



A Projected AR Serious Game for Shoulder Rehabilitation Using Hand-Finger Tracking and Performance Metrics: A Preliminary Study on Healthy Subjects


 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
- The application area (e.g., cognitive and motor rehabilitation);
- The game interface (e.g., two-dimensional or three-dimensional);
- The number of players (e.g., single or multi-player);
- The game genre (e.g., general videogames, serious games, etc.);
- The adaptability to the user competence level (e.g., novice versus proficient);
- The feedback on performance (e.g., no feedback or performance metrics);
- The monitoring of game progress (e.g., in-game monitoring or not);
- The portability of the game (e.g., special hardware required or not);
- The accessibility of the game (e.g., eliminating rehab barriers such as cost, etc.);
- The interaction technology (e.g., mouse/keyboard, gestures, touch screens, etc.).
- A wearable application “AR Rehab Game App” for training shoulder horizontal and vertical flexion, based on head-mounted display (HMD) technology (i.e., the Microsoft HoloLens). Our preliminary tests showed that AR technology allows promising results in terms of user motivation but needs further evolution to improve the FOV and reduce the physical discomfort (e.g., the weight of the HMD) [25];
- A non-wearable application for training shoulder horizontal adduction, based on a standard desktop computer, a screen, and the LMC as a hand-tracking system. A limitation of this version, compared to the HMD-based version, is the reduced portability. However, this limitation was balanced by other advantages such as improved ergonomics and lower cost [27].
2. Materials and Methods
- The tracking device must be able to detect the patient’s hand during the trial;
- The selected device must be non-invasive, easy-use, and affordable.
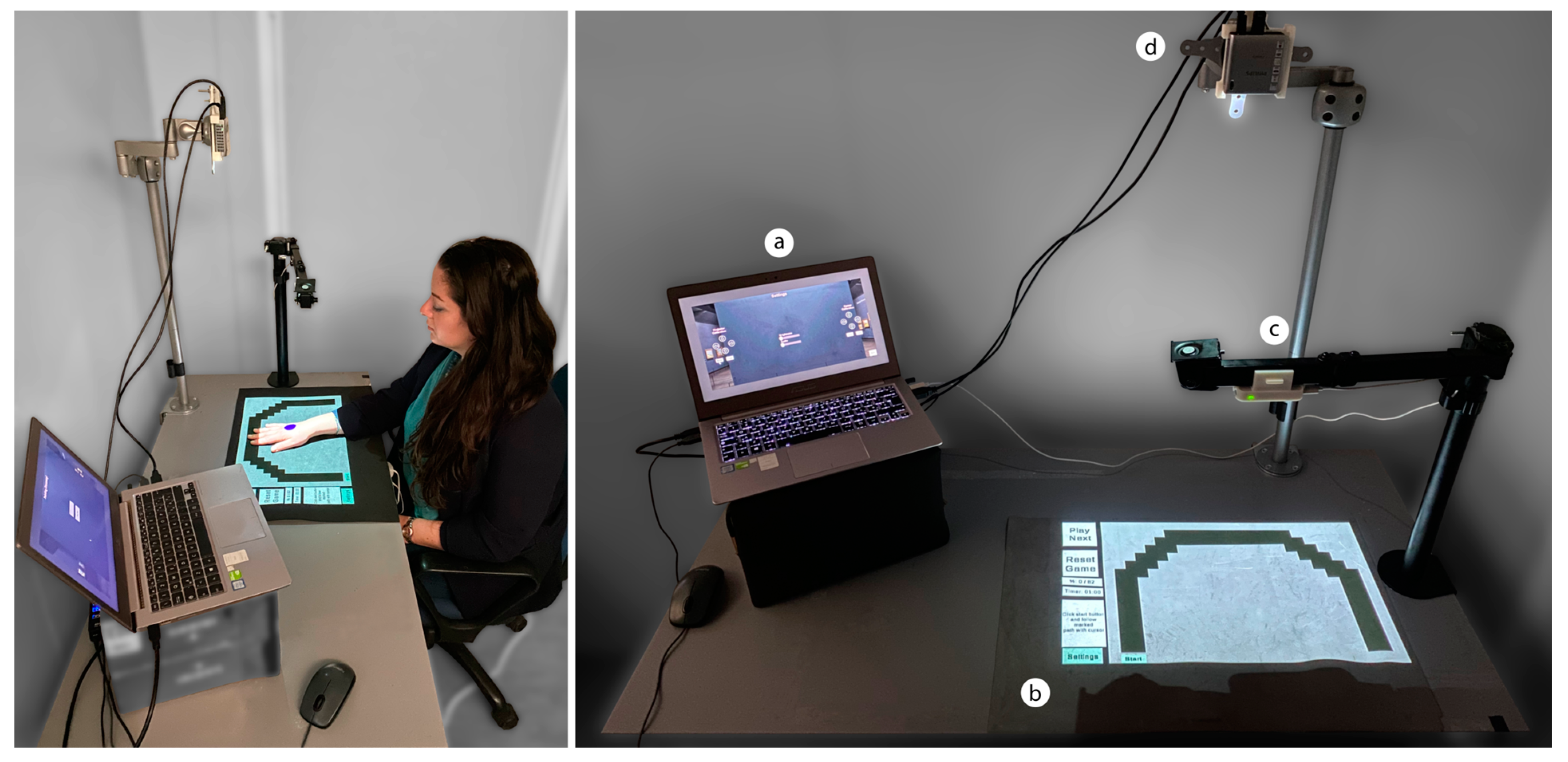
2.1. Apparatus
- A laptop (ASUS UX303UB, Intel Core i5-6200U @ 2.30 GHz processor, 8 GB RAM memory, and NVIDIA GeForce 940 M graphics board) running Microsoft Windows 10 Pro;
- A tilt-top table (range of tilt angle: 0–50°);
- A black rubber desk pad (60 × 40 cm), as the projection surface for the game;
- A portable PicoPix projector (Philips PPX4010, resolution 1280 × 720, screen distance 50–500 cm, aspect ratio 1.47:1, size 6.8 × 6.6 × 2.2 cm, weight 81.6 g) [33].
