
On the Treatment and Diagnosis of Attention Deficit Hyperactivity Disorder with EEG Assistance



Abstract
:1. Introduction
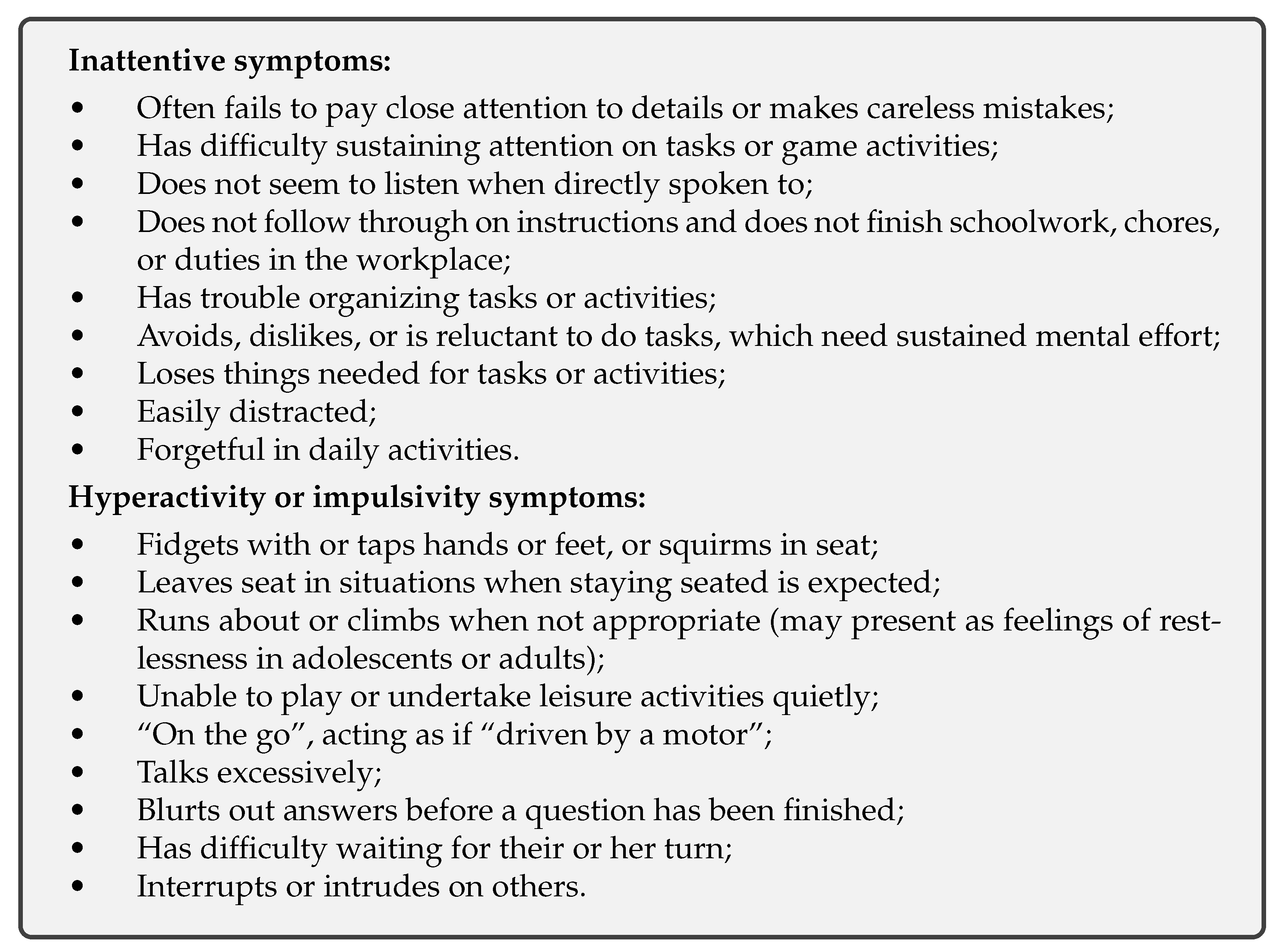
2. Pathology of ADHD
3. Electroencephalography (EEG)
Functional Description
4. Diagnosis and Treatment of ADHD with EEG
5. Potential Approaches for Improvement
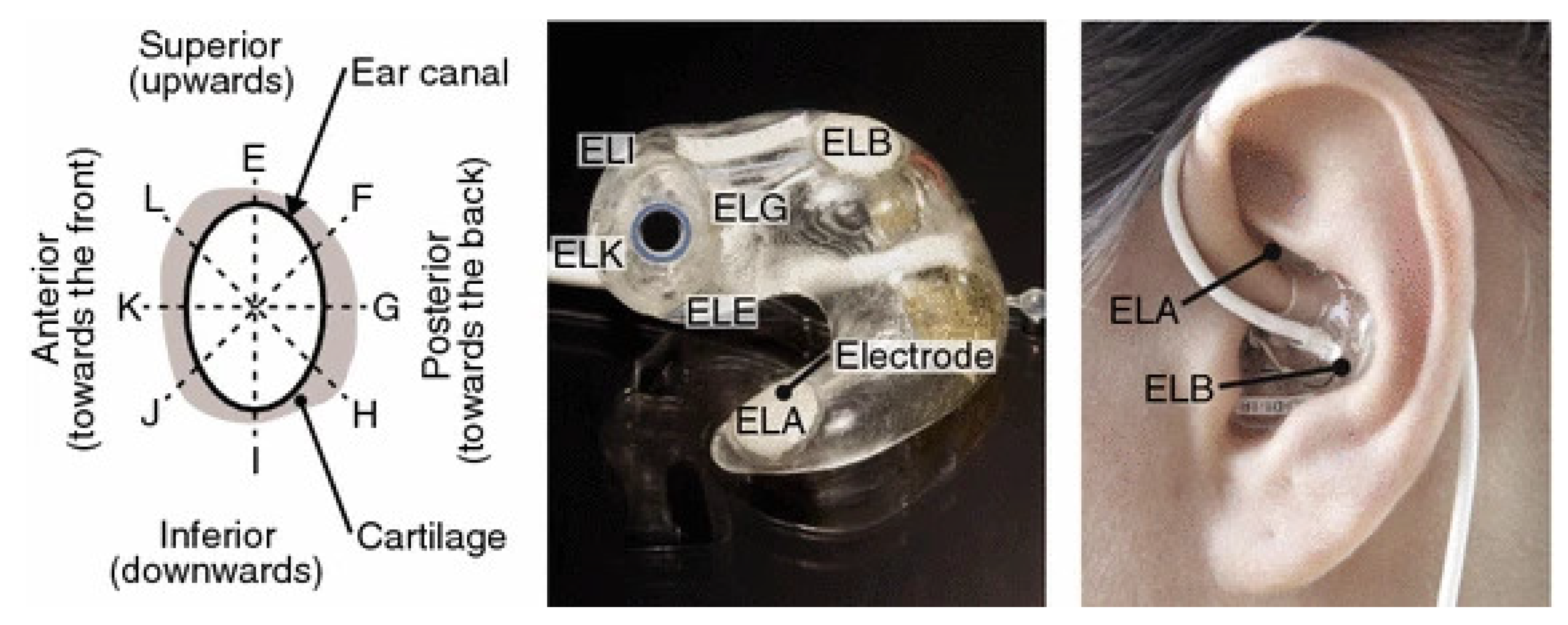
5.1. New Measurement Modes
5.1.1. Nonlinear Features
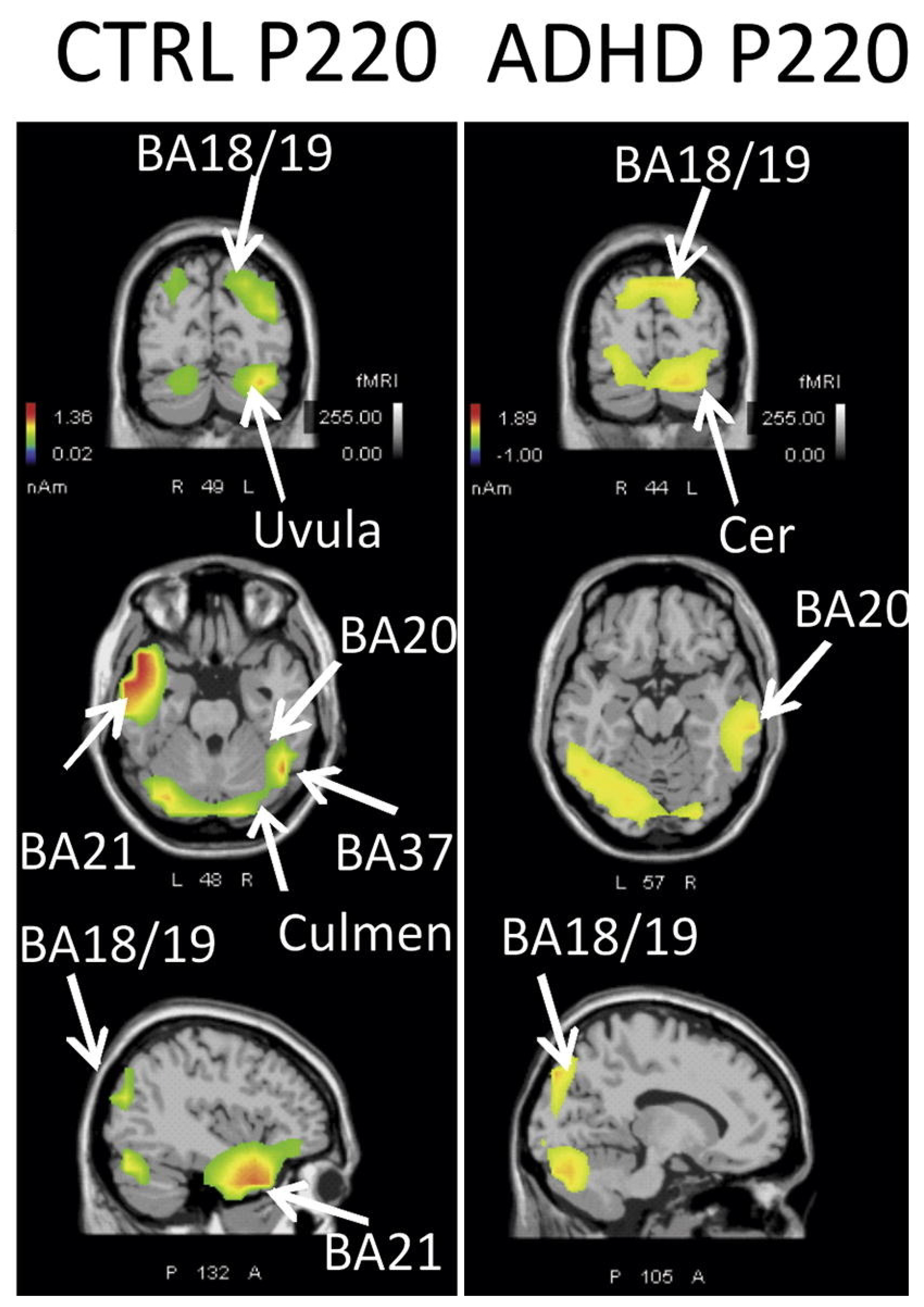
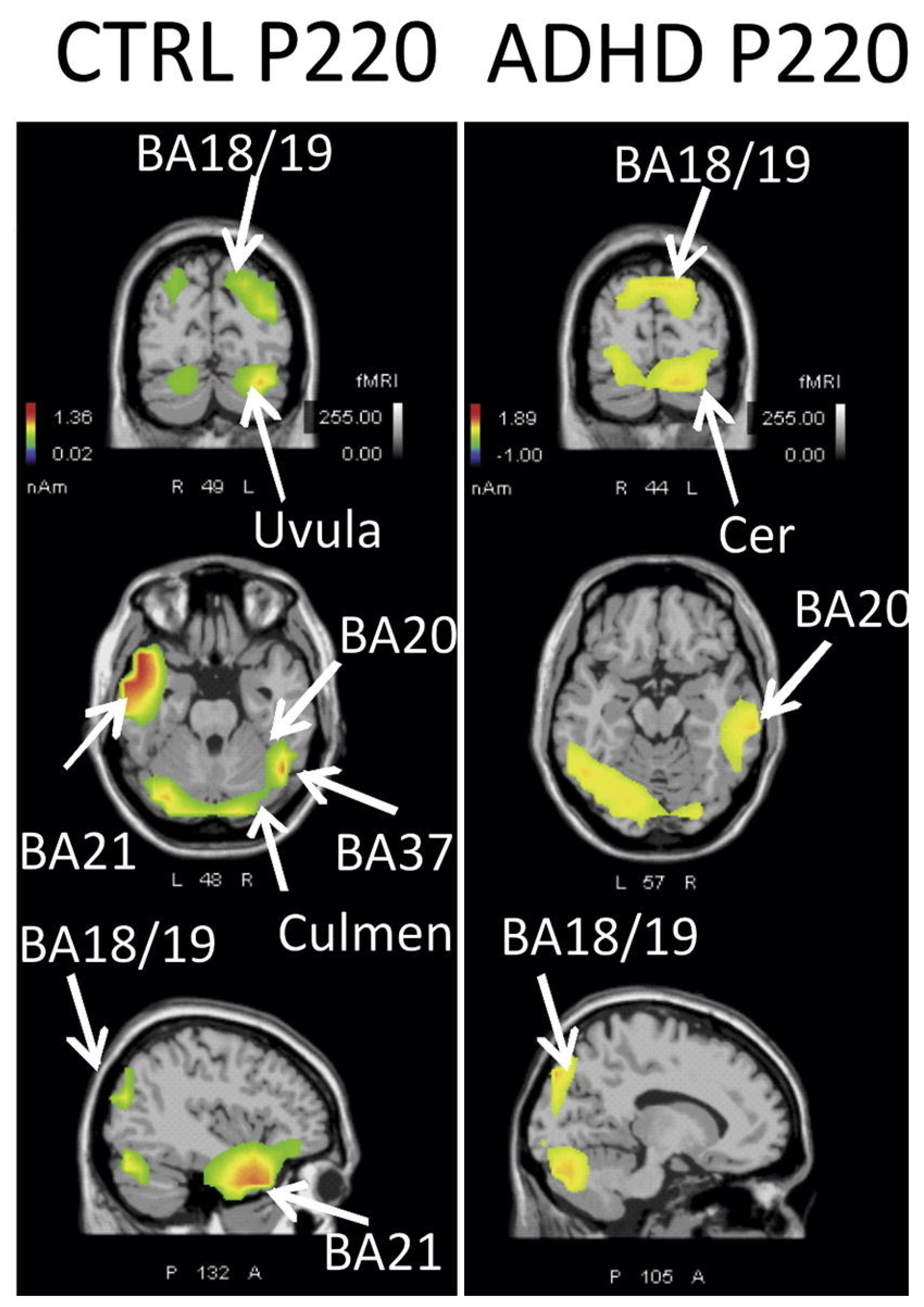
5.1.2. Identification of Neural Mechanisms
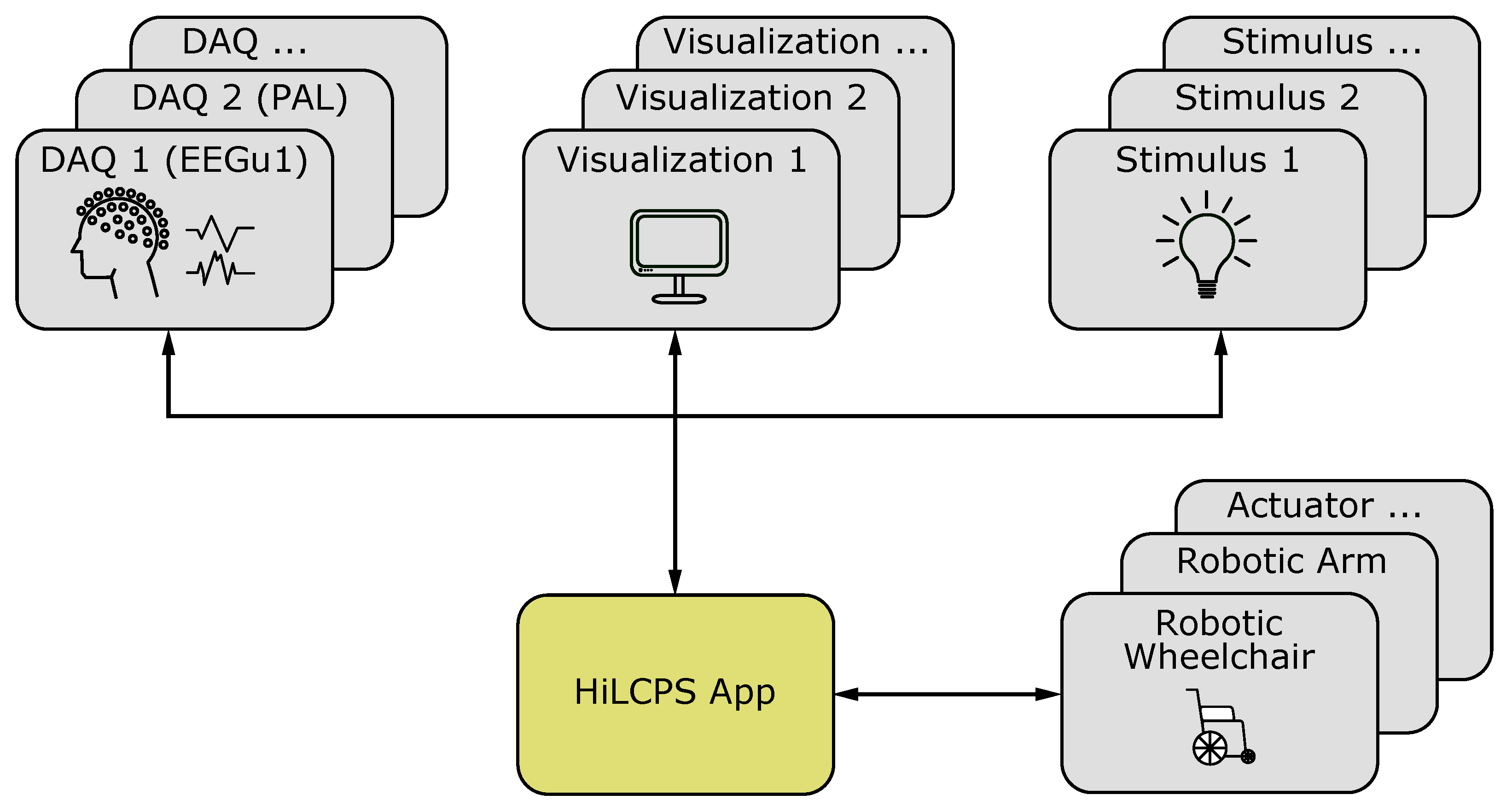
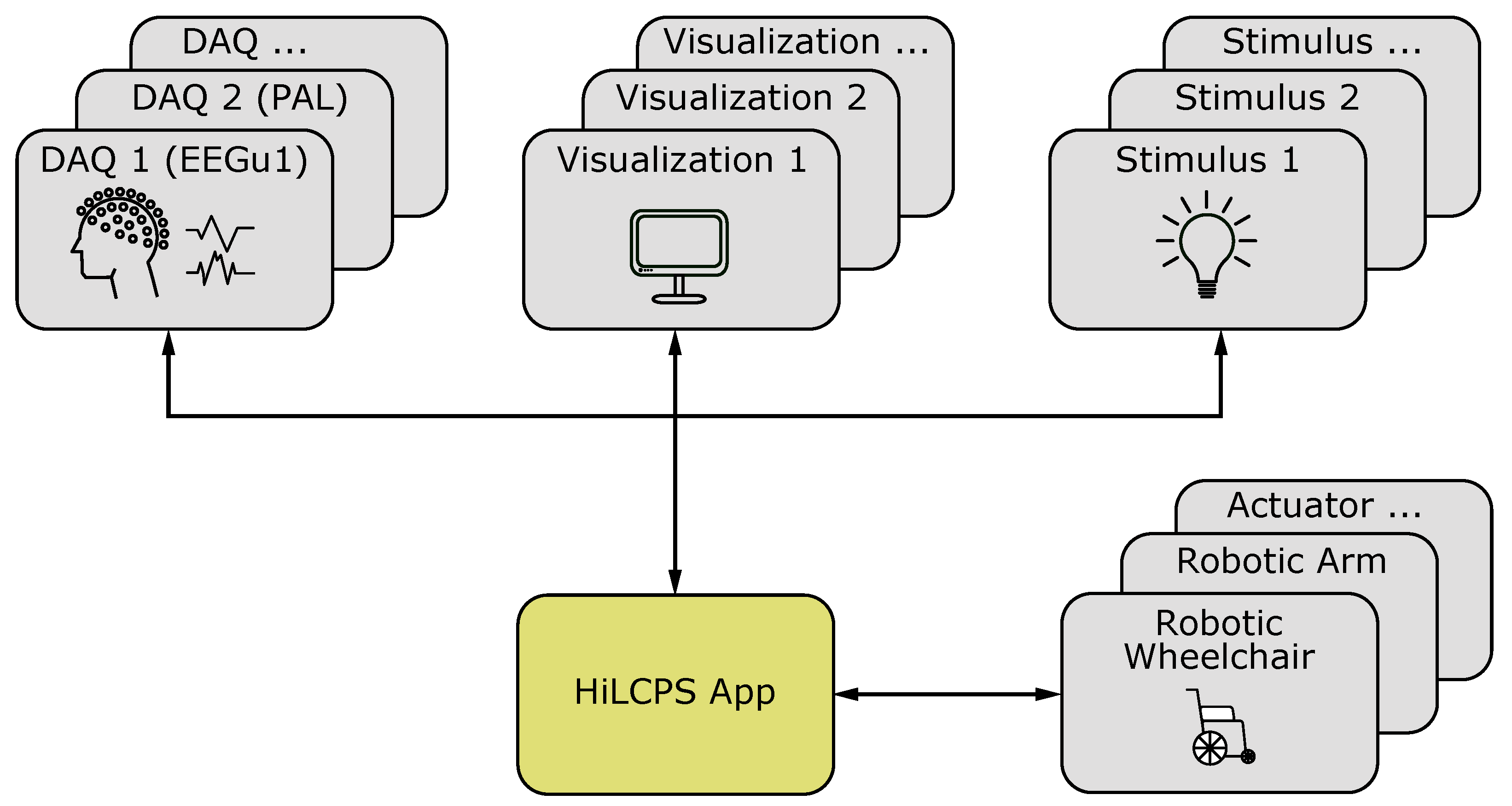
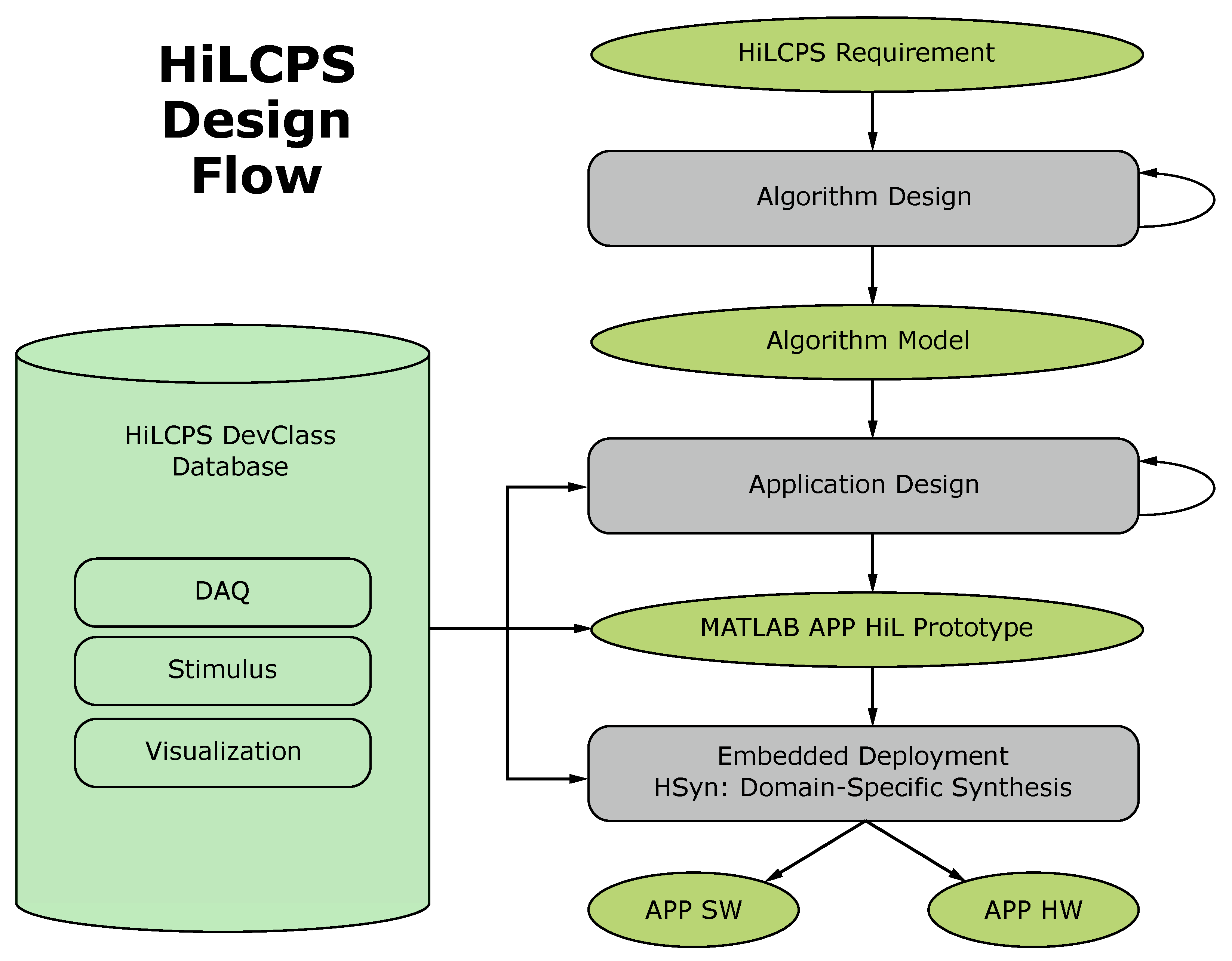
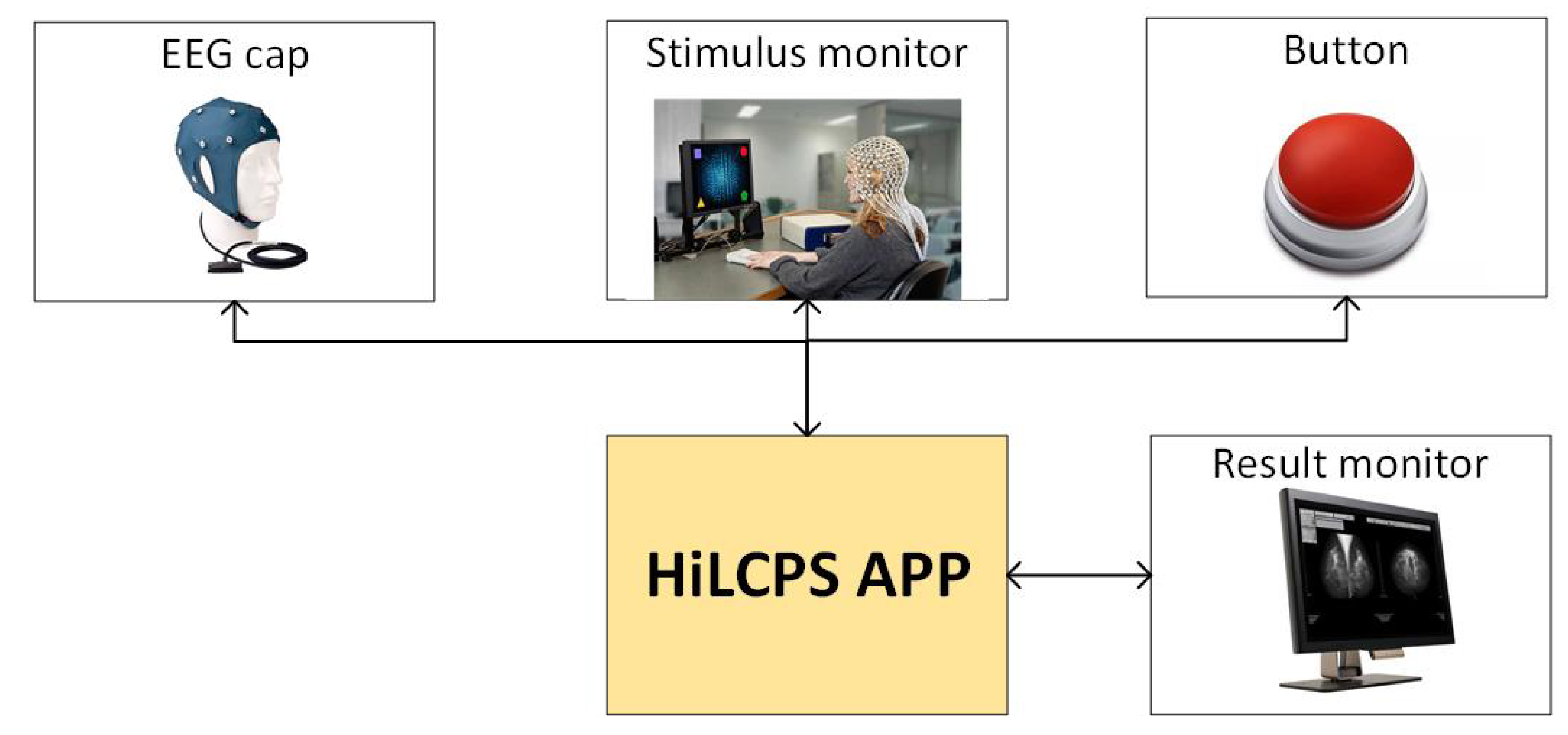
5.2. Human-in-the-Loop Cyber-Physical Systems Framework
- Hardware Transparent Access: Similar devices are grouped into device classes called DevClass. Members of the same device class are accessible via the same well-defined interface.
- Location Transparent Access: Allows simple development of distributed systems. Remote hardware components can be accessed as if locally connected.
