




AP-NURSE: A Modular Tool to Ease the Life of Patients Suffering from Cognitive Diseases

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
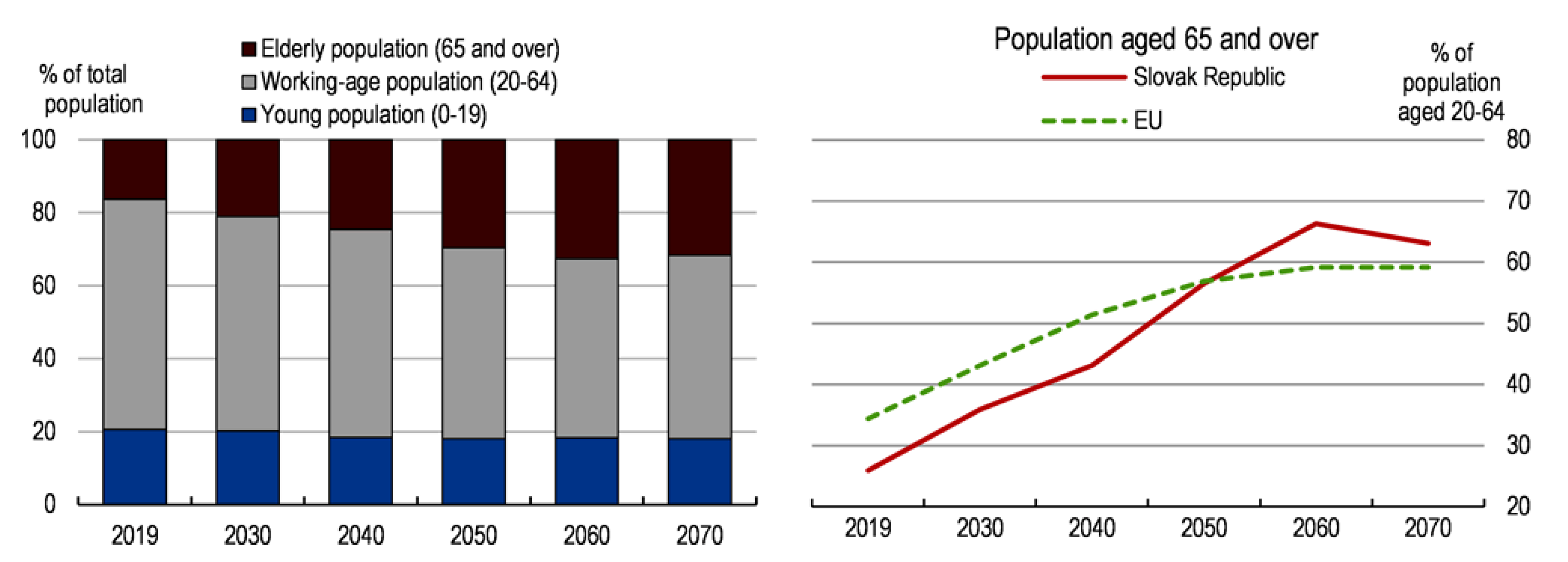
1.1. Aging of the Population
