





Context-Based, Predictive Access Control to Electronic Health Records

 ,
,  ,
, 

Abstract
1. Introduction
2. Related Works
2.1. Access Control in Emergency Situations
2.2. Contextual Attributes for Access Control
2.3. Data Analytics in Healthcare
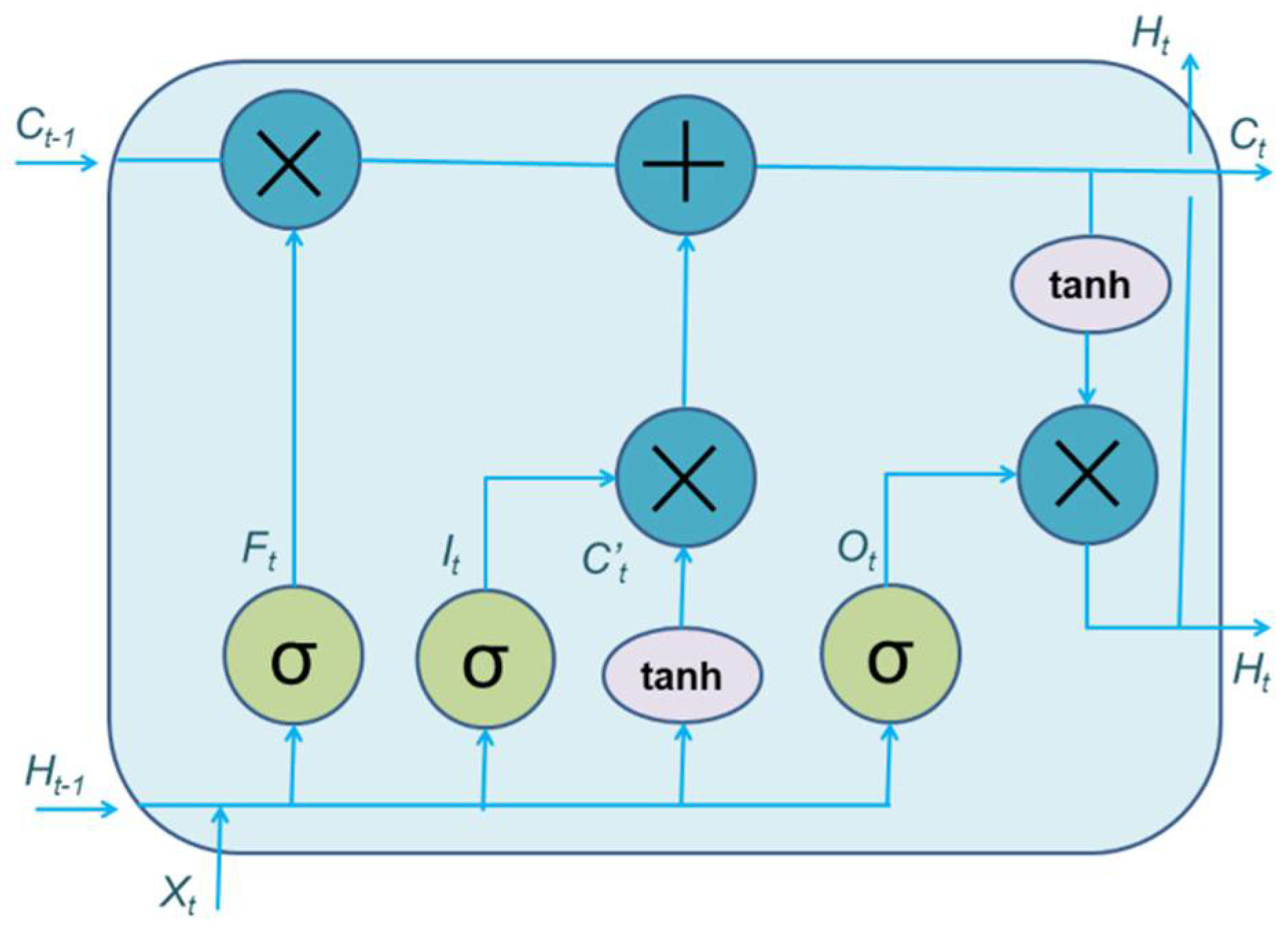
2.4. Health Analytics Using LSTM
3. Methods
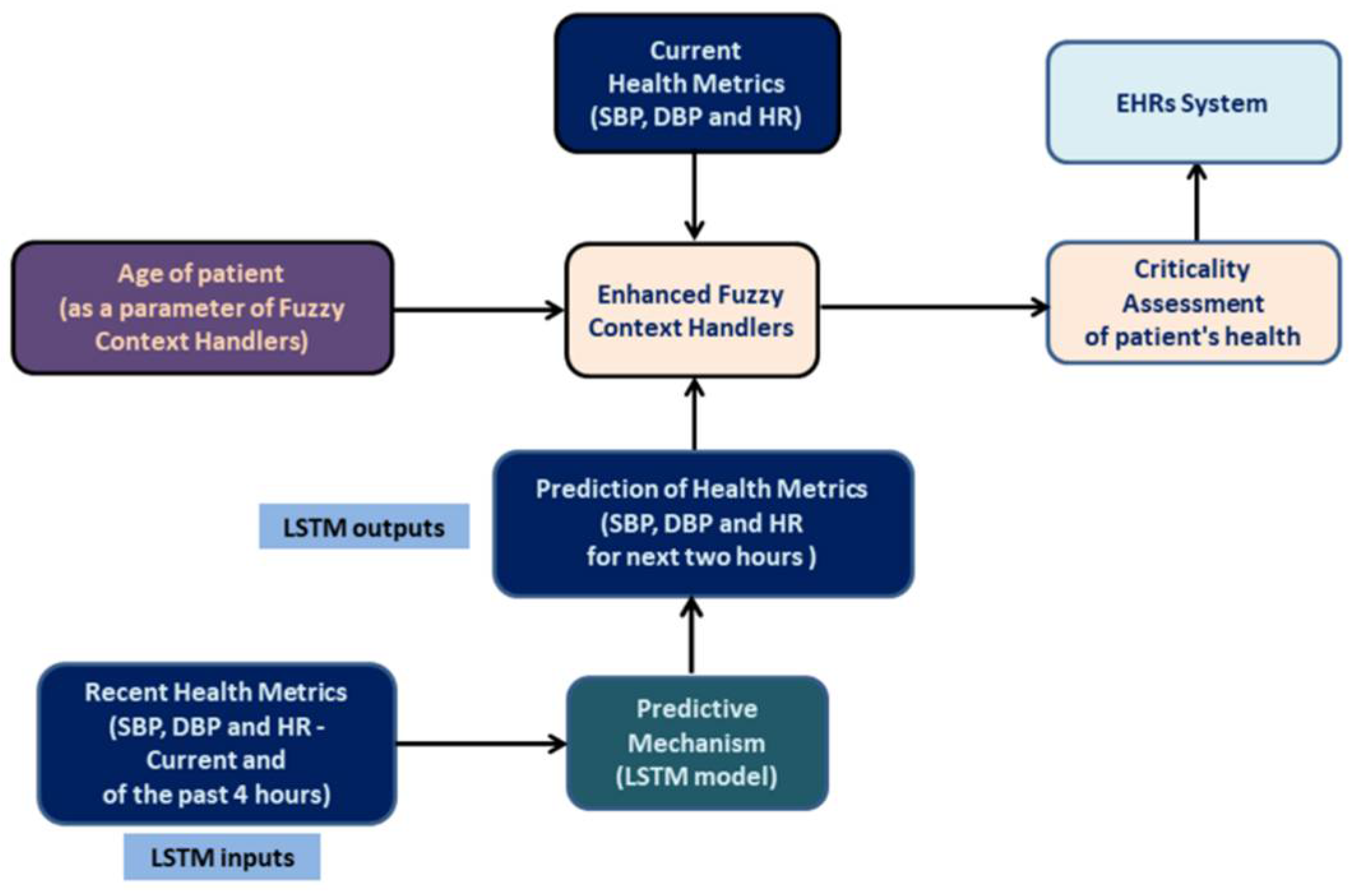
3.1. Fuzzy Context Handlers
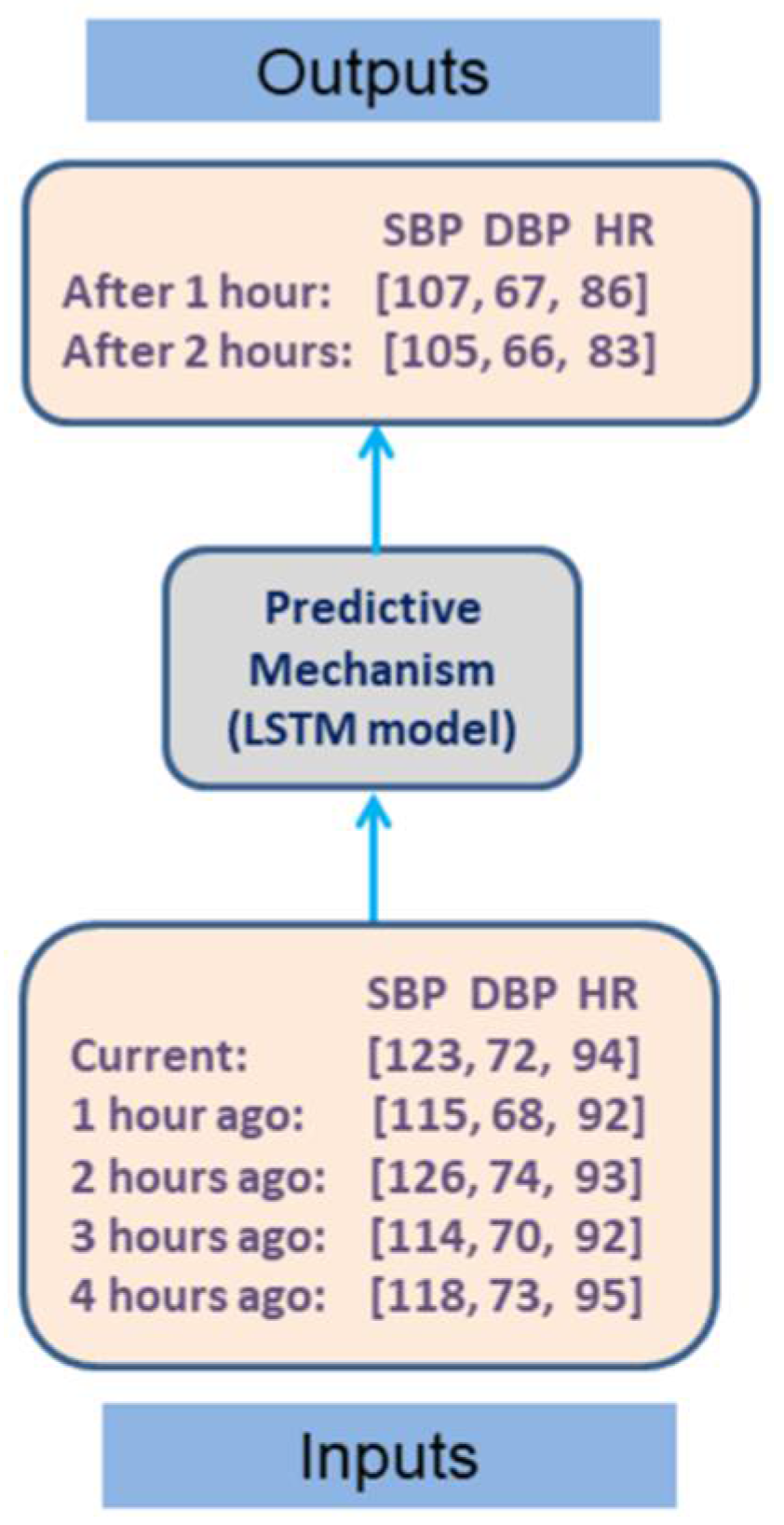
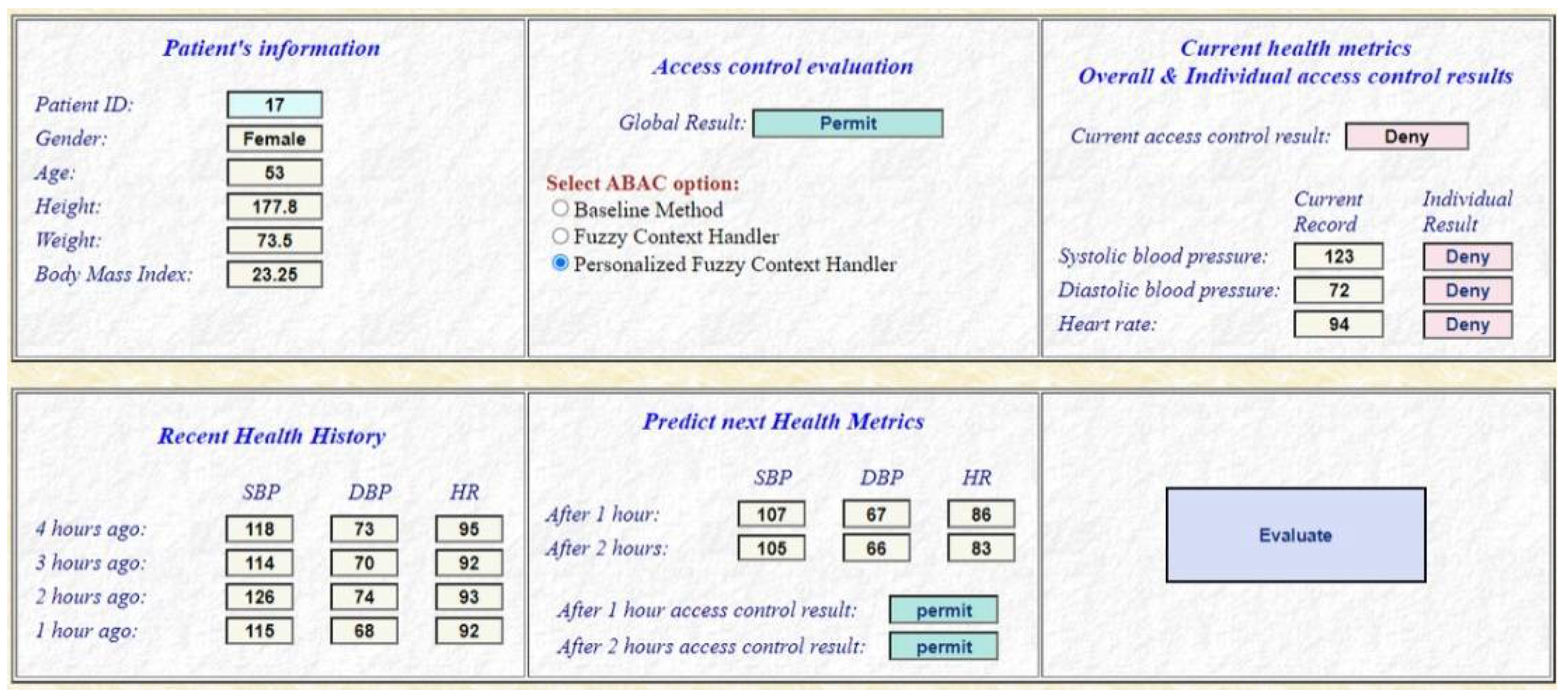
3.2. Predicting Mechanism
| Algorithm 1 Prediction of future health metrics |
| CHOOSE NUMBER OF INPUT STEPS (health history of last 4 h) |
| input_steps ← 5 |
| CHOOSE OUTPUT STEPS (future health metrics of the next two hours) |
| output_steps ← 2 |
| CHOOSE FEATURES (number of health metrics) |
| features ← 3 |
| REPEAT FOR ALL DATA FILES |
| READ EACH DATASET’S FILE PER PATIENT |
| SELECT TRAIN AND TEST SETS |
| data_train, data_test ← devide(dataset, 0.8) |
| SPLIT DATA ACCODING TO INPUT AND OUTPUT STEPS |
| X_train, Y_train ← split_dataset(data_train, input_steps) |
| X_test, Y_test ← split_dataset(data_test, input_steps) |
| RESHAPE X_train and X_test |
| Reshape X_train, X_test into (samples, inpute_steps, features) |
| DEFINE MODEL |
| add(LSTM(200, activation = ‘relu’, input_shape = (input_steps, features))) |
| add(RepeatVector(output_steps)) |
| add(LSTM(200, activation = ‘relu’, return_sequences = True)) |
| add(TimeDistributed(Dense(features))) |
| COMPILE MODEL |
| compile(optimizer = ‘adam’, loss = ‘mse’) |
| FIT MODEL (to improve the weights and biases of the network) |
| model.fit(X_train, Y_train, epochs = 200, verbose = 0) |
| EVALUATE MODEL |
| SAVE MODEL |
| model.save(model_file) |
| END REPEAT |
| INPUT A PATIENT’S HEALTH METRICS FOR THE LAST 4 HOURS METRICS |
| input_metrics: |
| sbp_current, dbp_current, hr_current current health metrics |
| sbp_before_1, dbp_before_1, hr_ before_1 health metrics before 1 h |
| sbp_ before_2, dbp_ before_2, hr_before_2 health metrics before 2 h |
| sbp_ before_3, dbp_ before_3, hr_before_3 health metrics before 3 h |
| sbp_before_4, dbp_before_4, hr_before_4 health metrics before 4 h |
| PREDICT AND OUTPUT PATIENT’S FUTURE HEALTH METRICS |
| output_metrcs: |
| sbp_next_1, dbp_next_1, hr_next_1 predicted health metrics after 1 h |
