


A Novel 6-DOF Multi-Technique Abdominal Massage Robot System: A New Solution for Relieving Constipation and an Exploration of Standardization

Abstract
1. Introduction
2. Materials and Methods
2.1. Design Objectives of the Abdominal Massage Robot
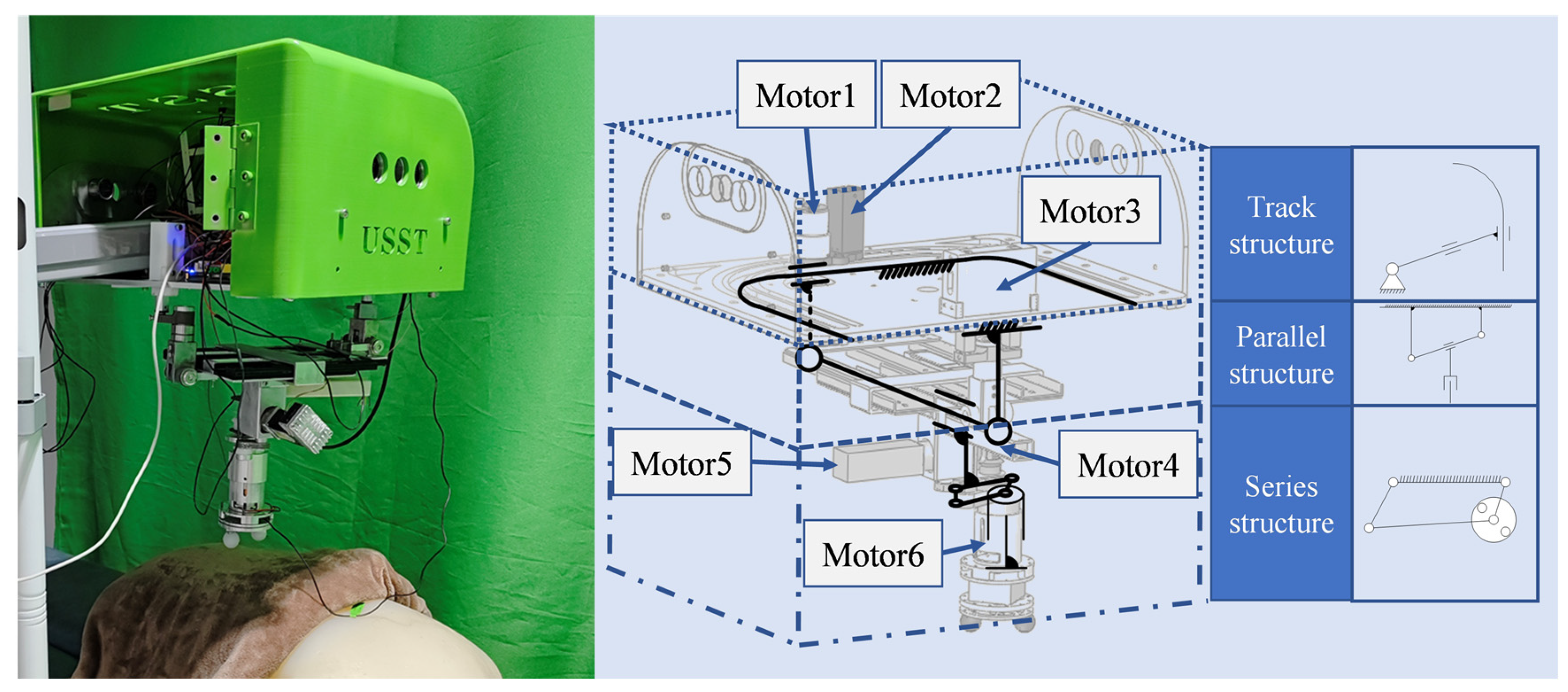
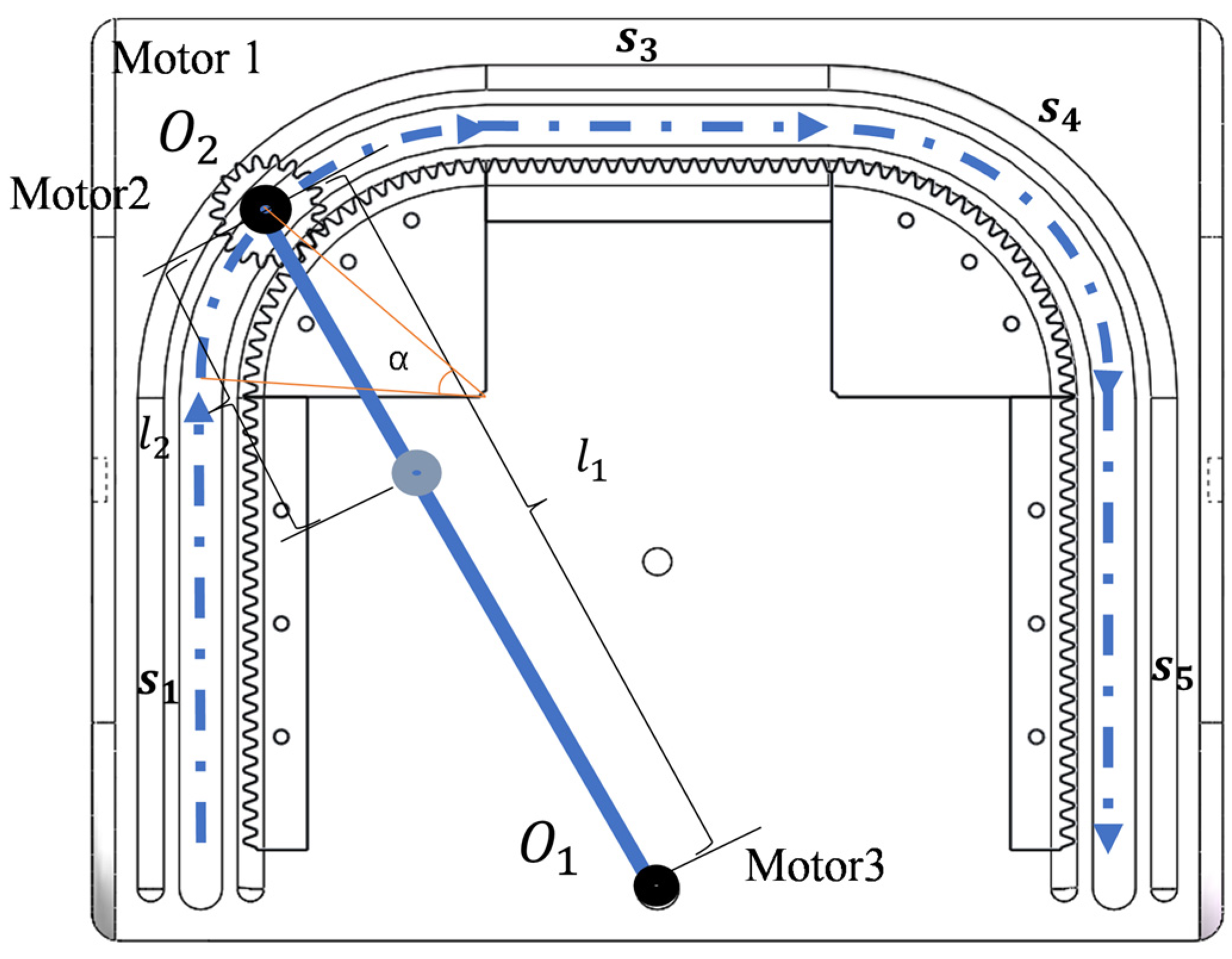
2.2. Mechanism Design
2.3. Kinematic Analysis of the End-Effector
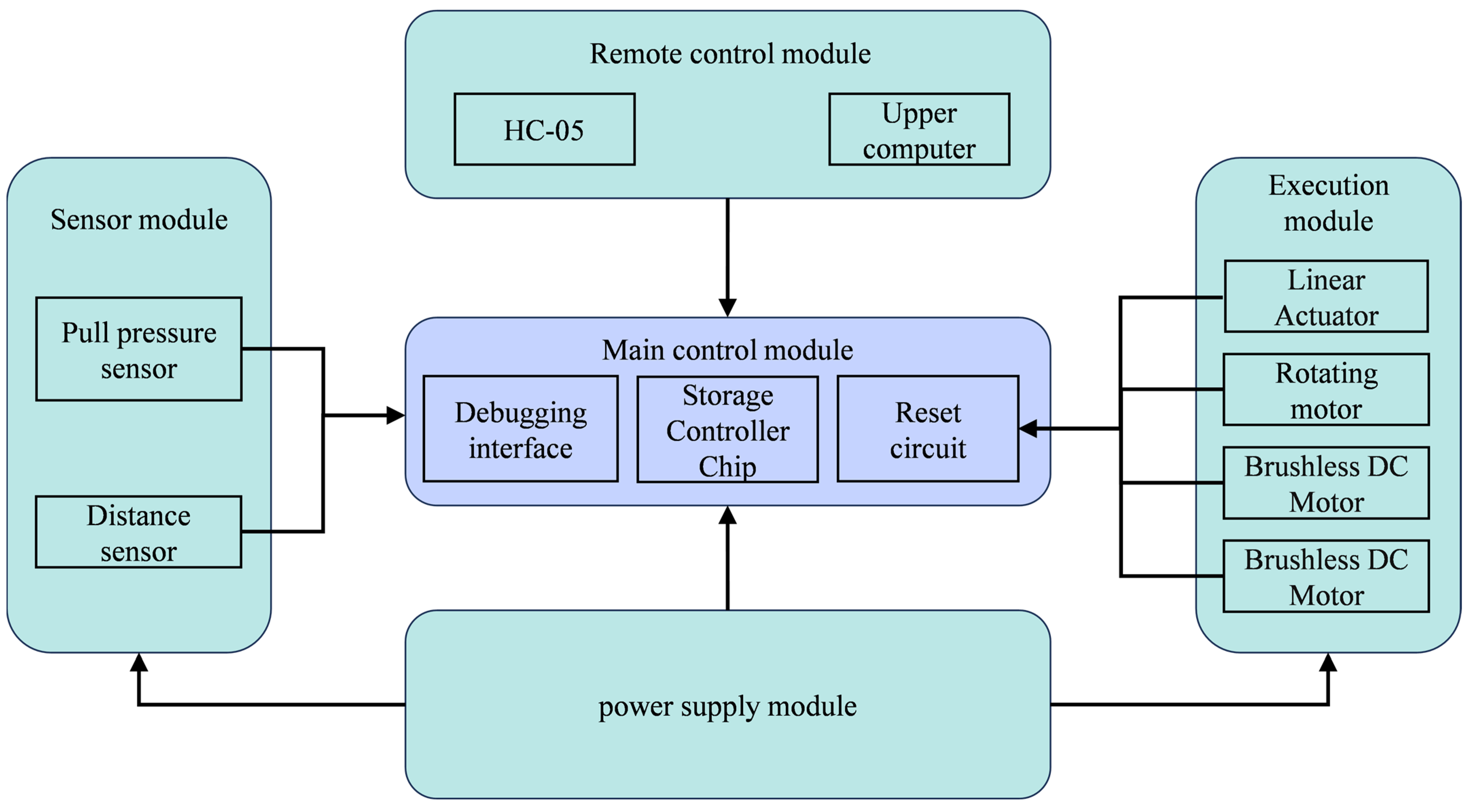
2.4. Hardware Control System of the Abdominal Massage Robot