1.2. Action to Be Taken
2. Design of AP-NURSE
2.1. General Design Objectives
2.2. AP-NURSE Versions
2.2.1. AP-NURSE Home
2.2.2. AP-NURSE Care
2.3. AP-NURSE Versions
2.3.1. AP-NURSE Home
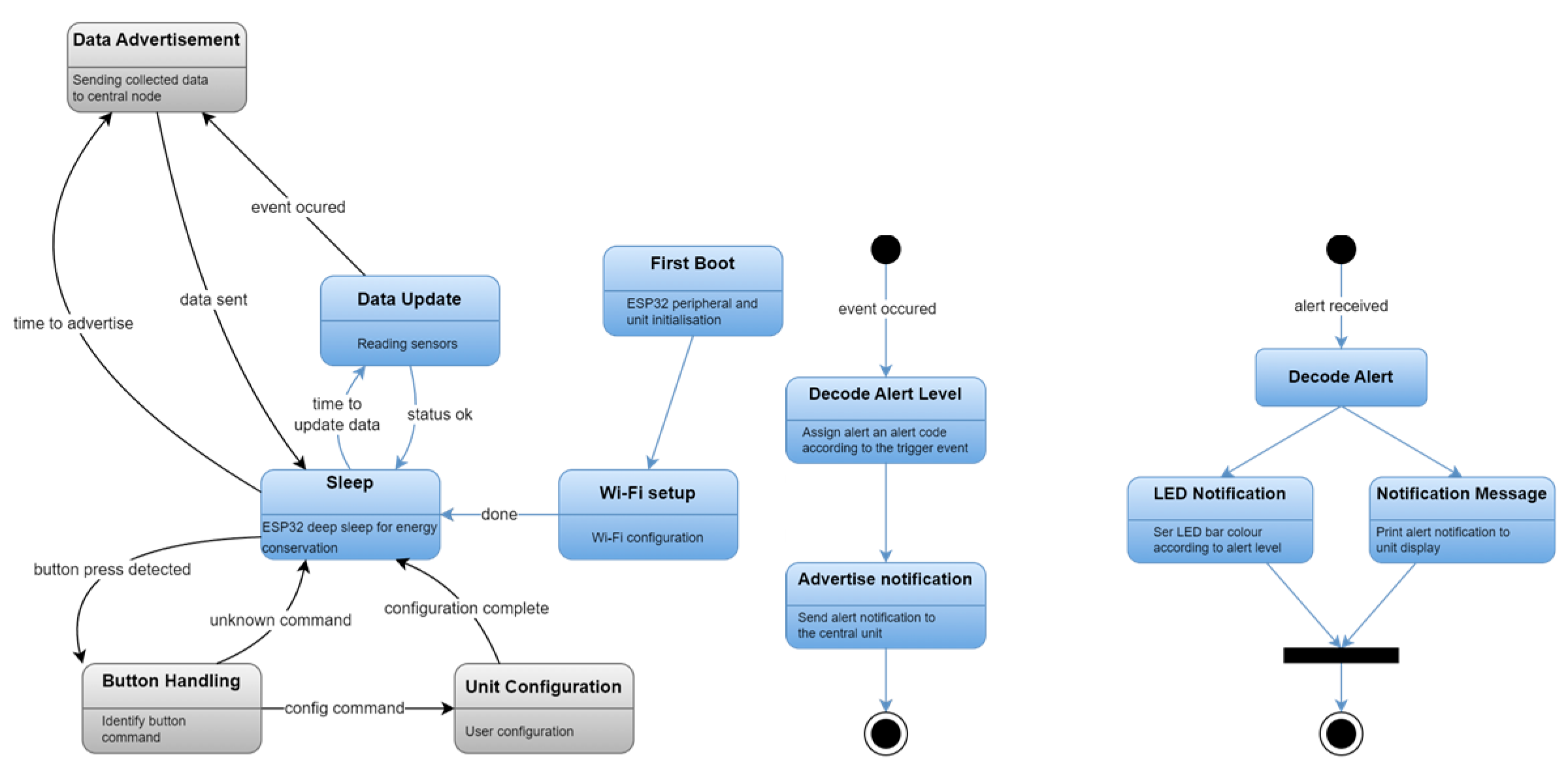
2.3.2. AP-NURSE Care M5stack
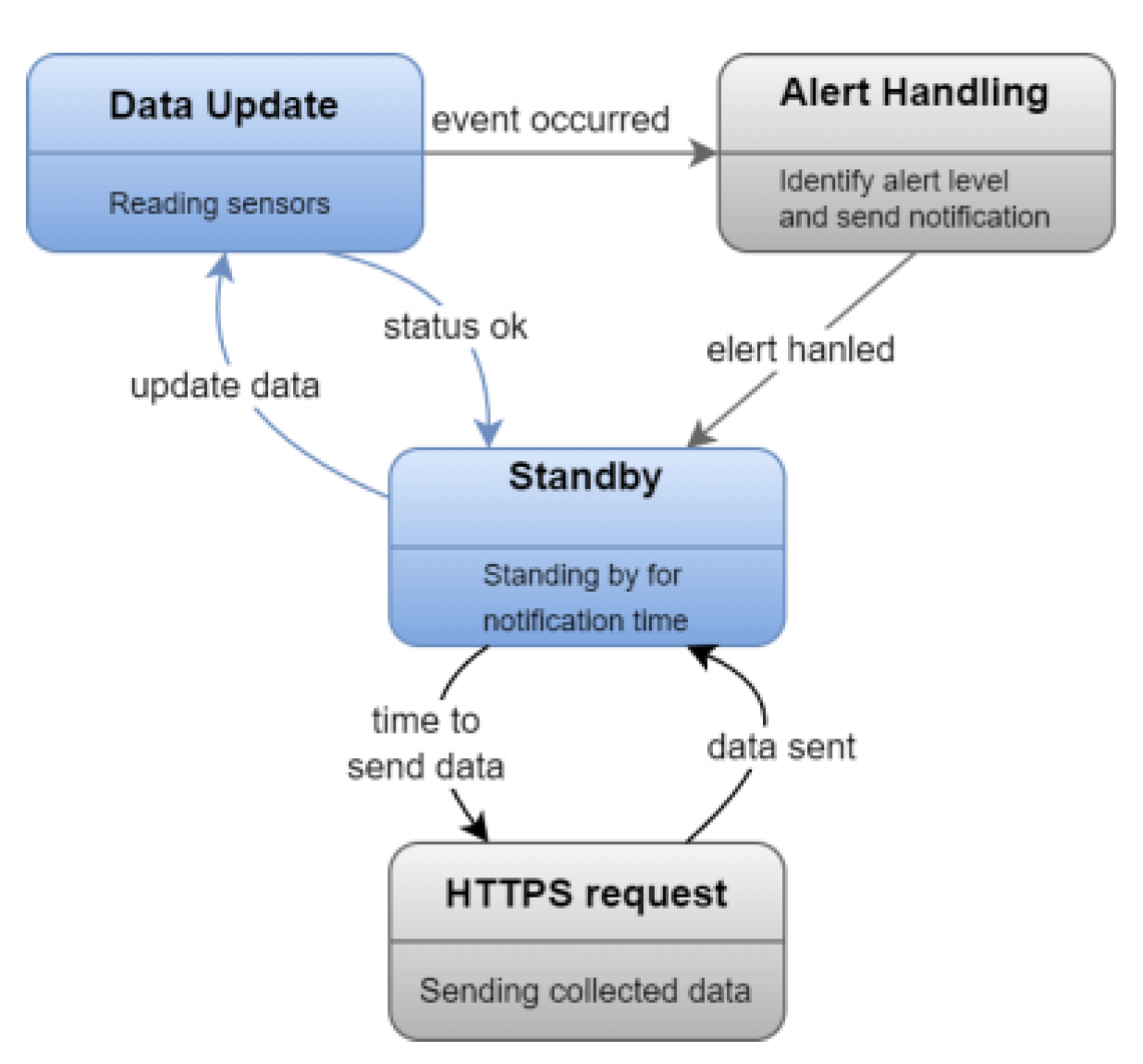
2.3.3. AP-NURSE Care Waspmote
2.4. AP-NURSE Casing
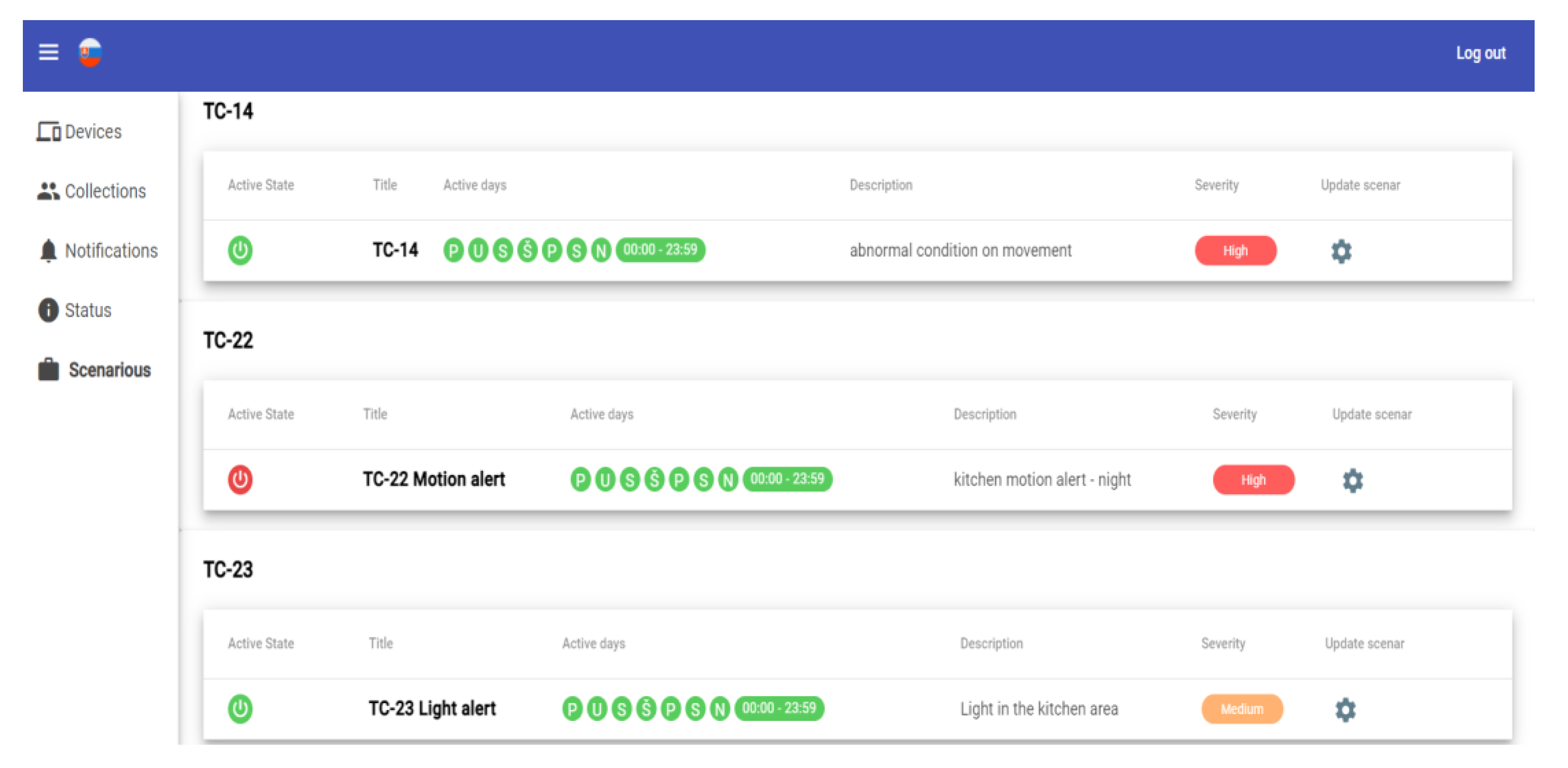
