
A Dual-Armed Robotic Puncture System: Design, Implementation and Preliminary Tests

 ,
,
Abstract
:
1. Introduction
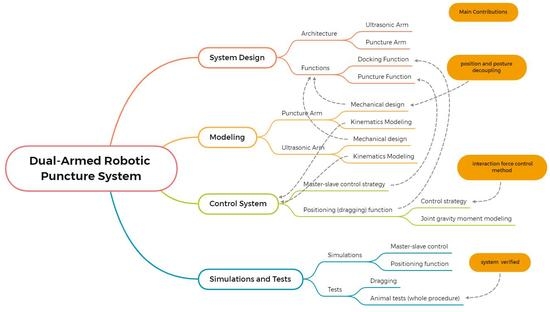
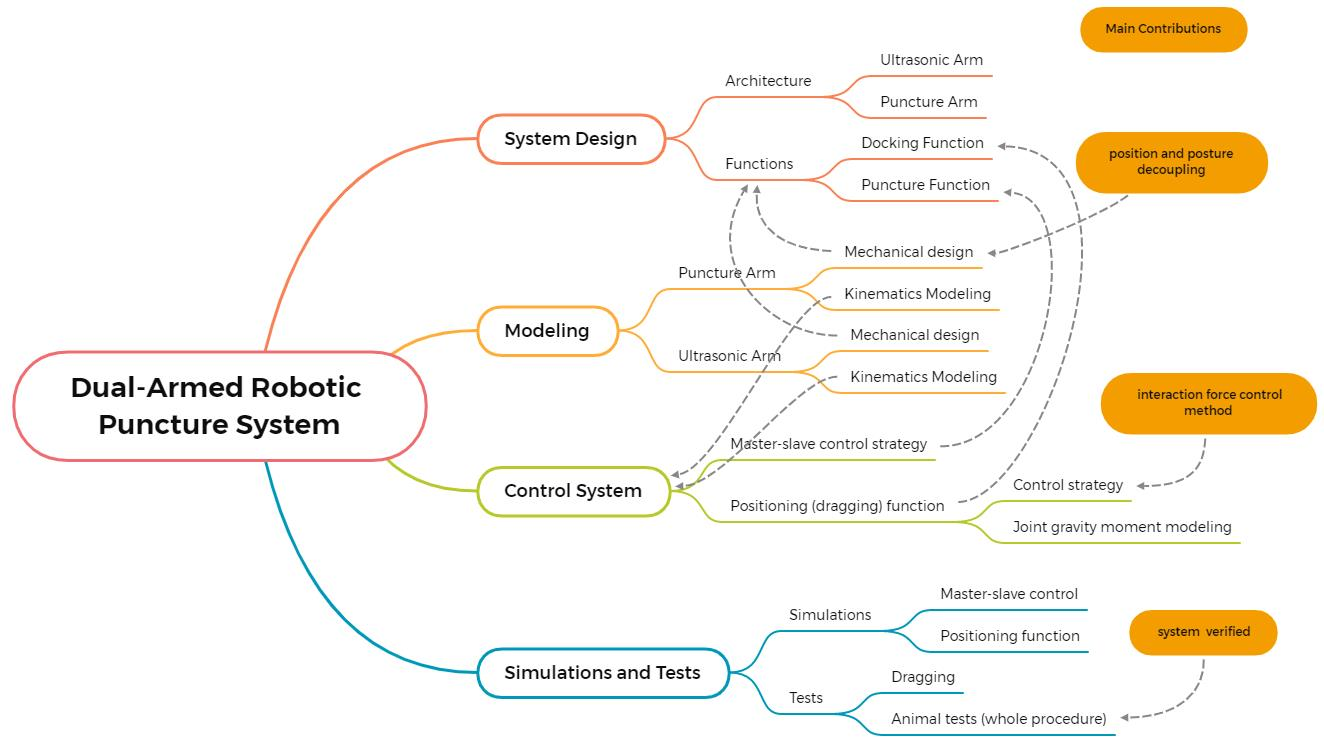
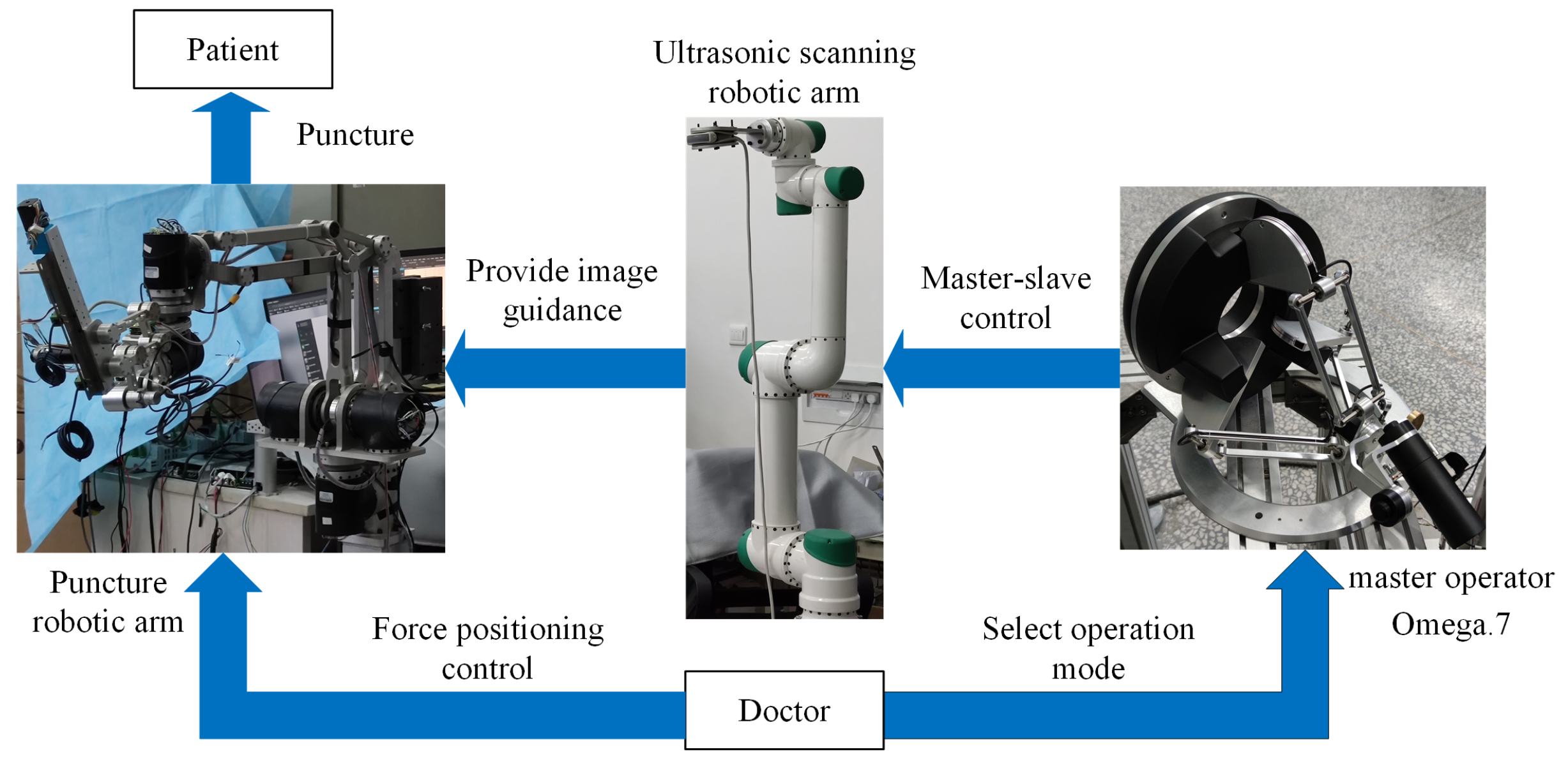
2. System Design and Modeling
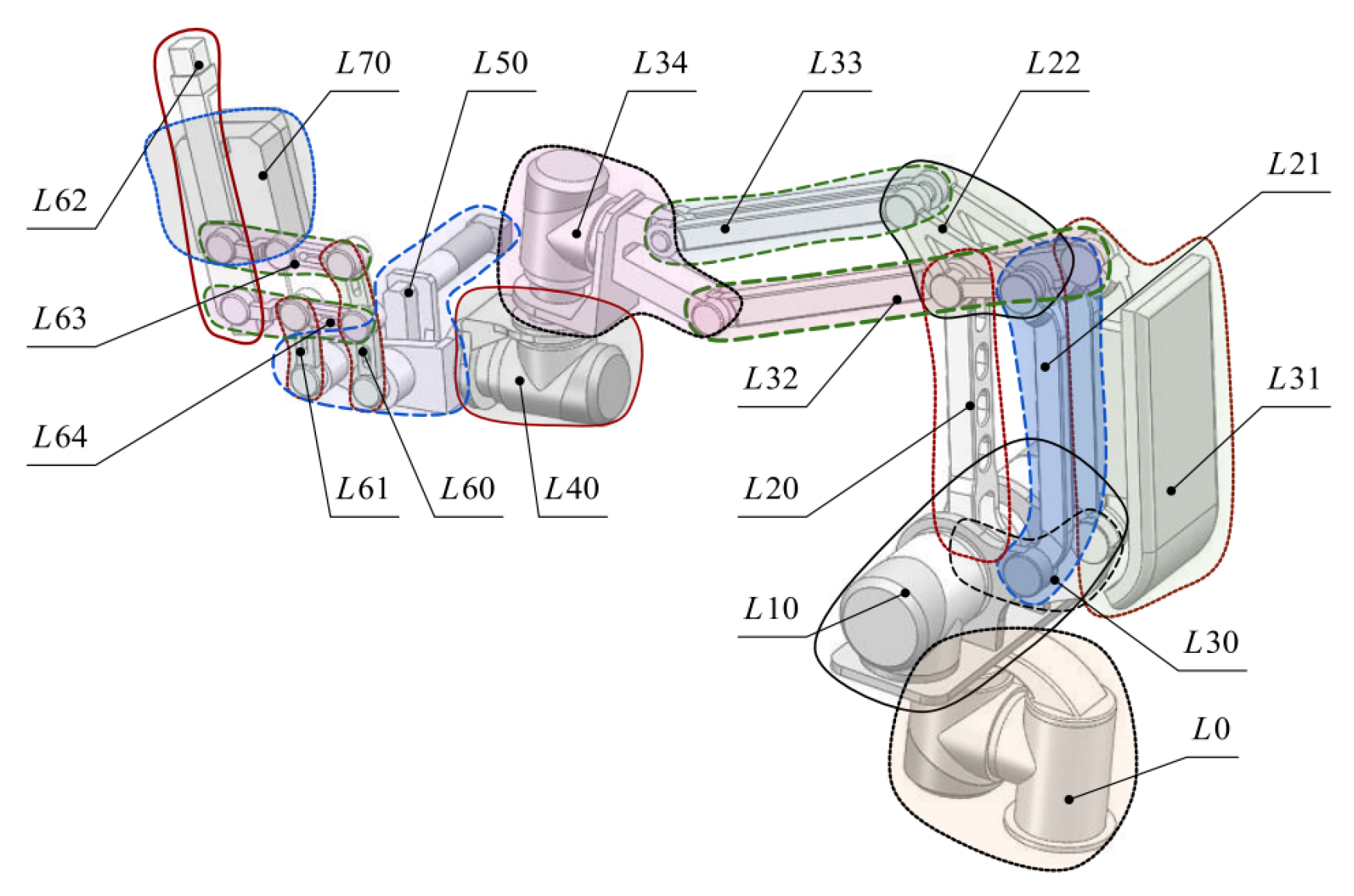
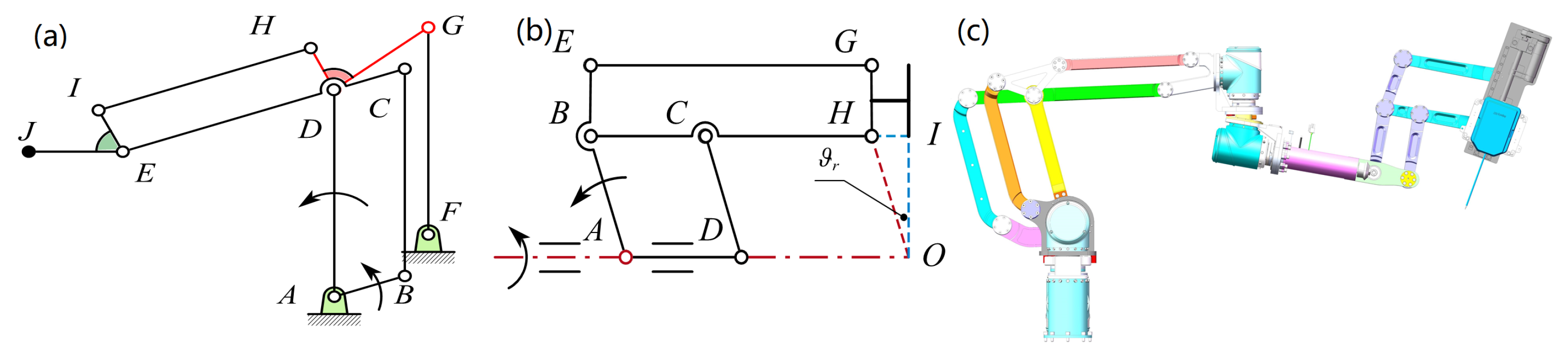
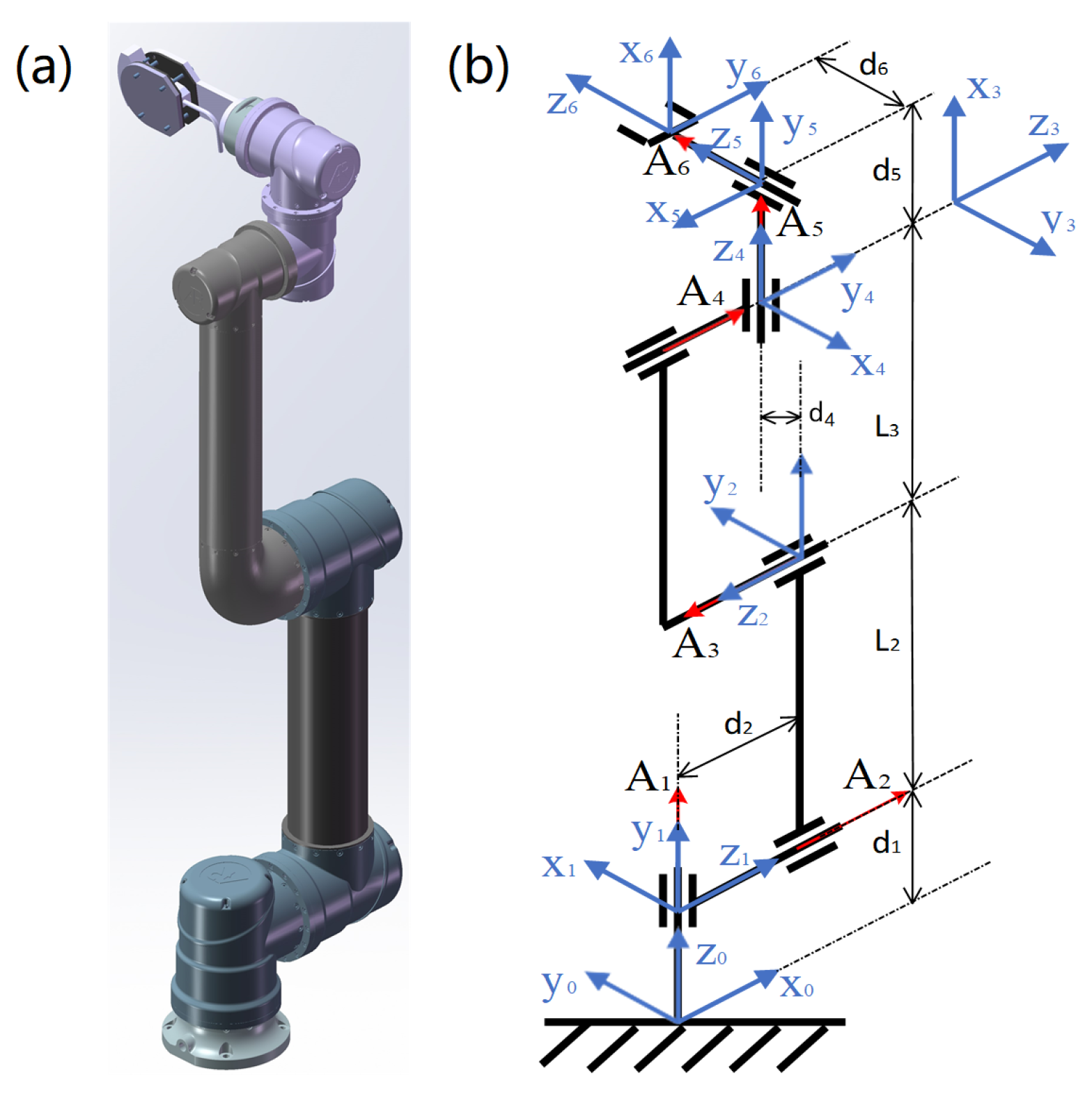
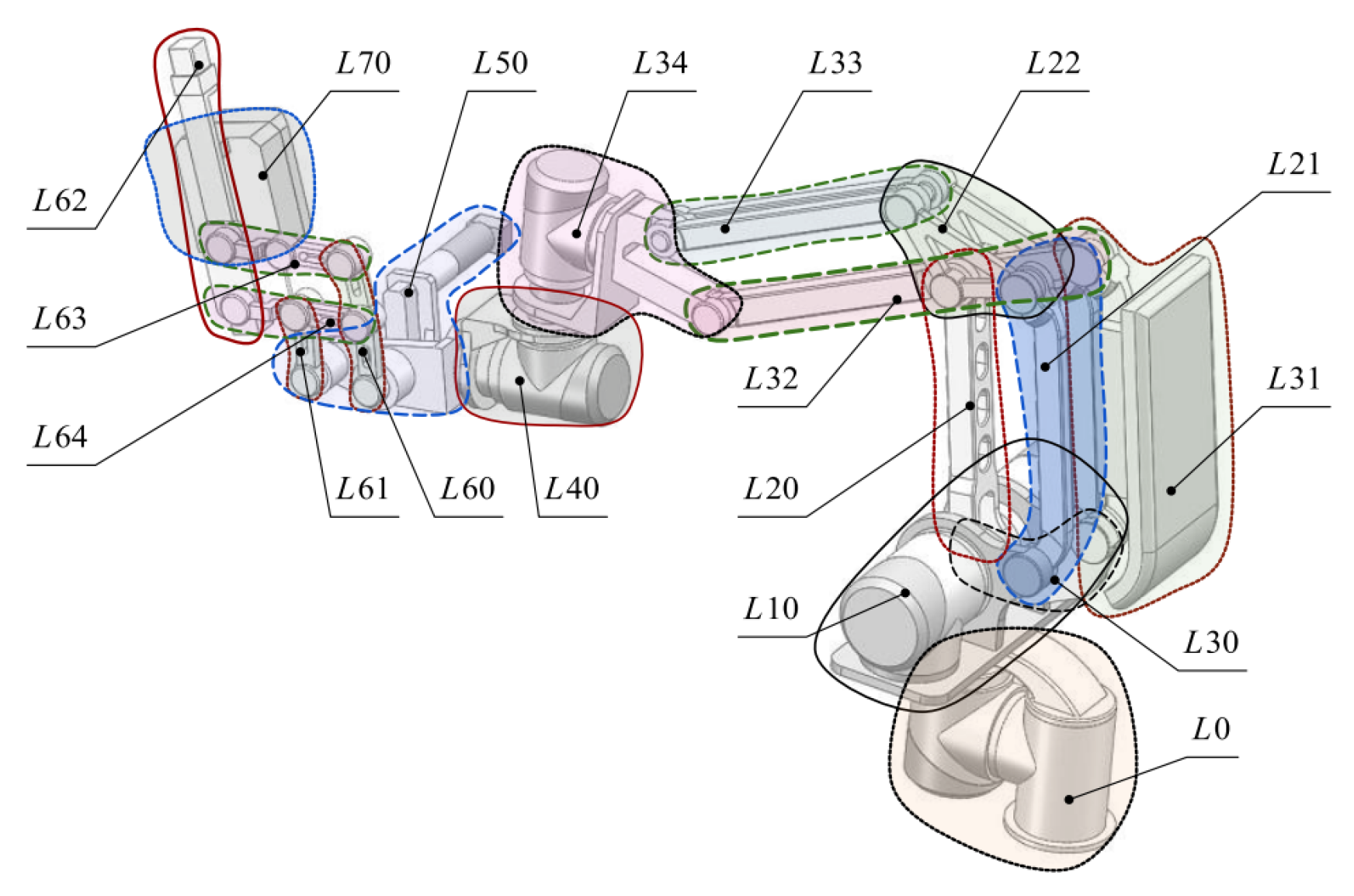
2.1. Mechanical Design and Kinematic Modeling of Puncture Arm
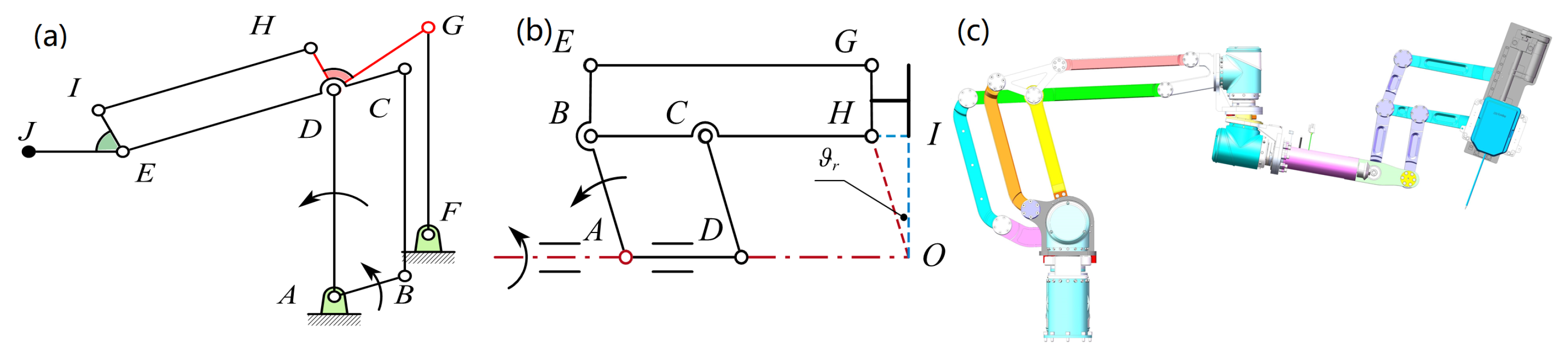
2.1.1. Mechanical Design of Puncture Arm
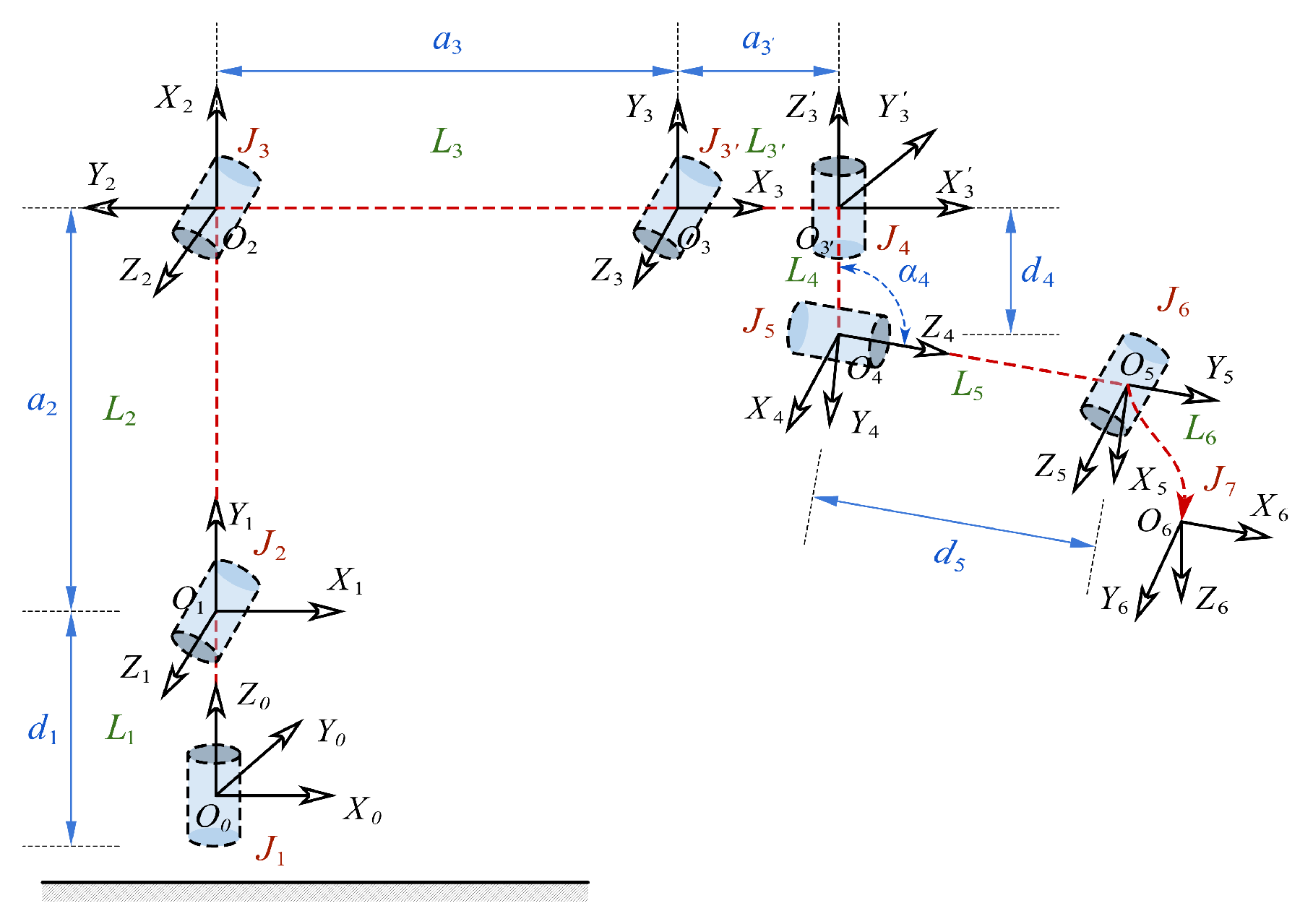
2.1.2. Kinematic Modeling of the Puncture Arm
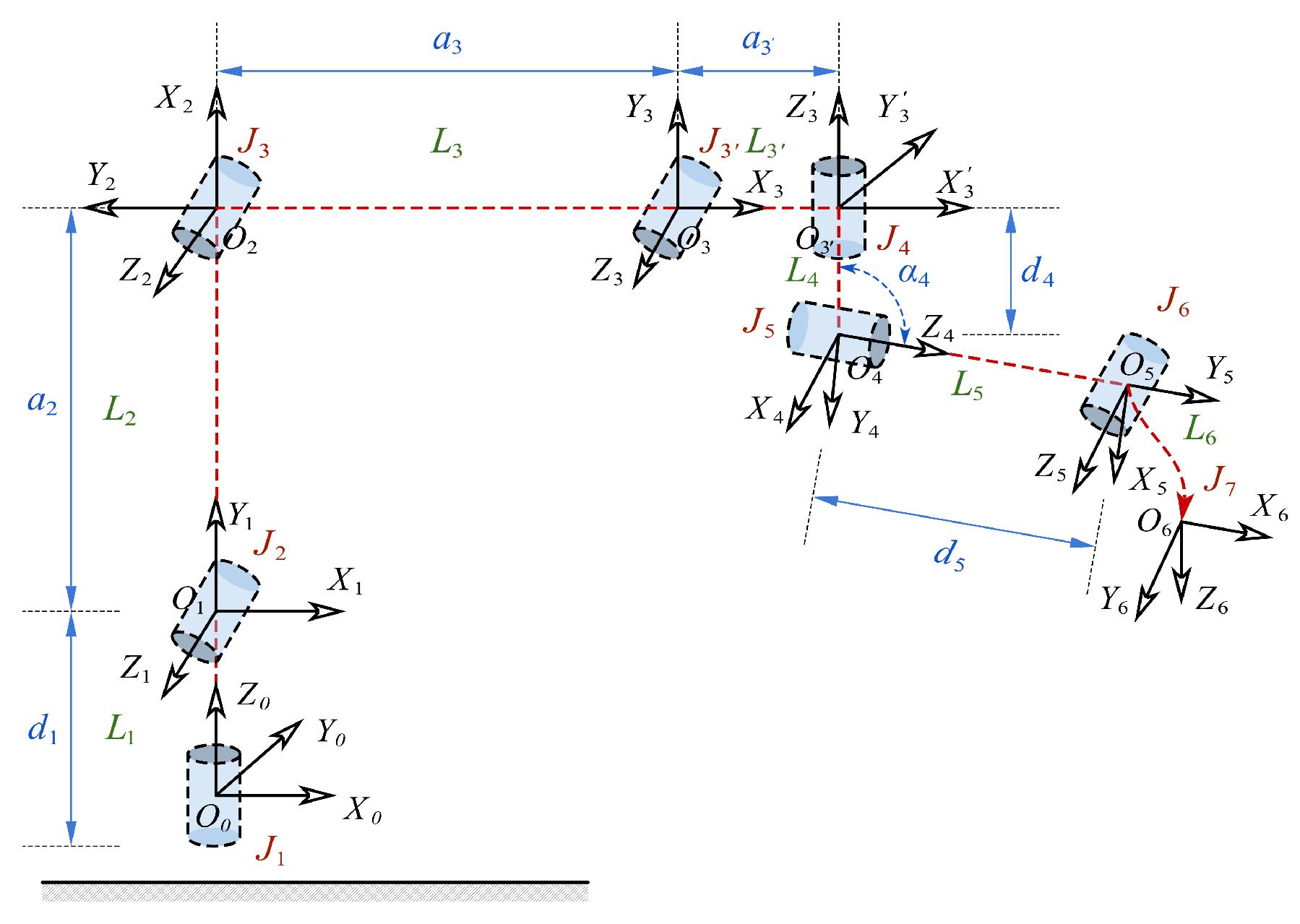
2.2. Mechanical Design and Kinematic Modeling of Scanning Arm
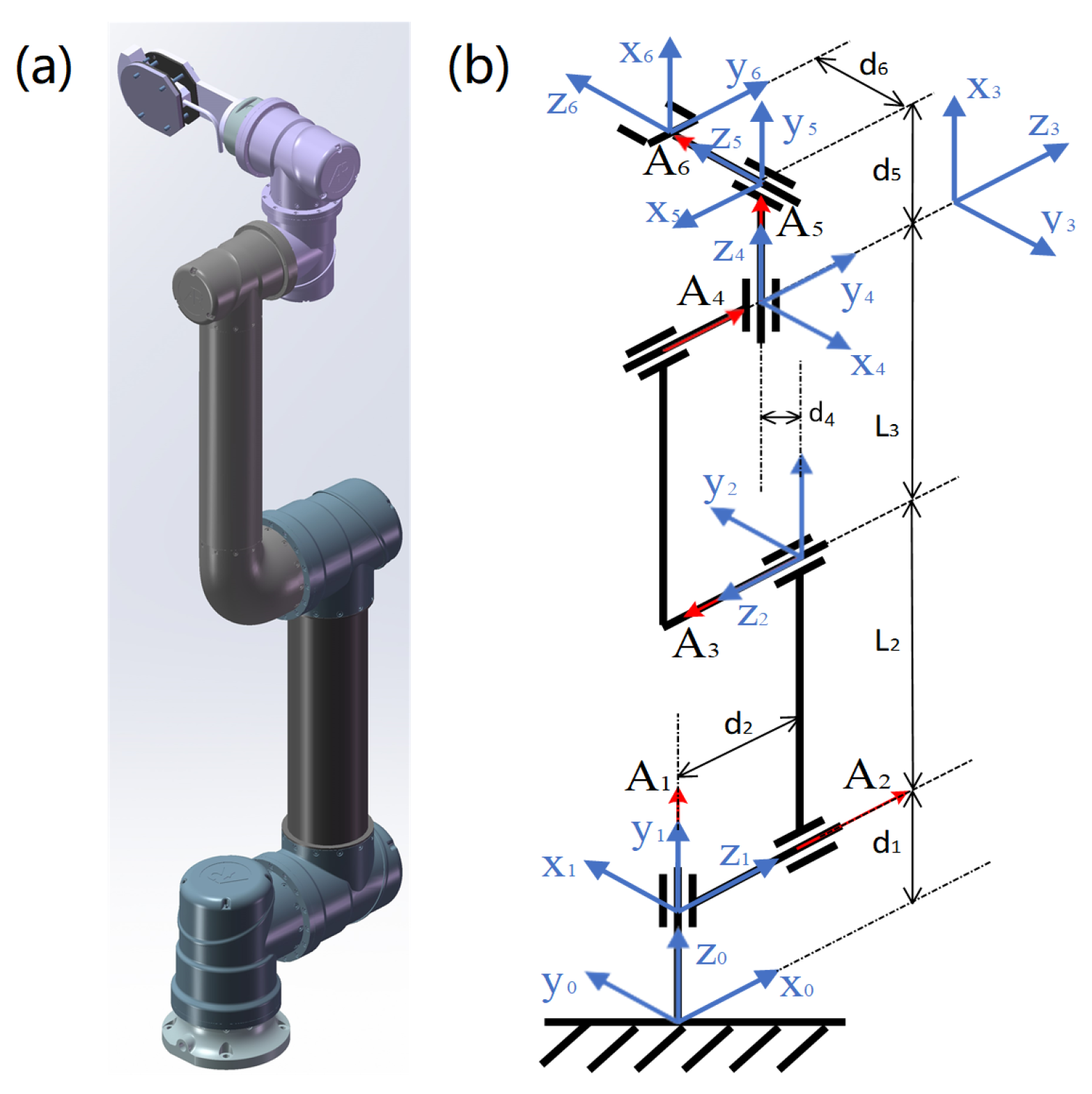
2.2.1. Mechanical Design of Scanning Arm
2.2.2. Kinematic Modeling of Scanning Arm
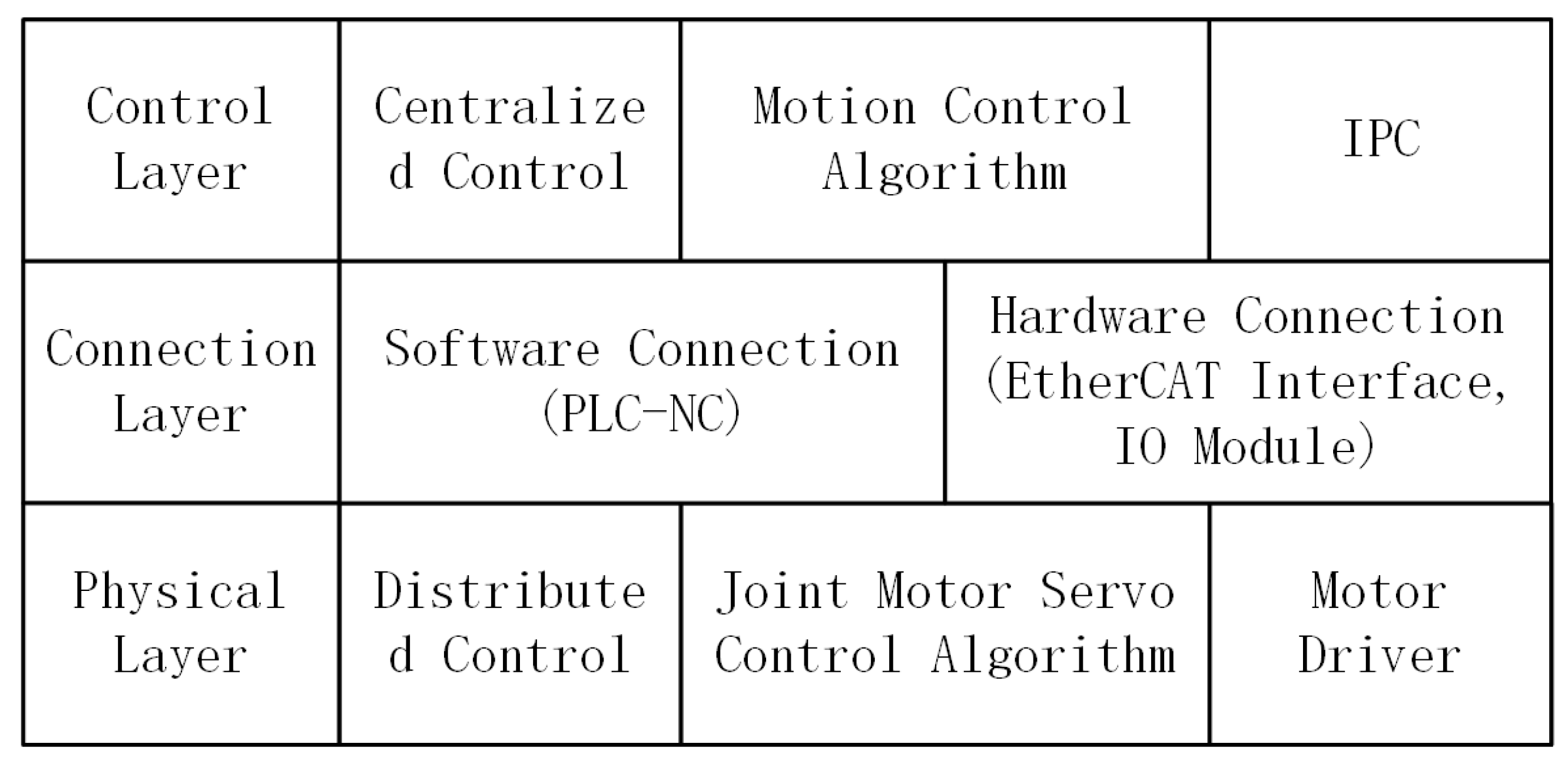
3. The Implementation of the Control System
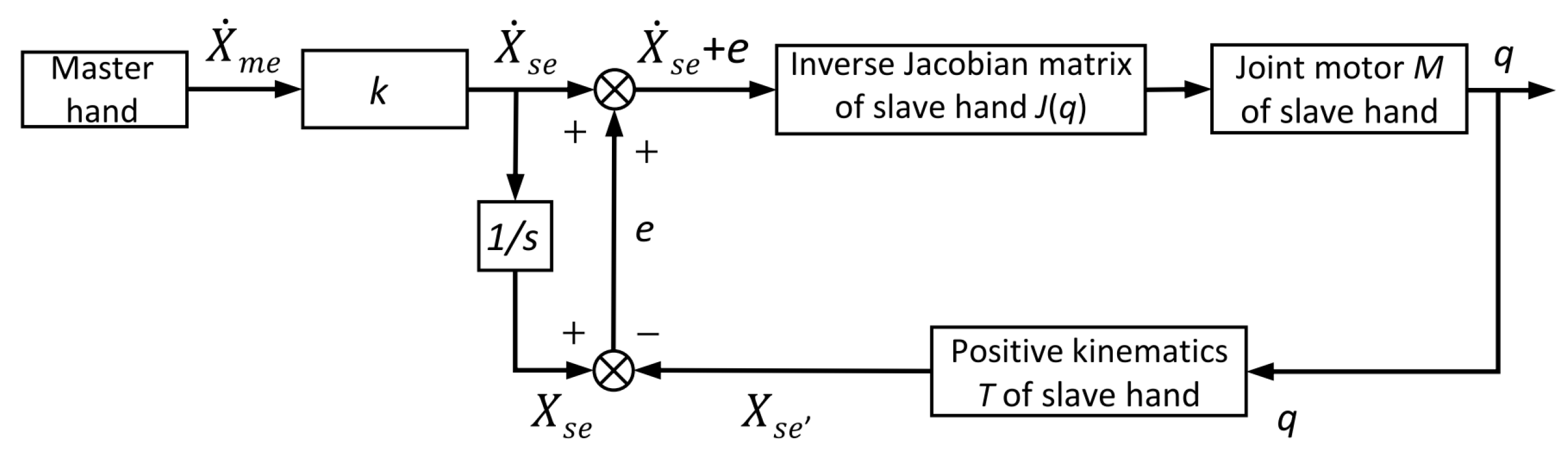
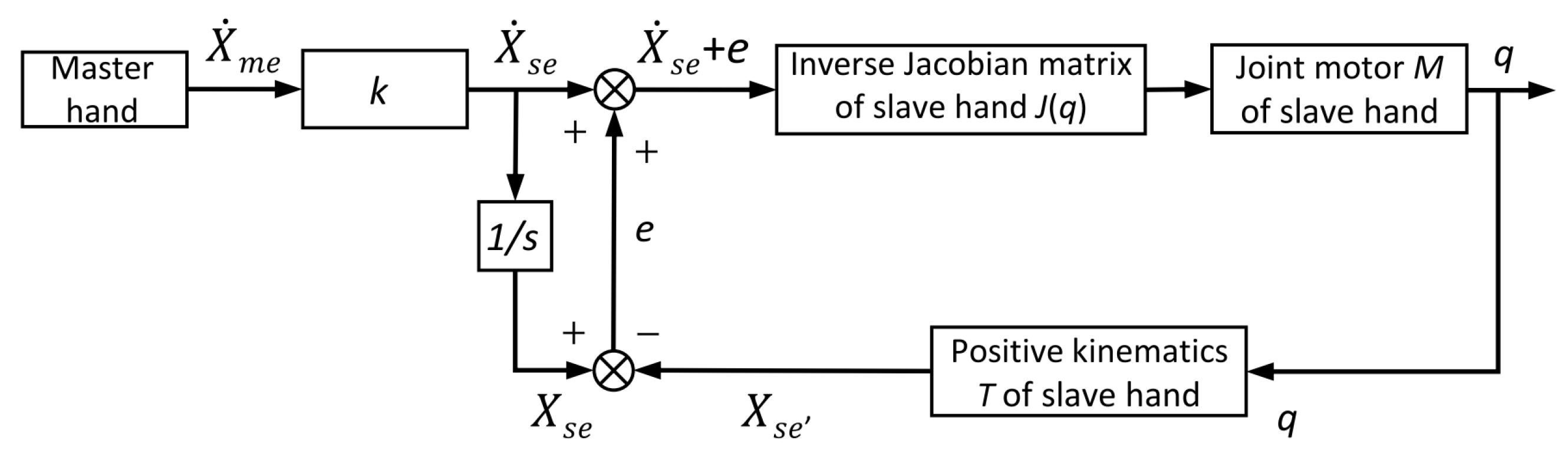
3.1. Master–Slave Control Strategy
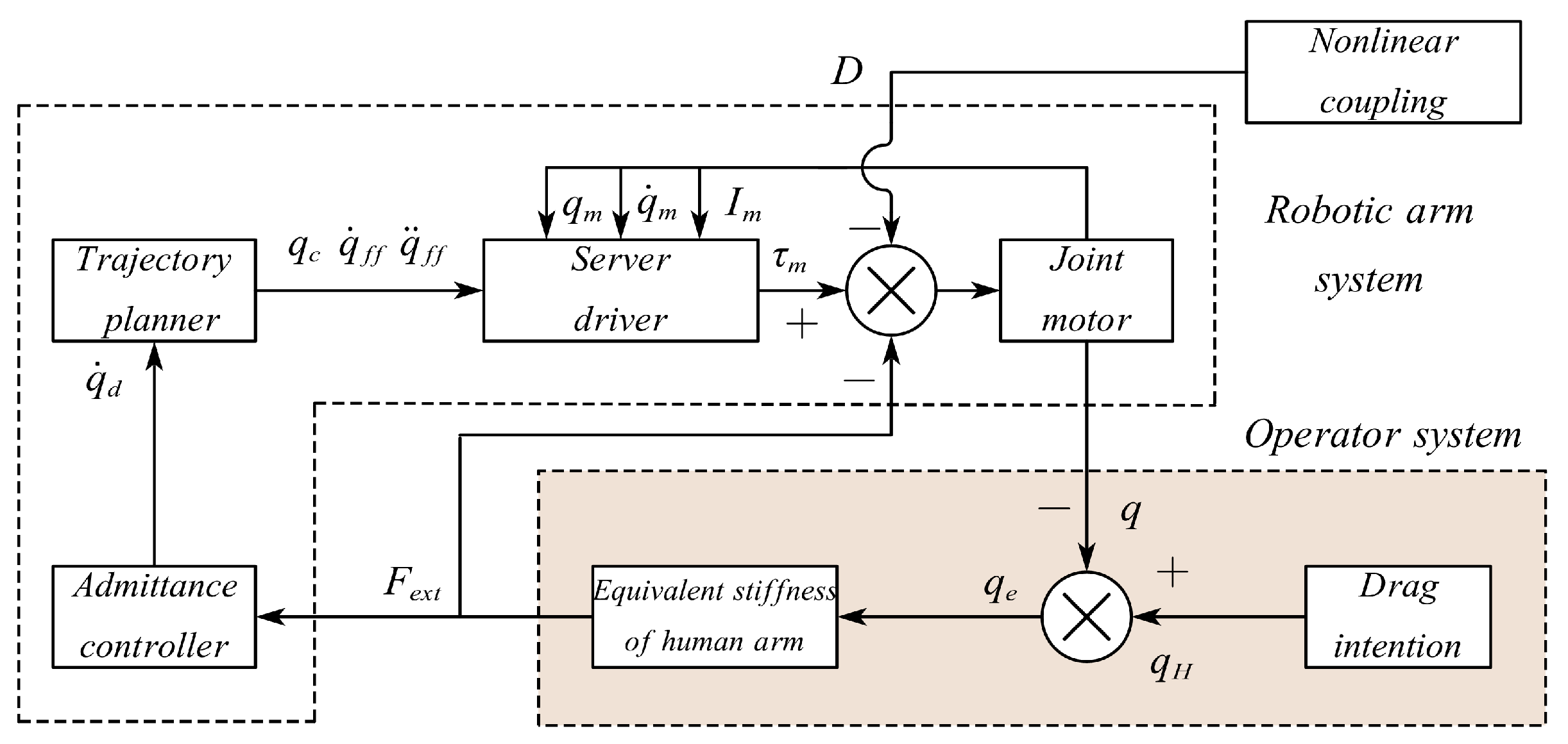
3.2. Control Strategy for Positioning during Docking