2.5. Software Control System of the Abdominal Massage Robot
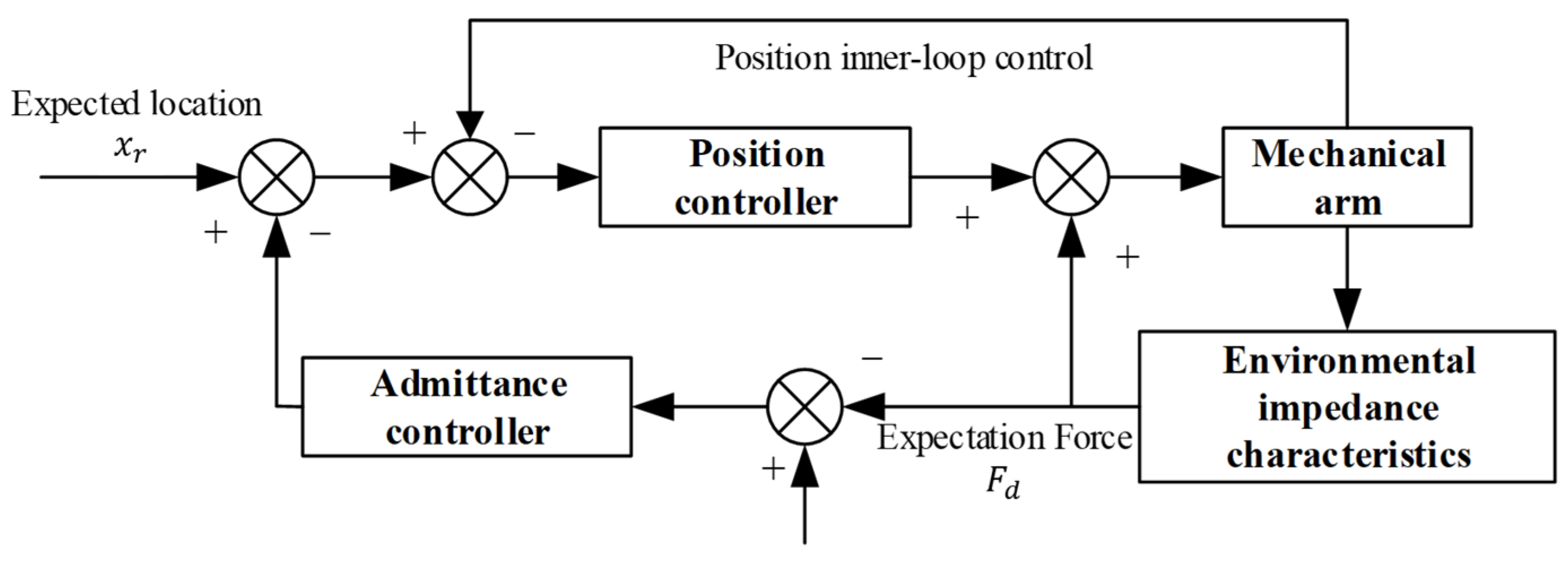
2.5.1. Admittance Control
2.5.2. Adaptive Fuzzy Variable Admittance Control
- If the force error E is positive and the force-error change rate EC is also positive, the error increases in the positive direction. Applying too much force may exceed the patient’s tolerance range. Currently, the controller should output the reverse maximum voltage NB for control.
