1. Introduction
Diabetic foot ulcer is a tough issue for both the clinical practitioners and the patients since it is a chronic wound, which is affected by many factors, resulting in the expansion of ulcer and infection. Further exacerbation may lead to invasive debridement for the poorly healing wound, or even amputation for necrotic tissues. This does not only affect the patient’s health condition and quality of life, but also increases the inpatient length of stay, medical expenses, and may lead to mortal sepsis. Therefore, the condition of a diabetes foot ulcer should be detected early, and minor lesions of patients’ extremities should also be noticed in advance.
The most important principle of chronic wound care is to continuously follow-up the wound healing condition to reduce the risk of persistent wound infection [
1]. According to the wound care treatment guideline announced by EWMA (European Wound Management), traditional chronic wound care must be treated with topical treatment by daily inspection (naked-eye observation) of the wound healing status when changing dressings, by surgeons, doctors, or nurse specialists; in other words, those who have performed surgical debridement or operation, suture, or skin graft, etc., to the patient. Therefore, the first impression of the wound will be observed through visual observation and should follow the rules of MOIST (Moisture balance, Oxygen balance, Infection control, Support treatment, and Tissue management) of the wound surface [
2]. That means visual observation to the wound bed surface is the most important part of wound care. For example, if the wound is too dry, it will be treated with wound gels, and if the wound is overly moist or surrounded by fluid, it will be treated with foams, hydro-fibers, or alginates for absorption to ensure a balanced moisture level, which may facilitate the formation of granulation tissue. Additionally, a paper ruler and marker pen may be used to measure and mark down the margin of the infected areas. A cotton swab may be used to measure the depth and the condition of wound discharge. Additionally, the details of the wound bed are observed, such as blood (active bleeding, blood clot, etc.), pus (infection wound or abscess, etc.), and other tissue fluid. Finally, the surgeon will prescribe the wound dressing or ointment for wound healing, such as antibiotics ointment for the infected wound, or hyperbaric oxygen therapy (HBO) as a kind of treatment for the wound care procedure.
According to MOIST, besides observing the formation of the granulation tissues, the complex pathophysiology of excess and unhealthy granulation induced by infection, oxygen supply should also be considered since the wound healing process in DM patients with multiple, complicated wounds may be affected [
3].
Due to the limitations in the traditional wound care procedures which rely on professional experiences, naked-eye assessment, and manual wound determination of necrotic, sloughing, and granulation tissue, a computational approach is highly suggested as a scientific method to identify tissue and to correctly predict the healing condition of the chronic wound [
4]. Relevant studies have confirmed that the diabetic foot medical care model is very sophisticated and requires cross-disciplinary cooperation through the integration of medicine (metabolism, infectious, surgery, orthopedics), nursing, digital technology, and biomedical engineering, etc., to joint efforts. With cross-disciplinary cooperation, optimal wound management can be achieved by managing the glycemic control and wound care with the assistance of modern informatics and communication technologies [
5].
Nowadays, electronic products and related communication devices, such as cellphones, wearable devices, tablet computers, consumer electronics, etc., have become very common in peoples’ lives. Cellphones’ built-in cameras with high resolution have begun to be used in managing chronic wounds, for example in diabetic foot care [
6]. It can quickly achieve the ability of screening and judging the wound condition. Some research found practical value in the actively developing digital assessment tools. According to the research of Australian scholars, the particularity of diabetic wounds’ detection apps can lead to variable reliability and validity of images captured by mobile devices. Interpretation of wound images in distal assessment does not exclude the risk of distortion. However, it is still recommended as a screening or diagnostic appliance [
7].
Therefore, through the modern information and communication technologies, mobile phone camera software can act as an assessment tool to analyze the preliminary diabetic foot screening. Monitoring the early pathological changes of the ulcer wound and understanding the quality of wound care at home during the COVID-19 pandemic can help to reduce the medical cost of serious infection and prevent the outcome of amputation to achieve effective diabetes health management, which is an important issue nowadays.
According to the epidemiological statistics, more than 80% of DM foot ulcers lead to amputation [
8]. Usually, through debridement of the surrounding callus, removal of slough and necrotic tissue, and scraping of the microbial membrane (biofilm) on the wound surface, the new granulation tissue can proliferate and promote wound healing [
9,
10]. Besides, removing the physically inappropriate shear forces of the patients’ feet, choosing the suitable dressing, applying topical oxygen supply, and providing related growth factors to stimulate the growth of granulation tissues are recommended treatments for diabetic foot ulcers according to the guidelines [
10].
