



Smart Waiting Room: A Systematic Literature Review and a Proposal

 ,
, 
 , ,
, ,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
- RQ1: what is the purpose of the proposed smart waiting room?
- RQ2: what category (or categories) of patients does the identified solution address?
- RQ3: what technologies do the identified solutions adopt?
- RQ4: in which clinical contexts (ER, hospital, GP office, etc.) are the identified solutions adopted?
2. Review Methodology
2.1. Database and Queries
- Q1: “smart” AND “waiting room”;
- Q2: “techn*” AND “waiting room”;
- Q3: “virtual” AND “waiting room”;
- Q4: “smart” AND “foyer”.
2.2. Article Retrieval and Selection Process
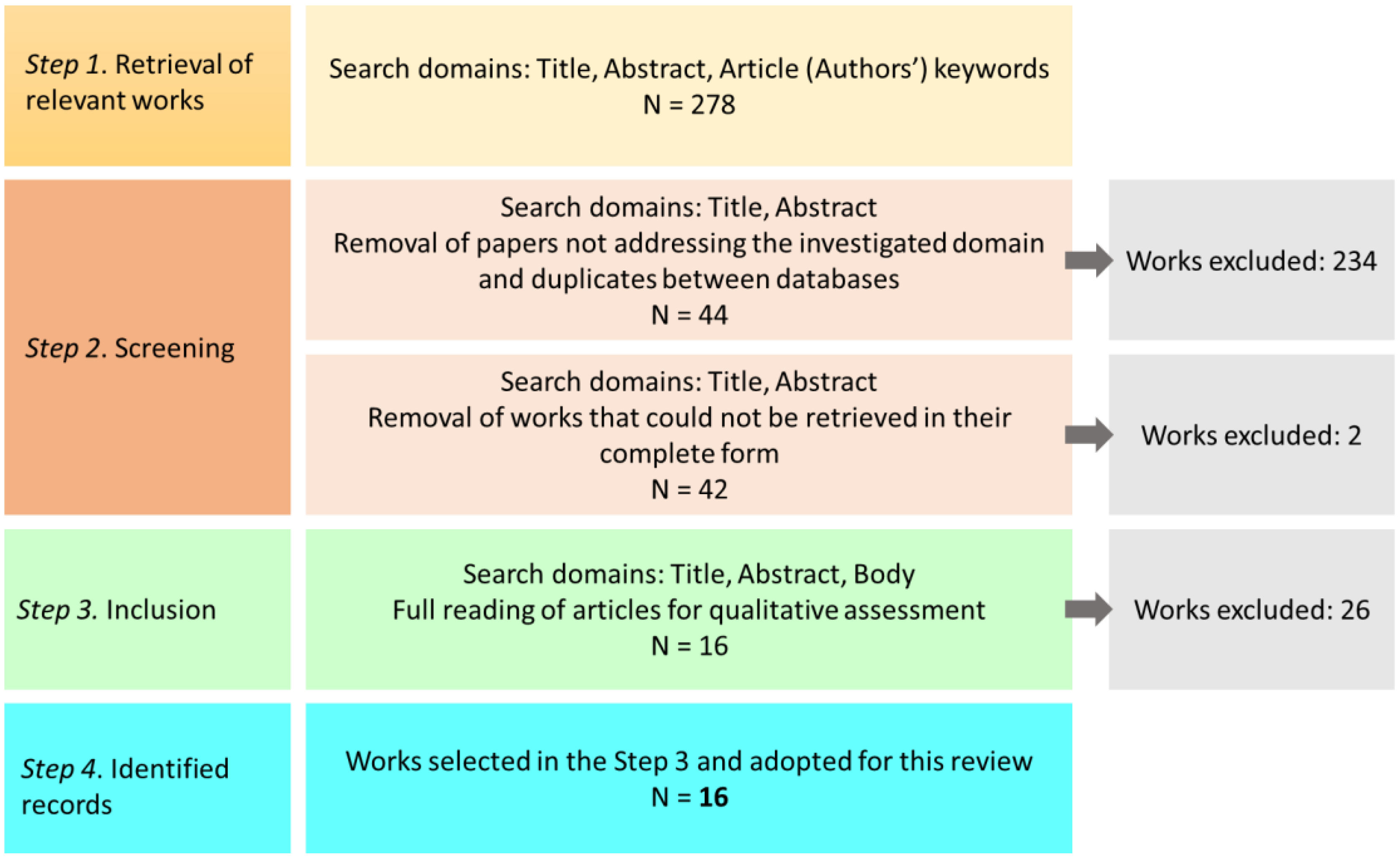
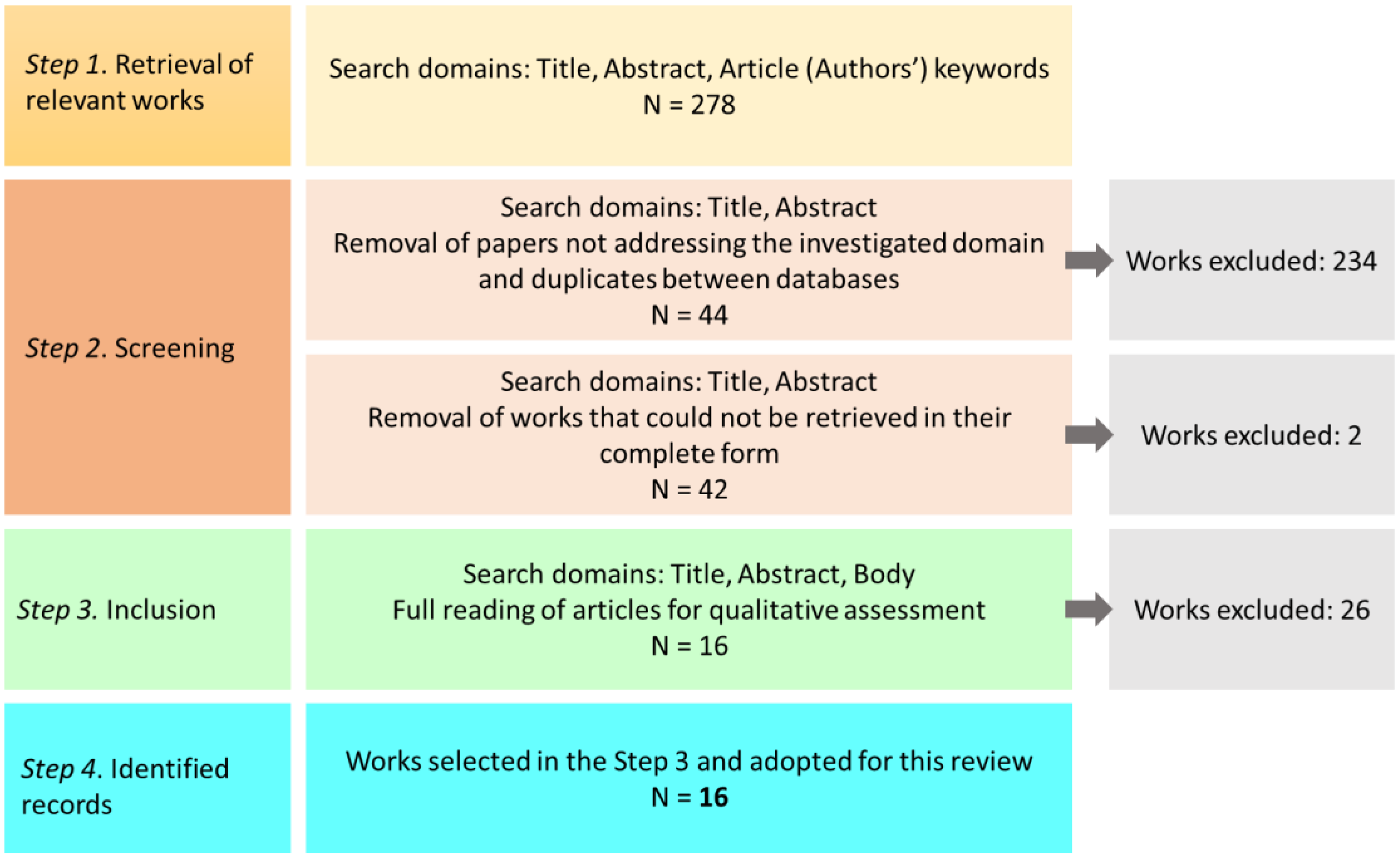
- Retrieval of the works: In this step, the search retrieved 278 works. Taking into account the specific RQs, the search was limited to subject areas: computer science, engineering, medicine, social sciences, and decision sciences.
- Screening: The retrieved works’ abstracts, titles, and authors’ keywords were scrutinized to provide a preliminary qualitative evaluation, assessing whether or not the retrieved works addressed the domain underlying the four RQs. In this step, duplicate works were also identified and removed. A total of 213 papers were found not to meet the criteria (i.e., they did not address clinical waiting rooms, or they did not rely on any technology). In comparison, 21 papers were duplicated among the different databases. The number of papers identified as relevant was 44. Finally, the 44 works were accessed in their complete form, resulting in 2 papers being removed due to their inaccessibility.