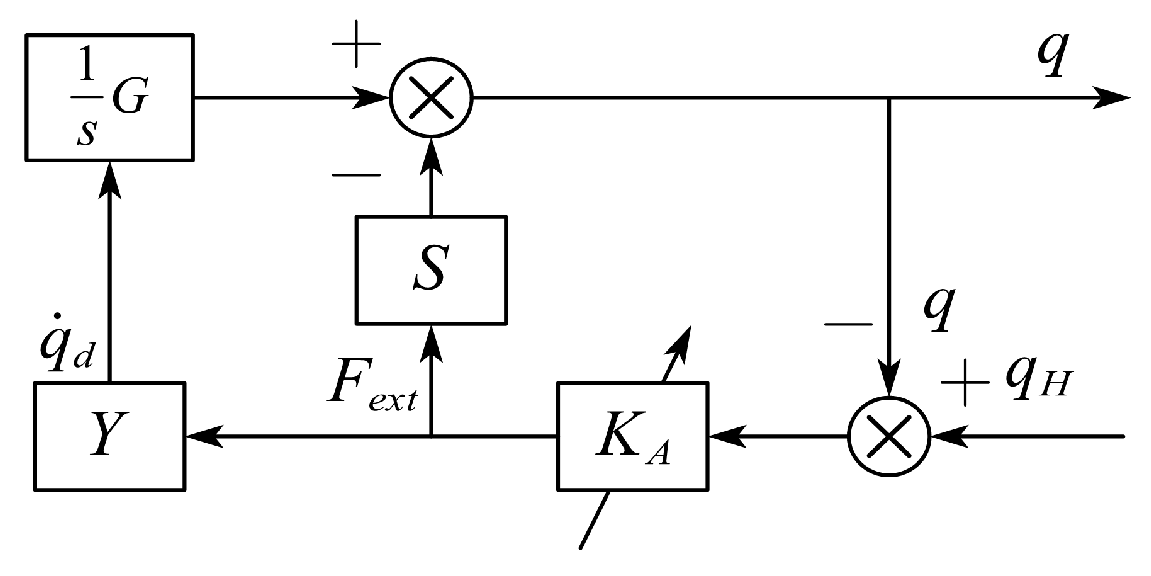
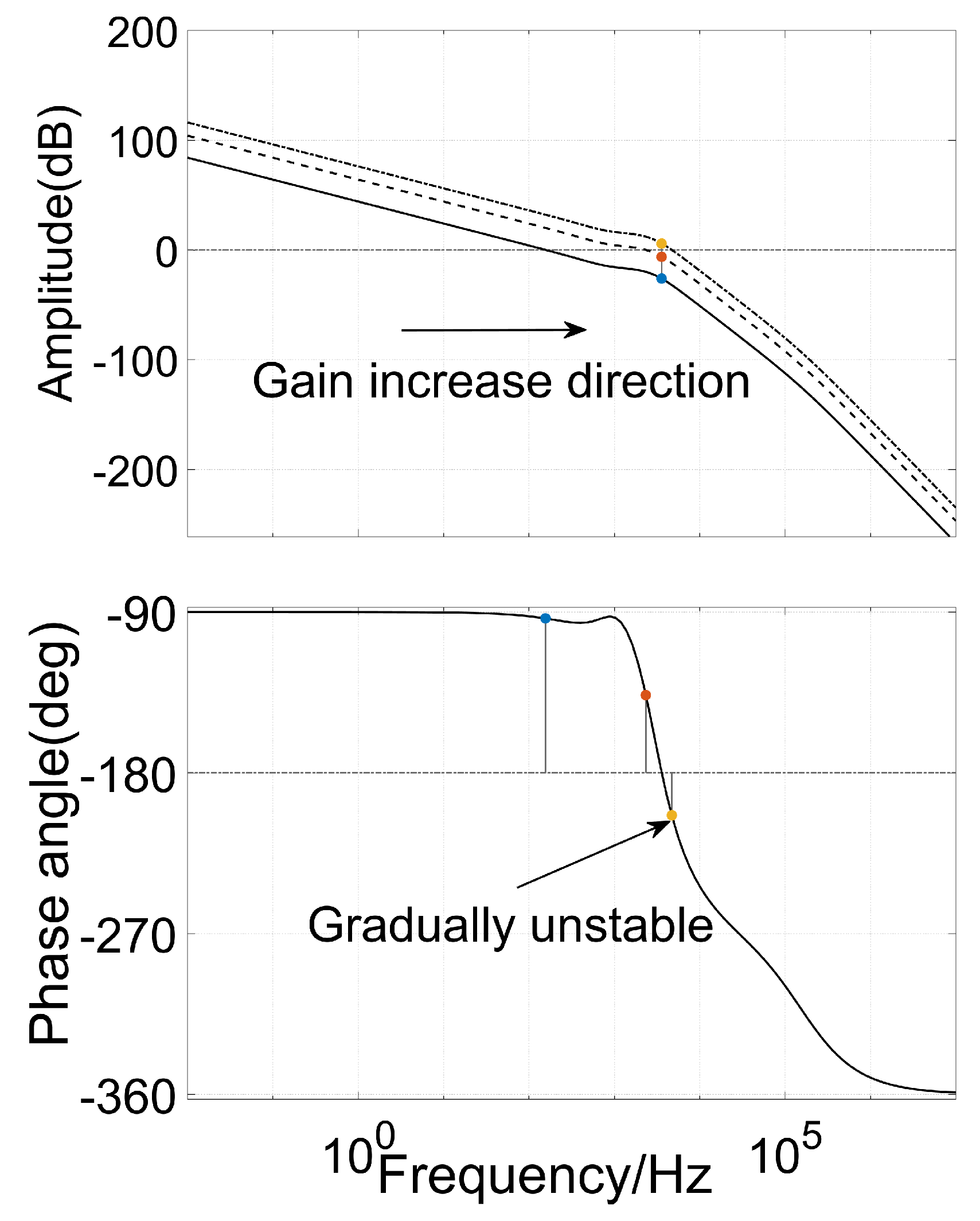
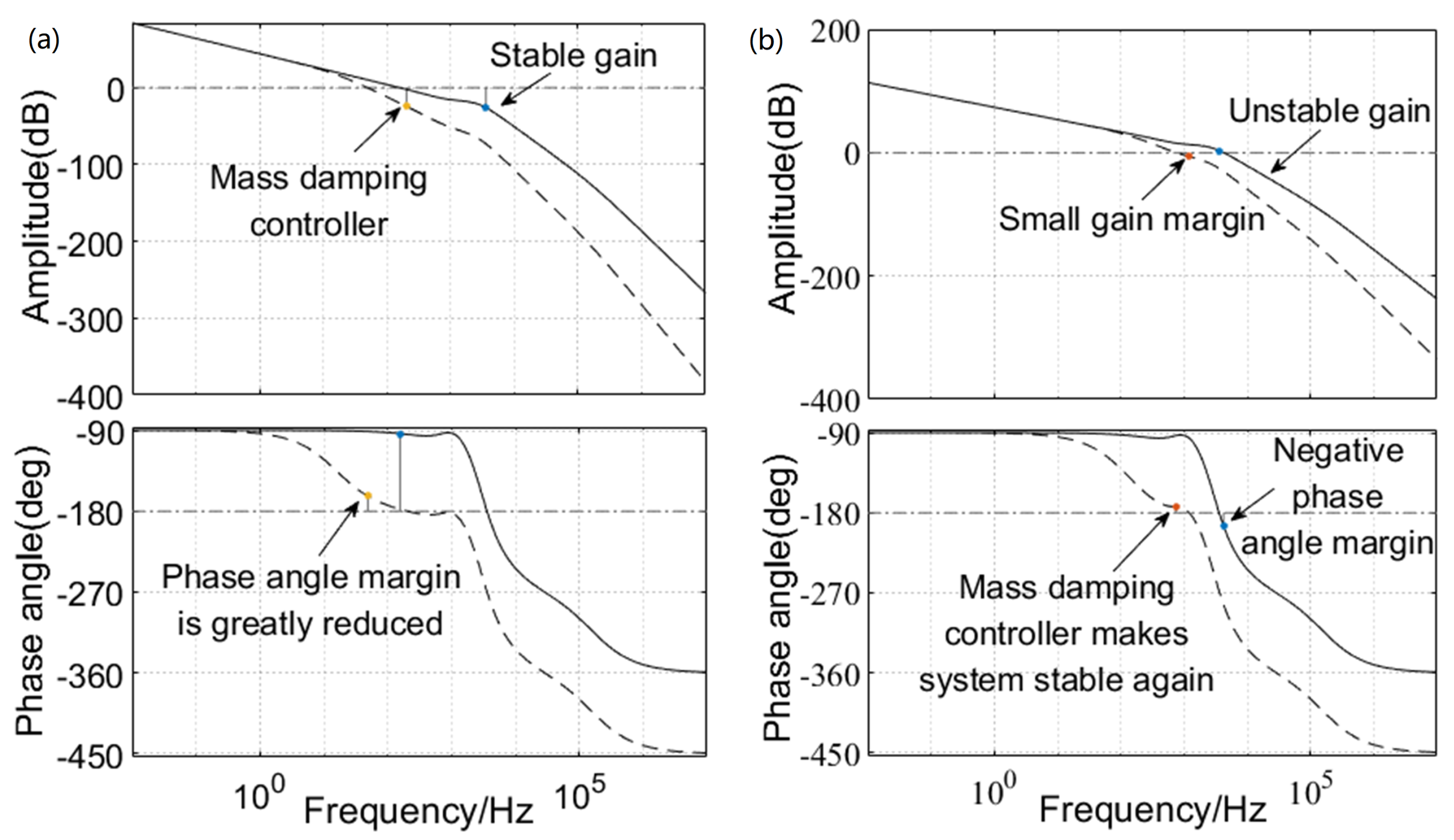
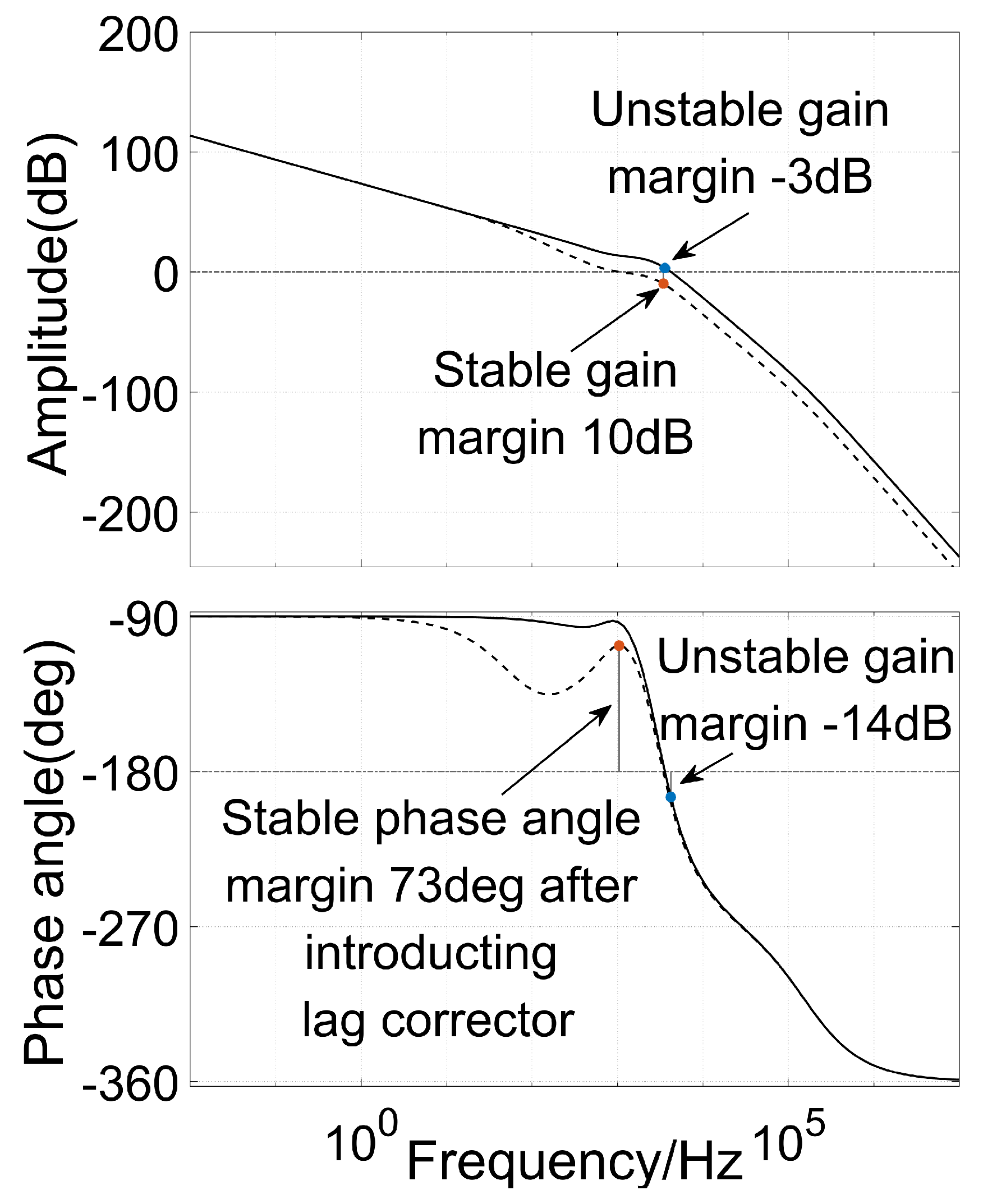
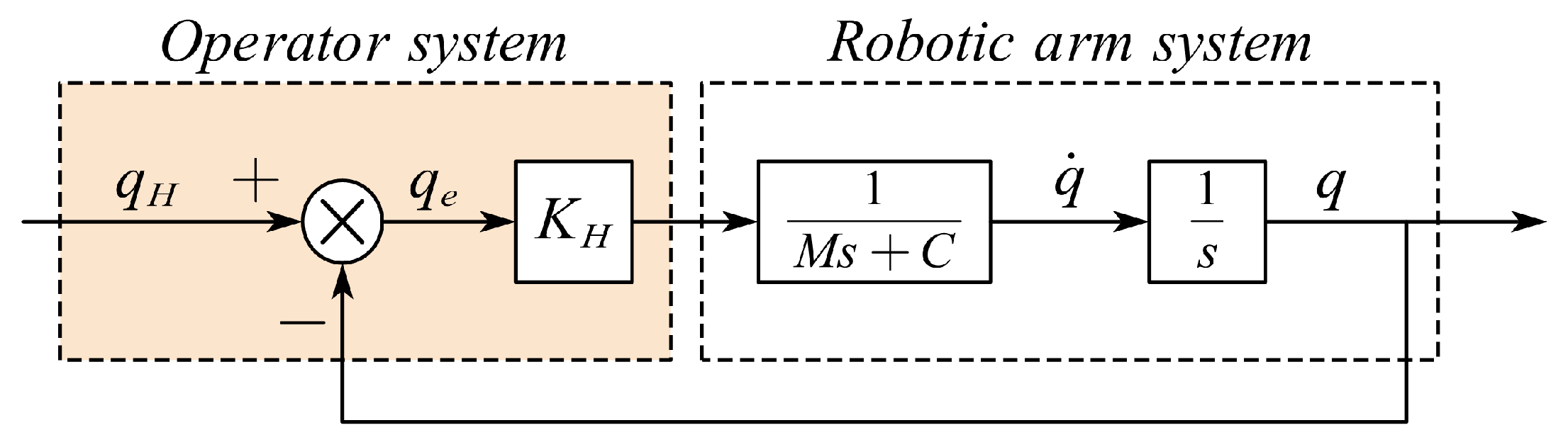
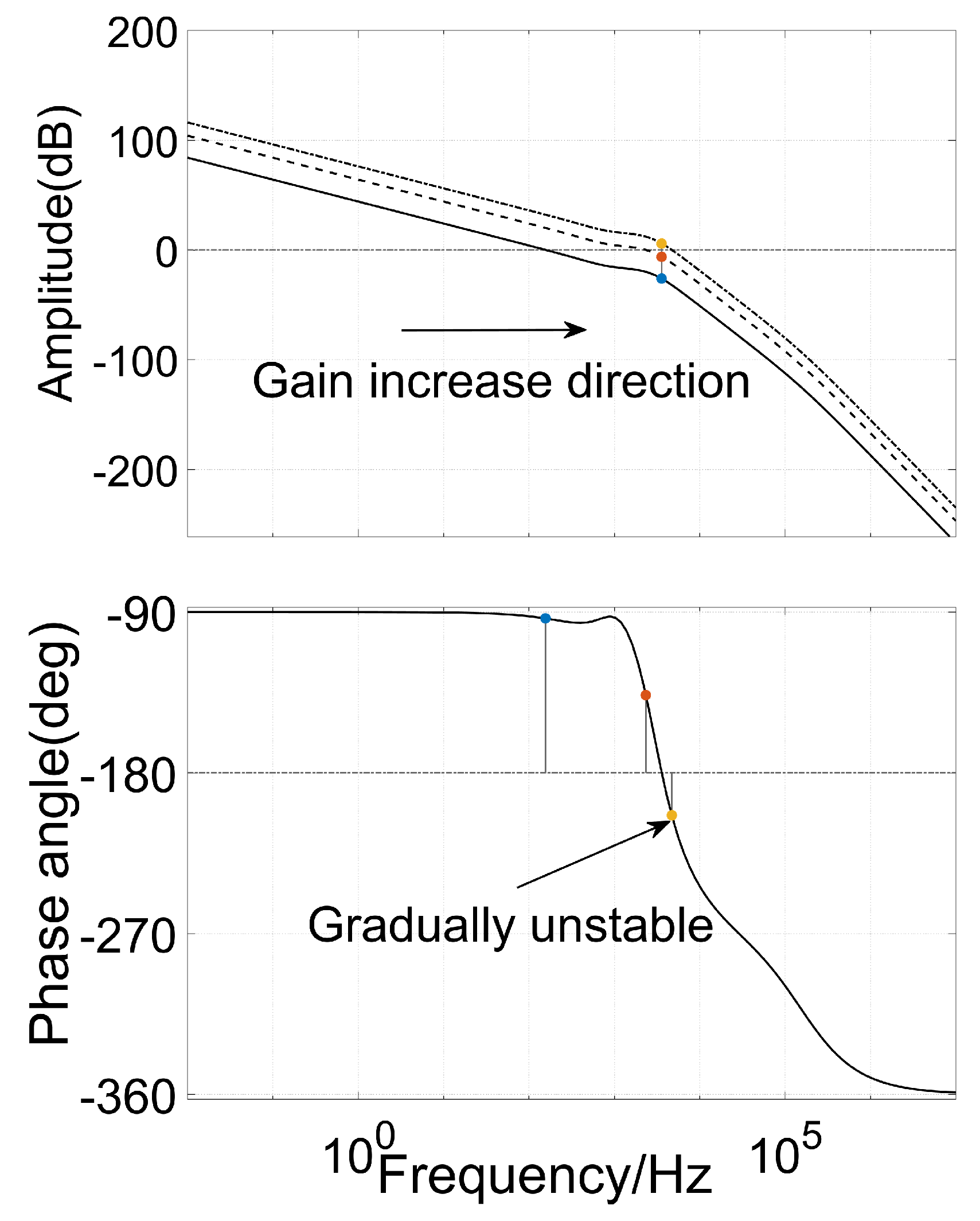
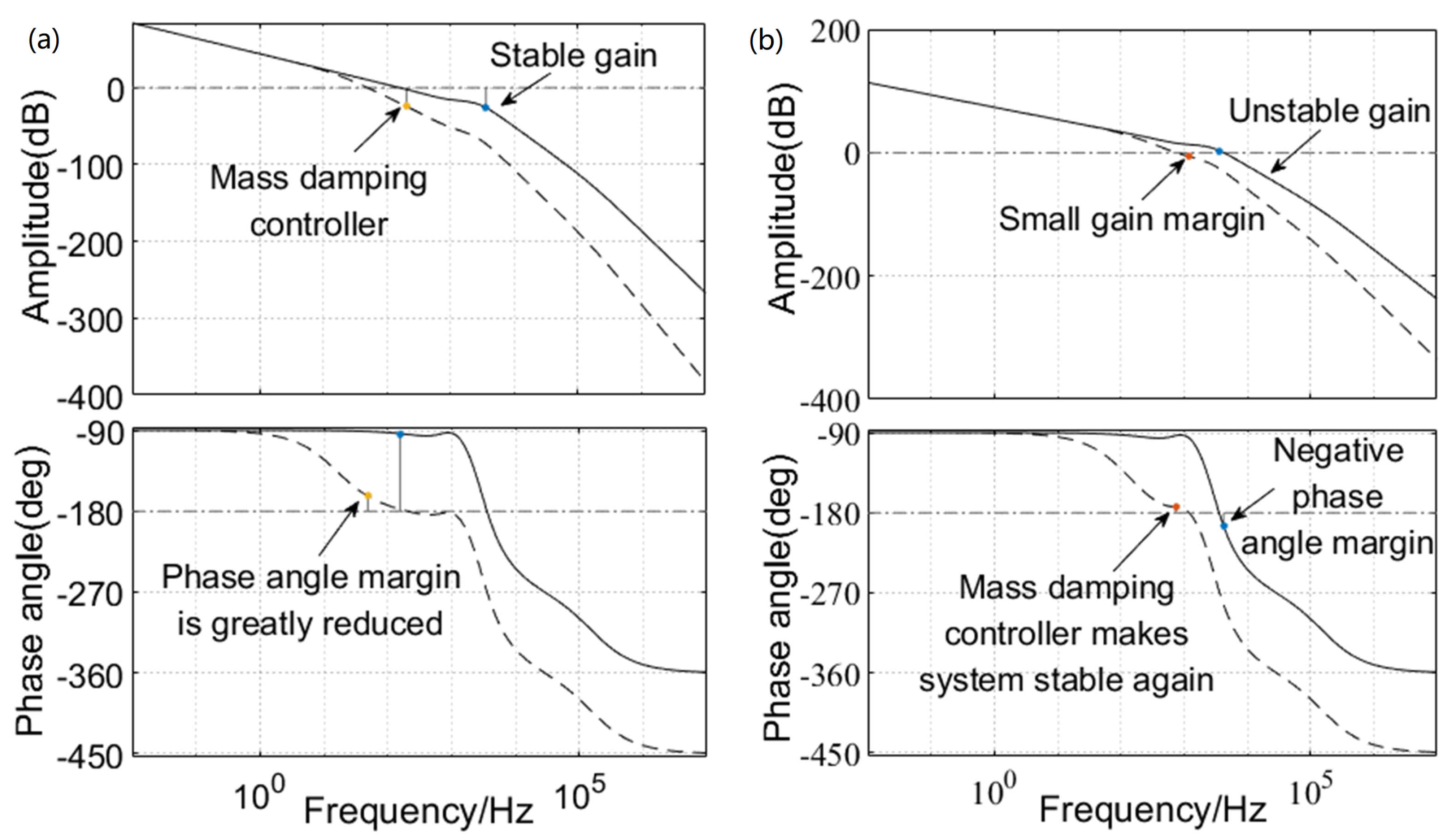
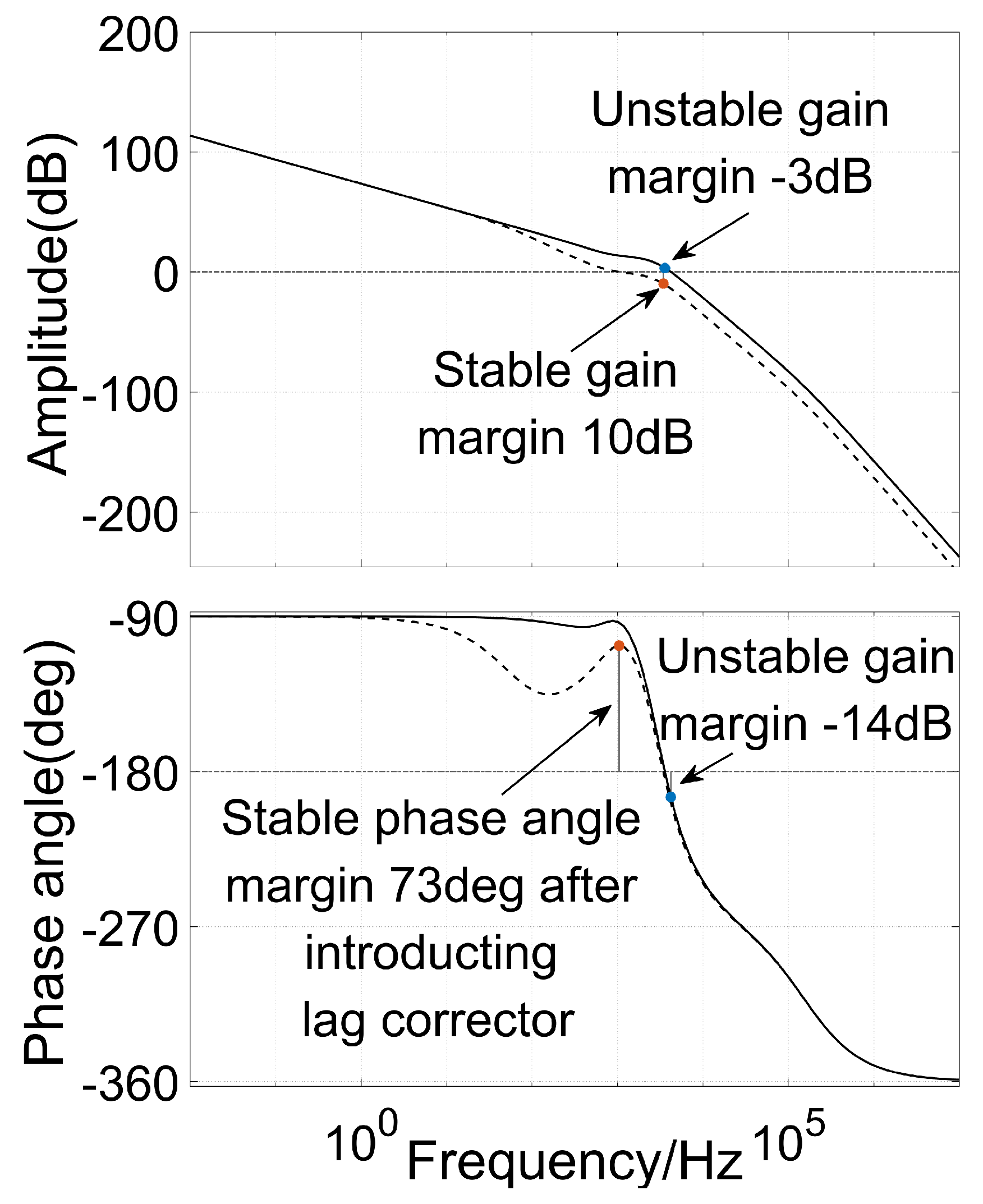
3.2.1. Design of Mass Damping Controller
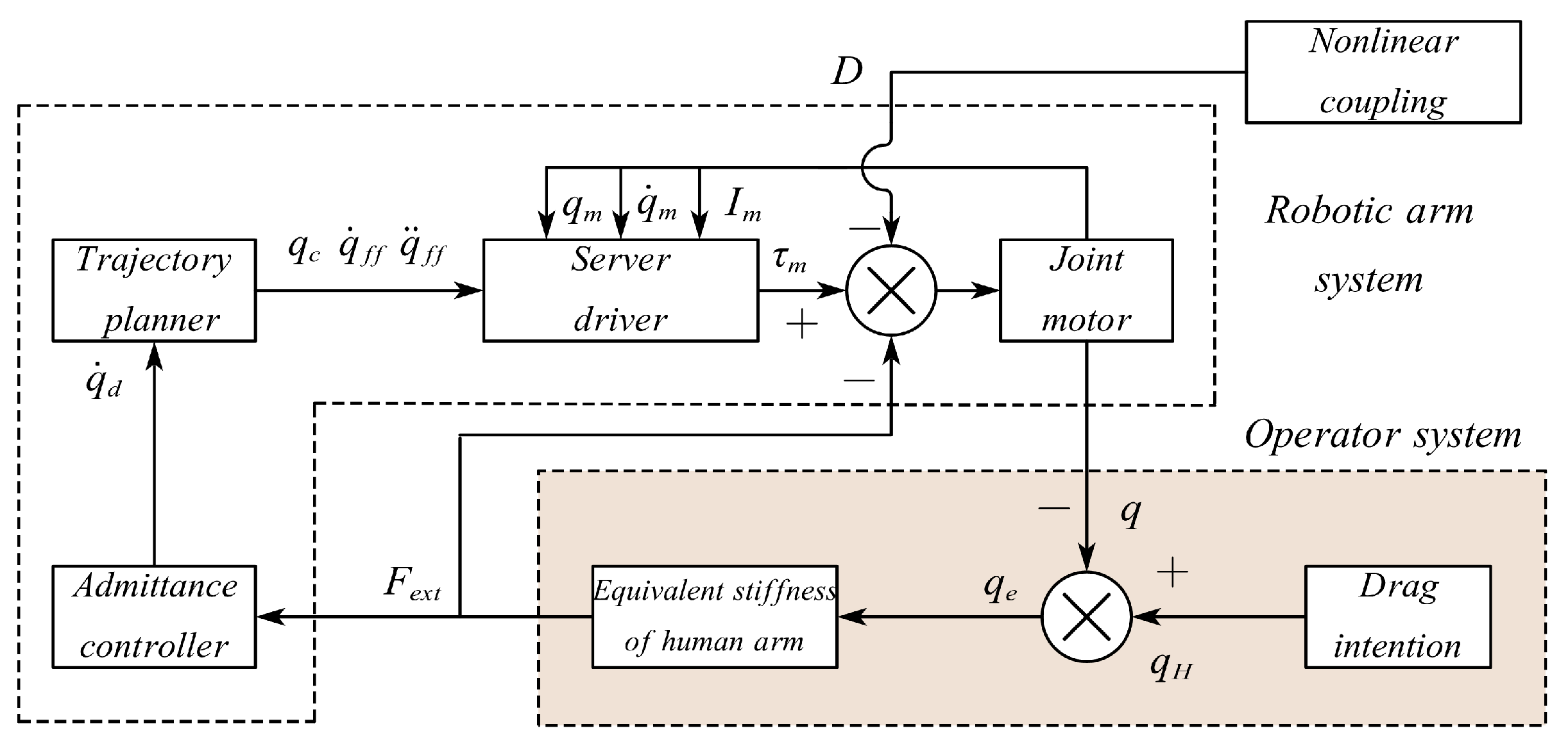
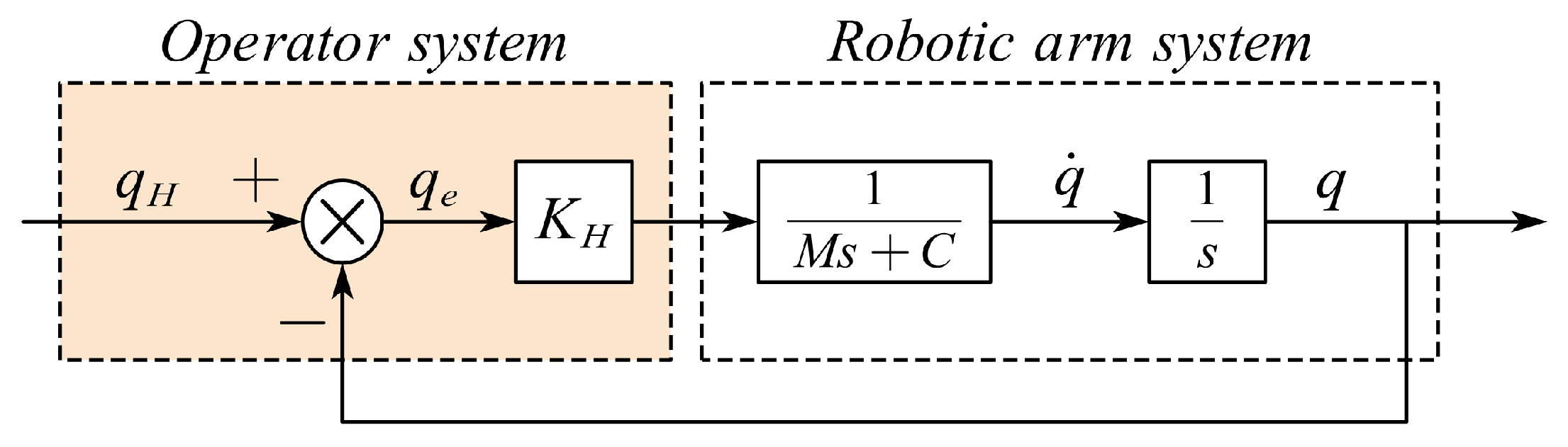
3.2.2. Design of Human–Computer Interactive Admittance Controller
3.3. Joint Gravity Moment Modeling and Parameter Identification
4. System Simulations and Animal Tests
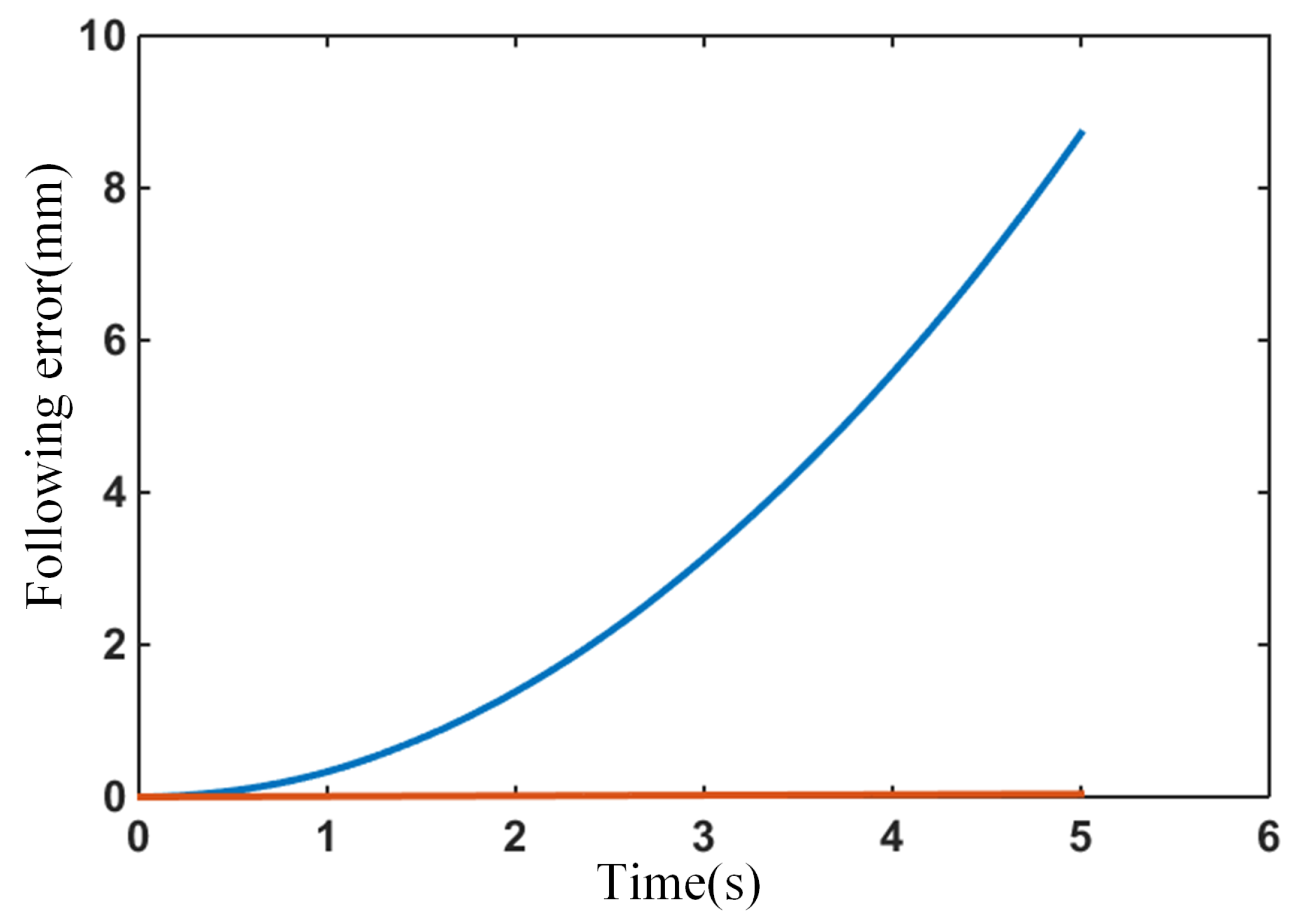
4.1. Master–Slave Control Algorithm Simulation
4.2. Simulation of Admittance Controller for Arm Positioning
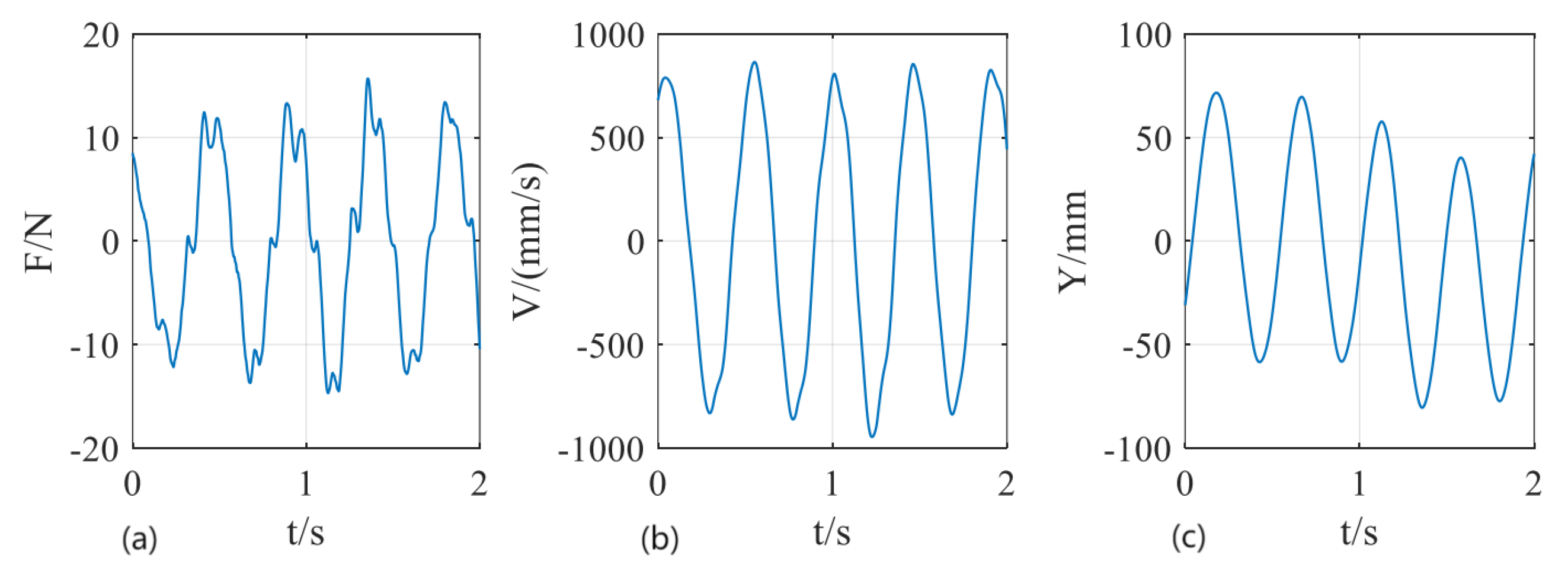
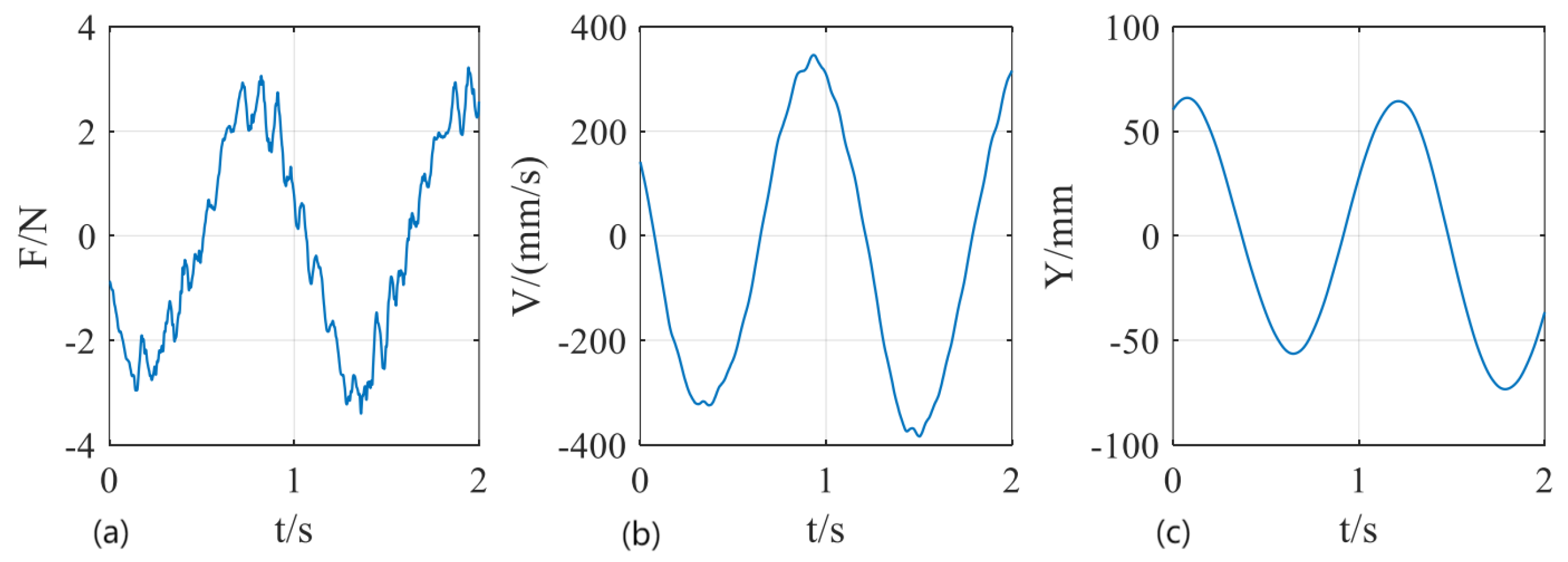
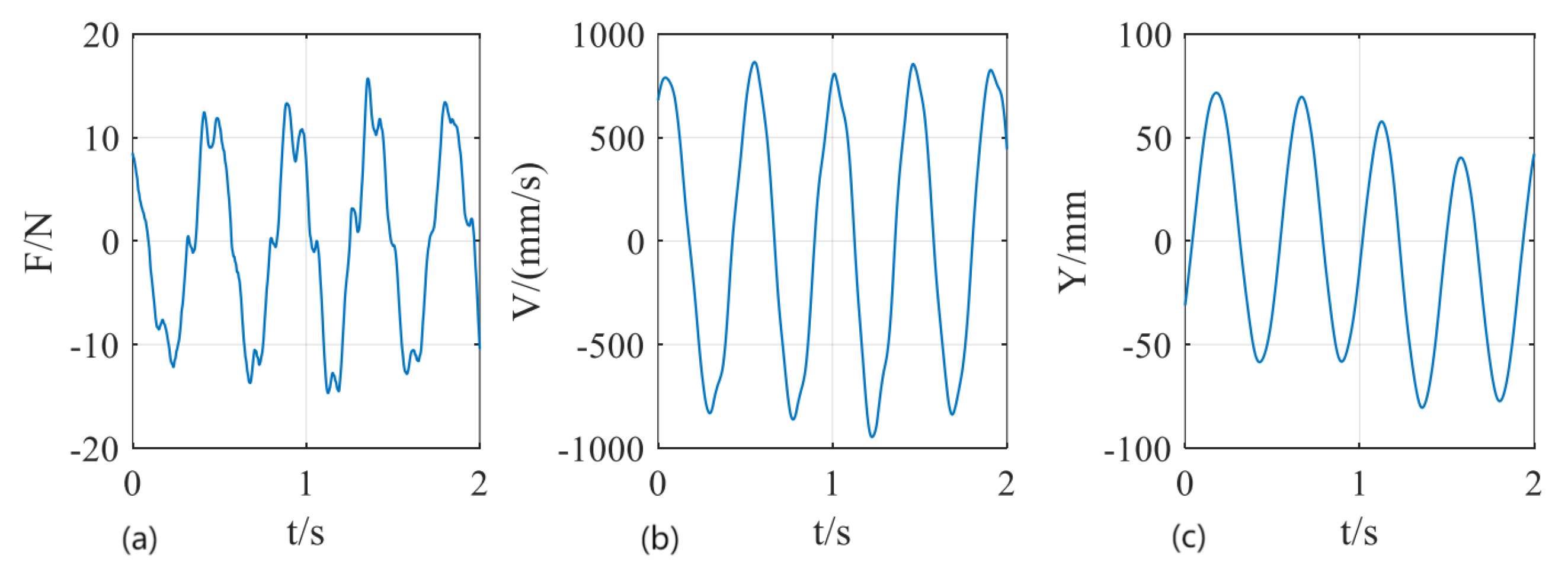
4.3. Cycled Reciprocating Motion of Dragging Tests
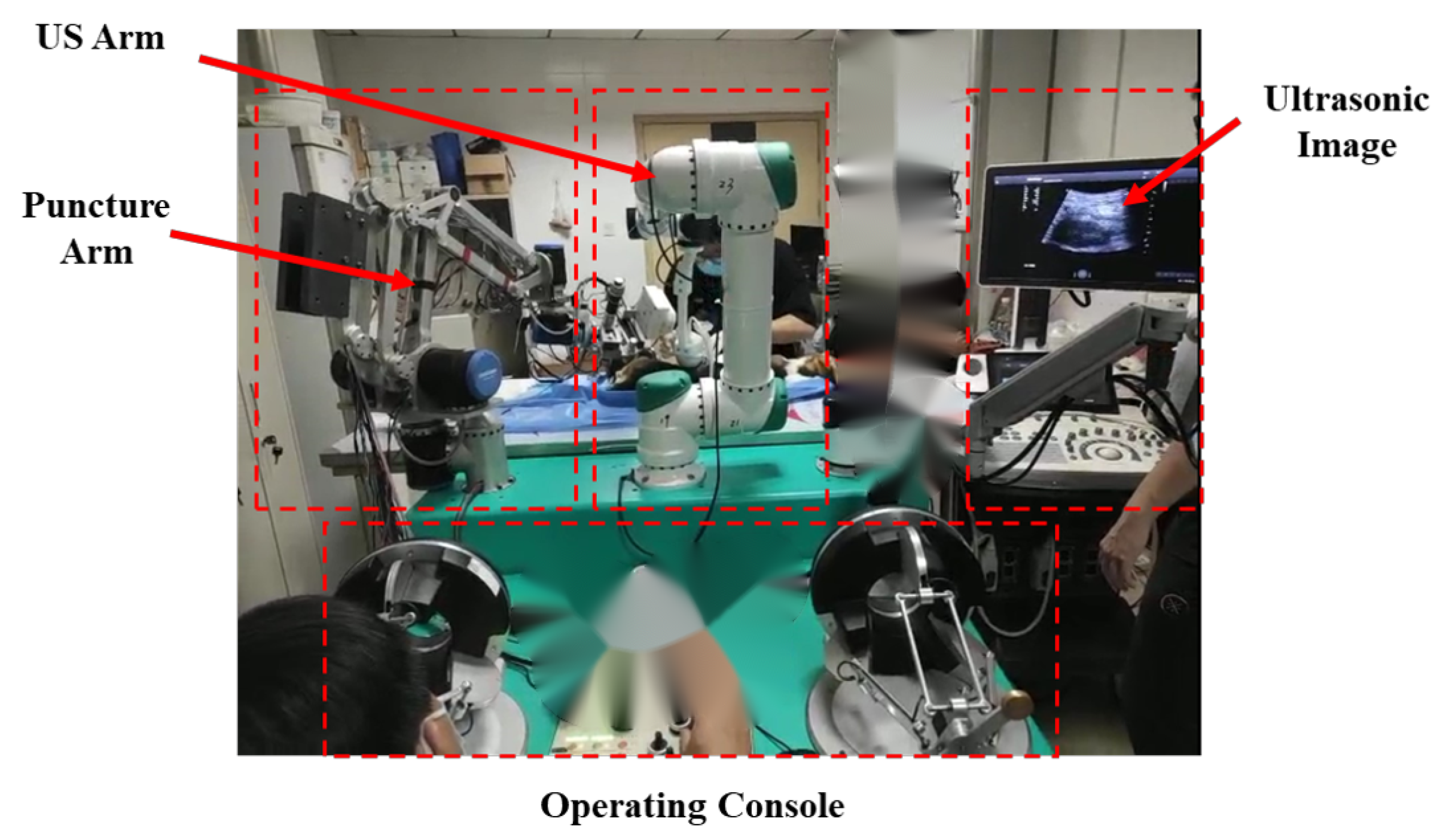
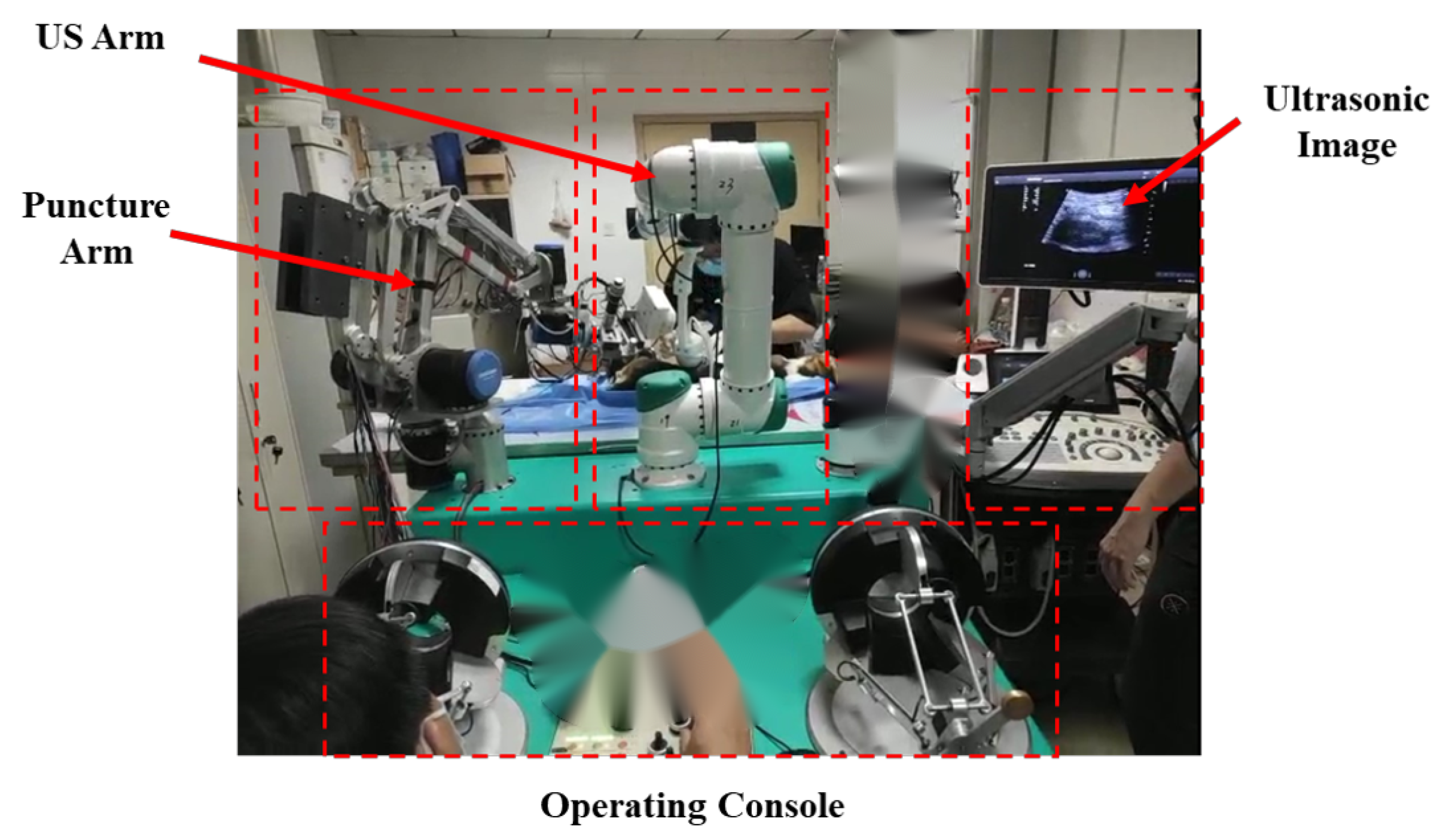
4.4. Animal Tests
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Jun, J.; Yaqing, C.; Yongchang, Z. Analysis of complications in ultrasound-guided percutaneous renal biopsy. Chin. J. Ultrasound Med. 2006, 22, 858–860. [Google Scholar]