2.5. AP-NURSE Information System
3. Laboratory Testing of AP-NURSE
3.1. Testing Environment
3.2. Testing Procedure
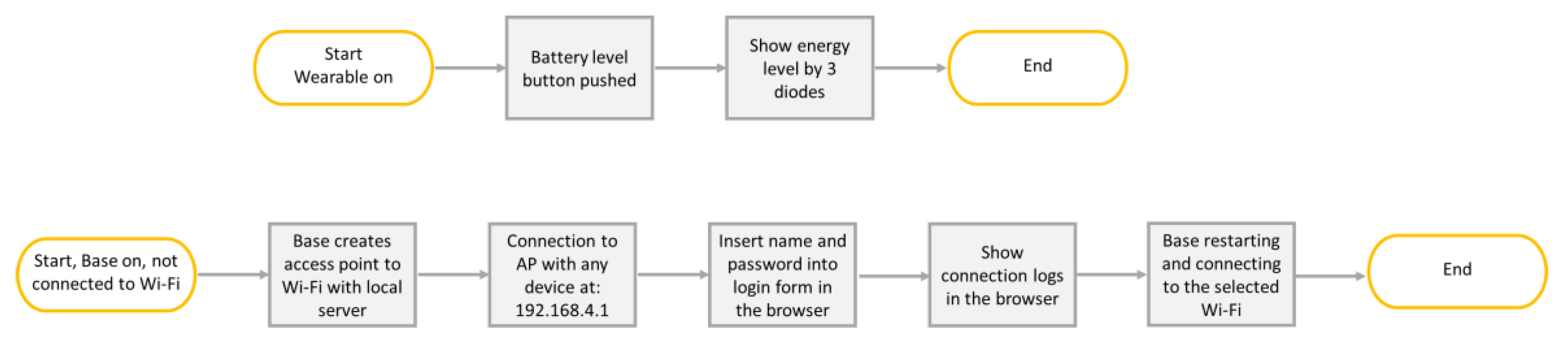
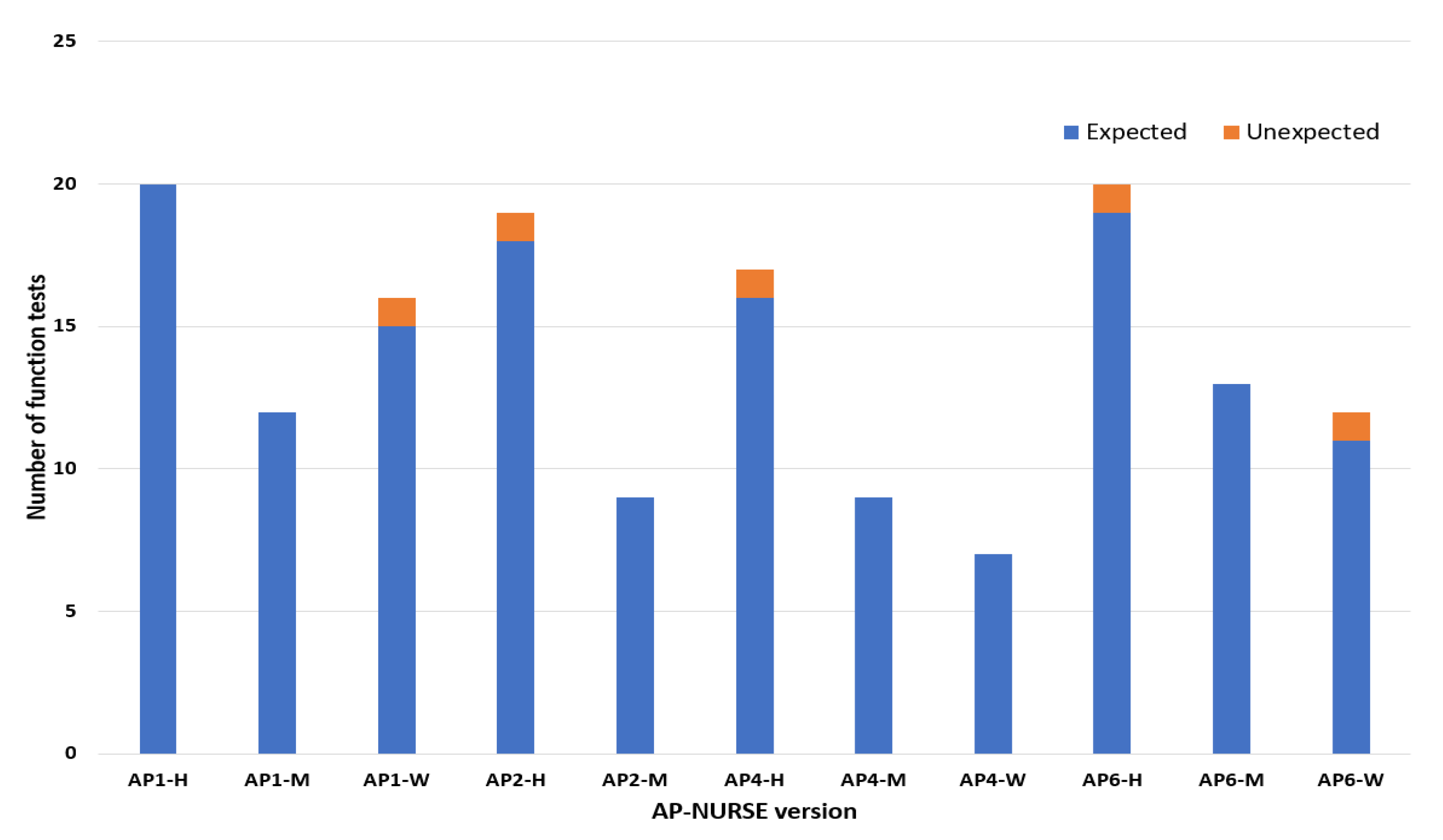