| sbp_next_2, dbp_next_2, hr_next_2 predicted health metrics after 2 h |
| output_metrics ← model_file.predict(input_metrics) |
4. Evaluation
4.1. Technical Implementation
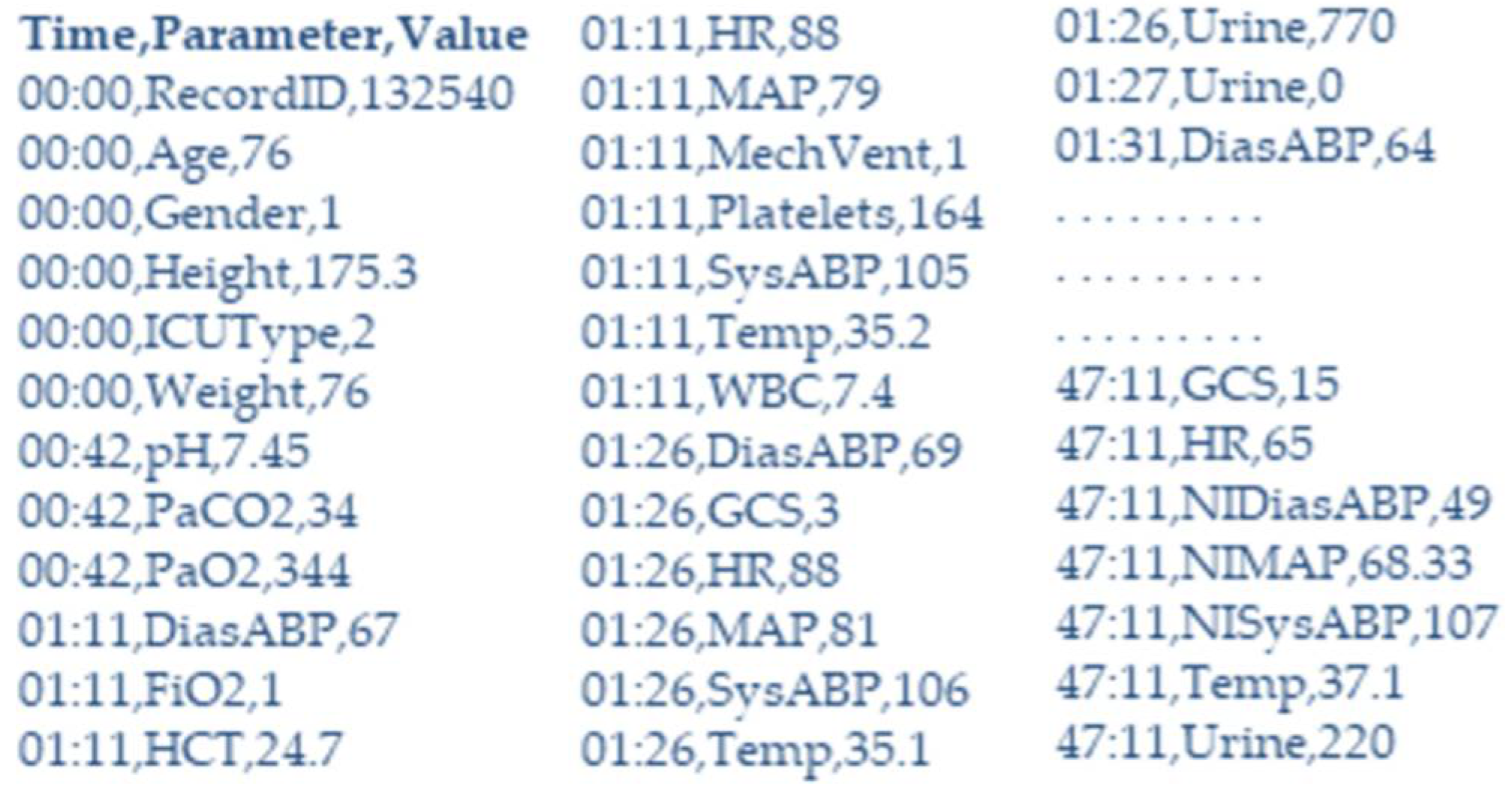
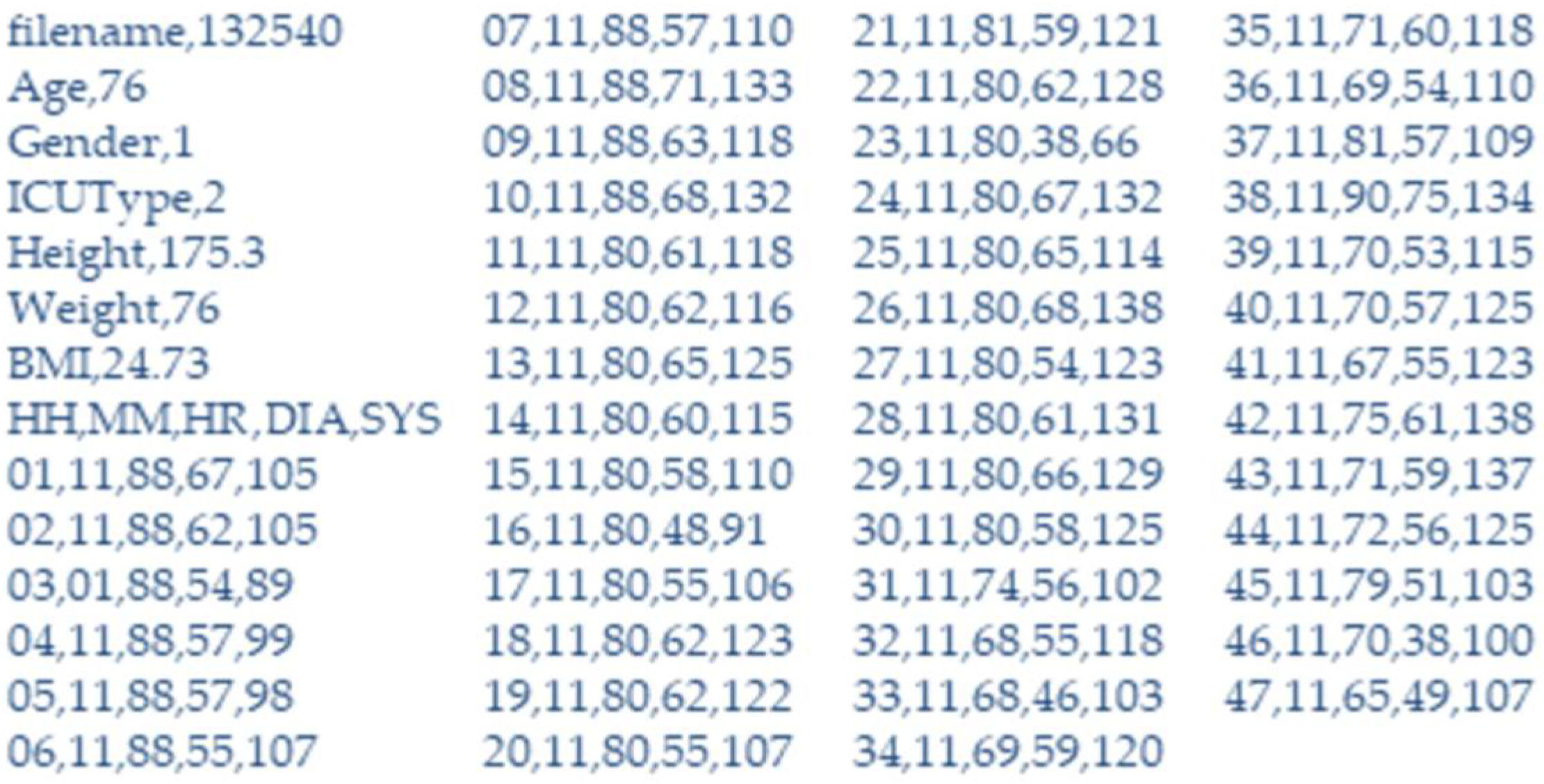
4.2. Evaluation Scenarios and Datasets
4.3. Results
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ferrari, E. Access Control in Data Management Systems. Synth. Lect. Data Manag. 2010, 2, 1–117. [Google Scholar] [CrossRef]
- Hu, V.C.; Ferraiolo, D.; Kuhn, R.; Schnitzer, A.; Sandlin, K.; Miller, R.; Scarfone, K. Guide to Attribute Based Access Control (ABAC) Definition and Considerations. NIST Spec. Publ. 2013, 800, 162. [Google Scholar] [CrossRef]
- Dey, A.K. Understanding and Using Context. Pers. Ubiquitous Comput. 2001, 5, 4–7. [Google Scholar] [CrossRef]
- Yao, R.; Guo, C.; Deng, W.; Zhao, H. A novel mathematical morphology spectrum entropy based on scale-adaptive techniques. ISA Trans. 2021, 126, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Miao, F.; Chen, Y.; Xiong, Y.; Chen, T. A Hyperspectral Image Classification Method Using Multifeature Vectors and Optimized KELM. IEEE J. Sel. Top. Appl. Earth Obs. Remote Sens. 2021, 14, 2781–2795. [Google Scholar] [CrossRef]
- Wu, D.; Wu, C. Research on the Time-Dependent Split Delivery Green Vehicle Routing Problem for Fresh Agricultural Products with Multiple Time Windows. Agriculture 2022, 12, 793. [Google Scholar] [CrossRef]
- Psarra, E.; Verginadis, Y.; Patiniotakis, I.; Apostolou, D.; Mentzas, G. Accessing electronic health records in critical incidents using context-aware attribute-based access control. Intell. Decis. Technol. 2021, 1–13, preprint. [Google Scholar] [CrossRef]
- Ben-Assuli, O.; Ziv, A.; Sagi, D.; Ironi, A.; Leshno, M. Cost-effectiveness evaluation of EHR: Simulation of an abdominal aortic aneurysm in the emergency department. J. Med. Syst. 2016, 40, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Povey, D. Optimistic security: A new access control paradigm. In Proceedings of the 1999 workshop on New security paradigms, Caledon Hills, ON, Canada, 22–25 September 1999; pp. 40–45. [Google Scholar]