- Inclusion: The 42 papers identified in the previous step were carefully read by three of the authors of this review to assess their adherence to the RQs identified in the Introduction. At the end of this step, 26 papers were found unsuitable to answer any of the RQs.
- Identified records: the number of papers included in this review was 16.
3. Results
3.1. Biliometric Results
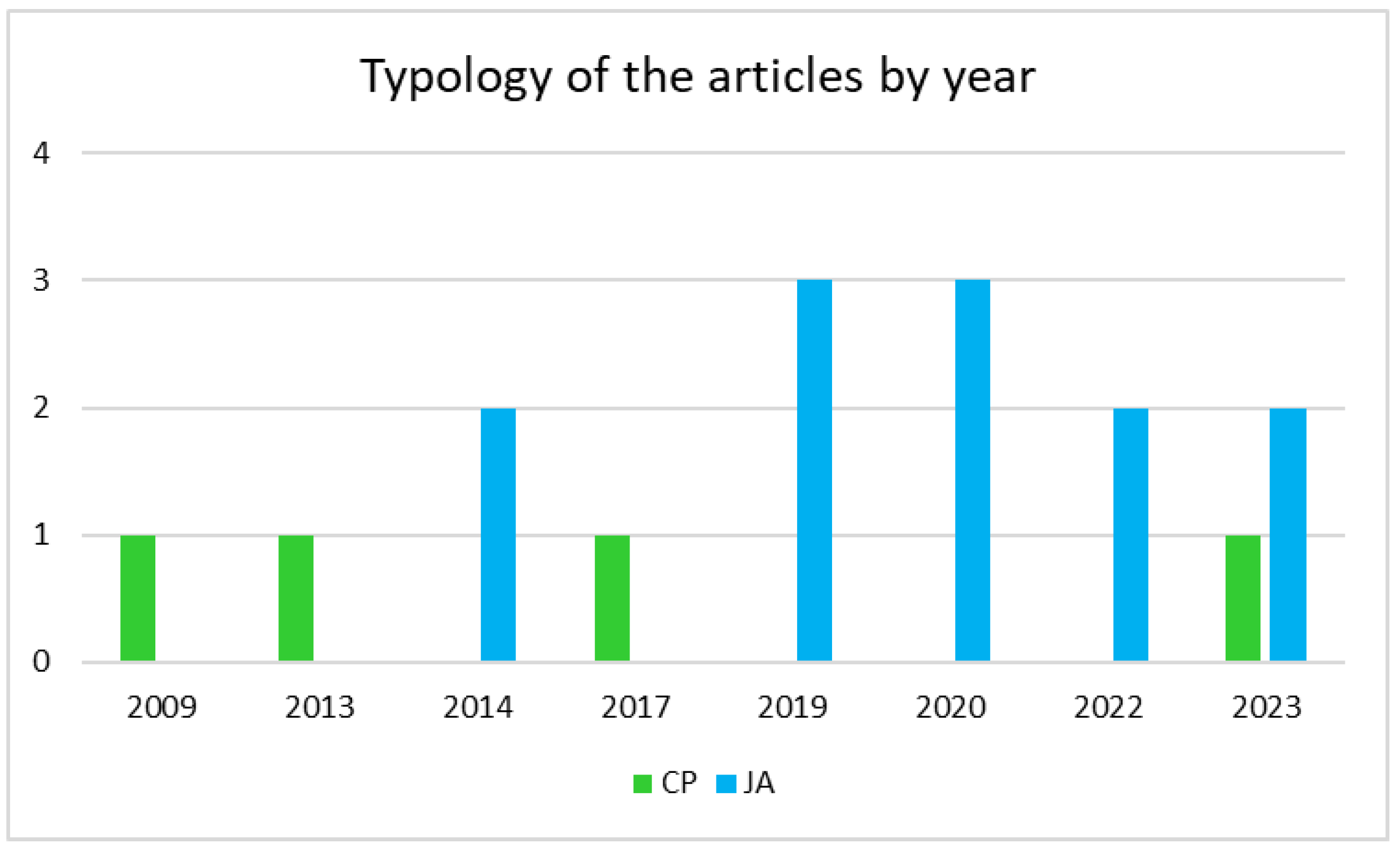
3.1.1. Temporal Distribution and Type of Articles by Year
3.1.2. Geographical Distribution of the Authors
3.2. Content Analysis
3.2.1. Purposes of the Smart Waiting Rooms
- (A)
- Waiting enhancement: the solutions address the problem of shortening or optimizing the waiting times or produce some effects on the waiting patients (e.g., reduce anxiety, provide them with more information about the medical procedures they are going to experience, inform them of some particular aspects of a disease);
- (B)
- Pre-visit data acquisition: the solutions are devoted to exploiting the waiting time in the waiting rooms to acquire physiological or psychological measurements from patients; the acquired data are necessary for the subsequent visit;
- (C)
- Assessment and diagnosis: waiting times are exploited to perform an assessment of some clinical aspects of the patients and are not necessarily related to the visit they are undergoing.
3.2.2. Types of Patients Addressed by Smart Waiting Rooms
3.2.3. Technologies Involved in the Surveyed Smart Waiting Rooms
3.2.4. Clinically Applicative Contexts
4. Discussion
4.1. Late Attention towards Waiting Rooms
4.2. Acting on the Waiting
4.3. The Role of Smart Technologies in the Surveyed Solutions
4.4. Smart Waiting Rooms Designed Not for All
4.5. Challenges and Research Directions for Smart Waiting Room
- The review results underlined the lack of generalizability of the smart waiting rooms surveyed; the majority of the solutions were designed for specific types of patients, thus hindering the adoption of such solutions on a larger scale. However, a few works also tackled exploiting EHRs; these data can be adopted to understand patients’ needs and provide them with tailored solutions—similar to what occurs in smart homes and environments [53,54,55]. Smart waiting rooms should, thus, be able to provide layered services—i.e., smart services for every waiter with the possibility of personalizing each of them in some regard according to the user’s specific needs. For example, the self-assessment of blood pressure relying on biomedical equipment and mobile applications should take into account the patient’s age and health condition (sight, cognitive abilities, and other information entailed by patient’s EHR) and their familiarity with technologies; for older patients or non-tech-savvy patients, the smart waiting room system should adapt the interface and provide a detailed tutorial regarding how to conduct a self-assessment using the equipment at hand. Similarly to [30], such a system should also be able to assess whether or not the patient was able to perform the required measurement in an appropriate way.
- Virtual reality is a powerful technology for stress relief in waiting rooms; however, this technology can also be exploited for diagnostic purposes and to acquire relevant insights regarding patients’ conditions. Virtual technologies are indeed known for the possibility of supporting the diagnosis and assessment of both cognitive and neurological conditions [56,57]. Smart waiting rooms should provide virtual technologies with the dual aim of reducing pre-intervention anxiety and stress while acquiring diagnostic data. This, combined with the possibility of leveraging EHRs, could enhance diagnostic processes and make wait times both more bearable and fruitful.
- It is striking that AI adoption in smart waiting rooms is limited to patients’ flow prediction or simulation, with only three works addressing decision support; wearable IoT technologies combined with AI can support the early diagnosis of several diseases and conditions (see, for example, [58,59,60]). The integration of non-invasive wearable monitoring technologies into smart waiting rooms is more than plausible, supporting the prompt identification of conditions that should be monitored and, ultimately, reducing the burden on healthcare structures.
- There is a relevant absence in the solutions reviewed; none of the works analyzed referred to the physical and built environment of the waiting room. However, researchers have spent a large amount of effort to identify the interactions and effects between the waiting room environment and waiters [38,42,61]. On the other hand, the design of waiting spaces (physical and environmental features) can completely change the healthcare experience. A significant challenge could be the integration between physical and digital IoT-enabled environments to meet one or more of the purposes identified by the three clusters (Section 3.2.1). Patients’ physical interactions with one or more components of the environment could be used for diagnostic and monitoring purposes, as well as for entertainment and relaxation purposes by stimulating the senses, enhancing psychological comfort, and physical activities.
- Emerging from the discussions in Section 4, smart waiting rooms should be characterized by a variety of technologies. Although the adoption of “safe and sound” technologies such as mobile applications makes the whole smart solution more acceptable, it hinders the “smartness” of the solution itself and its generalizability. More studies on adopting IoT technologies within smart waiting room environments should be conducted to investigate the acceptance of such technologies from both the patients’ and clinical personnel’s perspectives.