- If both the force error E and the force-error change rate EC are negative, the error increases in the opposite direction. In this case, the controller should output the positive maximum voltage PB for control.
- If the force error E is positive while the force-error change rate EC is negative, the error decreases in the opposite direction. The controller can only output the standard PM control.
- If the force error E is zero and the force-error change rate EC is also 0, the error decreases in the opposite direction. The controller outputs a voltage of ZO.
2.6. Safety Strategies for the Abdominal Massage Robots
2.6.1. Hardware Safety Strategies
2.6.2. Software Safety Strategies
3. Results
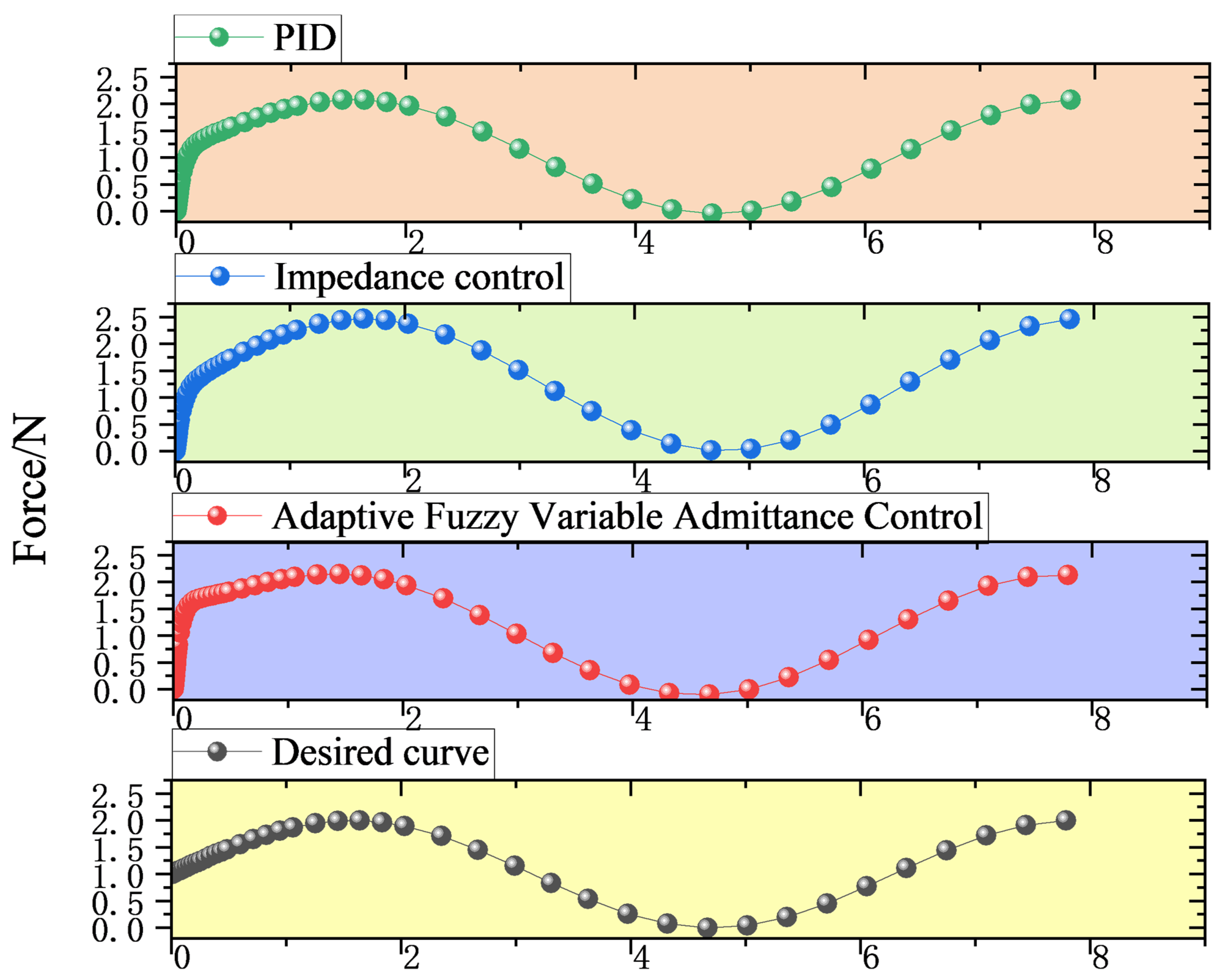
3.1. Simulation Verification
3.2. Experiments and Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sinclair, M. The Use of Abdominal Massage to Treat Chronic Constipation. J. Bodyw. Mov. Ther. 2011, 15, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Gallegos-Orozco, J.F.; Foxx-Orenstein, A.E.; Sterler, S.M.; Stoa, J.M. Chronic Constipation in the Elderly. Am. J. Gastroenterol. 2012, 107, 18–25. [Google Scholar] [CrossRef]
- Sharma, A.; Rao, S. Constipation: Pathophysiology and Current Therapeutic Approaches. In Handbook of Experimental Pharmacology; Springer: Cham, Switzerland, 2017; Volume 239, pp. 59–74. [Google Scholar]
- Goldenberg, M.; Kalichman, L. The Underlying Mechanism, Efficiency, and Safety of Manual Therapy for Functional Gastro-intestinal Disorders: A Narrative Review. J. Bodyw. Mov. Ther. 2024, 38, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vigano, A.; Bruera, E. Pain Management in Functional Gastrointestinal Disorders. Can. J. Gastroenterol. Hepatol. 1995, 9, 802590. [Google Scholar] [CrossRef]
- Dehghan, M.; Malakoutikhah, A.; Ghaedi Heidari, F.; Zakeri, M.A. The Effect of Abdominal Massage on Gastrointestinal Functions: A Systematic Review. Complement. Ther. Med. 2020, 54, 102553. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Z.; Sun, J.; Li, X.; Chu, Y.; Zhao, D.; Ju, H.; Wu, X.; Cong, D. Abdominal Massage: A Review of Clinical and Experimental Studies from 1990 to 2021. Complement. Ther. Med. 2022, 70, 102861. [Google Scholar] [CrossRef]
- Chen, Q.; Zhou, Z.; Liao, Y. Clinical Observation on the Treatment of Constipation after Thoracolumbar Fracture with Acupoint Massage Combined with Application. Chin. Med. Mod. Distance Educ. China 2025, 23, 111–113. [Google Scholar]
- Xiao, S.S.; Huang, L.S.; Wang, L.; Xu, Y. Application of Abdominal Acupoint Massage Combined with Chewing Gum in Preventing Constipation in Patients after Posterior Lumbar Interbody Fusion. J. Qilu Nurs. 2024, 30, 121–123. [Google Scholar]
- Wang, T.T.; Fang, Q. Effects of Abdominal Acupoint Massage Combined with Moxibustion Therapy on Defecation and Quality of Life in Parkinson’s Constipation Patients. Clin. Res. Pract. 2024, 9, 175–178. [Google Scholar] [CrossRef]
- Smith, G.D. Abdominal Massage for Constipation: Techniques, Evidence Base and Safety. Gastrointest. Nurs. 2013, 11, 13–14. [Google Scholar] [CrossRef]
- Mimidis, K.; Galinsky, D.; Rimon, E.; Papadopoulos, V.; Zicherman, Y.; Oreopoulos, D. Use of a Device That Applies External Kneading-like Force on the Abdomen for Treatment of Constipation. World J. Gastroenterol. 2005, 11, 2027–2031. [Google Scholar] [CrossRef] [PubMed]
- Mowoot II. Available online: https://www.mowoot.com/en/product/mowoot-2/#moreinfo (accessed on 9 February 2025).