- Domain-Specfic Synthesis: The framework provides the HSyn submodule, which allows automatic appropriation of MATLAB algorithms, so they can be implemented on embedded hardware.
5.3. System on Chip Implementations
- 1
- Accuracy: “The SoC shall produce accurate results.”
- 2
- Feasibility: “The cost of the SoC shall be low, and its application shall be simple.”
- 3
- Robustness: “The result shall be impervious to noise.”
- 4
- Interpretability: “The result of the SoC shall be accessible and comprehensible.”
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- International Statistical Classification of Diseases and Related Health Problems Online Catalog. Available online: https://icd.who.int/browse10/2016/en (accessed on 30 January 2022).
- Diagnostic and Statistical Manual of Mental Disorders. Available online: https://www.psychiatry.org/psychiatrists/practice/dsm/history-of-the-dsm (accessed on 30 January 2022).
- Willcutt, E.G. The Prevalence of DSM-IV Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Cowen, P.; Harrison, P.; Burns, T. Shorter Oxford Textbook of Psychiatry; OUP Oxford: Oxford, UK, 2012. [Google Scholar]
- Perego, P.; Rahmani, A.M.; Taherinejad, N. Wireless Mobile Communication and Healthcare; Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering; Springer International Publishing: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Yin, H.; Ozge Akmandor, A.; Mosenia, A.; K. Jha, N. Smart healthcare. In Foundations and Trends® in Electronic Design Automation; Foundations and Trends in Electronic Design Automation: Boston, MA, USA, 2018; Volume 2, pp. 401–466. [Google Scholar]
- Perego, P.; Taherinejad, N.; Caon, M. Wearables in Healthcare; Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering Book Series (LNICST, Volume 376); Springer International Publishing: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Götzinger, M.; Taherinejad, N.; Rahmani, A.M.; Liljeberg, P.; Jantsch, A.; Tenhunen, H. Enhancing the early warning score system using data confidence. In Proceedings of the 6th International Conference, MobiHealth 2016, Milan, Italy, 14–16 November 2016; Springer: Berlin/Heidelberg, Germany, 2016; pp. 91–99. [Google Scholar]