Through retrospection, literature about wound identification systems for diabetic foot ulcers has been recorded by Wang et al., who used real-time wound image data with a deep learning algorithm [
11]. A recent systematic review concluded that the results of the research in AI wound assessments and monitoring systems are useful to improve DM foot clinical care, but some of them were focused on how to recognize ischemia and infection while providing strong validation or adequate reliability in assessing ischemia [
12]. They use images taken by cellphone cameras to identify wounds through image smoothing and image segmentation, especially with good validity to identify the wound size and ischemic tissues [
13]. However, a knowledge gap exists in the measurement of the extent of the ulcers, the differential diagnoses of the tissues, and the estimation of wound recovery. These are important focuses in the wound healing process, especially for the growth of the granulation tissues.
In recent years, almost every country in the world has been impacted by COVID-19. COVID-19 has affected the public’s lives in various ways, including their health, living environments, and social networks. Most importantly, the working burden of medical staff increased while the willingness of patients to seek medical treatment decreased, thus causing a rise in amputation rates among DM foot ulcer patients.
For this reason, this study aims to develop and test an AI detection model as a screening tool by using an active learning method to identify the growth of granulation tissue and to understand the wound healing status of the DM foot ulcer wound bed for home care patients, especially during the COVID-19 pandemic.
3. Results
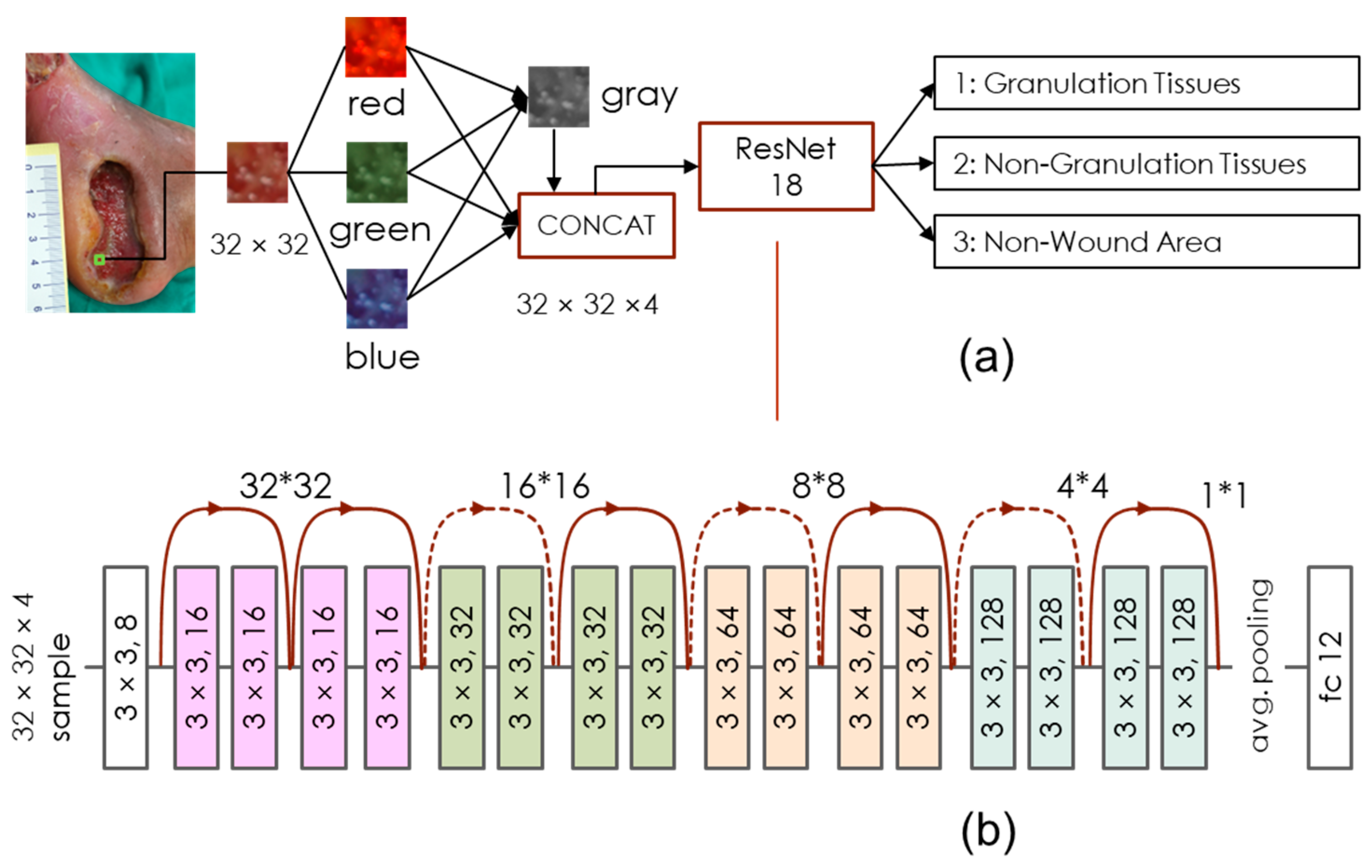