3.2.1. Function Tests
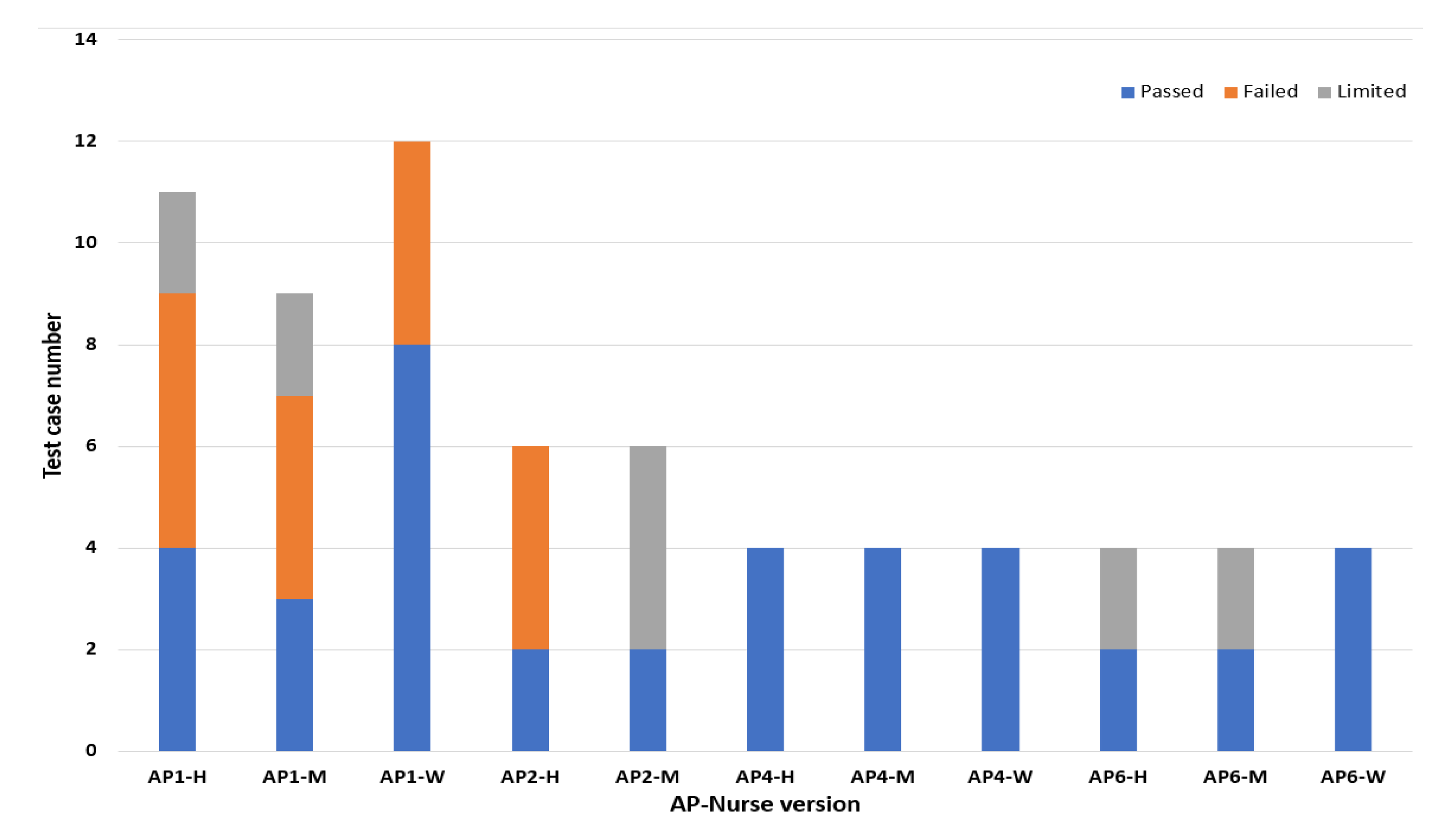
3.2.2. Test Cases
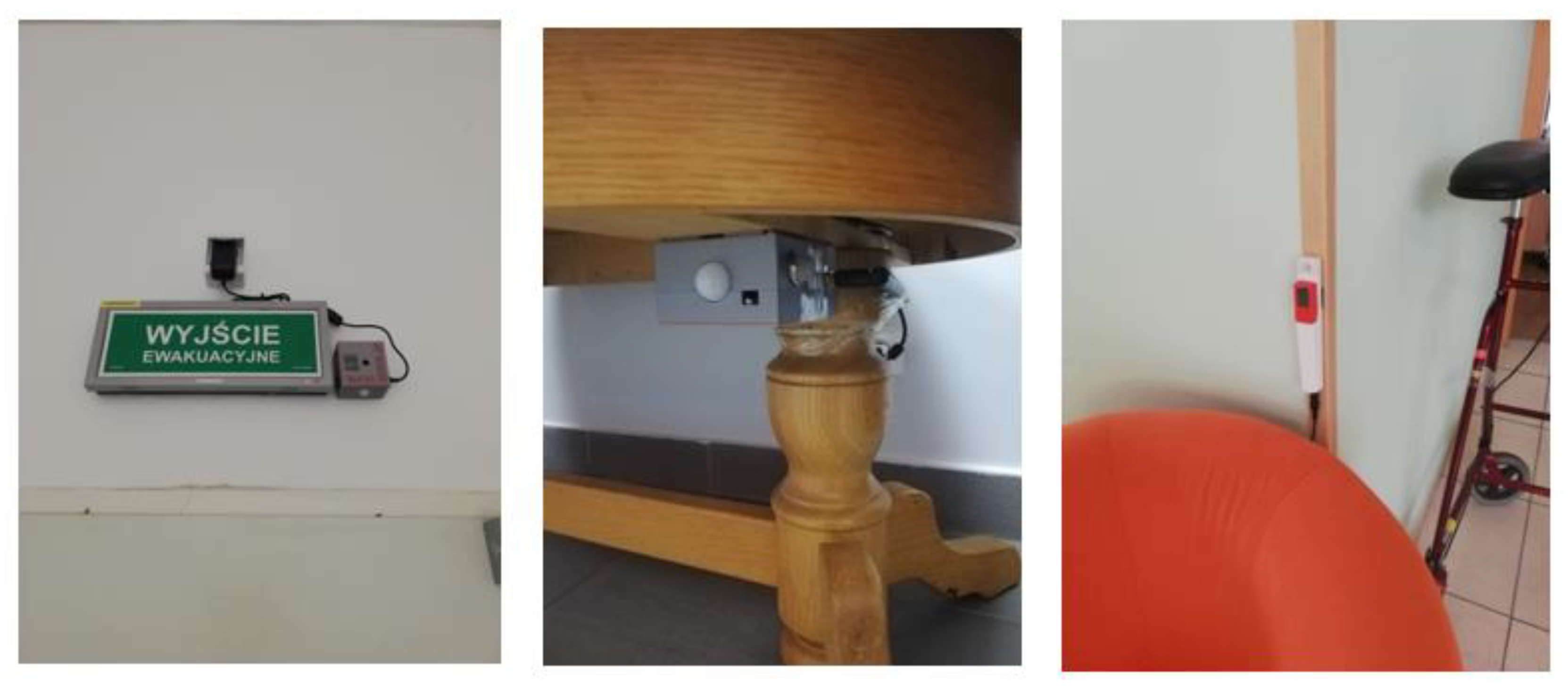
- The location where the AP-NURSE devices are installed (on the wall, under the bed, etc.).