- Mcclurg, D.; Booth, L.; Herrero-Fresneda, I. Safety and Efficacy of Intermittent Colonic Exoperistalsis Device to Treat Chronic Constipation: A Prospective Multicentric Clinical Trial. Clin. Transl. Gastroenterol. 2020, 11, e00267. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Wang, M.; Li, N. Intestinal Management Training Massager. Patent CN205515489U, 31 August 2016. [Google Scholar]
- Li, H.Y.; Zhao, H.; Gong, Z.K. Application of a New Intestinal Massager in Stroke Patients with Constipation. Chin. Nurs. Res. 2018, 32, 636–638. [Google Scholar]
- Kim, T.Y.; Moon, S.I. Device for Treating Constipation Using Heat and Air Cells. Patent KR200452102 Y1, 27 November 2018. [Google Scholar]
- Choi, Y.I.; Kim, K.O.; Chung, J.W.; Kwon, K.A.; Kim, Y.J.; Kim, J.H.; Park, D.K. Effects of Automatic Abdominal Massage Device in Treatment of Chronic Constipation Patients: A Prospective Study. Dig. Dis. Sci. 2020, 66, 3105–3112. [Google Scholar] [CrossRef]
- Ning, P.F. A Nursing Massage Robot for Promoting Digestion. Patent CN109498397A, 22 March 2019. [Google Scholar]
- Zhu, H.L. A New Type of Abdominal Massage Device. Patent CN202020731814, 7 May 2020. [Google Scholar]
- Gou, Y.Q.; Yang, L.X. An Abdominal Massage Device for Gastroenterology. Patent CN211750916U, 27 October 2020. [Google Scholar]
- Jones, K.C.; Du, W. Development of a massage robot for medical therapy. In Proceedings of the 2003 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Honolulu, HI, USA, 2–5 June 2003. [Google Scholar]
- Aitreat-About Emma. Available online: https://www.aitreat.com/about-emma (accessed on 6 March 2025).
- Kuka-Solutions Database. Available online: https://www.kuka.cn/zh-cn (accessed on 6 March 2025).
- Hou, P.; Han, L. Development of a Home-use Back-rubbing and Massage Robot. Mach. Des. Res. 2009, 25, 101–105. [Google Scholar] [CrossRef]
- Jiao, C.B. Structural Analysis and Optimization of the LLR-1 Traditional Chinese Medicine Massage and Physiotherapy Robot. Master’s Thesis, Shandong Jianzhu University, Jinan, China, 2012. [Google Scholar]
- Lu, S.; Gao, H.; Liu, C.; Wang, T. Design of Chinese medical massage robot system. In Proceedings of the 2011 International Conference on Electrical and Control Engineering, Yichang, China, 16–18 September 2011. [Google Scholar]
- Gao, H.B.; Lu, S.Y.; Wang, T.; Liu, C.G.; Kang, B.Y.; Ji, Y.; Bi, H.Y. Research and Development of a Traditional Chinese Medicine Massage Robot. Robot 2011, 33, 553–562. [Google Scholar]
- Xie, J.; Zhang, J.; Ma, L.Z.; Yang, Q.Z.; Yin, X.Q. Mechanism Design and Motion Simulation of a Traditional Chinese Medicine Tuina Manipulator. J. Eng. Des. 2011, 18, 344–348. [Google Scholar]
- Lu, S.Y.; Li, C. Research Progress on Key Technologies of Traditional Chinese Medicine Massage Robots. J. Shandong Jianzhu Univ. 2017, 32, 60–68. [Google Scholar]
- Wang, Y.R. System Analysis and Prospect of Traditional Chinese Medicine Massage Robots. Inf. Technol. Informatiz. 2012, 76–79. [Google Scholar]
- Tao, W.; Liu, Z.; Li, Y. Research and realization of the Chinese massage robot based on three-dimensional model. In Proceedings of the 2010 8th World Congress on Intelligent Control and Automation, Jinan, China, 27–29 June 2010. [Google Scholar]
- Su, Y.L. Design and Research of a Tuina Robot Based on a Decoupled Parallel Mechanism. Ph.D. Thesis, Yanshan University, Qinhuangdao, China, 2015. [Google Scholar]
- Kong, Y.X. Design and Research of a Hybrid-connected Robot Based on Traditional Chinese Medicine Tuina Manipulation. Ph.D. Thesis, North University of China, Taiyuan, China, 2021. [Google Scholar] [CrossRef]
- Aubo-Robotic. Available online: https://www.aubo-robotics.cn/cases_m (accessed on 6 March 2025).
- Universal Robots. Available online: http://www.universal-robots.com/ (accessed on 6 March 2025).
- Grebenstein, M.; Albu-Schaffer, A.; Bahls, T.; Chalon, M.; Eiberger, O.; Friedl, W.; Gruber, R.; Haddadin, S.; Hagn, U.; Haslinger, R.; et al. The DLR hand arm system. In Proceedings of the 2011 IEEE International Conference on Robotics and Automation, Shanghai, China, 9–13 May 2011. [Google Scholar]
- Huang, Z.; Yu, C.; Yu, Z.; Long, R.; Li, Y.; Li, Y. Soft Four-Leaf Clover Physiotherapy Robot for Traditional Chinese Medicine Massage Physiotherapy. In Proceedings of the 2023 China Automation Congress (CAC), Chongqing, China, 24–26 November 2023; pp. 1977–1982. [Google Scholar]
- Zhang, B.C.; Han, Y.Y.; Wang, Z.L.; Pang, Z.X.; Zhang, Y.L. Design of the Arm Control System of a Humanoid Massage Robot Based on PMAC. Mach. Des. Manuf. 2012, 4, 56–58. [Google Scholar]
- Si, W.; Srivastava, G.; Zhang, Y.; Jiang, L. Green Internet of Things Application of a Medical Massage Robot With System Interruption. IEEE Access 2019, 7, 127066–127077. [Google Scholar] [CrossRef]
- Dong, H.; Feng, Y.; Qiu, C.; Chen, I.-M. Construction of interaction parallel manipulator: Towards rehabilitation massage. IEEE/ASME Trans. Mechatron. 2022, 28, 372–384. [Google Scholar] [CrossRef]
- Khoramshahi, M.; Henriks, G.; Naef, A.; Salehian, S.S.M.; Kim, J.; Billard, A. Arm-hand motion-force coordination for physical interactions with non-flat surfaces using dynamical systems: Toward compliant robotic massage. In Proceedings of the 2020 IEEE International Conference on Robotics and Automation (ICRA), Paris, France, 31 May–31 August 2020. [Google Scholar] [CrossRef]
- Luo, R.C.; Hsieh, K.C. Tapping motion detection incorporate with impedance control of robotics tapotement massage on human tissue. In Proceedings of the 2018 IEEE 15th Int Workshop Advanced Motion Control (AMC), Nagoya, Japan, 10–12 April 2018; pp. 160–165. [Google Scholar]
- Meng, X.; Tie, Z.; Wen, X.W. Study on force control for robot massage with a model-based reinforcement learning algorithm. Intell. Serv. Robot. 2023, 16, 509–519. [Google Scholar]
- Zhang, X.; Xiong, G.; Yin, P.; Gao, Y.; Feng, Y. Autonomous path planning and stabilizing force interaction control for robotic massage in unknown environment. Ind. Robot 2024, 51, 518–527. [Google Scholar] [CrossRef]
- GB/T 12346-2021; Nomenclature and Location of Meridian Points. China Standards Press: Beijing, China, 2021.