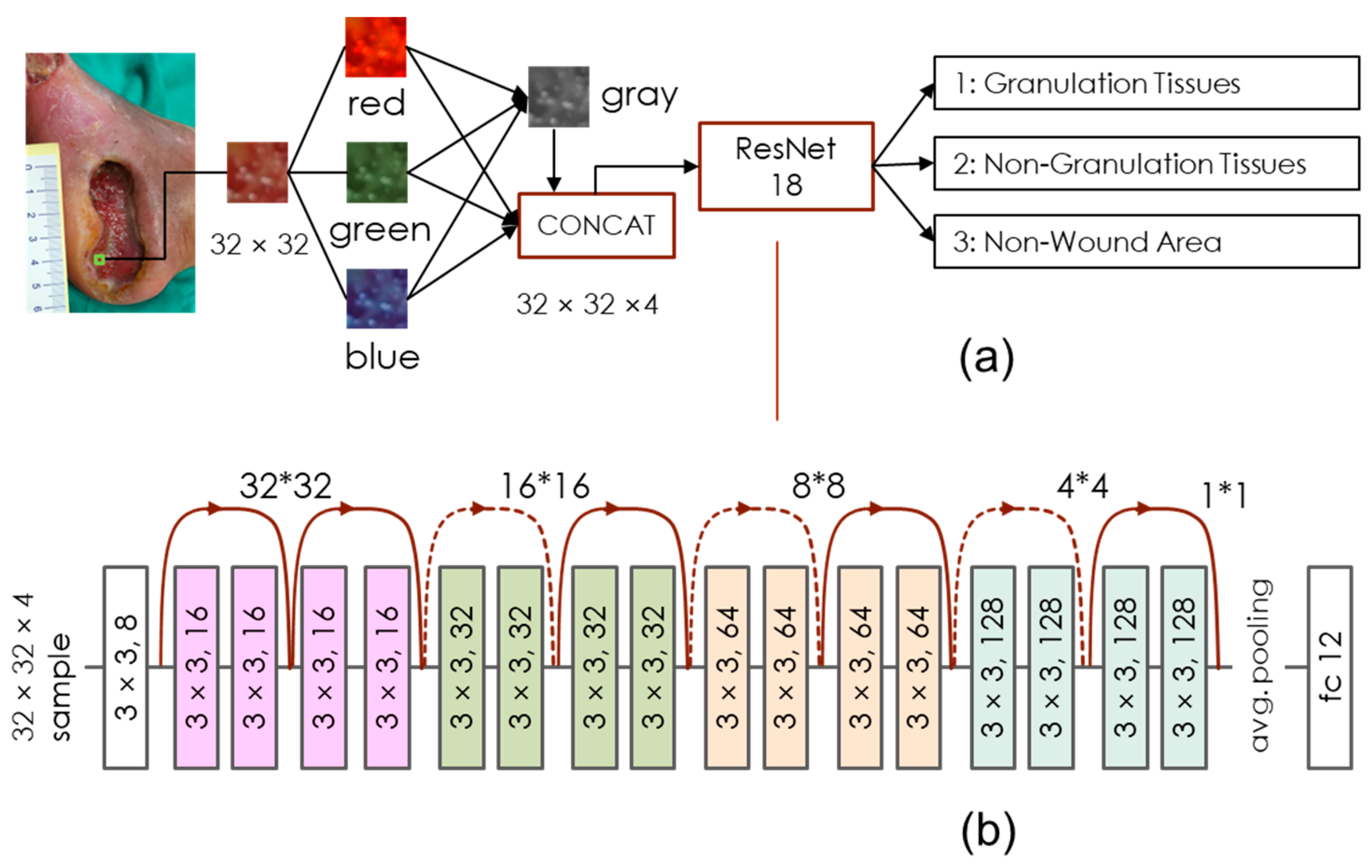
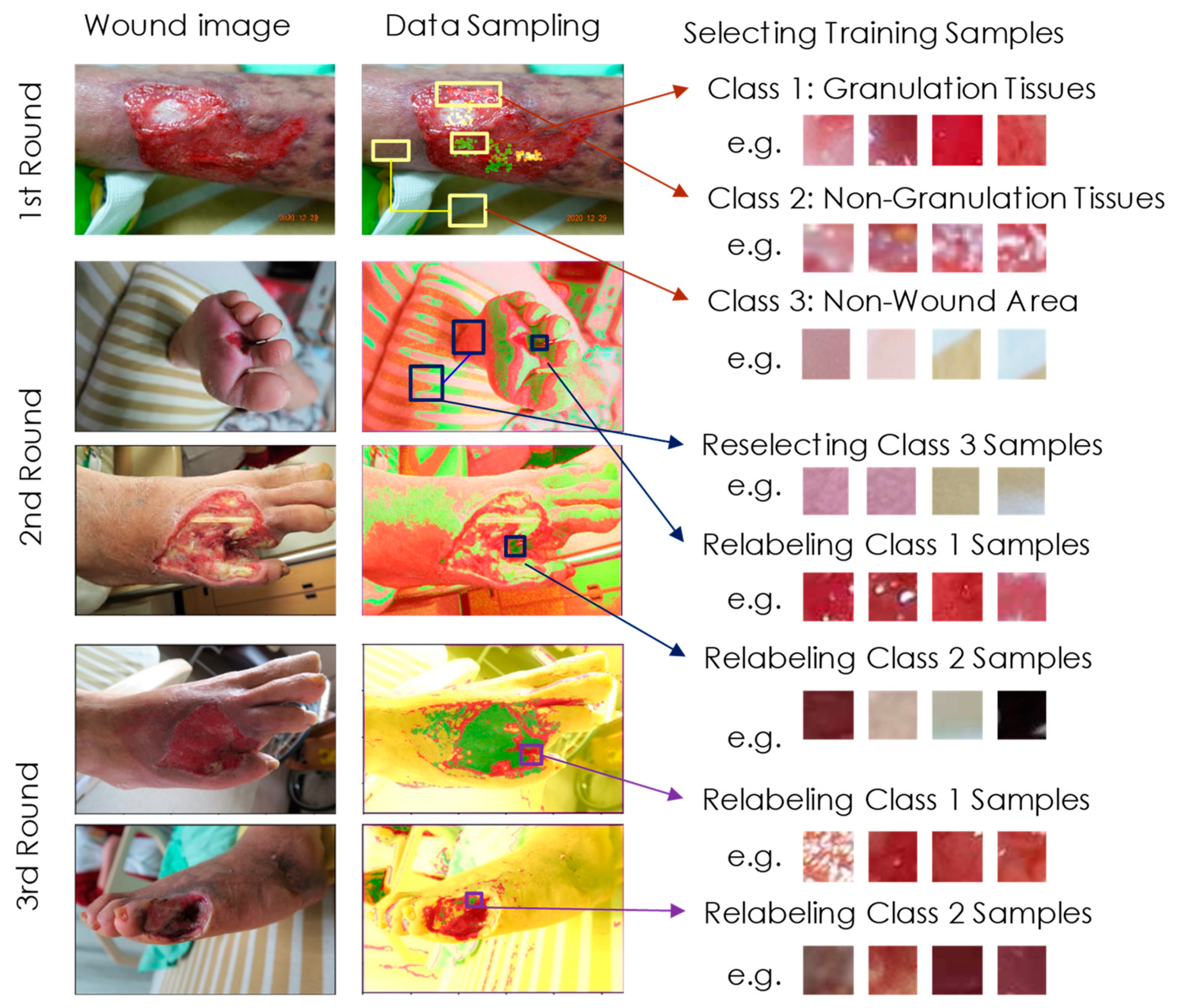
As mentioned above, after three rounds of active learning, we kept nine uninvolved wound images. These images were from three patients, called Case 1 (1-1, 1-2, 1-3), Case 2 (2-1, 2-2, 2-3), and Case 3 (3-1, 3-2, 3-3). Clearly, each case went through a three-stage healing process. Of these cases, the first two had larger areas and more complex wound beds compared to case 3. The picture resolutions for these images are 150, 300, and 300 dpi, respectively, for each case. We applied our detection model to evaluate each 32 × 32 block and then used Equation (1) to identify regions of granulation tissue pixel-by-pixel. We only focused on class 1 results, as the granulation tissue growth indicated good wound healing. Clinical specialists had also labeled the ground truth for us to verify our experimental results.