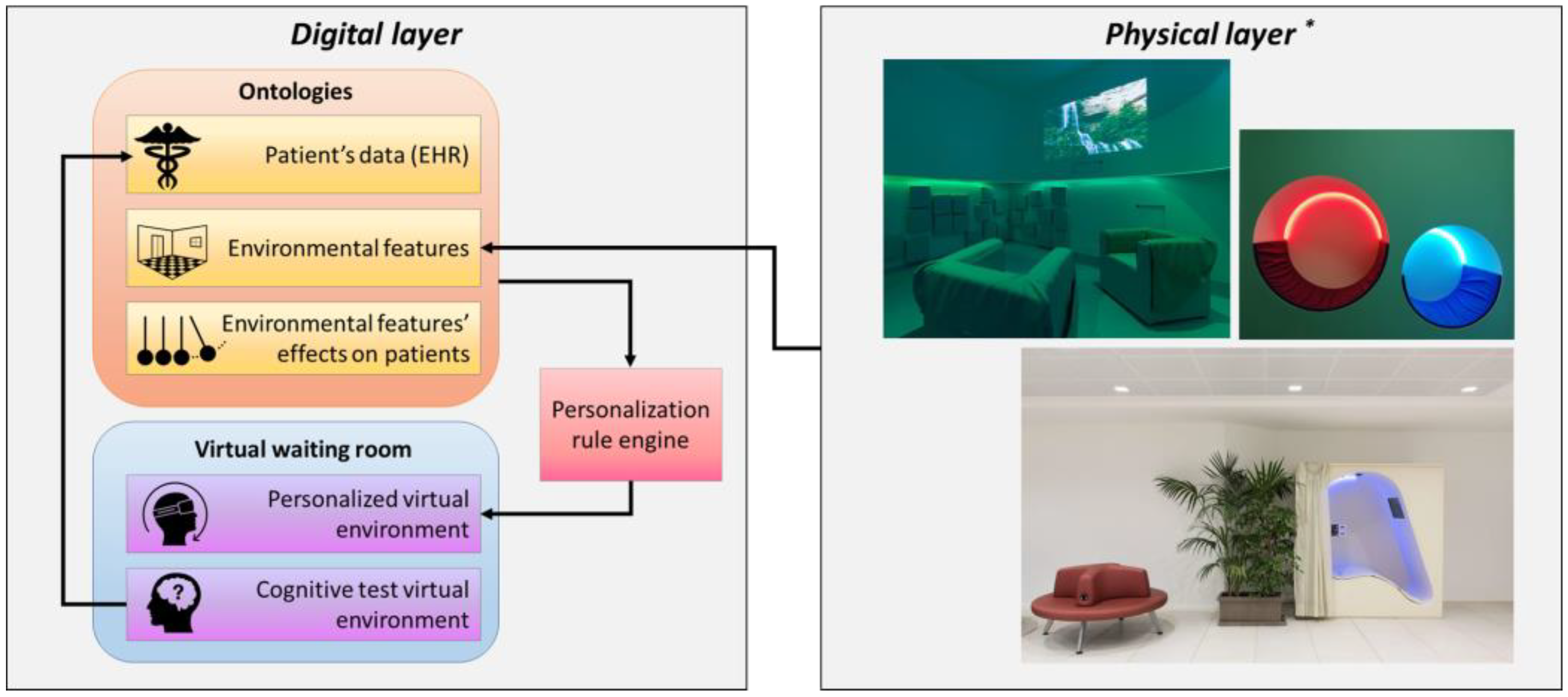
5. A proposal for a Smart Waiting Room
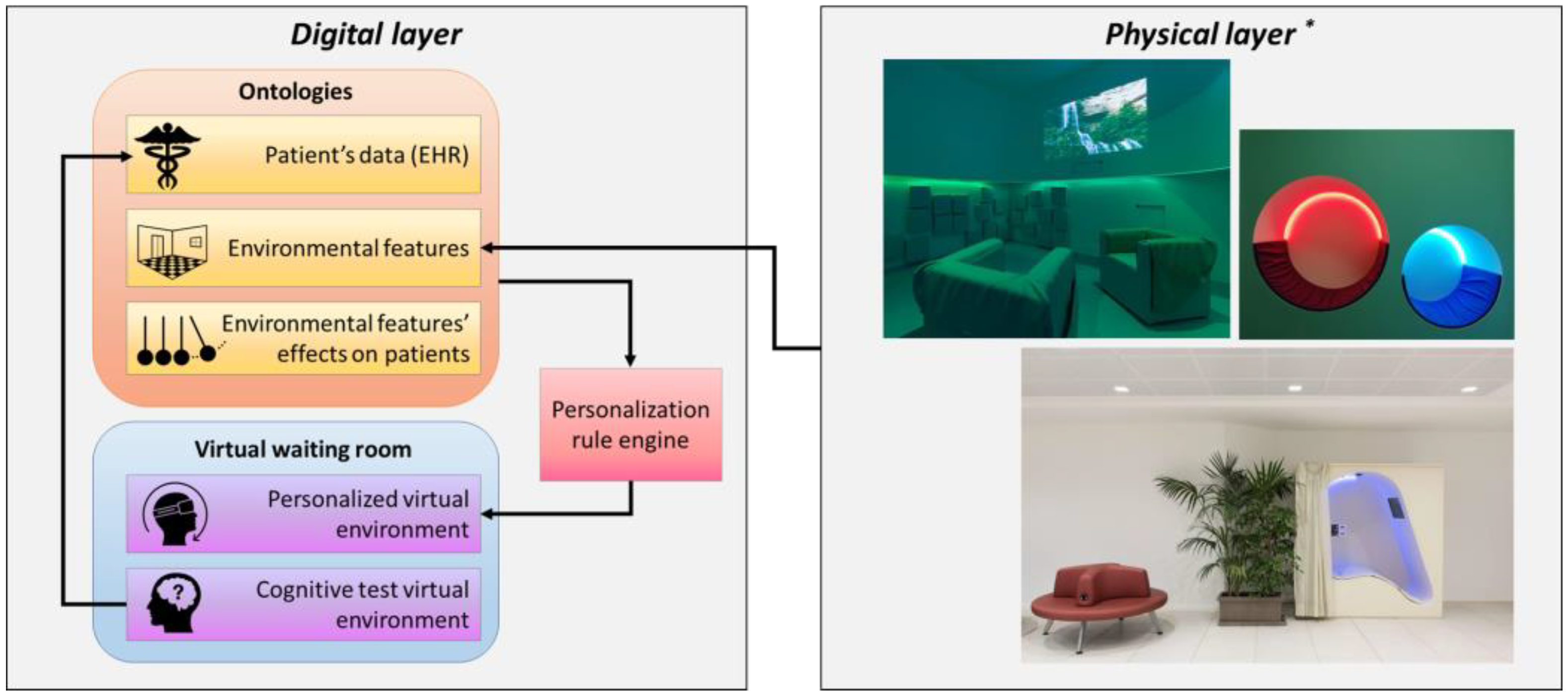
5.1. Physical Layer
- It is important to maintain a good balance in sensory stimulation, to not be overwhelmed with too many stimuli, and, on the contrary, to not cause boredom and sensory deprivation. As an example, noise and strong lights, such as crowded environments, activate people’s sensory stimulation and can produce stress.
- The coherence and the comprehension of spaces reduce the level of stress in people (both outpatients and staff).
- The affordances of spaces and components improve the user experience, affecting people’s behaviors.
- One of the most important elements affecting stress is the possibility of controlling aspects of the physical and social environment and customizing spaces (acting on light, indoor temperature, etc.). Privacy is another example of perception control, as it affects the ability to control social interactions.
5.2. Digital Layer
5.2.1. Ontologies for EHR and Personalization
5.2.2. Virtual Environment for Cognitive Assessment
- Familiarization: In this phase, the user familiarizes her/himself with the VR scenario (e.g., looking around and observing all the objects) and VR equipment use (e.g., use of the controllers, movements in the virtual environment, selecting the items). Simultaneously, users receive straightforward instructions on the key actions they must perform in subsequent phases and are prompted to rehearse them. For example, to select objects in the scenario, the user physically approaches the object, and when the hand is in proximity to the object, the object lights up. To select it, the user must click the button in the controller.
- Encoding: In this phase, the user must memorize the location of four objects. The objects are presented one at a time, and each is presented four times for 12 searches. The user is asked to search for each object within the waiting room by physically reaching for it. Once the subject’s hands are near the object, the object will light up, and the user can pick it up by clicking on the controller button. The four objects are randomized in the four presentations, and the objects always appear in the same position (e.g., object 1 is always on the coffee table, object 2 is always next to the plant).
- Forgetting: in this phase, the user spends 10 min outside the virtual waiting room with the aim of generating oblivion.
- Recall: In this phase, the user, adhering to the instructions, must reposition the objects they found during the encoding phase to their original positions, exactly as they were initially discovered. The user starts the task in the middle of the room, and an object appears in front of him/her. Therefore, the user is instructed to bring the object to the original location when presented during the encoding phase. Once positioned, a second object appears in front of him/her, which must be positioned like the previous one. The total duration of the cognitive assessment in the virtual waiting room, including the four phases, is approximately 30–35 min.