- Saberi, M.A.; Adda, M.; Mcheick, H. Towards an ABAC Break-Glass to access EMRs in case of emergency based on Blockchain. In Proceedings of the 2021 IEEE International Conference on Digital Health (ICDH), Online, 11–15 September 2021; pp. 220–222. [Google Scholar]
- Saberi, M.A.; Adda, M.; Mcheick, H. Break-Glass Conceptual Model for Distributed EHR management system based on Blockchain, IPFS and ABAC. Procedia Comput. Sci. 2022, 198, 185–192. [Google Scholar] [CrossRef]
- Manasa, D.; Khanna, K.R. Sharing of PHR’s in Cloud Computing. Int. J. Comput. Sci. Netw. Secur. (IJCSNS) 2015, 15, 86. [Google Scholar]
- Tsegaye, T.; Flowerday, S. A Clark-Wilson and ANSI role-based access control model. Inf. Comput. Secur. 2020, 28, 373–395. [Google Scholar] [CrossRef]
- Li, M.; Yu, S.; Ren, K.; Lou, W. Securing Personal Health Records in Cloud Computing: Patient-Centric and Fine-Grained Data Access Control in Multi-owner Settings. In Proceedings of the International Conference on Security and Privacy in Communication Systems, Washington, WA, USA, 21–23 October 2021; Springer: Berlin/Heidelberg, Germany, 2010; pp. 89–106. [Google Scholar] [CrossRef]
- Jagdale, V.; Kekan, D.; Baride, I. Secure Sharing of Personal Health Records in Cloud using Attribute-based Encryption. Int. J. Comput. Sci. Mob. Comput. 2015, 4, 309–312. [Google Scholar]
- Farinha, P.; Cruz-Correia, R.; Antunes, L.; Almeida, F.; Ferreira, A. From Legislation to Practice—A Case Study of Break the Glass in Healthcare. In Proceedings of the International Conference on Health Informatics, Arlington, VI, USA, 11–12 November 2010; Volume 2, pp. 114–120. [Google Scholar]
- Brucker, A.D.; Petritsch, H. Extending access control models with break-glass. In Proceedings of the 14th ACM Symposium on Access Control Models and Technologies, Athens, Greece, 11–15 June 2014; pp. 197–206. [Google Scholar]
- Georgakakis, E.; Nikolidakis, S.A.; Vergados, D.D.; Douligeris, C. Spatio temporal emergency role based access control (STEM-RBAC): A time and location aware role based access control model with a break the glass mechanism. In Proceedings of the 2011 IEEE Symposium on Computers and Communications (ISCC), Washington, DC, USA, 28 June–1 July 2011; pp. 764–770. [Google Scholar] [CrossRef]