- Whittier, W.L.; Korbet, S.M. Timing of complications in percutaneous renal biopsy. J. Am. Soc. Nephrol. 2004, 15, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoianovici, D.; Cleary, K.; Patriciu, A.; Mazilu, D.; Stanimir, A.; Craciunoiu, N.; Watson, V.; Kavoussi, L. AcuBot: A robot for radiological interventions. IEEE Trans. Robot. Autom. 2003, 19, 927–930. [Google Scholar] [CrossRef]
- Stoianovici, D.; Jun, C.; Lim, S.; Li, P.; Petrisor, D.; Fricke, S.; Sharma, K.; Cleary, K. Multi-imager compatible, MR safe, remote center of motion needle-guide robot. IEEE Trans. Biomed. Eng. 2017, 65, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, B.; Koo, J.; Iordachita, I.; Kazanzides, P.; Kapoor, A.; Handa, J.; Hager, G.; Taylor, R. Development and application of a new steady-hand manipulator for retinal surgery. In Proceedings of the 2007 IEEE International Conference on Robotics and Automation, Rome, Italy, 10–14 April 2007; pp. 623–629. [Google Scholar]
- Üneri, A.; Balicki, M.A.; Handa, J.; Gehlbach, P.; Taylor, R.H.; Iordachita, I. New steady-hand eye robot with micro-force sensing for vitreoretinal surgery. In Proceedings of the 2010 3rd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Tokyo, Japan, 26–29 September 2010; pp. 814–819. [Google Scholar]