- Type of the patient (mobile/immobile).
- Monitoring regime (day/night).
3.2.3. Sensor Sensitivity Tests
3.3. Testing Results
3.3.1. Function Tests
3.3.2. Test Cases
3.3.3. Sensor Sensitivity Tests
3.4. Finalisation and Prototype Production
4. Testing in Real Environment
4.1. Definition of the Testing Pilots
4.1.1. The Aim of the Pilots
- To install the AP-NURSE smart monitoring tool in two pilot sites and to maintain it in operation as long as possible, but at least two months without interruption.
- To test the information system designed to collect data from AP-NURSE devices.
- Train the selected centres’ personnel to use the information system and the AP-NURSE devices, maintain the nodes in operation, and provide sufficient feedback.
- Collect feedback from the caregivers and the representatives of the centre.
- Based on feedback from caregivers, further improve the system.
- Collect and analyse operational data from the devices.
- Determine whether the system has improved the work of caregivers.
- Identify areas of further development and conditions to be used in the care centre.
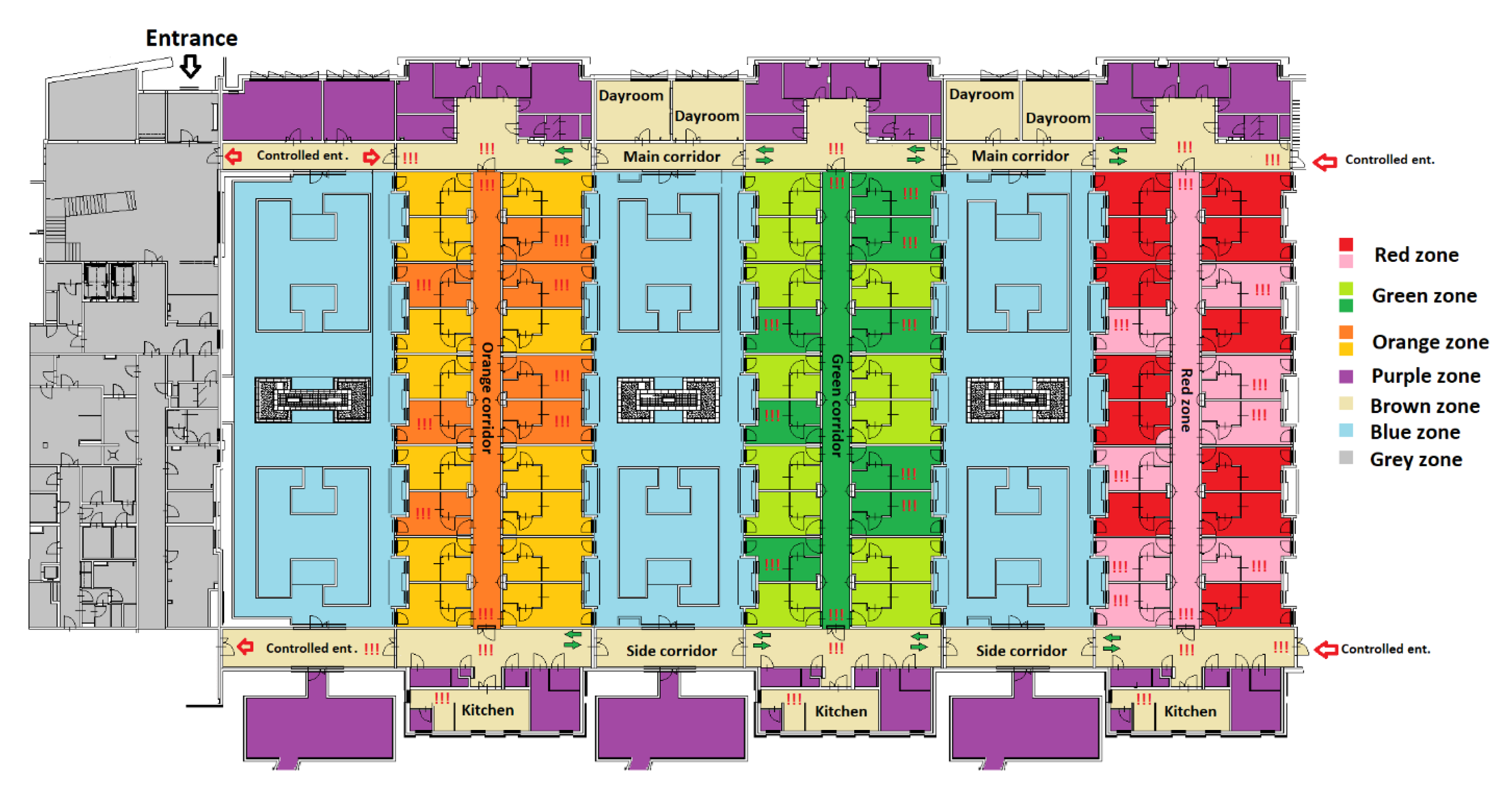
4.1.2. Overview of the Testing Sites
4.1.3. Installation of Devices
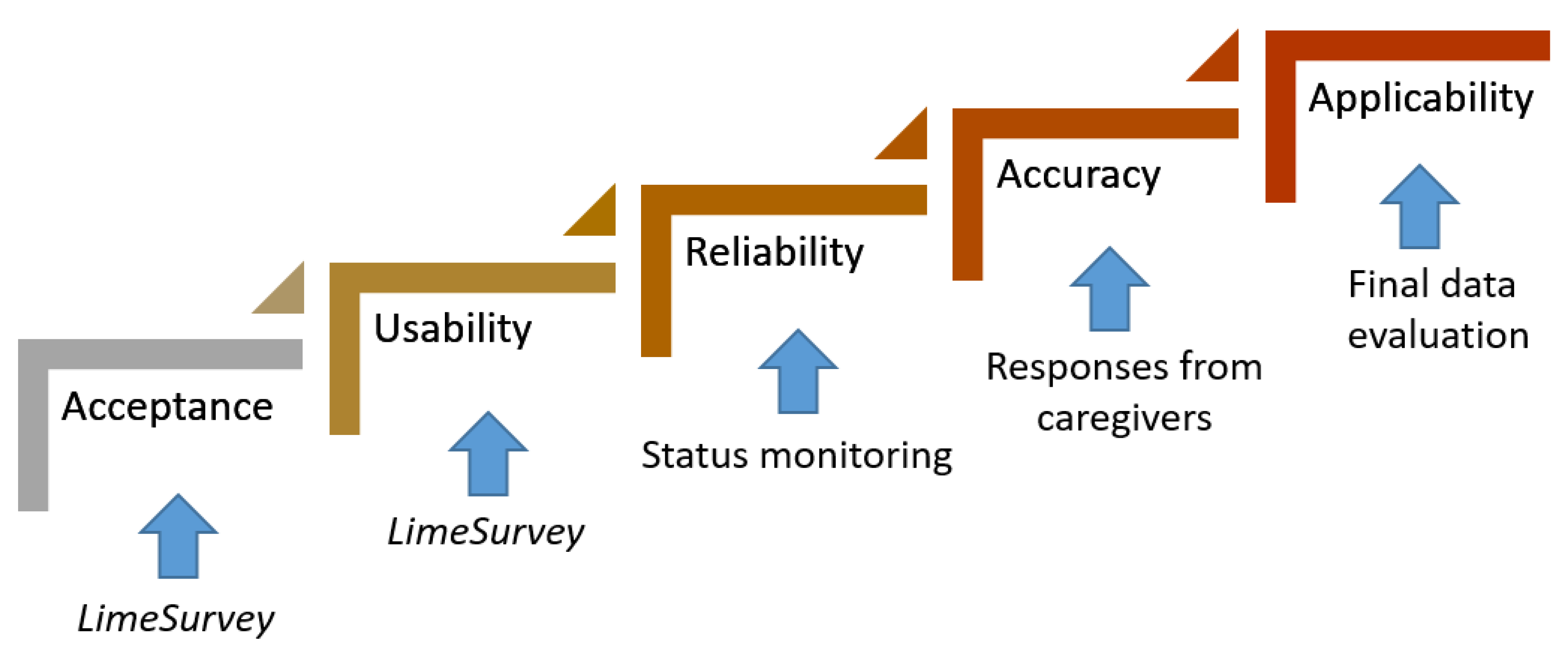
4.2. Evaluation Procedure
Local Indicators
- Acceptance -> confirmed by 60% of respondents.
- Usability -> confirmed by 70% of respondents.
- Reliability -> operational 70% of the time.
- Accuracy -> Rate of false alarms <20%.
- Applicability -> Confirmation of a specific event from at least two sensors or one sensor and caregivers.
4.3. Results of the Evaluation
4.3.1. Warsaw Pilot
4.3.2. Bratislava Pilot
4.4. Collected Feedback
4.4.1. False Alarms
- False alarms: open balcony, patient not in bed.
- Missed notifications: movement, leaving the bed.
- Physical damage: dismantled sensor, unplugged device.
