electronics. 2025; 14(8):1501. https://doi.org/10.3390/electronics14081501
Chicago/Turabian StylePark, Hyun-A. 2025. "The DtMin Protocol: Implementing Data Minimization Principles in Medical Information Sharing" Electronics 14, no. 8: 1501. https://doi.org/10.3390/electronics14081501
APA StylePark, H.-A. (2025). The DtMin Protocol: Implementing Data Minimization Principles in Medical Information Sharing. Electronics, 14(8), 1501. https://doi.org/10.3390/electronics14081501