- He, X.; Roppenecker, D.; Gierlach, D.; Balicki, M.; Olds, K.; Gehlbach, P.; Handa, J.; Taylor, R.; Iordachita, I. Toward clinically applicable steady-hand eye robot for vitreoretinal surgery. In Proceedings of the ASME International Mechanical Engineering Congress and Exposition, Houston, TX, USA, 9–15 November 2012; Volume 45189, pp. 145–153. [Google Scholar]
- Kettenbach, J.; Kronreif, G. Robotic systems for percutaneous needle-guided interventions. Minim. Invasive Ther. Allied Technol. 2015, 24, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Thiruvalluvan, K.; Krzeminski, L.; Moore, W.H.; Xu, Z.; Liang, Z. CT-guided robotic needle biopsy of lung nodules with respiratory motion—Experimental system and preliminary test. Int. J. Med. Robot. Comput. Assist. Surg. 2013, 9, 317–330. [Google Scholar] [CrossRef] [PubMed]
- Hungr, N.; Bricault, I.; Cinquin, P.; Fouard, C. Design and validation of a CT-and MRI-guided robot for percutaneous needle procedures. IEEE Trans. Robot. 2016, 32, 973–987. [Google Scholar] [CrossRef]
- Patel, N.A.; Azimi, E.; Monfaredi, R.; Sharma, K.; Cleary, K.; Iordachita, I. Robotic system for MRI-guided shoulder arthrography: Accuracy evaluation. In Proceedings of the 2018 International Symposium on Medical Robotics (ISMR), Atlanta, GA, USA, 1–3 March 2018; pp. 1–6. [Google Scholar]
- Stoianovici, D.; Kim, C.; Srimathveeravalli, G.; Sebrecht, P.; Petrisor, D.; Coleman, J.; Solomon, S.B.; Hricak, H. MRI-Safe Robot for Endorectal Prostate Biopsy. IEEE/ASME Trans. Mechatron. 2014, 19, 1289–1299. [Google Scholar] [CrossRef] [Green Version]
- Boctor, E.M.; Fischer, G.; Choti, M.A.; Fichtinger, G.; Taylor, R.H. A dual-armed robotic system for intraoperative ultrasound guided hepatic ablative therapy: A prospective study. In Proceedings of the IEEE International Conference on Robotics and Automation, ICRA’04, New Orleans, LA, USA, 26 April–1 May 2004. [Google Scholar]
- Hong, J.; Dohi, T.; Hashizume, M.; Konishi, K.; Hata, N. An ultrasound-driven needle-insertion robot for percutaneous cholecystostomy. Phys. Med. Biol. 2004, 49, 441–455. [Google Scholar] [CrossRef]
- Kettenbach, J.; Kronreif, G.; Figl, M.; Fürst, M.; Birkfellner, W.; Hanel, R.; Bergmann, H. Robot-assisted biopsy using ultrasound guidance: Initial results from in vitro tests. Eur. Radiol. 2005, 15, 765. [Google Scholar] [CrossRef]