- GB/T 23237-2009; Methods of Anthropometry for Locating Acupuncture Points. China Standards Press: Beijing, China, 2009.
- Mouri, K.; Terashima, K.; Minyong, P.; Kitagawa, H.; Miyoshi, T. Identification and hybrid impedance control of human skin muscle by multi-fingered robot hand. In Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, Nice, France, 22–26 September 2008. [Google Scholar]
- Wang, W.; Wang, S.Y.; Zhang, T.Q.; Yang, J.Y. Control Method of a Wheeled Walking-aid Robot Based on the DDPG Algorithm of Reinforcement Learning. Robot. Technol. Appl. 2023, 39–43. [Google Scholar]
- Shi, S.K.; Diao, Y.; Yang, J.B.; Yang, S.Y.; You, D.H.; Wang, F. Research on the Impedance Control of a Non-metallic Curved Surface Local Grinding and Polishing Repair Robot. Modul. Mach. Tool Autom. Manuf. Technol. 2023, 8, 57–61. [Google Scholar] [CrossRef]
- Zhai, J.; Zeng, X.; Su, Z. An intelligent control system for robot massaging with uncertain skin characteristics. Ind. Robot 2022, 49, 634–644. [Google Scholar] [CrossRef]
- Tan, J.Y.; Wei, S.B.; Rong, Y.S.; Zhang, Z.L. Research on the Contact Force Tracking of a Robot Based on Variable-damping Impedance Control. Modul. Mach. Tool Autom. Manuf. Technol. 2021, 5, 69–71, 76. [Google Scholar] [CrossRef]
- Zhai, J.; Li, R.; Su, Z. Friction and Deformation Behavior of Human Skin During Robotic Sliding Massage Operation. J. Bionic Eng. 2024, 21, 1892–1904. [Google Scholar] [CrossRef]
- Filipe, J.; Terashima, K.; Kitagawa, H.; Miyoshi, T.; Minyong, P.; Kondo, T. Modeling and massage control of human skin muscle by using multi-fingered robot hand. Integr. Comput.-Aided Eng. 2006, 13, 233–248. [Google Scholar]
- Li, G.; Tao, L.; Meng, J.; Ye, S.; Feng, G.; Zhao, D.; Hu, Y.; Tang, M.; Song, T.; Fu, R.; et al. Research on mode adjustment control strategy of upper limb rehabilitation robot based on interactive force fuzzy recognition. J. Biomed. Eng. 2018, 41, 90–97. [Google Scholar]
- Zhou, Z.; Meng, W.; Ai, Q.; Liu, Q.; Wu, X. Practical Velocity Tracking Control of a Parallel Robot Based on Fuzzy Adaptive Algorithm. Adv. Mech. Eng. 2019, 5, 574896. [Google Scholar] [CrossRef]
- Arkhipov, M.V.; Kocherevskaya, L.B.; Matrosova, V.V. Control of Manipulation Robot Interacting with Elastic Objects Using Simmechanics. In Proceedings of the 2021 International Conference on Industrial Engineering, Applications and Manufacturing (ICI-EAM), Sochi, Russia, 24–28 May 2021. [Google Scholar] [CrossRef]
- Wang, L.; Li, C.; Liu, Y.; Zhang, J. Experimental Research on Force-based Impedance Control of Arm Rehabilitation Robot. China Mech. Eng. 2008, 19, 1518–1522. [Google Scholar]
- Gao, J.; Liu, L.; Wang, J.; Li, X.; Ding, S.; Gao, Y.; Wang, X. Upper limb rehabilitation robot based on fuzzy control variable admittance control. J. Zhengzhou Univ. (Eng. Sci.) 2024, 2024, 12–20. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Application Part | Equipment/Robot | Scope of Action | Technical Type and Mode of Action | Number of Techniques | Manipulation Techniques | Cost-Effectiveness | Core Advantages | Main Limitations | Common Points | R&D Stage |