- Kabbani, B.; Laborde, R.; Barrère, F.; Benzekri, A. Managing Break-The-Glass using Situation-oriented authorizations. In Proceedings of the 9ème Conférence sur la Sécurité des Architectures Réseaux et Systèmes d’Information-SAR-SSI, Paris, France, 13–16 May 2014. [Google Scholar]
- Marinovic, S.; Craven, R.; Ma, J.; Dulay, N. Rumpole: A flexible break-glass access control model. In Proceedings of the 16th ACM Symposium on Access Control Models and Technologies, New York, NY, USA, 7–9 June 2011; pp. 73–82. [Google Scholar]
- Maw, H.A.; Xiao, H.; Christianson, B.; Malcolm, J.A. An evaluation of break-the-glass access control model for medical data in wireless sensor networks. In Proceedings of the 2014 IEEE 16th International Conference on E-Health Networking, Applications and Services (Healthcom), Natal, Brazil, 15–18 October 2014; pp. 130–135. [Google Scholar] [CrossRef]
- Guan, S.; Wang, Y.; Shen, J. Fingerprint-based access to personally controlled health records in emergency situations. Sci. China Inf. Sci. 2018, 61, 059103. [Google Scholar] [CrossRef]
- Künzi, J.; Koster, P.; Petković, M. Emergency Access to Protected Health Records. MIE 2009, 150, 705–709. [Google Scholar] [CrossRef]
- Covington, M.J.; Sastry, M.R. A contextual attribute-based access control model. In On the Move to Meaningful Internet Systems 2006: OTM 2006 Workshops; Springer: Berlin/Heidelberg, Germany, 2006; pp. 1996–2006. [Google Scholar]
- Mahalle, P.N.; Thakre, P.A.; Prasad, N.R.; Prasad, R. A fuzzy approach to trust based access control in internet of things. In Wireless VITAE; IEEE: Piscataway, NJ, USA, 2013; pp. 1–5. [Google Scholar]
- D’Aniello, G.; Loia, V.; Orciuoli, F. A multi-agent fuzzy consensus model in a Situation Awareness framework. Appl. Soft Comput. 2015, 30, 430–440. [Google Scholar] [CrossRef]
- De Maio, C.; Fenza, G.; Furno, D.; Loia, V. Swarm-based semantic fuzzy reasoning for situation awareness computing. In Proceedings of the 2012 IEEE International Conference on Fuzzy Systems, Brisbane, Australia, 10–15 June 2012; pp. 1–7. [Google Scholar] [CrossRef]
- Nomikos, G.D.; Dounias, G.; Tselentis, G.; Vemmos, K. Conventional vs. fuzzy modeling of diagnostic attributes for classifying acute stroke cases. In Proceedings of the ESIT-2000, European Symposium on Intelligent Techniques, Aachen, Germany, 9–13 September 2000; pp. 192–200. [Google Scholar]