5.3. Use Cases
5.4. Relevance of the Use Cases
6. Challenges and Limitations of the Age-IT Smart Waiting Room
7. Conclusions and Future Works
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Alaa, M.; Zaidan, A.A.; Zaidan, B.B.; Talal, M.; Kiah, M.L.M. A Review of Smart Home Applications Based on Internet of Things. J. Netw. Comput. Appl. 2017, 97, 48–65. [Google Scholar] [CrossRef]
- Hutton, D.M. Smart Environments: Technology, Protocols and Applications. Kybernetes 2005, 34, 903–904. [Google Scholar] [CrossRef]
- Solaimani, S.; Bouwman, H.; Baken, N. The Smart Home Landscape: A Qualitative Meta-Analysis. In Proceedings of the toward Useful Services for Elderly and People with Disabilities—9th International Conference on Smart Homes and Health Telematics, ICOST 2011, Montreal, QC, Canada, 20–22 June 2011; pp. 192–199. [Google Scholar]
- Liu, P.; Li, G.; Jiang, S.; Liu, Y.; Leng, M.; Zhao, J.; Wang, S.; Meng, X.; Shang, B.; Chen, L.; et al. The Effect of Smart Homes on Older Adults with Chronic Conditions: A Systematic Review and Meta-Analysis. Geriatr. Nurs. 2019, 40, 522–530. [Google Scholar] [CrossRef] [PubMed]
- McIlvennie, C.; Sanguinetti, A.; Pritoni, M. Of Impacts, Agents, and Functions: An Interdisciplinary Meta-Review of Smart Home Energy Management Systems Research. Energy Res. Soc. Sci. 2020, 68, 101555. [Google Scholar] [CrossRef]
- Thompson, D.A.; Yarnold, P.R.; Williams, D.R.; Adams, S.L. Effects of Actual Waiting Time, Perceived Waiting Time, Information Delivery, and Expressive Quality on Patient Satisfaction in the Emergency Department. Ann. Emerg. Med. 1996, 28, 657–665. [Google Scholar] [CrossRef]
- Camacho, F.; Anderson, R.; Safrit, A.; Jones, A.S.; Hoffmann, P. The Relationship between Patient’s Perceived Waiting Time and Office-Based Practice Satisfaction. N. Carol. Med. J. 2006, 67, 409–413. [Google Scholar] [CrossRef]
- Bleustein, C.; Rothschild, D.B.; Valen, A.; Valatis, E.; Schweitzer, L.; Jones, R. Wait Times, Patient Satisfaction Scores, and the Perception of Care. Am. J. Manag. Care 2014, 20, 393–400. [Google Scholar]
- Reichert, A.; Jacobs, R. The Impact of Waiting Time on Patient Outcomes: Evidence from Early Intervention in Psychosis Services in England. Health Econ. 2018, 27, 1772–1787. [Google Scholar] [CrossRef]
- Mowen, J.C.; Licata, J.W.; McPhail, J. Waiting in the Emergency Room: How to Improve Patient Satisfaction. J. Health Care Mark. 1993, 13, 26–33. [Google Scholar]
- Arneill, A.B.; Devlin, A.S. Perceived quality of Care: The influence of the waiting room environment. J. Environ. Psychol. 2002, 22, 345–360. [Google Scholar] [CrossRef]
- Naiker, U.; FitzGerald, G.; Dulhunty, J.M.; Rosemann, M. Time to Wait: A Systematic Review of Strategies that Affect out-Patient Waiting Times. Aust. Health Rev. 2018, 42, 286. [Google Scholar] [CrossRef]
- Fernández-Aguilar, C.; Casado-Aranda, L.-A.; Farrés Fernández, M.; Minué Lorenzo, S. Has COVID-19 Changed the Workload for Primary Care Physicians? The Case of Spain. Fam. Pract. 2021, 38, 780–785. [Google Scholar] [CrossRef]
- Katz, G.M.; Bach, K.; Bobos, P.; Cheung, A.; Décary, S.; Goulding, S.; Herridge, M.S.; McNaughton, C.D.; Palmer, K.S.; Razak, F.A.; et al. Understanding How Post–COVID-19 Condition Affects Adults and Health Care Systems. JAMA Health Forum 2023, 4, e231933. [Google Scholar] [CrossRef]
- KFF Health Tracking Poll—May 2020. Available online: https://www.kff.org/report-section/kff-health-tracking-poll-may-2020-health-and-economic-impacts/ (accessed on 12 December 2023).
- Macdonald, N.; Clements, C.; Sobti, A.; Rossiter, D.; Unnithan, A.; Bosanquet, N. The Building Backlog of NHS Elective Cases Post COVID-19. Br. J. Surg. 2020, 107, e377–e378. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.E.; Haydon, H.M.; Mehrotra, A.; Caffery, L.J.; Snoswell, C.L.; Banbury, A.; Smith, A.C. Building on the Momentum: Sustaining Telehealth beyond COVID-19. J. Telemed. Telecare 2022, 28, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Biddiss, E.; Knibbe, T.J.; McPherson, A. The Effectiveness of Interventions Aimed at Reducing Anxiety in Health Care Waiting Spaces. Anesth. Analg. 2014, 119, 433–448. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Mtonga, K.; Kumaran, S.; Mikeka, C.; Jayavel, K.; Nsenga, J. Machine Learning-Based Patient Load Prediction and IoT Integrated Intelligent Patient Transfer Systems. Future Internet 2019, 11, 236. [Google Scholar] [CrossRef]
- Miller, S.; Gilbert, S.; Virani, V.; Wicks, P. Patients’ Utilization and Perception of an Artificial Intelligence–Based Symptom Assessment and Advice Technology in a British Primary Care Waiting Room: Exploratory Pilot Study. JMIR Hum. Factors 2020, 7, e19713. [Google Scholar] [CrossRef]
- Lin, Y.-C.; Padman, R. Process Visibility Analysis in Ambulatory Care: A Simulation Study with RFID Data. Stud. Health Technol. Inform. 2013, 192, 768–772. [Google Scholar]
- Gilliam, M.L.; Martins, S.L.; Bartlett, E.; Mistretta, S.Q.; Holl, J.L. Development and Testing of an IOS Waiting Room “App” for Contraceptive Counseling in a Title X Family Planning Clinic. Am. J. Obstet. Gynecol. 2014, 211, 481.e1–481.e8. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.U.I.; Jaradat, R.M.; Khasawneh, M.T. Reducing Patient Waiting Time in an Outpatient Clinic: A Discrete Event Simulation (DES) Based Approach. In Proceedings of the 2017 Industrial and Systems Engineering Conference, Pittsburgh, PA, USA, 20–23 May 2017. [Google Scholar]
- Bao, T.; Deng, G.; DeMarzo, L.A.; Zhi, W.I.; DeRito, J.L.; Blinder, V.; Chen, C.; Li, Q.S.; Green, J.; Pendleton, E.; et al. A Technology-Assisted, Brief Mind-Body Intervention to Improve the Waiting Room Experience for Chemotherapy Patients: Randomized Quality Improvement Study. JMIR Cancer 2019, 5, e13217. [Google Scholar] [CrossRef] [PubMed]
- Al-Nerabieah, Z.; Alhalabi, M.-N.; Owayda, A.; Alsabek, L.; Bshara, N.; Kouchaji, C. Effectiveness of Using Virtual Reality Eyeglasses in the Waiting Room on Preoperative Anxiety: A Randomized Controlled Trial. Perioper. Care Oper. Room Manag. 2020, 21, 100129. [Google Scholar] [CrossRef]
- Ehrler, F.; Rochat, J.; Siebert, J.N.; Guessous, I.; Lovis, C.; Spechbach, H. Use of a Semiautomatic Text Message System to Improve Satisfaction with Wait Time in the Adult Emergency Department: Cross-Sectional Survey Study. JMIR Med. Inform. 2022, 10, e34488. [Google Scholar] [CrossRef]
- Reinders, I.M.A.; Cremers, G.R.; van Rooijen, S.J.; Leemans, J.C.; Perquin, C.W.; Geomini, P.M.A.J.; Maas, J.W.M.; Bongers, M.Y. The Effect of an Informative 360-Degree Virtual Reality Video on Anxiety for Women Visiting the One-Stop Clinic for Abnormal Uterine Bleeding: A Randomized Controlled Trial (VISION-Trial). Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 272, 96–103. [Google Scholar] [CrossRef]
- Liu, B.; Wang, W.; Zhang, Y.; Huang, R.; Raiti, J. Lullaland: A Multisensory Virtual Reality Experience to Reduce Stress. In Proceedings of the Extended Abstracts of the 2023 CHI Conference on Human Factors in Computing Systems, Hamburg, Germany, 23–28 April 2023; ACM: New York, NY, USA, 2023; pp. 1–6. [Google Scholar]
- Wagner, S.; Kamper, C.H.; Rasmussen, N.H.; Ahrendt, P.; Toftegaard, T.S.; Bertelsen, O.W. Reliable Blood Pressure Self-Measurement in the Obstetric Waiting Room. Methods Inf. Med. 2014, 53, 225–234. [Google Scholar] [CrossRef]
- Desai, S.; Stevens, E.; Emani, S.; Meyers, P.; Iversen, M.; Solomon, D.H. Improving Quality of Care in Rheumatoid Arthritis Through Mobile Patient-Reported Outcome Measurement: Focus Group Study. JMIR Form. Res. 2020, 4, e15158. [Google Scholar] [CrossRef]
- Doyle, T.E.; Kalsi, M.; Aiyush, B.; Yousuf, J.; Waseem, O. Non-Invasive Health Monitoring System (NIHMS). In Proceedings of the 2009 IEEE Toronto International Conference Science and Technology for Humanity (TIC-STH), Toronto, ON, Canada, 26–27 September 2009; pp. 703–707. [Google Scholar]
- Grant, R.W.; Lyles, C.; Uratsu, C.S.; Vo, M.T.; Bayliss, E.A.; Heisler, M. Visit Planning Using a Waiting Room Health IT Tool: The Aligning Patients and Providers Randomized Controlled Trial. Ann. Fam. Med. 2019, 17, 141–149. [Google Scholar] [CrossRef]
- Giskes, K.; Lowres, N.; Orchard, J.; Li, J.; McKenzie, K.; Hespe, C.M.; Freedman, B. Increasing Screening for Atrial Fibrillation in General Practice: The Atrial Fibrillation Self-Screening, Management and guideline-Recommended Therapy (AF Self-SMART) Study. Med. J. Aust. 2023, 218, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Alberts, J.L.; Shuaib, U.; Fernandez, H.; Walter, B.L.; Schindler, D.; Miller Koop, M.; Rosenfeldt, A.B. The Parkinson’s Disease Waiting Room of the Future: Measurements, Not Magazines. Front. Neurol. 2023, 14, 1212113. [Google Scholar] [CrossRef]
- IEEE. IEEE Thesaurus (July 2023). Available online: https://www.ieee.org/content/dam/ieee-org/ieee/web/org/pubs/ieee-thesaurus.pdf (accessed on 12 December 2023).