2.2. Technical Details
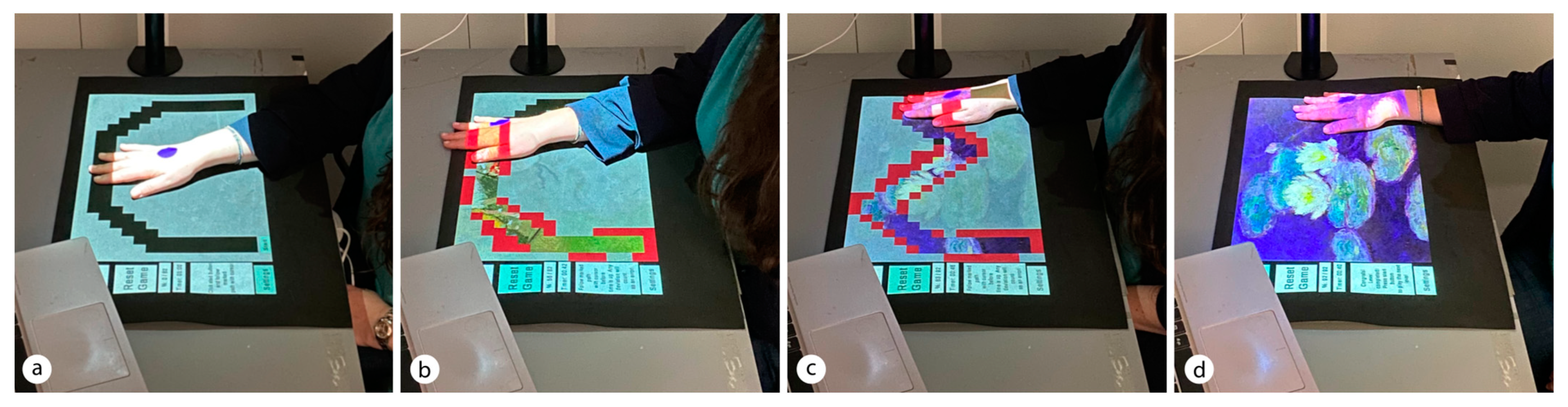
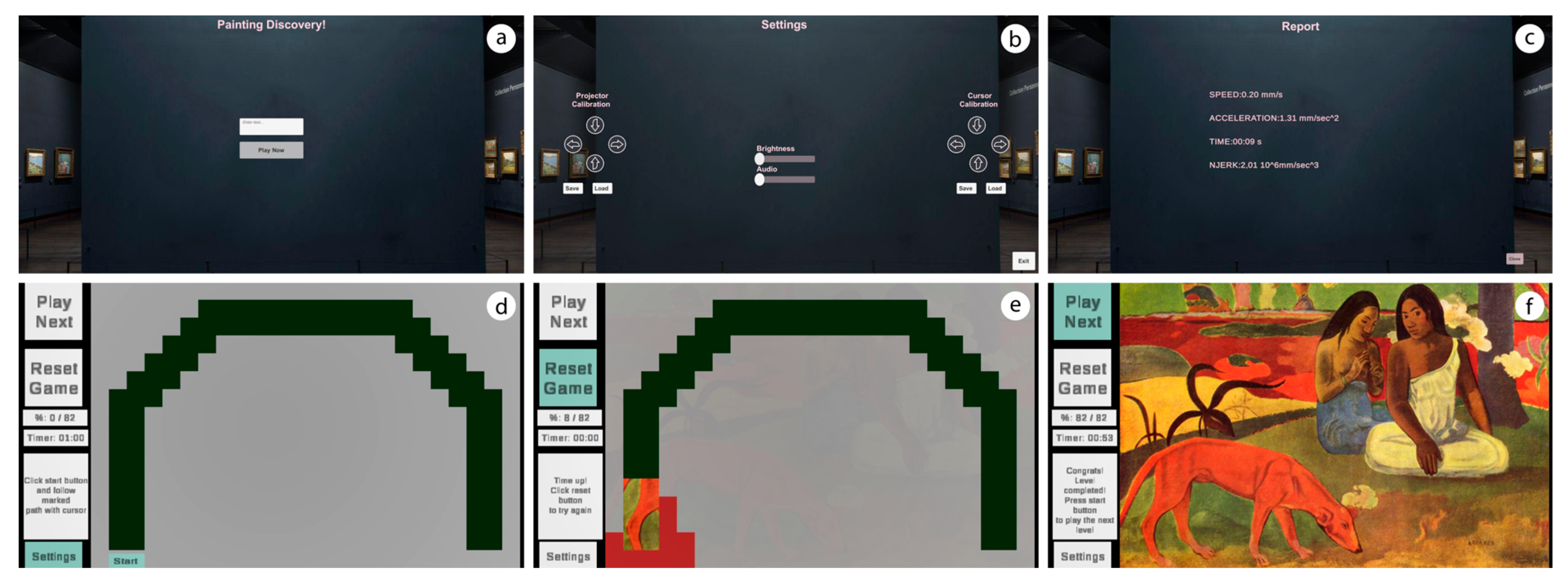
2.3. Serious Game Design
2.4. Performance Metrics
2.5. System Testing
3. Results
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Rego, P.; Moreira, P.M.; Reis, L.P. Serious games for rehabilitation: A survey and a classification towards a taxonomy. In Proceedings of the 5th Iberian Conference on Information Systems and Technologies, Santiago de Compostela, Spain, 16–19 June 2010; pp. 1–6. [Google Scholar]
- Vallati, C.; Virdis, A.; Gesi, M.; Carbonaro, N.; Tognetti, A. ePhysio: A Wearables-Enabled Platform for the Remote Management of Musculoskeletal Diseases. Sensors 2019, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; Torres-Carrion, P.V. Serious games for rehabilitation: Gestural interaction in personalized gamified exercises through a recommender system. J. Biomed. Inform. 2019, 97, 103266. [Google Scholar] [CrossRef] [PubMed]
- Pirovano, M.; Surer, E.; Mainetti, R.; Lanzi, P.L.; Alberto Borghese, N. Exergaming and rehabilitation: A methodology for the design of effective and safe therapeutic exergames. Entertain. Comput. 2016, 14, 55–65. [Google Scholar] [CrossRef]
- Kostoulas, T.; Mporas, I.; Kocsis, O.; Ganchev, T.; Katsaounos, N.; Santamaria, J.J.; Jimenez-Murcia, S.; Fernandez-Aranda, F.; Fakotakis, N. Affective speech interface in serious games for supporting therapy of mental disorders. Expert Syst. Appl. 2012, 39, 11072–11079. [Google Scholar] [CrossRef]
- Valladares-Rodríguez, S.; Pérez-Rodríguez, R.; Anido-Rifón, L.; Fernández-Iglesias, M. Trends on the application of serious games to neuropsychological evaluation: A scoping review. J. Biomed. Inform. 2016, 64, 296–319. [Google Scholar] [CrossRef] [PubMed]