- Mahmood, U.; Al-Jumaily, A. Type-2 fuzzy classification of blood pressure parameters. In Proceedings of the 2007 3rd International Conference on Intelligent Sensors, Sensor Networks and Information, Piscataway, NJ, USA, 3–6 December 2007; pp. 595–600. [Google Scholar]
- Djam, X.Y.; Kimbi, Y.H. Fuzzy expert system for the management of hypertension. Pac. J. Sci. Technol. 2011, 12, 390–402. [Google Scholar]
- Moameri, S.; Samadinai, N. Diagnosis of coronary artery disease via a Novel Fuzzy expert system optimized by CUCKOO SEARCH. Int. J. Eng. 2018, 31, 2028–2036. [Google Scholar]
- Zerkouk, M.; Mhamed, A.; Messabih, B. A User Profile Based Access Control Model and Architecture. Int. J. Comput. Networks Commun. 2013, 5, 171–181. [Google Scholar] [CrossRef]
- Røstad, L.; Nytrø, Ø. Personalized access control for a personally controlled health record. In Proceedings of the 2nd ACM Workshop on Computer Security Architectures—CSAW’08, Alexandria, VA, USA, 16 June 2008; pp. 9–16. [Google Scholar] [CrossRef]
- Petković, M.; Conrado, C.; Hammoutène, M. Cryptographically Enforced Personalized Role-Based Access Control. Secur. Priv. Dyn. Environ. 2006, 8, 364–376. [Google Scholar] [CrossRef]
- Son, J.; Kim, J.-D.; Na, H.-S.; Baik, D.-K. Dynamic access control model for privacy preserving personalized healthcare in cloud environment. Technol. Health Care 2015, 24, S123–S129. [Google Scholar] [CrossRef] [PubMed]
- Simpao, A.F.; Ahumada, L.M.; Gálvez, J.; Rehman, M.A. A Review of Analytics and Clinical Informatics in Health Care. J. Med. Syst. 2014, 38, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cortada, J.W.; Gordon, D.; Lenihan, B. The Value of Analytics in Healthcare: From Insights to Outcomes; IBM Global Business Services, Executive Report: Armonk, NY, USA, 2012. [Google Scholar]
- Tomar, D.; Agarwal, S. A survey on Data Mining approaches for Healthcare. Int. J. Bio-Sci. Bio-Technol. 2013, 5, 241–266. [Google Scholar] [CrossRef]
- Lustig, I.; Dietrich, B.; Johnson, C.; Dziekan, C. The analytics journey. Anal. Mag. 2010, 3, 11–13. [Google Scholar]
- Khalifa, M. Health Analytics Types, Functions and Levels: A Review of Literature. ICIMTH 2018, 251, 137–140. [Google Scholar] [CrossRef]
- Basu, A.T.A.N.U. Five pillars of prescriptive analytics success. Anal. Mag. 2013, 2, 8–12. [Google Scholar]