- Risteska Stojkoska, B.L.; Trivodaliev, K.V. A Review of Internet of Things for Smart Home: Challenges and Solutions. J. Clean. Prod. 2017, 140, 1454–1464. [Google Scholar] [CrossRef]
- Lai, J.C.-Y.; Amaladoss, N. Music in Waiting Rooms: A Literature Review. HERD Health Environ. Res. Des. J. 2022, 15, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Cass, S.J.; Ball, L.E.; Leveritt, M.D. Passive Interventions in Primary Healthcare Waiting Rooms Are Effective in Promoting Healthy Lifestyle Behaviours: An Integrative Review. Aust. J. Prim. Health 2016, 22, 198. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, D.; Chow, C.K. Waiting Time as an Indicator for Health Services Under Strain: A Narrative Review. INQUIRY J. Health Care Organ. Provis. Financ. 2020, 57, 004695802091030. [Google Scholar] [CrossRef]
- Bishop, P. Surveying “The Waiting Room”. Archit. Theory Rev. 2013, 18, 135–149. [Google Scholar] [CrossRef]
- Keirnan, A.; Murphy, A.; Pedell, S.; Marcello, F. Exploring Emotions for Technology and Service Design in Health Care Setting Waiting Rooms. In Proceedings of the 28th Australian Conference on Computer-Human Interaction—OzCHI ’16, Launceston, TAS, Australia, 29 November–2 December 2016; ACM Press: New York, NY, USA, 2016; pp. 348–352. [Google Scholar]
- Garavand, A.; Samadbeik, M.; Kafashi, M.; Abhari, S. Acceptance of Health Information Technologies, Acceptance of Mobile Health: A Review Article. J. Biomed. Phys. Eng. 2017, 7, 403–408. [Google Scholar] [PubMed]
- Nadal, C.; Sas, C.; Doherty, G. Technology Acceptance in Mobile Health: Scoping Review of Definitions, Models, and Measurement. J. Med. Internet Res. 2020, 22, e17256. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.R.; De Schutter, B.; Franks, K.; Radina, M.E. Older Adults’ Experiences with Audiovisual Virtual Reality: Perceived Usefulness and Other Factors Influencing Technology Acceptance. Clin. Gerontol. 2019, 42, 27–33. [Google Scholar] [CrossRef]
- Mahalil, I.; Yusof, A.M.; Ibrahim, N. A Literature Review on the Usage of Technology Acceptance Model for Analysing a Virtual Reality’s Cycling Sport Applications with Enhanced Realism Fidelity. In Proceedings of the 2020 8th International Conference on Information Technology and Multimedia (ICIMU), Selangor, Malaysia, 24–25 August 2020; pp. 237–242. [Google Scholar]
- Wilson, C.; Hargreaves, T.; Hauxwell-Baldwin, R. Smart Homes and Their Users: A Systematic Analysis and Key Challenges. Pers. Ubiquitous Comput. 2015, 19, 463–476. [Google Scholar] [CrossRef]
- Spoladore, D.; Arlati, S.; Colombo, V.; Modoni, G.; Sacco, M. A Semantic-Enabled Smart Home for AAL and Continuity of Care. In Studies in Computational Intelligence; Springer: Berlin/Heidelberg, Germany, 2021; Volume 933. [Google Scholar]
- Tanabe, S.; Saitoh, E.; Koyama, S.; Kiyono, K.; Tatemoto, T.; Kumazawa, N.; Kagaya, H.; Otaka, Y.; Mukaino, M.; Tsuzuki, A.; et al. Designing a Robotic Smart Home for Everyone, Especially the Elderly and People with Disabilities. Fujita Med. J. 2019, 5, 31–35. [Google Scholar] [CrossRef]
- Dafferianto Trinugroto, Y.B.; Reichert, F.; Fensli, R.W. A SOA-Based Health Service Platform in Smart Home Environment. In Proceedings of the 2011 IEEE 13th International Conference on e-Health Networking, Applications and Services, Columbia, MO, USA, 13–15 June 2011; pp. 201–204. [Google Scholar]
- Knaup, P.; Schöpe, L. Using Data from Ambient Assisted Living and Smart Homes in Electronic Health Records. Methods Inf. Med. 2014, 53, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.S.; Halooq, A.; Dening, J.; Uddin, R.; Laranjo, L.; Chow, C.K.; Maddison, R. Healthcare Providers’ Perspectives on Using Smart Home Systems to Improve Self-Management and Care in People with Heart Failure: A Qualitative Study. Int. J. Med. Inform. 2022, 167, 104837. [Google Scholar] [CrossRef] [PubMed]
- Baldassini, D.; Colombo, V.; Spoladore, D.; Sacco, M.; Arlati, S. Customization of Domestic Environment and Physical Training Supported by Virtual Reality and Semantic Technologies: A Use-Case. In Proceedings of the RTSI 2017—IEEE 3rd International Forum on Research and Technologies for Society and Industry, Modena, Italy, 11–13 September 2017. [Google Scholar]
- Spoladore, D.; Mahroo, A.; Trombetta, A.; Sacco, M. Comfont: A Semantic Framework for Indoor Comfort and Energy Saving in Smart Homes. Electronics 2019, 8, 1449. [Google Scholar] [CrossRef]
- Nolich, M.; Spoladore, D.; Carciotti, S.; Buqi, R.; Sacco, M. Cabin as a Home: A Novel Comfort Optimization Framework for IoT Equipped Smart Environments and Applications on Cruise Ships. Sensors 2019, 19, 1060. [Google Scholar] [CrossRef]
- Tsirlin, I.; Dupierrix, E.; Chokron, S.; Coquillart, S.; Ohlmann, T. Uses of Virtual Reality for Diagnosis, Rehabilitation and Study of Unilateral Spatial Neglect: Review and Analysis. CyberPsychology Behav. 2009, 12, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Tan, W.; Chen, C.; Liu, C.; Yang, J.; Zhang, Y. A Review of the Application of Virtual Reality Technology in the Diagnosis and Treatment of Cognitive Impairment. Front. Aging Neurosci. 2019, 11, 280. [Google Scholar] [CrossRef] [PubMed]
- Muthu, B.; Sivaparthipan, C.B.; Manogaran, G.; Sundarasekar, R.; Kadry, S.; Shanthini, A.; Dasel, A. IOT Based Wearable Sensor for Diseases Prediction and Symptom Analysis in Healthcare Sector. Peer Peer Netw. Appl. 2020, 13, 2123–2134. [Google Scholar] [CrossRef]
- Pavitra, B.; Singh, D.N.; Sharma, S.K. Predictive and Interactive IOT Diagnosis System with AI and ML Tools: Review. In Advances in Computational Intelligence and Informatics; Springer: Berlin/Heidelberg, Germany, 2020; pp. 9–16. [Google Scholar]
- Awotunde, J.B.; Folorunso, S.O.; Bhoi, A.K.; Adebayo, P.O.; Ijaz, M.F. Disease Diagnosis System for IoT-Based Wearable Body Sensors with Machine Learning Algorithm. In Hybrid Artificial Intelligence and IoT in Healthcare; Springer: Berlin/Heidelberg, Germany, 2021; pp. 201–222. [Google Scholar]
- Halpern, N.A. Innovative Designs for the Smart ICU. Chest 2014, 145, 646–658. [Google Scholar] [CrossRef]
- Fornara, F.; Bonaiuto, M.; Bonnes, M. Perceived Hospital Environment Quality Indicators: A Study of Orthopaedic Units. J. Environ. Psychol. 2006, 26, 321–334. [Google Scholar] [CrossRef]
- Becker, F.; Sweeney, B.; Parsons, K. Ambulatory Facility Design and Patients’ Perceptions of Healthcare Quality. HERD Health Environ. Res. Des. J. 2008, 1, 35–54. [Google Scholar] [CrossRef]
- Ehret, S.; Trukenbrod, A.K.; Thomaschke, R. Dynamics of Temporal Experience in Active and Passive Waiting Situations. Appl. Cogn. Psychol. 2021, 35, 900–908. [Google Scholar] [CrossRef]
- Jokic, T.; Zakay, D.; Wittmann, M. Individual Differences in Self-Rated Impulsivity Modulate the Estimation of Time in a Real Waiting Situation. Timing Time Percept. 2018, 6, 71–89. [Google Scholar] [CrossRef]
- Cohen, S.; Evans, G.W.; Stokols, D.; Krantz, D.S. Behavior, Health, and Environmental Stress; Springer: Boston, MA, USA, 1986; ISBN 978-1-4757-9382-6. [Google Scholar]
- Evans, G.W.; McCoy, J.M. When Buildings Don’t Work: The Role of Architecture In Human Health. J. Environ. Psychol. 1998, 18, 85–94. [Google Scholar] [CrossRef]
- Juliá-Nehme, B.; Yoon, S.-Y.; Cumsille, P.; Rodríguez, E. Assessing Spatial User Experience for Design Guidelines: A Comparative Study of Outpatient Waiting Rooms with Conventional versus Modern Features. HERD Health Environ. Res. Des. J. 2023, 16, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Del Nord, R.; Peretti, G. L’umanizzazione Degli Spazi Cura; 2012; Available online: https://www.dors.it/documentazione/testo/201904/Umanizzazione_degli_spazi_di_cura_LG.pdf (accessed on 12 December 2023).