- Bassan, H.; Hayes, T.; Patel, R.V.; Moallem, M. A Novel Manipulator for 3D Ultrasound Guided Percutaneous Needle Insertion. In Proceedings of the IEEE International Conference on Robotics & Automation, Rome, Italy, 10–14 April 2007. [Google Scholar]
- Ghodoussi, M. Robotic surgery-the transatlantic case. In Proceedings of the IEEE International Conference on Robotics & Automation, Washington, DC, USA, 11–15 May 2002. [Google Scholar]
- Marescaux, J.; Rubino, F. The ZEUS robotic system: Experimental and clinical applications. Surg. Clin. N. Am. 2003, 83, 1305–1315. [Google Scholar] [CrossRef]
- Guthart, G.S.; Salisbury, J.K. The IntuitiveTM telesurgery system: Overview and application. In Proceedings of the IEEE International Conference on Robotics & Automation, San Francisco, CA, USA, 24–28 April 2000; pp. 618–621. [Google Scholar]
- Goonewardene, S.S.; Catterwell, R.; Brown, M.; Challacombe, B. Robotic surgery with the Da Vinci Xi: Simultaneous upper and lower tract surgery. J. Robot. Surg. 2016, 11, 373–374. [Google Scholar] [CrossRef]
- Hannaford, B.; Rosen, J.; Friedman, D.W.; King, H.; Roan, P.; Cheng, L.; Glozman, D.; Ma, J.; Kosari, S.N.; White, L. Raven-II: An Open Platform for Surgical Robotics Research. IEEE Trans. Biomed. Eng. 2013, 60, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Konietschke, R.; Hagn, U.; Nickl, M.; Jorg, S.; Hirzinger, G. The DLR MiroSurge—A robotic system for surgery. In Proceedings of the 2009 IEEE International Conference on Robotics and Automation, ICRA’09, Kobe, Japan, 12–17 May 2009. [Google Scholar]
- Hagn, U.; Konietschke, R.; Tobergte, A.; Nickl, M.; Jörg, S.; Kübler, B.; Passig, G.; Gröger, M.; Fröhlich, F.; Seibold, U.; et al. DLR MiroSurge: A versatile system for research in endoscopic telesurgery. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Aksungur, S. Remote Center of Motion (RCM) Mechanisms for Surgical Operations. Int. J. Appl. Math. Electron. Comput. 2015, 3, 119. [Google Scholar] [CrossRef]
- Newman, W.S. Stability and Performance Limits of Interaction Controllers. J. Dyn. Syst. Meas. Control 1992, 114, 563–570. [Google Scholar] [CrossRef]
- Kazerooni, H.; Snyder, T.J. Case Study on Haptic Devices: Human-Induced Instability in Powered Hand Controllers. J. Guid. Control. Dyn. 1995, 18, 108–113. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Link | 1 | 2 | 3 | 3′ | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|