- Merians, A.S.; Jack, D.; Boian, R.; Tremaine, M.; Burdea, G.C.; Adamovich, S.V.; Recce, M.; Poizner, H. Virtual reality-augmented rehabilitation for patients following stroke. Phys. Ther. 2002, 82, 898–915. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Review of the Augmented Reality Systems for Shoulder Rehabilitation. Information 2019, 10, 154. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Condino, S.; Gesi, M.; Ferrari, M.; Ferrari, V. Augmented Reality Simulator for Laparoscopic Cholecystectomy Training. In Augmented and Virtual Reality, Proceedings of the AVR 2014, Lecce, Italy, 17–20 September 2014; De Paolis, L., Mongelli, A., Eds.; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2014; Volume 8853, pp. 428–433. [Google Scholar] [CrossRef]
- Taylor, J.; Curran, K. Glove-based technology in hand rehabilitation. In Gamification: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2015; pp. 983–1002. [Google Scholar]
- Ma, M.; Bechkoum, K. Serious games for movement therapy after stroke. In Proceedings of the 2008 IEEE International Conference on Systems, Man and Cybernetics, Singapore, 12–15 October 2008; pp. 1872–1877. [Google Scholar]
- Arip, E.S.M.; Ismail, W.; Nordin, M.J.; Radman, A. Virtual reality rehabilitation for stroke patients: Recent review and research issues. AIP Conf. Proc. 2017, 1905, 050007. [Google Scholar] [CrossRef]
- Cho, D.-R.; Lee, S.-H. Effects of virtual reality immersive training with computerized cognitive training on cognitive function and activities of daily living performance in patients with acute stage stroke: A preliminary randomized controlled trial. Medicine 2019, 98, e14752. [Google Scholar] [CrossRef]
- Microsoft Kinect. Available online: https://it.wikipedia.org/wiki/Microsoft_Kinect (accessed on 27 May 2023).
- Leap Motion Controller Product. Available online: https://www.ultraleap.com/product/leap-motion-controller/ (accessed on 27 May 2023).