- Other: system errors, delays, failed restart, etc.
4.4.2. Verbal Feedback
- Easier or better control of clients Easier or better control of clients.
- Better monitoring of clients at night.
- Better control of the working shifts.
- Better overview of what is happening in the centre.
- Prompt handling of exceptional situations.
- False alarms.
- The failure rate of the system.
- Generality of messages.
- Checking the detectors too frequently.
- Patients can dismantle the equipment.
5. Deployment and Commercialisation
- Implementation of small technical upgrades to the devices and information system based on the results from the pilot action.
- Development of blueprints for mass production.
- Final testing in the real environment.
- Selection of the production company with an implemented QA system.
- Certification according to the EU Medical Devices Regulation (MDR 2017/745).
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Population Projections in the EU. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?oldid=497115#Population_projections (accessed on 27 July 2023).
- NiCE-Life Project. Available online: https://programme2014-20.interreg-central.eu/Content.Node/niCE-life.html (accessed on 27 July 2023).
- Hwang, H.J.; Roehn, O. OECD Economic Surveys: Slovak Republic 2022; OECD: Paris, France, 2022. [Google Scholar]
- Wordlometer Femographics. Available online: https://www.worldometers.info/demographics/slovakia-demographics/ (accessed on 27 July 2023).
- Open Data Bratislava. Available online: https://opendata.bratislava.sk/en/page/people (accessed on 27 July 2023).
- STATdat. Available online: http://statdat.statistics.sk/cognosext/cgi-bin/cognos.cgi?b_action=cognosViewer&ui.action=run&ui.object=storeID%28%22iF41FA7A868E74315A56CF26B722E3A07%22%29&ui.name=Indexy%20vekov%C3%A9ho%20zlo%C5%BEenia%20-%20SR%2C%20oblasti%2C%20kraje%2C%20okresy%2C%20m (accessed on 27 July 2023).