|---|---|---|---|---|---|---|---|---|---|---|
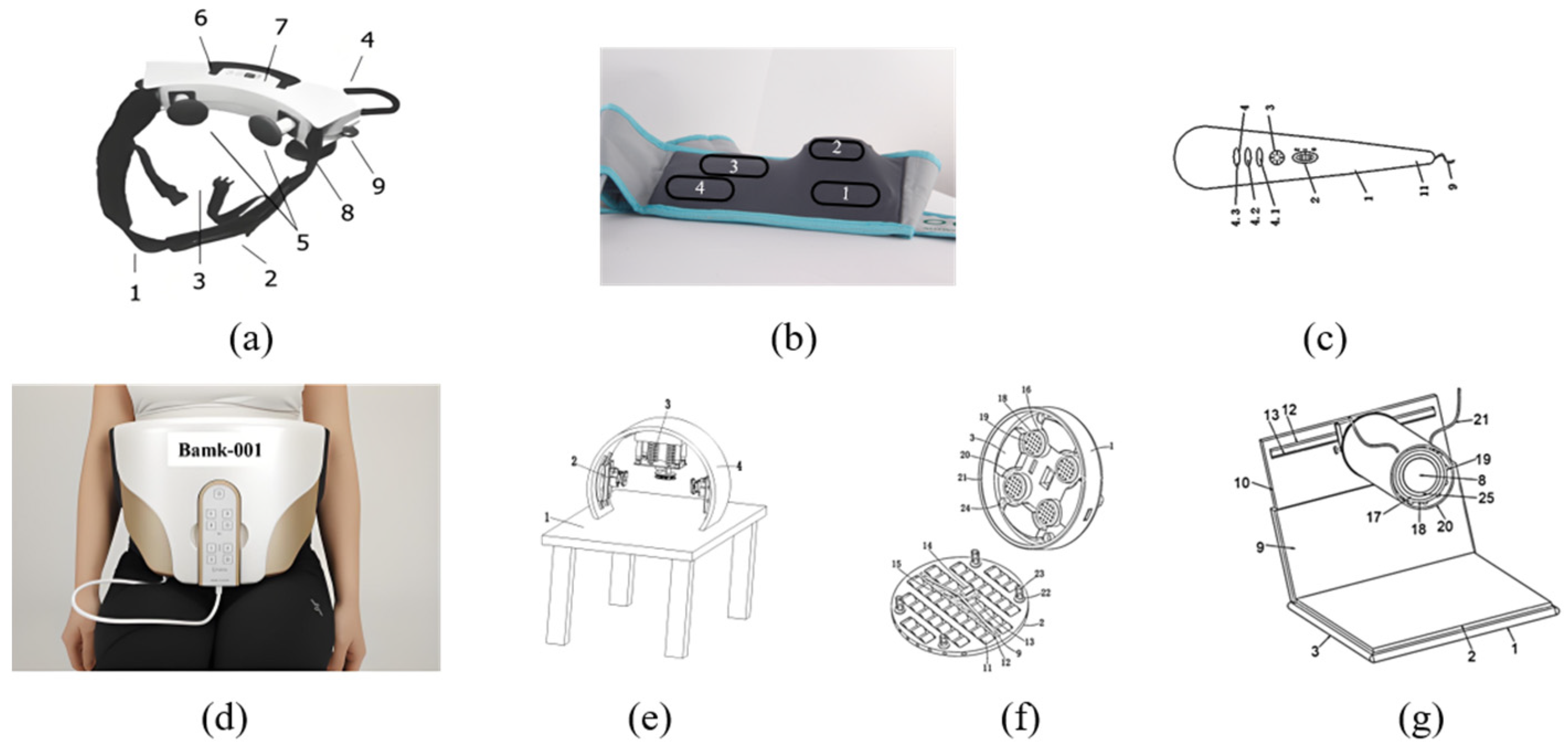
| Abdomen | Free-Lax (2005) [12] | 2 points | Mechanical action type | 1 | Vibrating | Low | An early clinical product; easy to operate; with three action frequencies | Single function, local normal mechanical vibration, only available for sitting massage, unable to adapt to complex abdominal contours | 1. No research on precise force control. 2. No intelligent path planning. 3. No biofeedback functions | Commercialized product |
| MOWOOT (2014) [13,14] | 4 points | Mechanical action type | 1 | Pressing | 1450 € | An early commercial product for clockwise massage, easy to operate, with rhythmic intermittent extracolonic peristalsis. | Single function, limited movement freedom due to wearable fixation, unable to dynamically adjust the path | Commercialized product | ||
| An intestinal management training massaging device (2016) [15] | The whole abdomen | Manually operated mode | 1 | Vibrating | Low | Flexible use for assisting manual operation | Relying on the operator; poor repeatability | Conceptual design | ||
| Bamk001 (2018) [17,18] | 5 points | Pneumatic pressurization | 1 | Pressing | 10,400 € | Even pressure distribution, with hot compress function, clockwise massage, and pressurized clockwise massage | Complex pneumatic circuit system; high maintenance cost | Commercialized product | ||
| A nursing massage robot for promoting digestion (2018) [19] | 3 points | Mechanical action type | 1 | Pressing | High | Considering the lateral action range of the abdomen, with a flexible energy storage structure, high safety | Large-scale equipment; single function; local directional action | Conceptual design | ||
| A new-type abdominal massage device (2020) [20] | The whole abdomen | Manually operated mode | 1 | Rolling | Low | Hot compress, wide action range, assisting manual operation | Relying on the operator; poor repeatability; planar rolling | Conceptual design | ||
| A digestive medicine abdominal massage device (2021) [21] | The whole abdomen | Mechanical action type | 1 | Rolling | Medium | Hot compress, adjustable according to the width of the human abdomen | The single function requires people to actively lie in the interlayer, inconvenient to use, tangential plane rolling, unable to adapt to complex abdominal contours | Conceptual design | ||
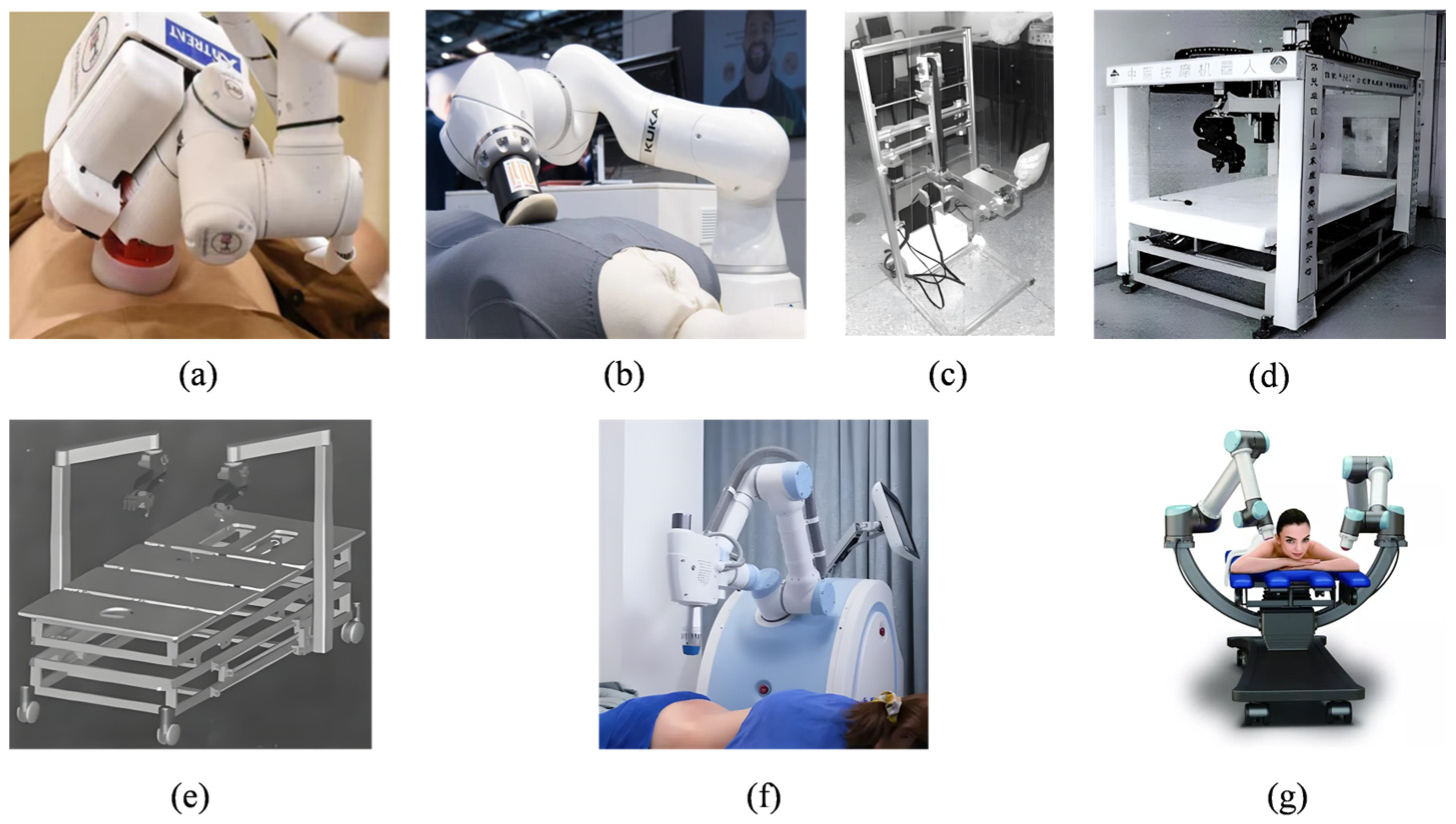
| Non-abdominal part | PUMA 562 (2003) [22] | Thoracic and lumbar regions of the back | Mechanical action type | 2 | Kneading and pinching | High | Force collection by single-axis pressure sensors, adaptive trajectories | Unable to adapt to the patient’s movement during the massage process | 1. High repeatability. 2. Relatively intelligent trajectory planning and force control matching. 3. More manipulation techniques. 4. High research costs. 5. Little research on massage force. 6. Not applicable to households | Commercialized product |