- Taylor, J.; Curran, K. Using leap motion and gamification to facilitate and encourage rehabilitation. In Handbook of Research on Holistic Perspectives in Gamification for Clinical Practice; IGI Global: Hershey, PA, USA, 2016; pp. 183–192. [Google Scholar]
- Vast.Rheab Product. Available online: https://vast.rehab/ (accessed on 27 May 2023).
- Oña, E.D.; Balaguer, C.; Cano-de la Cuerda, R.; Collado-Vázquez, S.; Jardón, A. Effectiveness of Serious Games for Leap Motion on the Functionality of the Upper Limb in Parkinson’s Disease: A Feasibility Study. Comput. Intell. Neurosci. 2018, 2018, 7148427. [Google Scholar] [CrossRef]
- Guzsvinecz, T.; Szucs, V.; Sik-Lanyi, C. Suitability of the Kinect sensor and Leap Motion controller—A literature review. Sensors 2019, 19, 1072. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Morone, G.; Fusco, A.; Castagnoli, M.; Fusco, F.R.; Pratesi, L.; Paolucci, S. Leap motion controlled videogame-based therapy for rehabilitation of elderly patients with subacute stroke: A feasibility pilot study. Top. Stroke Rehabil. 2015, 22, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Weiss Cohen, M.; Regazzoni, D. Hand rehabilitation assessment system using leap motion controller. AI Soc. 2020, 35, 581–594. [Google Scholar] [CrossRef]
- Khademi, M.; Mousavi Hondori, H.; McKenzie, A.; Dodakian, L.; Lopes, C.V.; Cramer, S.C. Free-hand interaction with leap motion controller for stroke rehabilitation. In CHI′14 Extended Abstracts on Human Factors in Computing Systems; Association for Computing Machinery: New York, NY, USA, 2014; pp. 1663–1668. [Google Scholar]
- Wang, Z.R.; Wang, P.; Xing, L.; Mei, L.P.; Zhao, J.; Zhang, T. Leap Motion-based virtual reality training for improving motor functional recovery of upper limbs and neural reorganization in subacute stroke patients. Neural Regen. Res. 2017, 12, 1823–1831. [Google Scholar] [PubMed]
- Wu, Y.T.; Chen, K.H.; Ban, S.L.; Tung, K.Y.; Chen, L.R. Evaluation of leap motion control for hand rehabilitation in burn patients: An experience in the dust explosion disaster in Formosa Fun Coast. Burn. J. Int. Soc. Burn Inj. 2019, 45, 157–164. [Google Scholar] [CrossRef]
- Condino, S.; Turini, G.; Viglialoro, R.; Gesi, M.; Ferrari, V. Wearable Augmented Reality Application for Shoulder Rehabilitation. Electronics 2019, 8, 1178. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Turini, G.; Condino, S.; Ferrari, V.; Gesi, M. Proof of concept: Vr rehabilitation game for people with shoulder disorders. In Augmented Reality, Virtual Reality, and Computer Graphics, Proceedings of the AVR 2019, Santa Maria al Bagno, Italy, 24–27 June 2019; De Paolis, L., Bourdot, P., Eds.; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2019; Volume 11613, pp. 344–350. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Mamone, V.; Carbone, M.; Ferrari, V.; Ghelarducci, G.; Ferrari, M.; Gesi, M. Interactive serious game for shoulder rehabilitation based on real-time hand tracking. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 2020, 28, 403–414. [Google Scholar] [CrossRef]
- Mousavi Hondori, H.; Khademi, M.; Dodakian, L.; McKenzie, A.; Lopes, C.V.; Cramer, S.C. Choice of Human–Computer Interaction Mode in Stroke Rehabilitation. Neurorehabilit. Neural Repair 2016, 30, 258–265. [Google Scholar] [CrossRef]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Augmented Reality, Mixed Reality, and Hybrid Approach in Healthcare Simulation: A Systematic Review. Appl. Sci. 2021, 11, 2338. [Google Scholar] [CrossRef]
- Amengual Alcover, E.; Jaume, I.C.A.; Moyà-Alcover, B. PROGame: A process framework for serious game development for motor rehabilitation therapy. PLoS ONE 2018, 13, e0197383. [Google Scholar] [CrossRef]
- Palacios-Navarro, G.; Hogan, N. Head-Mounted Display-Based Therapies for Adults Post-Stroke: A Systematic Review and Meta-Analysis. Sensors 2021, 21, 1111. [Google Scholar] [CrossRef] [PubMed]
- Penumudi, S.A.; Kuppam, V.A.; Kim, J.H.; Hwang, J. The effects of target location on musculoskeletal load, task performance, and subjective discomfort during virtual reality interactions. Appl. Ergon. 2019, 84, 103010. [Google Scholar] [CrossRef] [PubMed]
- PicoPix Projector Product. Available online: https://www.philips.it/c-p/PPX4010_INT/picopix-proiettore-tascabile (accessed on 27 May 2023).
- Rolyan Graded ROM Arc Product. Available online: https://www.performancehealth.com/graded-rom-arc (accessed on 27 May 2023).