- Bernstein, J.H. The Data-Information-Knowledge-Wisdom Hierarchy and its Antithesis. NASKO 2009, 2, 68. [Google Scholar] [CrossRef]
- Khalifa, M. Reducing Emergency Department Crowding Using Health Analytics Methods: Designing AnEvidence Based Decision Algorithm. Procedia Comput. Sci. 2015, 63, 409–416. [Google Scholar] [CrossRef][Green Version]
- Madsen, L. Healthcare Business Intelligence: A Guide to Empowering Successful Data Reporting and Analytics; John Wiley & Sons: Hoboken, NJ, USA, 2012. [Google Scholar]
- Kohn, M.S.; Sun, J.; Knoop, S.; Shabo, A.; Carmeli, B.; Sow, D.; Syed-Mahmood, T.; Rapp, W. IBM’s health analytics and clinical decision support. Yearb. Med. Inform. 2014, 23, 154–162. [Google Scholar]
- Chen, H.; Chiang, R.H.; Storey, V.C. Business intelligence and analytics: From big data to big impact. MIS Q. 2012, 36, 1165–1188. [Google Scholar] [CrossRef]
- Bates, D.W.; Saria, S.; Ohno-Machado, L.; Shah, A.; Escobar, G. Big Data In Health Care: Using Analytics To Identify And Manage High-Risk And High-Cost Patients. Health Aff. 2014, 33, 1123–1131. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Han, J.; Xie, R.; Wang, C.; Duan, X.; Rong, Y.; Zeng, X.Y.; Tao, J. MC-LSTM: Real-Time 3D Human Action Detection System for Intelligent Healthcare Applications. IEEE Trans. Biomed. Circuits Syst. 2021, 15, 259–269. [Google Scholar] [CrossRef]
- Kadri, F.; Baraoui, M.; Nouaouri, I. LSTM-based deep learning approach with application to predicting hospital emergency department admissions. In Proceedings of the 2019 International Conference on Industrial Engineering and Systems Management (IESM), Shanghai, China, 25–27 September 2019; pp. 1–6. [Google Scholar]
- Tsai, F.S.; Weng, Y.M.; Ng, C.J.; Lee, C.C. Embedding stacked bottleneck vocal features in a LSTM architecture for automatic pain level classification during emergency triage. In Proceedings of the 2017 Seventh International Conference on Affective Computing and Intelligent Interaction (ACII), San Antonio, TX, USA, 23–26 October 2017; pp. 313–318. [Google Scholar]
- Mantas, J. Using long short-term memory (LSTM) neural networks to predict emergency department wait time. The Importance of Health Informatics in Public Health during a Pandemic. Stud. Health Technol. Inform. 2020, 272, 199. [Google Scholar]