- National Health Service—England. Health Building Note 11-01: Facilities for Primary and Community Care Services; National Health Service: London, UK, 2013.
- Arakawa Martins, B.; Barrie, H.; Visvanathan, R.; Daniel, L.; Martins, L.A.; Ranasinghe, D.; Wilson, A.; Soebarto, V. A Multidisciplinary Exploratory Approach for Investigating the Experience of Older Adults Attending Hospital Services. HERD Health Environ. Res. Des. J. 2021, 14, 141–163. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress Recovery during Exposure to Natural and Urban Environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Pouyesh, V.; Amaniyan, S.; Haji Mohammad Hoseini, M.; Bashiri, Y.; Sieloff, C.; Griffiths, P.; Vaismoradi, M. The Effects of Environmental Factors in Waiting Rooms on Anxiety among Patients Undergoing Coronary Angiography: A Randomized Controlled Trial. Int. J. Nurs. Pract. 2018, 24, 12682. [Google Scholar] [CrossRef]
- Dijkstra, K.; Pieterse, M.; Pruyn, A. Physical Environmental Stimuli That Turn Healthcare Facilities into Healing Environments through Psychologically Mediated Effects: Systematic Review. J. Adv. Nurs. 2006, 56, 166–181. [Google Scholar] [CrossRef]
- Sarkamo, T.; Tervaniemi, M.; Laitinen, S.; Forsblom, A.; Soinila, S.; Mikkonen, M.; Autti, T.; Silvennoinen, H.M.; Erkkila, J.; Laine, M.; et al. Music Listening Enhances Cognitive Recovery and Mood after Middle Cerebral Artery Stroke. Brain 2008, 131, 866–876. [Google Scholar] [CrossRef]
- Selle, E.W.; Silverman, M.J. A Randomized Feasibility Study on the Effects of Music Therapy in the Form of Patient-Preferred Live Music on Mood and Pain in Patients on a Cardiovascular Unit. Arts Health 2017, 9, 213–223. [Google Scholar] [CrossRef]
- Jespersen, K.V.; Koenig, J.; Jennum, P.; Vuust, P. Music for Insomnia in Adults. Cochrane Database Syst. Rev. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.; Fitzpatrick, K.; Kiernan, A.M.; Moss, H.; Harmon, D. Pilot Study on Music in the Waiting Room of Outpatient Pain Clinics. Pain Manag. Nurs. 2022, 23, 318–323. [Google Scholar] [CrossRef]
- Cavanagh, B.; Haracz, K.; Lawry, M.; James, C. Receptive Arts Engagement for Health: A Holistic and Trans-Disciplinary Approach to Creating a Multisensory Environment. Sage Open 2020, 10, 215824402097842. [Google Scholar] [CrossRef]
- Golinowska, S.; Groot, W.; Baji, P.; Pavlova, M. Health Promotion Targeting Older People. BMC Health Serv. Res. 2016, 16, 345. [Google Scholar] [CrossRef] [PubMed]
- Gruber, T.R. A Translation Approach to Portable Ontology Specifications. Knowl. Acquis. 1993, 5, 199–220. [Google Scholar] [CrossRef]
- Baader, F.; Horrocks, I.; Sattler, U. Description Logics as Ontology Languages for the Semantic Web. In Mechanizing Mathematical Reasoning; Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar] [CrossRef]
- Bienvenu, M.; Leclère, M.; Mugnier, M.-L.; Rousset, M.-C. Reasoning with Ontologies. In A Guided Tour of Artificial Intelligence Research; Springer: Cham, Switzerland, 2020; pp. 185–215. [Google Scholar]
- Shoaip, N.; El-Sappagh, S.; Barakat, S.; Elmogy, M. Reasoning Methodologies in Clinical Decision Support Systems: A Literature Review. In U-Healthcare Monitoring Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 61–87. [Google Scholar]
- Dissanayake, P.I.; Colicchio, T.K.; Cimino, J.J. Using Clinical Reasoning Ontologies to Make Smarter Clinical Decision Support Systems: A Systematic Review and Data Synthesis. J. Am. Med. Inform. Assoc. 2020, 27, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Legaz-García, M.d.C.; Martínez-Costa, C.; Menárguez-Tortosa, M.; Fernández-Breis, J.T. A Semantic Web Based Framework for the Interoperability and Exploitation of Clinical Models and EHR Data. Knowl.-Based Syst. 2016, 105, 175–189. [Google Scholar] [CrossRef]
- Adel, E.; El-Sappagh, S.; Barakat, S.; Elmogy, M. Ontology-Based Electronic Health Record Semantic Interoperability: A Survey. In U-Healthcare Monitoring Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 315–352. [Google Scholar]
- Agenzia per l’Italia Digitale Digital Healthcare System. Available online: https://www.agid.gov.it/en/piattaforme/digital-healthcare-system (accessed on 12 December 2023).
- Stucki, G.; Cieza, A.; Ewert, T.; Kostanjsek, N.; Chatterji, S.; Üstün, T.B. Application of the International Classification of Functioning, Disability and Health (ICF) in Clinical Practice. Disabil. Rehabil. 2002, 24, 281–282. [Google Scholar] [CrossRef]
- DiSantostefano, J. International Classification of Diseases 10th Revision (ICD-10). J. Nurse Pract. 2009, 5, 56–57. [Google Scholar] [CrossRef]
- Spoladore, D.; Sacco, M.; Trombetta, A. A Review of Domain Ontologies for Disability Representation. Expert. Syst. Appl. 2023, 228, 120467. [Google Scholar] [CrossRef]
- Spoladore, D.; Mondellini, M.; Sacco, M.; Spoladore, D.; Trombetta, A. An Ontology-Based Framework for a Less Invasive Domestic Management System (LIDoMS). In Proceedings of the 2020 16th International Conference on Intelligent Environments, Madrid, Spain, 20–23 July 2020. IE 2020. [Google Scholar]
- Spoladore, D.; Arlati, S.; Carciotti, S.; Nolich, M.; Sacco, M. RoomFort: An Ontology-Based Comfort Management Application for Hotels. Electronics 2018, 7, 345. [Google Scholar] [CrossRef]
- Pan, J.Z. Resource Description Framework. In Handbook on Ontologies; Springer: Berlin/Heidelberg, Germany, 2009; pp. 71–90. [Google Scholar]
- Antoniou, G.; Harmelen, F. van Web Ontology Language: OWL. In Handbook on Ontologies; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Horrocks, I.; Patel-Schneider, P.F.; Boley, H.; Tabet, S.; Grosof, B.; Dean, M. SWRL: A Semantic Web Rule Language Combining OWL and RuleML. W3C Memb. Submiss. 2004, 21, 1–31. [Google Scholar]
- Barsocchi, P.; Ferro, E.; La Rosa, D.; Mahroo, A.; Spoladore, D. E-Cabin: A Software Architecture for Passenger Comfort and Cruise Ship Management. Sensors 2019, 19, 4978. [Google Scholar] [CrossRef] [PubMed]
- Spoladore, D.; Mahroo, A.; Trombetta, A.; Sacco, M. DOMUS: A Domestic Ontology Managed Ubiquitous System. J. Ambient. Intell. Humaniz. Comput. 2022, 13, 3037–3052. [Google Scholar] [CrossRef]
- Hommeaux, E.P.; Seaborne, A. SPARQL Query Language for RDF. W3C Recommendation. 2008. Available online: http://www.w3.org/TR/rdf-sparql-query/ (accessed on 12 December 2023).