- Elgendi, M.; Picon, F.; Magnenat-Thalmann, N.; Abbott, D. Arm movement speed assessment via a Kinect camera: A preliminary study in healthy subjects. Biomed. Eng. Online 2014, 13, 88. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.-S.; Soh, J.; Bae, Y.J.; Seung Yang, H. Hand gesture recognition using combined features of location, angle and velocity. Pattern Recognit. 2001, 34, 1491–1501. [Google Scholar] [CrossRef]
- Rohrer, B.; Fasoli, S.; Krebs, H.I.; Hughes, R.; Volpe, B.; Frontera, W.R.; Stein, J.; Hogan, N. Movement smoothness changes during stroke recovery. J. Neurosci. 2002, 22, 8297–8304. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. NeuroEng. Rehabil. 2015, 12, 112. [Google Scholar] [CrossRef]
- Kato, N.; Tanaka, T.; Sugihara, S.; Shimizu, K.; Kudo, N. A study of the effect of visual depth information on upper limb movement by use of measurement of smoothness. J. Phys. Ther. Sci. 2016, 28, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Krastev, G.; Andreeva, M. A software tool for experimental study leap motion. AIRCC’s Int. J. Comput. Sci. Inf. Technol. 2015, 7, 145–153. [Google Scholar] [CrossRef]
- Mamone, V.; Viglialoro, R.M.; Cutolo, F.; Cavallo, F.; Guadagni, S.; Ferrari, V. Robust Laparoscopic Instruments Tracking Using Colored Strips. In Augmented Reality, Virtual Reality, and Computer Graphics, Proceedings of the AVR 2017, Ugento, Italy, 12–15 June 2017; De Paolis, L., Bourdot, P., Mongelli, A., Eds.; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2017; Volume 10325, pp. 129–143. [Google Scholar] [CrossRef]
- Teulings, H.L.; Contreras-Vidal, J.L.; Stelmach, G.E.; Adler, C.H. Parkinsonism reduces coordination of fingers, wrist, and arm in fine motor control. Exp. Neurol. 1997, 146, 159–170. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Contact-Free | Hand Tracking | Low Cost |