- Nwakanma, C.I.; Islam, F.B.; Maharani, M.P.; Kim, D.S.; Lee, J.M. Iot-based vibration sensor data collection and emergency detection classification using long short term memory (lstm). In Proceedings of the 2021 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Rome, Italy, 5–9 April 2021; pp. 273–278. [Google Scholar]
- Reddy, B.K.; Delen, D. Predicting hospital readmission for lupus patients: An RNN-LSTM-based deep-learning methodology. Comput. Biol. Med. 2018, 101, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Li, L.; Zhu, Y.; Yu, P.; Wen, J. CNN-LSTM neural network model for fine-grained negative emotion computing in emergencies. Alex. Eng. J. 2022, 61, 6755–6767. [Google Scholar] [CrossRef]
- Mou, H.; Yu, J. CNN-LSTM Prediction Method for Blood Pressure Based on Pulse Wave. Electronics 2021, 10, 1664. [Google Scholar] [CrossRef]
- Chae, M.; Han, S.; Lee, H. Outdoor Particulate Matter Correlation Analysis and Prediction Based Deep Learning in the Republic of Korea. Electronics 2020, 9, 1146. [Google Scholar] [CrossRef]
- Mumtaz, R.; Zaidi, S.; Shakir, M.Z.; Shafi, U.; Malik, M.M.; Haque, A.; Mumtaz, S.; Zaidi, S. Internet of Things (IoT) Based Indoor Air Quality Sensing and Predictive Analytic—A COVID-19 Perspective. Electronics 2021, 10, 184. [Google Scholar] [CrossRef]
- Oasis-open.org. Available online: http://docs.oasis-open.org/xacml (accessed on 16 September 2021).
- Quirolgico, S.; Hu, V.; Karygiannis, T. Access Control for SAR Systems; Department of Commerce US: Washington, DC, USA, 2011. [CrossRef]
- Psarra, E.; Verginadis, Y.; Patiniotakis, I.; Apostolou, D.; Mentzas, G. A Context-Aware Security Model for a Combination of Attribute-Based Access Control and Attribute-Based Encryption in the Healthcare Domain. In Proceedings of the Workshops of the International Conference on Advanced Information Networking and Applications, Caserta, Italy, 15–17 April 2020; Springer: Cham, Switzerland, 2020; pp. 1133–1142. [Google Scholar] [CrossRef]
- Rasjid, Z.E.; Setiawan, R.; Effendi, A. A Comparison: Prediction of Death and Infected COVID-19 Cases in Indonesia Using Time Series Smoothing and LSTM Neural Network. Procedia Comput. Sci. 2021, 179, 982–988. [Google Scholar] [CrossRef]