- U.S. Food & Drug Administration. Patient-Focused Drug Development: Collecting Comprehensive and Representative Input. 2020. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-focused-drug-development-collecting-comprehensive-and-representative-input (accessed on 12 December 2023).
- Piau, A.; Wild, K.; Mattek, N.; Kaye, J. Current State of Digital Biomarker Technologies for Real-Life, Home-Based Monitoring of Cognitive Function for Mild Cognitive Impairment to Mild Alzheimer Disease and Implications for Clinical Care: Systematic Review. J. Med. Internet Res. 2019, 21, e12785. [Google Scholar] [CrossRef]
- Vasudevan, S.; Saha, A.; Tarver, M.E.; Patel, B. Digital Biomarkers: Convergence of Digital Health Technologies and Biomarkers. NPJ Digit. Med. 2022, 5, 36. [Google Scholar] [CrossRef]
- Cavedoni, S.; Chirico, A.; Pedroli, E.; Cipresso, P.; Riva, G. Digital Biomarkers for the Early Detection of Mild Cognitive Impairment: Artificial Intelligence Meets Virtual Reality. Front. Hum. Neurosci. 2020, 14, 245. [Google Scholar] [CrossRef]
- Ding, Z.; Lee, T.; Chan, A.S. Digital Cognitive Biomarker for Mild Cognitive Impairments and Dementia: A Systematic Review. J. Clin. Med. 2022, 11, 4191. [Google Scholar] [CrossRef]
- Ansart, M.; Epelbaum, S.; Bassignana, G.; Bône, A.; Bottani, S.; Cattai, T.; Couronné, R.; Faouzi, J.; Koval, I.; Louis, M.; et al. Predicting the Progression of Mild Cognitive Impairment Using Machine Learning: A Systematic, Quantitative and Critical Review. Med. Image Anal. 2021, 67, 101848. [Google Scholar] [CrossRef]
- Tsai, C.-F.; Chen, C.-C.; Wu, E.H.-K.; Chung, C.-R.; Huang, C.-Y.; Tsai, P.-Y.; Yeh, S.-C. A Machine-Learning-Based Assessment Method for Early-Stage Neurocognitive Impairment by an Immersive Virtual Supermarket. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 2124–2132. [Google Scholar] [CrossRef]
- Wang, S.; Yin, H.; Li, G.; Jia, Y.; Leng, M.; Meng, Q.; Wang, C.; Chen, L. Detection of Mild Cognitive Impairment Based on Virtual Reality: A Scoping Review. Curr. Alzheimer Res. 2020, 17, 126–140. [Google Scholar] [CrossRef] [PubMed]
- de los Reyes-Guzmán, A.; Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; Monasterio-Huelin, F.; Torricelli, D.; Gil-Agudo, A. Quantitative Assessment Based on Kinematic Measures of Functional Impairments during Upper Extremity Movements: A Review. Clin. Biomech. 2014, 29, 719–727. [Google Scholar] [CrossRef]
- Cooper, C.; Li, R.; Lyketsos, C.; Livingston, G. Treatment for Mild Cognitive Impairment: Systematic Review. Br. J. Psychiatry 2013, 203, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Zhu, H. Hyper-Parameter Optimization: A Review of Algorithms and Applications. arXiv 2020, arXiv:2003.05689. [Google Scholar]
- Castegnaro, A.; Howett, D.; Li, A.; Harding, E.; Chan, D.; Burgess, N.; King, J. Assessing Mild Cognitive Impairment Using Object-Location Memory in Immersive Virtual Environments. Hippocampus 2022, 32, 660–678. [Google Scholar] [CrossRef] [PubMed]
- Adlin, T.; Pruitt, J. The Essential Persona Lifecycle: Your Guide to Building and Using Personas; Elsevier: Amsterdam, The Netherlands, 2010; ISBN 9780123814180. [Google Scholar]
- Cieza, A.; Stucki, A.; Geyh, S.; Berteanu, M.; Quittan, M.; Simon, A.; Kostanjsek, N.; Stucki, G.; Walsh, N. ICF Core Sets for Chronic Ischaemic Heart Disease. J. Rehabil. Med. 2004, 36, 94–99. [Google Scholar] [CrossRef]
- Jung, C.-C.; Hsia, Y.-F.; Hsu, N.-Y.; Wang, Y.-C.; Su, H.-J. Cumulative Effect of Indoor Temperature on Cardiovascular Disease–Related Emergency Department Visits among Older Adults in Taiwan. Sci. Total Environ. 2020, 731, 138958. [Google Scholar] [CrossRef]
- Higuma, T.; Yoneyama, K.; Nakai, M.; Kaihara, T.; Sumita, Y.; Watanabe, M.; Doi, S.; Miyamoto, Y.; Yasuda, S.; Ishibashi, Y.; et al. Effects of Temperature and Humidity on Acute Myocardial Infarction Hospitalization in a Super-Aging Society. Sci. Rep. 2021, 11, 22832. [Google Scholar] [CrossRef]
- Janssen, H.; Ford, K.; Gascoyne, B.; Hill, R.; Roberts, M.; Bellis, M.A.; Azam, S. Cold Indoor Temperatures and Their Association with Health and Well-Being: A Systematic Literature Review. Public Health 2023, 224, 185–194. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità Malattie Cardiovascolari—Online. Available online: https://www.epicentro.iss.it/cardiovascolare/ (accessed on 10 January 2024).
- Eurostat Cardiovascular Diseases Statistics—Online. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=cardiovascular_diseases_statistics (accessed on 10 January 2024).
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef]
- Cimler, R.; Maresova, P.; Kuhnova, J.; Kuca, K. Predictions of Alzheimer’s Disease Treatment and Care Costs in European Countries. PLoS ONE 2019, 14, e0210958. [Google Scholar] [CrossRef]
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing Populations: The Challenges Ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Bonacina, S.; Marceglia, S.; Pinciroli, F. Barriers Against Adoption of Electronic Health Record in Italy. J. Healthc. Eng. 2011, 2, 509–526. [Google Scholar] [CrossRef]
- Nalin, M.; Baroni, I.; Faiella, G.; Romano, M.; Matrisciano, F.; Gelenbe, E.; Martinez, D.M.; Dumortier, J.; Natsiavas, P.; Votis, K.; et al. The European Cross-Border Health Data Exchange Roadmap: Case Study in the Italian Setting. J. Biomed. Inform. 2019, 94, 103183. [Google Scholar] [CrossRef]
- Rouhani, S.; Deters, R. Security, Performance, and Applications of Smart Contracts: A Systematic Survey. IEEE Access 2019, 7, 50759–50779. [Google Scholar] [CrossRef]
- Tawalbeh, L.; Muheidat, F.; Tawalbeh, M.; Quwaider, M. IoT Privacy and Security: Challenges and Solutions. Appl. Sci. 2020, 10, 4102. [Google Scholar] [CrossRef]
- Grafenstein, M.; Heumüller, J.; Belgacem, E.; Jakobi, T.; Smiesko, P. Effective Regulation through Design—Aligning the EPrivacy Regulation with the EU General Data Protection Regulation (GDPR): Tracking Technologies in Personalised Internet Content and the Data Protection by Design Approach. SSRN Electron. J. 2021. [Google Scholar] [CrossRef]
- Demiris, G.; Hensel, B.K.; Skubic, M.; Rantz, M. Senior Residents’ Perceived Need of and Preferences for “Smart Home” Sensor Technologies. Int. J. Technol. Assess. Health Care 2008, 24, 120–124. [Google Scholar] [CrossRef]
- Balta-Ozkan, N.; Davidson, R.; Bicket, M.; Whitmarsh, L. Social Barriers to the Adoption of Smart Homes. Energy Policy 2013, 63, 363–374. [Google Scholar] [CrossRef]
- Zakerabasali, S.; Ayyoubzadeh, S.M. Internet of Things and Healthcare System: A Systematic Review of Ethical Issues. Health Sci. Rep. 2022, 5, e863. [Google Scholar] [CrossRef]
- van Ginneken, E.; Reed, S.; Siciliani, L.; Eriksen, A.; Schlepper, L.; Tille, F.; Zapata, T. Addressing Backlogs and Managing Waiting Lists during and beyond the COVID-19 Pandemic; European Observatory on Health Systems and Policies: Brussels, Belgium, 2022.