| The physiotherapy robot EMMA (2016) [23] | Mainly in the back | 2 | Pressing and pushing | High | Analysis of patients’ conditions with 3D vision technology, measurement of muscle stiffness degree using sensors, scientific traditional Chinese medicine evaluation, temperature ranging from 38 °C to 40 °C | Insufficient diversity of manipulation techniques | Commercialized product | |||
| The IYU massage robot (2018) [24] | Mainly in the back | 3 | Pressing, pushing and kneading | High | 3D vision technology adaptable to patients’ body shapes, with massage gloves at the end featuring rich manipulation techniques | Complex operation | Commercialized product | |||
| A 4-degree-of-freedom household massage robot [25] | Back | 3 | Point pressing; tapping and kneading | Medium | Ensuring the number of manipulation techniques by switching massage heads, a high degree of integration | Lack of autonomous perception ability, relying on remote control, with preset movement trajectories, unable to adapt personally. | Principle prototype | |||
| The LLR-1 traditional Chinese medicine massage robot (2012) [26] | Mainly in the back | 6 | Kneading, pressing, pushing, vibrating, rolling and pinching | High | 3rd-generation iteration, rich manipulation techniques, safety mechanism, and capable of detecting physiological signals such as blood pressure and pulse | Visual recognition relying on color marking points, inconvenient in the application | Principle prototype | |||
| The JZMR-I traditional Chinese medicine massage robot (2012) [31,32] | Lumbar vertebrae and lower limbs | 5 | Kneading, rolling, pressing, pinching and vibrating | High | Individual adjustment of the pose and location of the massaging part with 2 robotic arms | Relying on operators to operate the robot according to the feedback information of the 3D model, lacking self-adaptive ability | Principle prototype | |||
| A massage robot based on a decoupled parallel mechanism (2015) [33] | Mainly in the back | 9 | Patting, pressing, pointing, pushing, rubbing, vibrating, circular Rubbing, rolling and kneading | High | Serial–parallel mechanism configuration, reducing mechanism coupling and simplifying control difficulty | The maturity of the working end needs improvement | Principle prototype | |||
| A hybrid-connected robot based on traditional Chinese medicine massage techniques (2021) [34] | Not specified | 13 | Rolling, kneading, circular rubbing, pushing, rubbing, wiping, pressing, pointing, patting, beating, plucking, vibrating and one-finger meditation pushing | High | Series-type massage robotic arm and parallel-type massage device with a reasonable working space | Low maturity of control research | Conceptual design | |||
| The AUBO collaborative robot [35] | 2 | Pressing and pushing | High | Infrared diagnosis and treatment, radio-frequency thermodynamics, flexible robotic arm, ergonomic design | Lack of sufficient materials | Commercialized product | ||||
| The UR collaborative robot [36] | 2 | Pressing and pushing | High | High safety, easy to use, and intuitive programming function | Not specifically designed for massage, intelligent control of massage at the engineering level | Commercialized product | ||||