- Götzinger, M.; Azanpour, A.; Azimi, I.; Taherinejad, N.; Rahmani, A.M. Enhancing the Self-Aware Early Warning Score System through Fuzzified Data Reliability Assessment. In Proceedings of the 6th International Conference, MobiHealth 2016, Milan, Italy, 14–16 November 2016; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Anzanpour, A.; Azimi, I.; Götzinger, M.; Rahmani, A.M.; TaheriNejad, N.; Liljeberg, P.; Jantsch, A.; Dutt, N. Self-Awareness in Remote Health Monitoring Systems using Wearable Electronics. In Proceedings of the Design and Test Europe Conference (DATE), Lausanne, Switzerland, 27–31 March 2017. [Google Scholar]
- Götzinger, M.; Anzanpour, A.; Azimi, I.; TaheriNejad, N.; Jantsch, A.; Rahmani, A.; Liljeberg, P. Confidence-Enhanced Early Warning Score Based on Fuzzy Logic. Mob. Netw. Appl. 2019, 1–18. [Google Scholar] [CrossRef] [Green Version]
- TaheriNejad, N.; Rahmati, Y. Blood Pressure Estimation using a Single PPG Signal. In Proceedings of the 2nd EAI International Conference on Wearables in Healthcare (Healthwear 2020), Virtual Event, 9–11 June 2020; pp. 1–9. [Google Scholar]