{kind=link}
{kind=link}
{kind=link}
| Continent | Country | Number of Unique Authors |
|---|---|---|
| Africa | Rwanda | 3 |
| Malawi | 1 | |
| Asia | India | 1 |
| Syria | 6 | |
| Europe | Denmark | 6 |
| Germany | 3 | |
| Switzerland | 6 | |
| The Netherlands | 8 | |
| UK | 1 | |
| North America | Canada | 5 |
| USA | 47 | |
| Oceania | Australia | 7 |
| Cluster | Reference | Brief Description |
|---|---|---|
| A | [22] | To increase patient satisfaction and processes’ efficiency in an outpatient surgery clinic, RFID tags worn by patients and clinical staff are adopted to map real-time location data; collected data aim to reduce patients’ waiting time while optimizing care delivery processes. |
| [23] | To increase women’s knowledge about long-acting reversible contraceptive methods, an app is developed to enhance clinic counseling during waiting times. | |
| [24] | Using discrete event simulation, the bottlenecks of a campus healthcare outpatient clinic are identified and addressed with the aim of reducing patients’ waiting time. | |
| [20] | To control overcrowding and long waiting times in health centers, a machine learning prediction model is developed to forecast patient loads; demand excess is transferred to other clinics via an IoT smart bus system | |
| [25] | Patients waiting for chemotherapy were provided with instructional videos related to acupressure and meditation or an integrative oncology lecture to reduce their levels of anxiety before the therapy. | |
| [26] | Virtual reality (VR) eyeglasses are adopted to alleviate preoperative anxiety levels in pediatric patients in a dental waiting room. | |
| [27] | Patients with low-severity conditions can wait outside an emergency department waiting room and monitor the progression of their waiting with a smart system, which eventually warns them of their visit via SMS. | |
| [28] | This solution aims at reducing preoperative anxiety using an informative 360-degree VR video for women visiting a one-stop clinic for abnormal uterine bleeding. | |
| [29] | A multisensory VR game is developed to reduce anxiety and stress levels in hospital waiting rooms, leveraging a full-immersion environment. | |
| B | [30] | A system for measuring women’s blood pressure in an obstetric waiting room; the data acquired are sent to the clinical personnel for the subsequent visit via a web-based clinical decision support system. |
| [31] | Patient-reported outcomes (PROs) in rheumatic patients are self-assessed via mobile technology; the results of the self-assessment are sent to the rheumatologist as an Electronic Medical Record (EMR) as part of the clinical assessment for the visit. | |
| C | [32] | Taking into account the increase in waiting time in any clinical setting, this solution proposes a non-invasive system aimed at assessing vital signs (oxygen saturation, blood pressure, heart rate, breath rate, temperature, resting potential, or retina) that may be of possible use for a diagnostic process. |
| [33] | Considering the limited time during visits, a digital tool to be used during the waiting time is presented to support patients in the identification of their top priorities for their visit. | |
| [21] | An AI-based system to support patients in assessing their symptoms during waiting times based on their basic health information and most troubling current symptoms. | |
| [34] | A smart atrial fibrillation station is to be deployed in medical waiting rooms to support the self-screening of strokes in patients older than 64. | |
| [35] | A smart waiting room for Parkinson’s disease patients aimed at assessing their motor and non-motor function (manual dexterity, walking speed, information processing, visual memory, quality of life); acquired data are stored in the patient’s Electronic Health Record (EHR). |
| Reference | Year | Patient Type | Health Condition |
|---|---|---|---|
| [32] | 2009 | General | - |
| [22] | 2013 | General | - |
| [23] | 2014 | Women | Fertility |
| [30] | 2014 | Women | Diabetes and pregnancy |
| [24] | 2017 | General | - |
| [20] | 2019 | General | - |
| [25] | 2019 | General | Chemotherapy |
| [33] | 2019 | General | Chronic conditions |
| [31] | 2020 | General | Rheumatoid arthritis |
| [21] | 2020 | General | - |
| [26] | 2020 | Pediatric | Dental surgery |
| [27] | 2022 | General | - |
| [28] | 2022 | Women | Abnormal uterine bleeding |
| [34] | 2023 | 65+ aged patients | - |
| [35] | 2023 | General | Parkinson disease |
| [29] | 2023 | General | - |
| Reference | Year | Technology (Broad Term/Narrow Term) | |||
|---|---|---|---|---|---|
| [32] | 2009 | Biomedical measurement/Photoplethysmography | CMOS technology/Microcontroller | Electrooculography/Electro-oculography | Algorithms/Software |
| [22] | 2013 | RFID tags/Active RFID tags | Digital simulation/Discrete event simulation | - | - |
| [23] | 2014 | Computer applications/Mobile application | - | - | - |
| [30] | 2014 | Knowledge representation/Ontologies | Biomedical equipment/Pulse oximeter | Activity recognition/sensor systems | 3G mobile communication |
| [24] | 2017 | Digital simulation/Discrete event simulation | - | - | - |
| [20] | 2019 | Algorithms/Machine learning | Cloud computing/Internet of Things | Algorithms/Prediction algorithms | - |
| [25] | 2019 | Computer applications/Mobile application | - | - | - |
| [33] | 2019 | Computer applications/Mobile application | Artificial intelligence/Decision support systems | - | - |
| [31] | 2020 | Computer applications/Mobile application | Electronic medical records/Electronic health records | - | - |
| [21] | 2020 | Computer applications/Mobile application | Artificial intelligence/Decision support systems | - | - |
| [26] | 2020 | Virtual reality/Immersive experience | - | - | - |
| [27] | 2022 | Cellular technology/GSM | Artificial intelligence/Decision support systems | - | - |
| [28] | 2022 | Virtual reality/Immersive experience | - | - | - |
| [34] | 2023 | Computer applications/Mobile application | Biomedical equipment/Electrocardiography | Electronic medical records/Electronic health records | - |
| [35] | 2023 | Computer applications/Mobile application | Electronic medical records/Electronic health records | Virtual reality/Immersive experience | - |
| [29] | 2023 | Virtual reality/Immersive experience | Ventilation/Fans | - | - |
| Reference | Year | Applicative Context |
|---|---|---|
| [32] | 2009 | Unspecified waiting room |
| [22] | 2013 | Primary care waiting room |
| [23] | 2014 | Specific clinical practice waiting room (family planning) |
| [30] | 2014 | Specific clinical practice waiting room (obstetric) |
| [24] | 2017 | Primary care waiting room |
| [20] | 2019 | Laboratory waiting room (blood testing) |
| [25] | 2019 | Specific clinical practice waiting room (cancer treatment) |
| [33] | 2019 | Primary care waiting room |
| [31] | 2020 | Specific clinical practice waiting room (rheumatic) |
| [21] | 2020 | Primary care waiting room |
| [26] | 2020 | Specific clinical practice waiting room (dental) |
| [27] | 2022 | Emergency room |
| [28] | 2022 | Specific clinical practice waiting room (gynecological) |
| [34] | 2023 | Primary care waiting room |
| [35] | 2023 | Specific clinical practice waiting room (neurologic) |
| [29] | 2023 | Hospital waiting room |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spoladore, D.; Mondellini, M.; Mahroo, A.; Chicchi-Giglioli, I.A.; De Gaspari, S.; Di Lernia, D.; Riva, G.; Bellini, E.; Setola, N.; Sacco, M. Smart Waiting Room: A Systematic Literature Review and a Proposal. Electronics 2024, 13, 388. https://doi.org/10.3390/electronics13020388
Spoladore D, Mondellini M, Mahroo A, Chicchi-Giglioli IA, De Gaspari S, Di Lernia D, Riva G, Bellini E, Setola N, Sacco M. Smart Waiting Room: A Systematic Literature Review and a Proposal. Electronics. 2024; 13(2):388. https://doi.org/10.3390/electronics13020388
Chicago/Turabian StyleSpoladore, Daniele, Marta Mondellini, Atieh Mahroo, Irene Alice Chicchi-Giglioli, Stefano De Gaspari, Daniele Di Lernia, Giuseppe Riva, Elena Bellini, Nicoletta Setola, and Marco Sacco. 2024. "Smart Waiting Room: A Systematic Literature Review and a Proposal" Electronics 13, no. 2: 388. https://doi.org/10.3390/electronics13020388
APA StyleSpoladore, D., Mondellini, M., Mahroo, A., Chicchi-Giglioli, I. A., De Gaspari, S., Di Lernia, D., Riva, G., Bellini, E., Setola, N., & Sacco, M. (2024). Smart Waiting Room: A Systematic Literature Review and a Proposal. Electronics, 13(2), 388. https://doi.org/10.3390/electronics13020388