- LimeSurvey: An Open Source Survey Tool. Available online: http://www.limesurvey.org (accessed on 27 July 2023).
- Kachman, O.; Findura, J.; Balaz, M.; Gyepes, G.; Majer, L.; Vojs, M. Inteligent Monitoring System for Universal Data Collection and Analysis. In Proceedings of the Inteligent Monitoring System for Universal Data Collection and Analysis, Košice, Slovakia, 21–22 April 2022. [Google Scholar]
- Expressif Inc. ESP8266 Technical Refefence V 1.7, 2020. Available online: https://www.espressif.com/sites/default/files/documentation/esp8266-technical_reference_en.pdf (accessed on 27 July 2023).
- M5Stack. M5Stack, Shenzen, China, 2023. Available online: https://m5stack.com (accessed on 27 July 2023).
- Libelum. Waspmote Technical Guide, Zaragoza, Spain, 2019. Available online: https://development.libelium.com/waspmote-technical-guide/hardware (accessed on 27 July 2023).
- Expressif Inc. SP32 Technical Reference Manual V5, 2022. Available online: https://www.espressif.com/sites/default/files/documentation/esp32_technical_reference_manual_en.pdf (accessed on 27 July 2023).
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Version | Use | Sub-Version | Safety Level |
|---|---|---|---|
| AP1 | Located under the patients’ bed to monitor leaving the bed | AP1-H | Level 1—patient in bed |
| AP1-M | |||
| AP1-W | |||
| AP2 | Placed at the doors to monitor leaving the room | AP2-H | Level 2—patient in the room |
| AP2-M | |||
| AP4 | Located in common areas, stairs, or forbidden zones to prevent danger | AP4-H | Level 3—patient in the centre |
| AP4-M | |||
| AP4-W | |||
| AP6 | Located in the kitchen or cafeteria to prevent fire events | AP6-H | Level 4—safety of the centre |
| AP6-M | |||
| AP6-W |
| Sensor Type | Specification | Used for AP-NURSE Version |
|---|---|---|
| Light sensor | GL5528 | AP1H, AP1W, AP6M |
| Temperature sensor | BME280, BME680, NCIR-MLX90614 | AP1H, AP1M, AP1W, AP6M |
| PIR sensors | HC-SR505, SB312 | AP1H, AP2H, AP6H, AP1M, AP1W, AP4M, AP4W, AP6 |
| ToF sensors | VI53L0X | AP2H, AP2M, AP4M, AP4W |
| Smoke sensor | MQ-135, MQ-5, BME680 | AP1H, AP6H, AP1M, AP1W |
| Bed pressure sensor | FSR402 | AP1H, AP1M, AP1W |
| Testing Pilot | Patients | Formal Caregivers | Professionals |
|---|---|---|---|
| Warsaw | 117 | 13 | 8 |
| Bratislava | 20 | 7 | 3 |
| Total | 137 | 20 | 11 |
| AP-NURSE Version | Installed in Warsaw | Installed in Bratislava |
|---|---|---|
| AP1-H | 9 | 8 |
| AP1-M | 8 | - |
| AP1-W | 5 | - |
| AP2-H | - | 2 |
| AP2-M | 13 | - |
| AP4-H | 8 | 3 |
| AP4-M | 1 | - |
| AP4-W | 1 | - |
| AP6-H | - | 1 |
| AP6-M | - | 1 |
| AP6-W | 3 | - |
| Total | 48 | 15 |
| Version | AP1 | AP2 | AP4 | AP6 |
|---|---|---|---|---|
| Acceptance |  | | | |
| Usability | | | | |
| Reliability |  |  | | |
| Accuracy | | | | |
| Applicability | | | | |
| Decision | Passed | Failed | Passed | Failed |
| Version | AP1 | AP2 | AP4 | AP6 |
|---|---|---|---|---|
| Acceptance | | | | |
| Usability | | | | |
| Reliability | | | | |
| Accuracy | | | | |
| Applicability | | | | |
| Decision | Passed | Failed | Passed | Failed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čerba, Š.; Vrban, B.; Lüley, J.; Vojs, M.; Vrška, M.; Behúl, M.; Bendík, J.; Cenký, M.; Janíček, F.; Majer, L.; et al. AP-NURSE: A Modular Tool to Ease the Life of Patients Suffering from Cognitive Diseases. Electronics 2023, 12, 3818. https://doi.org/10.3390/electronics12183818
Čerba Š, Vrban B, Lüley J, Vojs M, Vrška M, Behúl M, Bendík J, Cenký M, Janíček F, Majer L, et al. AP-NURSE: A Modular Tool to Ease the Life of Patients Suffering from Cognitive Diseases. Electronics. 2023; 12(18):3818. https://doi.org/10.3390/electronics12183818
Chicago/Turabian StyleČerba, Štefan, Branislav Vrban, Jakub Lüley, Marian Vojs, Martin Vrška, Miroslav Behúl, Jozef Bendík, Matej Cenký, František Janíček, Libor Majer, and et al. 2023. "AP-NURSE: A Modular Tool to Ease the Life of Patients Suffering from Cognitive Diseases" Electronics 12, no. 18: 3818. https://doi.org/10.3390/electronics12183818
APA StyleČerba, Š., Vrban, B., Lüley, J., Vojs, M., Vrška, M., Behúl, M., Bendík, J., Cenký, M., Janíček, F., Majer, L., & Gyepes, G. (2023). AP-NURSE: A Modular Tool to Ease the Life of Patients Suffering from Cognitive Diseases. Electronics, 12(18), 3818. https://doi.org/10.3390/electronics12183818