- Hadizadeh, E.; Elmi, M.; TaheriNejad, N.; Fotowat, A.; Mirabbasi, S. A Low-Power Signal-Dependent Sampling Technique: Analysis, Implementation, and Application. IEEE Trans. Circuits Syst. I Regul. Pap. 2020, 67, 4334–4347. [Google Scholar]
- Hafshejani, E.H.; TaheriNejad, N.; Rabbani, R.; Azizi, Z.; Mohin, S.; Fotowat-Ahmady, A.; Mirabbasi, S. Self-aware Data Processing for Power Saving in Resource-Constrained IoT Cyber-Physical Systems. IEEE Sens. J. 2021, 1–12. [Google Scholar] [CrossRef]
- TaheriNejad, N.; Pollreisz, D. Assessment of Physiological Signals during Happiness, Sadness, Pain or Anger. In Proceedings of the 6th International Conference, MobiHealth 2016, Milan, Italy, 14–16 November 2016. [Google Scholar]
- Pollreisz, D.; TaheriNejad, N. A simple algorithm for emotion recognition, using physiological signals of a smart watch. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; pp. 2353–2356. [Google Scholar] [CrossRef]
- Miller, T.; Leger, M.C. A Very Childish Moral Panic: Ritalin. J. Med. Humanit. 2003, 24, 9–33. [Google Scholar] [CrossRef]
- Mieszkowski, K. Scientology’s War on Psychiatry. Available online: https://www.salon.com/2005/07/01/sci_psy/ (accessed on 30 January 2022).