| Link | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Y.; Liu, X.; Zhang, X.; Zhou, Z.; Jiang, W.; Chen, L.; Liu, Z.; Wu, D.; Dong, W. A Dual-Armed Robotic Puncture System: Design, Implementation and Preliminary Tests. Electronics 2022, 11, 740. https://doi.org/10.3390/electronics11050740
Gao Y, Liu X, Zhang X, Zhou Z, Jiang W, Chen L, Liu Z, Wu D, Dong W. A Dual-Armed Robotic Puncture System: Design, Implementation and Preliminary Tests. Electronics. 2022; 11(5):740. https://doi.org/10.3390/electronics11050740
Chicago/Turabian StyleGao, Yongzhuo, Xiaomin Liu, Xu Zhang, Zhanfeng Zhou, Wenhe Jiang, Lei Chen, Zheng Liu, Dongmei Wu, and Wei Dong. 2022. "A Dual-Armed Robotic Puncture System: Design, Implementation and Preliminary Tests" Electronics 11, no. 5: 740. https://doi.org/10.3390/electronics11050740
APA StyleGao, Y., Liu, X., Zhang, X., Zhou, Z., Jiang, W., Chen, L., Liu, Z., Wu, D., & Dong, W. (2022). A Dual-Armed Robotic Puncture System: Design, Implementation and Preliminary Tests. Electronics, 11(5), 740. https://doi.org/10.3390/electronics11050740