|---|---|---|---|
| Nintendo Wii Remote MotionPlus | no | yes | yes |
| Microsoft HoloLens | no | yes | no |
| Leap Motion Controller (LMC) | yes | yes | yes |
| Number of Subjects | |
|---|---|
| Gender (male, female, non-binary) | 5, 11, 0 |
| Age (min, max, mean, STD) | 21, 46, 31, 7 |
| Physiotherapists (yes, no) | 7, 9 |
| Handedness (left, right, ambidextrous) | 0, 16, 0 |
| Vision (10/10 naked eyes, corrected to 10/10 with lenses) | 7, 9 |
| Experience with videogames (none, limited, familiar, experienced) | 2, 5, 8, 1 |
| Experience with AR (none, limited, familiar, experienced) | 4, 3, 7, 2 |
| Diagnosed with a shoulder disorder (no, yes) | 16, 0 |
| Perceived shoulder pain (no, yes) | 16, 0 |
| Item | Median (25°~75°) | p-Value (All) | |||||
|---|---|---|---|---|---|---|---|
| All | Ph * | Eng * | Profession * | VG * | AR * | ||
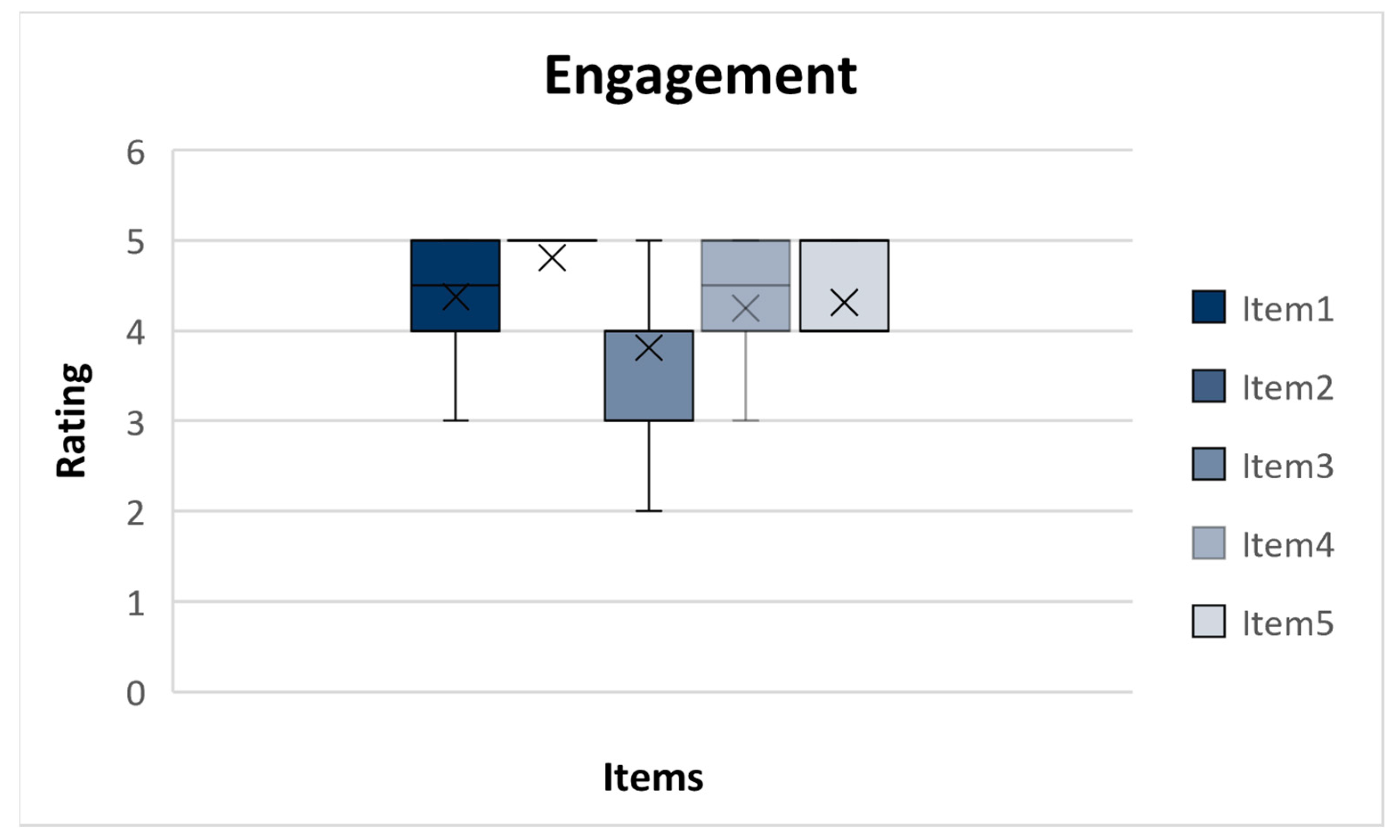
| Engagement | The game goal (discovering the painting) is motivating, interesting, and engaging. | 4.5 (5–4) | 4 (5–4) | 5 (5–4) | 0.418 | 0.103 | 0.885 |
| The game goal is clear. | 5 (5–5) | 5 (5–4.25) | 5 (5–5) | 0.535 | 0.442 | 0.312 | |
| The visual feedback such as countdown timer and scoring system is motivating. | 4 (4–3) | 4 (4.75–3.25) | 4 (4–3) | 0.427 | 0.115 | 0.268 | |
| The game visuals and audio are enjoyable. | 4.5 (5–4) | 4 (4.75–3.25) | 5 (5–4.25) | 0.077 | 0.169 | 0.834 | |
| Likely to play again. | 4 (5–4) | 4 (5–4) | 4.5 (5–4) | 0.480 | 0.228 | 0.790 | |
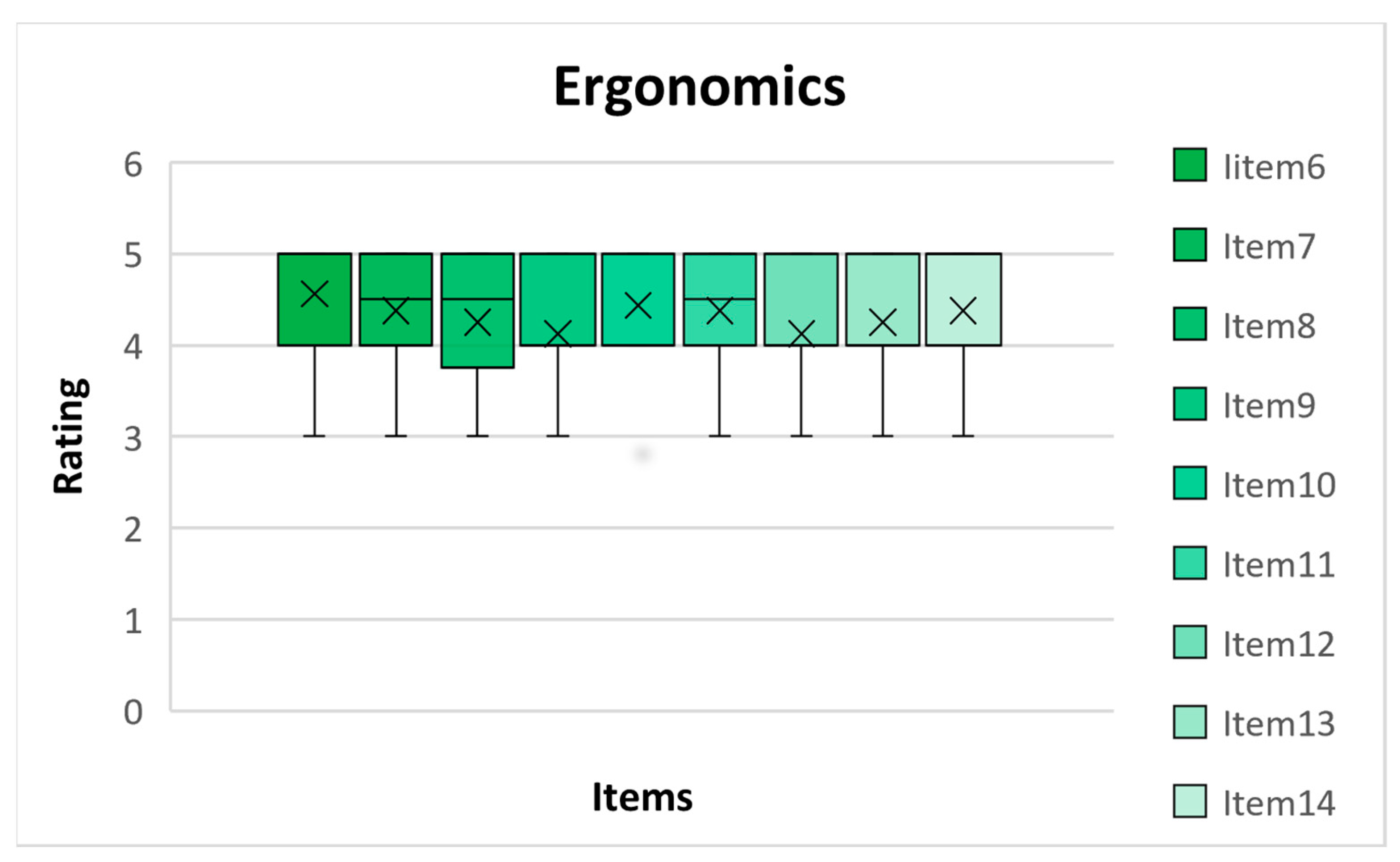
| Ergonomics | The graphical user interface (buttons) is intuitive and user-friendly. | 5 (5–4) | 5 (5–4.25) | 5 (5–4) | 0.653 | 0.387 | 0.634 |