- Thapar, A.; Cooper, M. Attention deficit hyperactivity disorder. Lancet 2016, 387, 1240–1250. [Google Scholar] [CrossRef]
- Singh, I. Beyond polemics: Science and ethics of ADHD. Nat. Rev. Neurosci. 2009, 9, 957–964. [Google Scholar] [CrossRef]
- Konrad, K.; Eickhoff, S.B. Is the ADHD brain wired differently? A review on structural and functional connectivity in attention deficit hyperactivity disorder. Hum. Brain Mapp. 2010, 31, 904–916. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Meltzer, H.; Gatward, R.; Goodman, R.; Ford, T. Mental health of children and adolescents in Great Britain. Int. Rev. Psychiatry 2003, 15, 185–187. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Carlström, E.; Råstam, M.; Gillberg, C.; Anckarsäter, H. The Genetics of Autism Spectrum Disorders and Related Neuropsychiatric Disorders in Childhood. Am. J. Psychiatry 2010, 167, 1357–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, C.M.; Steinhausen, H.C. Comorbid mental disorders in children and adolescents with attention-deficit/hyperactivity disorder in a large nationwide study. ADHD Atten. Deficit Hyperact. Disord. 2014, 7, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, A.; Martin, J.; Langley, K.; Thapar, A. Intellectual Disability in Children with Attention Deficit Hyperactivity Disorder. J. Pediatr. 2013, 163, 890–895.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, J.M.; Kinsbourne, M.; Nigg, J.; Lanphear, B.; Stefanatos, G.A.; Volkow, N.; Taylor, E.; Casey, B.J.; Castellanos, F.X.; Wadhwa, P.D. Etiologic Subtypes of Attention-Deficit/Hyperactivity Disorder: Brain Imaging, Molecular Genetic and Environmental Factors and the Dopamine Hypothesis. Neuropsychol. Rev. 2007, 17, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Russell, V.A. Overview of Animal Models of Attention Deficit Hyperactivity Disorder (ADHD). Curr. Protoc. Neurosci. 2011, 54, 9.35.1–9.35.25. [Google Scholar] [CrossRef]
- Sontag, T.A.; Tucha, O.; Walitza, S.; Lange, K.W. Animal models of attention deficit/hyperactivity disorder (ADHD): A critical review. ADHD Atten. Deficit Hyperact. Disord. 2010, 2, 1–20. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J.; Monuteaux, M.C. Toward guidelines for pedigree selection in genetic studies of attention deficit hyperactivity disorder. Genet. Epidemiol. 2000, 18, 1–16. [Google Scholar] [CrossRef]
- Thapar, A.; Cooper, M.; Eyre, O.; Langley, K. Practitioner Review: What have we learnt about the causes of ADHD? J. Child Psychol. Psychiatry 2012, 54, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Bhutta, A.T.; Cleves, M.A.; Casey, P.H.; Cradock, M.M.; Anand, K.J.S. Cognitive and Behavioral Outcomes of School-Aged Children Who Were Born Preterm. JAMA 2002, 288, 728. [Google Scholar] [CrossRef]
- Liew, Z.; Ritz, B.; Rebordosa, C.; Lee, P.C.; Olsen, J. Acetaminophen Use During Pregnancy, Behavioral Problems, and Hyperkinetic Disorders. JAMA Pediatr. 2014, 168, 313. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.M.D.; Waldie, K.E.; Wall, C.R.; Murphy, R.; Mitchell, E.A. Associations between Acetaminophen Use during Pregnancy and ADHD Symptoms Measured at Ages 7 and 11 Years. PLoS ONE 2014, 9, e108210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence Clinical Guideline 72: Attention Deficit Hyperactivity Disorder: Diagnosis and Management of ADHD in Children, Young People and Adults. Available online: https://www.nice.org.uk/guidance/cg72 (accessed on 30 January 2022).