| The 7-degree-of-freedom redundant robotic arm DLR [37] | 2 | Pressing and pushing | High | A hand with 19 degrees of freedom, high flexibility, capable of performing fine movements, high integration, and high robustness | Not specifically designed for massage, intelligent control of massage at the engineering level | Commercialized product |
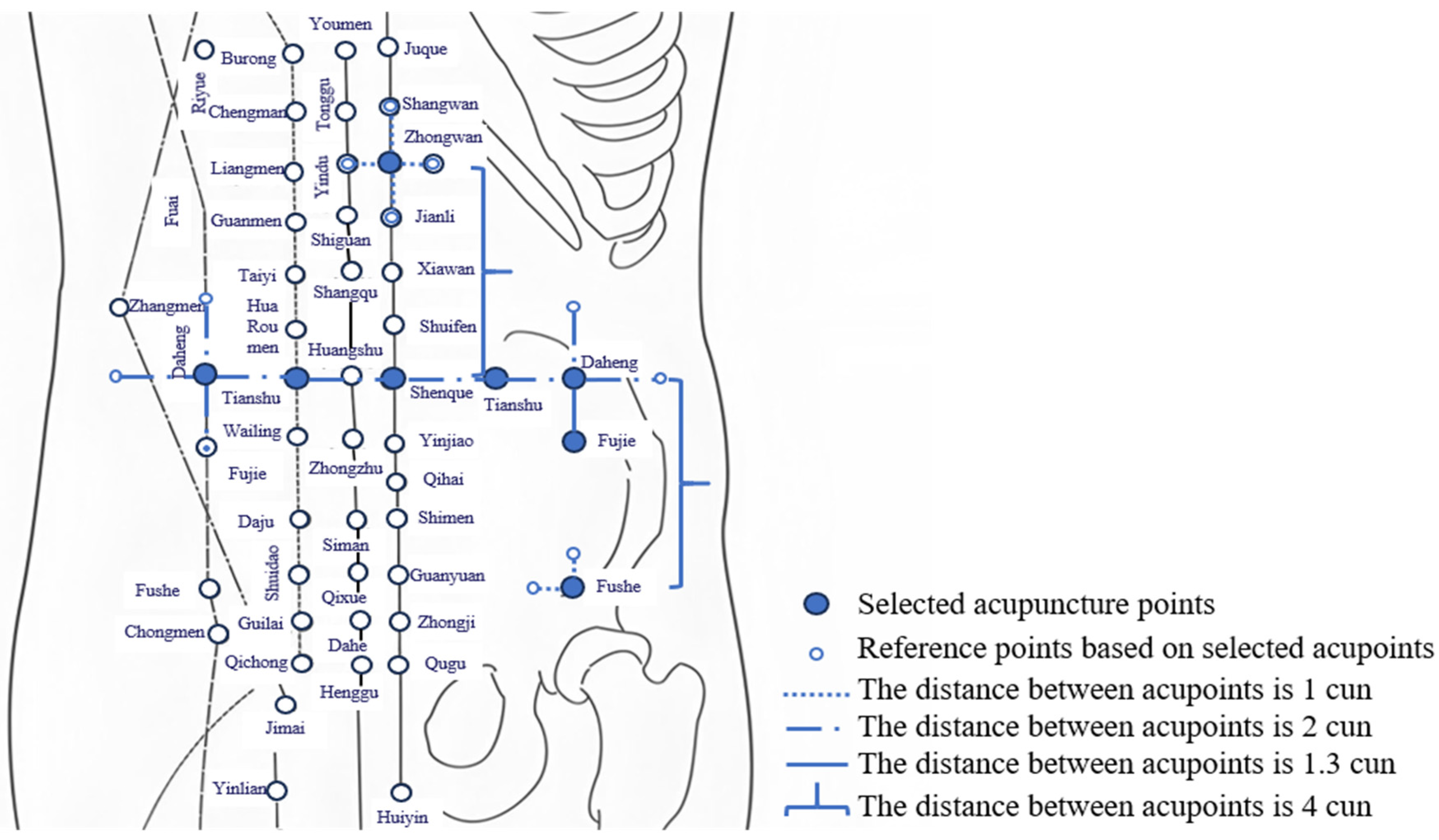
| The Selected Body Surface Features or Acupoints of the Human Body | Representative Distance |
|---|---|
| From the left Yunmen acupoint to the right Yunmen acupoint | 12 cun * |
| Between the two nipples of the human body | 8 cun |
| From Tiantu sSuprasternal fossa) to Qigu (the midpoint of the xiphisternal joint) | 9 cun |
| From Qigu (the midpoint of the xiphisternal joint) to Shenque (umbilicus) | 8 cun |
| Thumb breadth measurement | 1 cun |
| Middle finger breadth measurement | 1 cun |
| Four-finger breadth measurement | 3 cun |
| Fuzzy Set | Left Border a | Vertex b | Right Border c |
|---|---|---|---|
| NB (negative large) | 0 | 0 | 5 |
| NS (negative large) | 0 | 5 | 10 |
| ZO (zero) | 5 | 10 | 15 |
| PS (positive small) | 10 | 15 | 20 |
| PB (positive large) | 15 | 20 | 20 |
| EC\E | NB (Negative Large) | NS (Negative Small) | ZO (Zero) | PS (Positive Small) | PB (Positive Large) |
|---|---|---|---|---|---|
| NB (negative large) | PB | PB | PS | ZO | NM |
| NS (negative small) | PB | PM | PS | NS | NM |
| ZO (zero) | PB | PS | ZO | NS | NB |
| PS (positive small) | PM | S | PS | NM | NB |
| PB (positive large) | PM | ZO | PS | NM | NB |
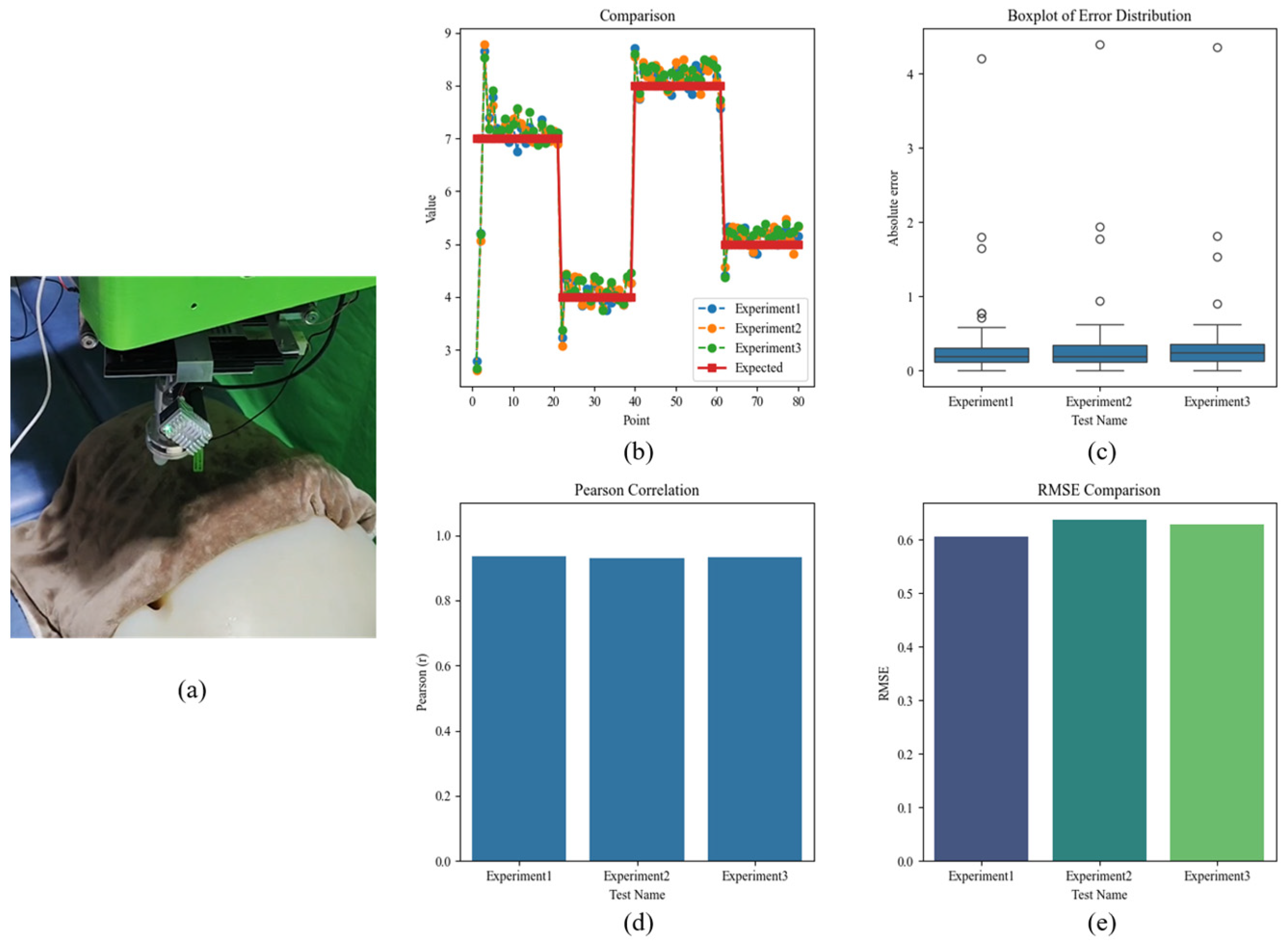
| Test | MRE (%) | MAE | RMSE | Pearson Correlation Coefficient | Margin of Error | |
|---|---|---|---|---|---|---|
| Experiment1 | Test 1 | 5.0184 | 0.3061 N | 0.6050 | 0.9353 | 4.2129 |
| Experiment2 | 5.3711 | 0.3232 N | 0.6371 | 0.9286 | 4.3934 | |
| Experiment3 | 5.6272 | 0.3391 N | 0.6292 | 0.9315 | 4.3632 | |
| Experiment1 | Test 2 | 9.6815 | 0.5157 N | 0.8348 | 0.8872 | 4.0483 |
| Experiment2 | 8.0326 | 0.4329 N | 0.7130 | 0.9172 | 4.0156 | |
| Experiment3 | 7.2070 | 0.3821 N | 0.6609 | 0.9273 | 3.9724 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, X.; Shi, P.; Luo, Z.; Yu, H. A Novel 6-DOF Multi-Technique Abdominal Massage Robot System: A New Solution for Relieving Constipation and an Exploration of Standardization. Electronics 2025, 14, 1123. https://doi.org/10.3390/electronics14061123
Tang X, Shi P, Luo Z, Yu H. A Novel 6-DOF Multi-Technique Abdominal Massage Robot System: A New Solution for Relieving Constipation and an Exploration of Standardization. Electronics. 2025; 14(6):1123. https://doi.org/10.3390/electronics14061123
Chicago/Turabian StyleTang, Xinyi, Ping Shi, Zhenjie Luo, and Hongliu Yu. 2025. "A Novel 6-DOF Multi-Technique Abdominal Massage Robot System: A New Solution for Relieving Constipation and an Exploration of Standardization" Electronics 14, no. 6: 1123. https://doi.org/10.3390/electronics14061123
APA StyleTang, X., Shi, P., Luo, Z., & Yu, H. (2025). A Novel 6-DOF Multi-Technique Abdominal Massage Robot System: A New Solution for Relieving Constipation and an Exploration of Standardization. Electronics, 14(6), 1123. https://doi.org/10.3390/electronics14061123