- Brownlee, J. Deep learning for time series forecasting: Predict the future with MLPs, CNNs and LSTMs in Python. In Machine Learning Mastery; Jason Brownlee: Cambridge, MA, USA, 2018. [Google Scholar]
- Joshi, M.; Joshi, K.; Finin, T. Attribute Based Encryption for Secure Access to Cloud Based EHR Systems. In Proceedings of the 2018 IEEE 11th International Conference on Cloud Computing (CLOUD), San Francisco, CA, USA, 2–7 July 2018. [Google Scholar]
- Gutierrez, P.P. Cloud EHRServer by CaboLabs. Available online: https://cloudehrserver.com/ (accessed on 18 September 2021).
- Sam Heard, T.B. OpenEhr Home. Available online: https://www.openehr.org/ (accessed on 18 September 2021).
- Silva, I.; Moody, G.; Mark, R.; Celi, L.A. Predicting Mortality of ICU Patients: The PHYSIONET/Computing in Cardiology Challenge 2012. Predicting Mortality of ICU Patients: The PhysioNet/Computing in Cardiology Challenge 2012 v1.0.0. Available online: https://physionet.org/content/challenge-2012/1.0.0/ (accessed on 24 March 2020).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Access Control Case | Criticality Prediction Error |
|---|---|
| ABAC with Personalized Fuzzy context handler. | 6.86% |
| ABAC with non-Personalized Fuzzy context handler. | 17.31% |
| Baseline ABAC. | 17.74% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Psarra, E.; Apostolou, D.; Verginadis, Y.; Patiniotakis, I.; Mentzas, G. Context-Based, Predictive Access Control to Electronic Health Records. Electronics 2022, 11, 3040. https://doi.org/10.3390/electronics11193040
Psarra E, Apostolou D, Verginadis Y, Patiniotakis I, Mentzas G. Context-Based, Predictive Access Control to Electronic Health Records. Electronics. 2022; 11(19):3040. https://doi.org/10.3390/electronics11193040
Chicago/Turabian StylePsarra, Evgenia, Dimitris Apostolou, Yiannis Verginadis, Ioannis Patiniotakis, and Gregoris Mentzas. 2022. "Context-Based, Predictive Access Control to Electronic Health Records" Electronics 11, no. 19: 3040. https://doi.org/10.3390/electronics11193040
APA StylePsarra, E., Apostolou, D., Verginadis, Y., Patiniotakis, I., & Mentzas, G. (2022). Context-Based, Predictive Access Control to Electronic Health Records. Electronics, 11(19), 3040. https://doi.org/10.3390/electronics11193040