| The text instructions, buttons, and counters are readable and clear. | 4.5 (5–4) | 4 (5–4) | 4 (5–4) | 0.418 | 0.226 | 0.228 | |
| Adjusting the projected image brightness and volume improves playability. | 4.5 (5–3.25) | 5 (5–3) | 5 (5–4) | 0.254 | 0.521 | 0.816 | |
| The trajectory thickness and the panel size allow good playability of the game. | 4 (5–4) | 4 (4.75–4) | 4 (5–4) | 0.637 | 0.659 | 0.932 | |
| The projected image is well contrasted to allow for good playability. | 4 (5–4) | 4 (5–4) | 4.5 (5–4) | 0.626 | 0.350 | 0.218 | |
| The projected image has a good resolution to enable good playability. | 4.5 (5–4) | 4.5 (5–3.25) | 4.5 (5–4) | 0.643 | 0.168 | 0.200 | |
| The latency (lag, delay) between real hand movement and virtual 3D cursor displacement is acceptable. | 4 (5–4) | 4.5 (5–4) | 4 (4–4) | 0.239 | 0.256 | 0.932 | |
| Interaction with the game does not require mental effort. | 4 (5–4) | 4 (4.75–3.25) | 5 (5–4) | 0.085 | 0.361 | 0.929 | |
| No postural discomfort (arm–shoulder excluded) is perceived during the game session. | 5 (5–4) | 4 (5–4) | 5 (5–4.25) | 0.195 | 0.763 | 0.612 | |
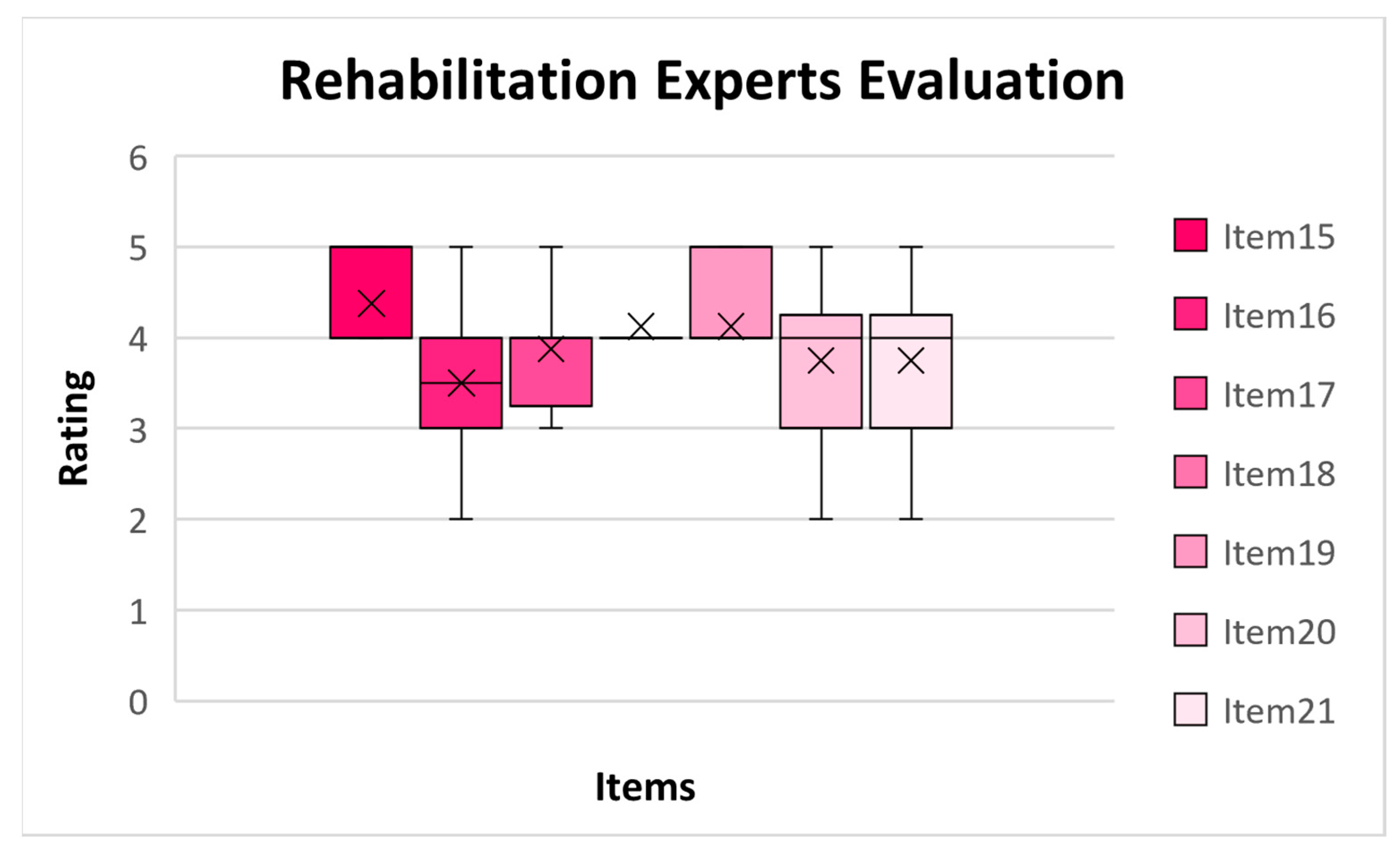
| Rehabilitation Experts Evaluation | The experimental setup allows the user to perform the task with the correct posture. | 5 (5–4) | - | - | - | - | |
| The system could bring more benefits than a traditional rehabilitation process. | 3.5(4–3) | - | - | - | - | ||
| System can help speed up patient recovery. | 4 (4–3.25) | - | - | - | - | ||
| The proposed system is useful for upper-arm rehabilitation. | 4 (4–4) | - | - | - | - | ||
| The proposed system allows the user to perform the rehabilitation task without the need for a supervisor. | 4 (5–4) | - | - | - | - | ||