- Taylor, E.; Döpfner, M.; Sergeant, J.; Asherson, P.; Banaschewski, T.; Buitelaar, J.; Coghill, D.; Danckaerts, M.; Rothenberger, A.; Sonuga-Barke, E.; et al. European clinical guidelines for hyperkinetic disorder—First upgrade. Eur. Child Adolesc. Psychiatry 2004, 13, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.T.; DuPaul, G.; Earls, M.; Feldman, H.M.; Ganiats, T.G.; Kaplanek, B.; Meyer, B.; Perrin, J.; Pierce, K.; Reiff, M.; et al. ADHD: Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics 2011, 128, 1007–1022. [Google Scholar] [CrossRef] [Green Version]
- Kempton, S.; Vance, A.; Maruff, P.; Luk, E.; Costin, J.; Pantelis, C. Executive function and attention deficit hyperactivity disorder: Stimulant medication and better executive function performance in children. Psychol. Med. 1999, 29, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Storebø, O.J.; Ramstad, E.; Krogh, H.B.; Nilausen, T.D.; Skoog, M.; Holmskov, M.; Rosendal, S.; Groth, C.; Magnusson, F.L.; Moreira-Maia, C.R.; et al. Methylphenidate for children and adolescents with attention deficit hyperactivity disorder (ADHD). Cochrane Database Syst. Rev. 2015, 2015, CD009885. [Google Scholar] [CrossRef] [Green Version]
- Schachter, H.M.; Pham, B.; King, J.; Langford, S.; Moher, D. How efficacious and safe is short-acting methylphenidate for the treatment of attention-deficit disorder in children and adolescents? A meta-analysis. CMAJ 2001, 165, 1475–1488. [Google Scholar]
- Faraone, S.V.; Biederman, J.; Morley, C.P.; Spencer, T.J. Effect of Stimulants on Height and Weight: A Review of the Literature. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 994–1009. [Google Scholar] [CrossRef]
- A 14-Month Randomized Clinical Trial of Treatment Strategies for Attention-Deficit/Hyperactivity Disorder. Arch. Gen. Psychiatry 1999, 56, 1073. [CrossRef]
- The Ten Twenty Electrode System: International Federation of Societies for Electroencephalography and Clinical Neurophysiology. Am. J. EEG Technol. 1961, 1, 13–19. [CrossRef]
- Klem, G.H.; LuÈders, H.O.; Jasper, H.; Elger, C. The Ten-Twenty Electrode System of the International Federation. Available online: http://media.journals.elsevier.com/content/files/clinph-chapter11-14082757.pdf (accessed on 11 February 2022).
- 10–20 Electrode Placement Guide. Available online: https://www.trans-cranial.com/docs/10_20_pos_man_v1_0_pdf.pdf (accessed on 11 February 2022).
- Ratti, E.; Waninger, S.; Berka, C.; Ruffini, G.; Verma, A. Comparison of Medical and Consumer Wireless EEG Systems for Use in Clinical Trials. Front. Hum. Neurosci. 2017, 11, 398. [Google Scholar] [CrossRef] [Green Version]
- IFCN. Recommendations for the Practice of Clinical Neurophysiology: Guidelines of the IFCN. Clin. Neurophysiol. 1999. Available online: https://www.journals.elsevier.com/clinical-neurophysiology/view-for-free/guidelines-of-the-ifcn-2nd-ed-published-1999 (accessed on 11 February 2022).
- Peng, G.; Nourani, M.; Harvey, J.; Dave, H. Feature Selection Using F-Statistic Values for EEG Signal Analysis; IEEE: New York, NY, USA, 2020; pp. 5963–5966. [Google Scholar] [CrossRef]
- Saby, J.N.; Marshall, P.J. The Utility of EEG Band Power Analysis in the Study of Infancy and Early Childhood. Dev. Neuropsychol. 2012, 37, 253–273. [Google Scholar] [CrossRef] [PubMed]
- Jasper, H.H.; Solomon, P.; Bradley, C. Electroencephalographic analyses of behavior problem children. Am. J. Psychiatry 1938, 95, 641–658. [Google Scholar] [CrossRef]
- FDA. FDA Permits Marketing of First Brain Wave Test to Help Assess Children and Teens for ADHD. Available online: https://web.archive.org/web/20130925093434/http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm360811.htm (accessed on 30 January 2022).
- Snyder, S.M.; Rugino, T.A.; Hornig, M.; Stein, M.A. Integration of an EEG biomarker with a clinician’s ADHD evaluation. Brain Behav. 2015, 5, e00330. [Google Scholar] [CrossRef] [PubMed]
- Quintana, H.; Snyder, S.M.; Purnell, W.; Aponte, C.; Sita, J. Comparison of a standard psychiatric evaluation to rating scales and EEG in the differential diagnosis of attention-deficit/hyperactivity disorder. Psychiatry Res. 2007, 152, 211–222. [Google Scholar] [CrossRef]
- Buyck, I.; Wiersema, J.R. Resting electroencephalogram in attention deficit hyperactivity disorder: Developmental course and diagnostic value. Psychiatry Res. 2014, 216, 391–397. [Google Scholar] [CrossRef]
- Liechti, M.D.; Valko, L.; Müller, U.C.; Döhnert, M.; Drechsler, R.; Steinhausen, H.C.; Brandeis, D. Diagnostic Value of Resting Electroencephalogram in Attention-Deficit/Hyperactivity Disorder Across the Lifespan. Brain Topogr. 2012, 26, 135–151. [Google Scholar] [CrossRef] [Green Version]
- Loo, S.K.; McGough, J.J.; McCracken, J.T.; Smalley, S.L. Parsing heterogeneity in attention-deficit hyperactivity disorder using EEG -based subgroups. J. Child Psychol. Psychiatry 2017, 59, 223–231. [Google Scholar] [CrossRef]
- Lenartowicz, A.; Loo, S.K. Use of EEG to Diagnose ADHD. Curr. Psychiatry Rep. 2014, 16, 498. [Google Scholar] [CrossRef] [Green Version]
- Esteller, R.; Vachtsevanos, G.; Echauz, J.; Litt, B. A comparison of waveform fractal dimension algorithms. IEEE Trans. Circuits Syst. I Fundam. Theory Appl. 2001, 48, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Stoica, P.; Moses, R. Introduction to Spectral Analysis; Prentice Hall: Upper Saddle River, NJ, USA, 1997; Volume 1. [Google Scholar]
- Principe, J.C.; Lo, P.C. Towards the determination of the largest Lyapunov exponent of EEG segments. Meas. Chaos Hum. Brain 1991, 86, 156–166. [Google Scholar]
- Meyer, P.E.; Schretter, C.; Bontempi, G. Information-Theoretic Feature Selection in Microarray Data Using Variable Complementarity. IEEE J. Sel. Top. Signal Process. 2008, 2, 261–274. [Google Scholar] [CrossRef]
- Peng, H.; Long, F.; Ding, C. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 1226–1238. [Google Scholar] [CrossRef]
- Mohammadi, M.R.; Khaleghi, A.; Nasrabadi, A.M.; Rafieivand, S.; Begol, M.; Zarafshan, H. EEG classification of ADHD and normal children using non-linear features and neural network. Biomed. Eng. Lett. 2016, 6, 66–73. [Google Scholar] [CrossRef]
- Leroy, A.; Petit, G.; Zarka, D.; Cebolla, A.; Palmero-Soler, E.; Strul, J.; Dan, B.; Verbanck, P.; Cheron, G. EEG Dynamics and Neural Generators in Implicit Navigational Image Processing in Adults with ADHD. Neuroscience 2018, 373, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Jouzizadeh, M.; Khanbabaie, R.; Ghaderi, A.H. A spatial profile difference in electrical distribution of resting-state EEG in ADHD children using sLORETA. Int. J. Neurosci. 2020, 130, 917–925. [Google Scholar] [CrossRef]
- Taleb, T.; Bottazzi, D.; Guizani, M.; Nait-Charif, H. Angelah: A framework for assisting elders at home. IEEE J. Sel. Areas Commun. 2009, 27, 480–494. [Google Scholar] [CrossRef] [Green Version]
- Müller-Putz, G.R. Tools for brain-computer interaction: A general concept for a hybrid BCI. Front. Neuroinform. 2011, 5, 30. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Quivira, F.; Schirner, G. Framework for Rapid Development of Embedded Human-in-the-Loop Cyber-Physical Systems. In Proceedings of the 2016 IEEE 16th International Conference on Bioinformatics and Bioengineering (BIBE), Taichung, Taiwan, 31 October–2 November 2016. [Google Scholar] [CrossRef]
- Undulator (EEG Machine). Available online: https://braintour.harvard.edu/archives/portfolio-items/undulator-eeg-machine (accessed on 30 January 2022).
- Available online: https://ear-eeg.org/ (accessed on 28 November 2021).
- Wei, Y.; Zhou, J.; Wang, Y.; Liu, Y.; Liu, Q.; Luo, J.; Wang, C.; Ren, F.; Huang, L. A Review of Algorithm & Hardware Design for AI-Based Biomedical Applications. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 145–163. [Google Scholar] [CrossRef]
- Page, A.; Sagedy, C.; Smith, E.; Attaran, N.; Oates, T.; Mohsenin, T. A Flexible Multichannel EEG Feature Extractor and Classifier for Seizure Detection. IEEE Trans. Circuits Syst. II Express Briefs 2015, 62, 109–113. [Google Scholar] [CrossRef]
- Tsou, C.; Liao, C.C.; Lee, S.Y. Epilepsy Identification System with Neural Network Hardware Implementation. In Proceedings of the 2019 IEEE International Conference on Artificial Intelligence Circuits and Systems (AICAS), Hsinchu, Taiwan, 18–20 March 2019. [Google Scholar] [CrossRef]
- Smetanin, N.; Lebedev, M.A.; Ossadtchi, A. Towards Zero-Latency Neurofeedback; Cold Spring Harbor Laboratory: Woodbury, NY, USA, 2018. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.D.; Wang, K.Y.; Ho, Y.L.; He, C.Y.; Fang, W.C. An Edge AI System-on-Chip Design with Customized Convolutional-Neural-Network Architecture for Real-time EEG-Based Affective Computing System. In Proceedings of the 2019 IEEE Biomedical Circuits and Systems Conference (BioCAS), Nara, Japan, 17–19 October 2019. [Google Scholar] [CrossRef]
- Imtiaz, S.A.; Jiang, Z.; Rodriguez-Villegas, E. An Ultralow Power System on Chip for Automatic Sleep Staging. IEEE J. Solid-State Circuits 2017, 52, 822–833. [Google Scholar] [CrossRef]
- Conti, F.; Schilling, R.; Schiavone, P.D.; Pullini, A.; Rossi, D.; Gurkaynak, F.K.; Muehlberghuber, M.; Gautschi, M.; Loi, I.; Haugou, G.; et al. An IoT Endpoint System-on-Chip for Secure and Energy-Efficient Near-Sensor Analytics. IEEE Trans. Circuits Syst. I Regul. Pap. 2017, 64, 2481–2494. [Google Scholar] [CrossRef] [Green Version]
- Sridhara, S.R.; DiRenzo, M.; Lingam, S.; Lee, S.J.; Blazquez, R.; Maxey, J.; Ghanem, S.; Lee, Y.H.; Abdallah, R.; Singh, P.; et al. Microwatt Embedded Processor Platform for Medical System-on-Chip Applications. IEEE J. Solid-State Circuits 2011, 46, 721–730. [Google Scholar] [CrossRef]
- Kam, J.W.; Griffin, S.; Shen, A.; Patel, S.; Hinrichs, H.; Heinze, H.J.; Deouell, L.Y.; Knight, R.T. Systematic comparison between a wireless EEG system with dry electrodes and a wired EEG system with wet electrodes. NeuroImage 2019, 184, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.J.; Song, J.I. A Chopper Stabilized Current-Feedback Instrumentation Amplifier for EEG Acquisition Applications. IEEE Access 2019, 7, 11565–11569. [Google Scholar] [CrossRef]
- Mondal, S.; Hall, D.A. An ECG chopper amplifier achieving 0.92 NEF and 0.85 PEF with AC-coupled inverter-stacking for noise efficiency enhancement. In Proceedings of the 2017 IEEE International Symposium on Circuits and Systems (ISCAS), Baltimore, MD, USA, 28–31 May 2017. [Google Scholar] [CrossRef]
- Liao, J.C.; Shih, W.Y.; Huang, K.J.; Fang, W.C. An online recursive ICA based real-time multichannel EEG system on chip design with automatic eye blink artifact rejection. In Proceedings of the 2013 International Symposium onVLSI Design, Automation, and Test (VLSI-DAT), Hsinchu, Taiwan, 22–24 April 2013. [Google Scholar] [CrossRef]
- Zhang, S.; McIntosh, J.; Shadli, S.M.; Neo, P.S.H.; Huang, Z.; McNaughton, N. Removing eye blink artefacts from EEG—A single-channel physiology-based method. J. Neurosci. Methods 2017, 291, 213–220. [Google Scholar] [CrossRef]
- Sturm, I.; Lapuschkin, S.; Samek, W.; Müller, K.R. Interpretable deep neural networks for single-trial EEG classification. J. Neurosci. Methods 2016, 274, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EEG | fMRI | fNIRS | |
|---|---|---|---|
| Temporal resolution | High | Low | High |
| Spatial resolution | Low | High | Low |
| Measurement of brain activity | Directly | Indirectly | Directly |
| Training needed | Some | Extensively | Some |
| Portability | Some systems are protable | Not portable | Some systems are protable |
| Cost (USD) | ∼100+ | 50 k+ | 10 k+ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freismuth, D.; TaheriNejad, N. On the Treatment and Diagnosis of Attention Deficit Hyperactivity Disorder with EEG Assistance. Electronics 2022, 11, 606. https://doi.org/10.3390/electronics11040606
Freismuth D, TaheriNejad N. On the Treatment and Diagnosis of Attention Deficit Hyperactivity Disorder with EEG Assistance. Electronics. 2022; 11(4):606. https://doi.org/10.3390/electronics11040606
Chicago/Turabian StyleFreismuth, David, and Nima TaheriNejad. 2022. "On the Treatment and Diagnosis of Attention Deficit Hyperactivity Disorder with EEG Assistance" Electronics 11, no. 4: 606. https://doi.org/10.3390/electronics11040606
APA StyleFreismuth, D., & TaheriNejad, N. (2022). On the Treatment and Diagnosis of Attention Deficit Hyperactivity Disorder with EEG Assistance. Electronics, 11(4), 606. https://doi.org/10.3390/electronics11040606