| The system is easier to customize than traditional rehabilitation treatment (e.g., Rolyan’s arch). | 4 (4.75–3) | - | - | - | - | ||
| The implemented trajectories are suitable for a range of motion rehabilitation. | 4 (4.75–3) | - | - | - | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viglialoro, R.M.; Turini, G.; Carbone, M.; Condino, S.; Mamone, V.; Coluccia, N.; Dell’Agli, S.; Morucci, G.; Ryskalin, L.; Ferrari, V.; et al. A Projected AR Serious Game for Shoulder Rehabilitation Using Hand-Finger Tracking and Performance Metrics: A Preliminary Study on Healthy Subjects. Electronics 2023, 12, 2516. https://doi.org/10.3390/electronics12112516
Viglialoro RM, Turini G, Carbone M, Condino S, Mamone V, Coluccia N, Dell’Agli S, Morucci G, Ryskalin L, Ferrari V, et al. A Projected AR Serious Game for Shoulder Rehabilitation Using Hand-Finger Tracking and Performance Metrics: A Preliminary Study on Healthy Subjects. Electronics. 2023; 12(11):2516. https://doi.org/10.3390/electronics12112516
Chicago/Turabian StyleViglialoro, Rosanna M., Giuseppe Turini, Marina Carbone, Sara Condino, Virginia Mamone, Nico Coluccia, Stefania Dell’Agli, Gabriele Morucci, Larisa Ryskalin, Vincenzo Ferrari, and et al. 2023. "A Projected AR Serious Game for Shoulder Rehabilitation Using Hand-Finger Tracking and Performance Metrics: A Preliminary Study on Healthy Subjects" Electronics 12, no. 11: 2516. https://doi.org/10.3390/electronics12112516
APA StyleViglialoro, R. M., Turini, G., Carbone, M., Condino, S., Mamone, V., Coluccia, N., Dell’Agli, S., Morucci, G., Ryskalin, L., Ferrari, V., & Gesi, M. (2023). A Projected AR Serious Game for Shoulder Rehabilitation Using Hand-Finger Tracking and Performance Metrics: A Preliminary Study on Healthy Subjects. Electronics, 12(11), 2516. https://doi.org/10.3390/electronics12112516