Table 2 lists the IOU rates between our detection results and ground truth. For all cases, we can find that the IOU rate increased during the first, second, and third resampling, implying that active learning can efficiently improve training performance. The IOU rates after the third round of training were mostly higher than 0.5, except for case 2 and 3 which was only 0.45, and the average IOU rate reached 0.62. We also tested 10 over 52, 10 over 78, and 10 over 80 images using the well-trained model on all 3 training datasets after the third round. The images were picked randomly and had mean IOUs of 0.71, 0.67, and 0.68, respectively. Although these images have been used to train our model, the active learning process does not globally examine all image content. Therefore, the IOU rates of the training data were not significantly better than the IOU rate of the final test images. This result likely confirms the generality of our model. An IOU rate above 0.5 met the original goal of our study, revealing the ability of our detection model to aid caregivers in DM foot wound healing. Below, we use
Figure 3,
Figure 4 and
Figure 5 to explain the details of wound assessment for cases 1–3, respectively. Notably, the following cases provided the representative images of common DM foot ulcer wound status.
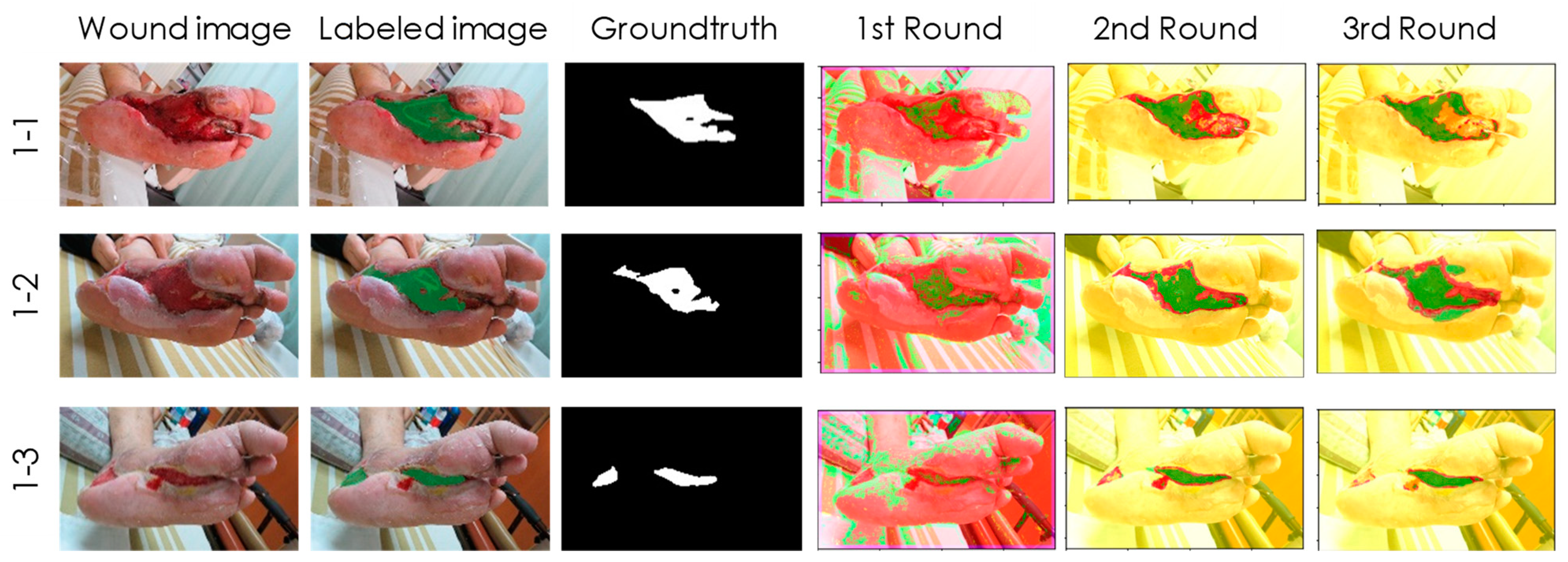
Case 1 (
Figure 3) is a male patient aged 65 who has been diagnosed with Type 2 DM for 8 years. In the past 5 years, he suffered from DM neuropathy and cerebrovascular disease. He fell from his wheelchair and was injured by the pedal of the wheelchair. After debridement and wet dressing of Sulfasil cream and skin graft, the granulation tissue gradually grew hyperplastic micro-vessels, fibrous connective tissue, and many inflammatory cells. This tissue has a large network of micro-vessels, so the color appears red with slight hemorrhage, and the periphery is a new epidermis that has completed re-epithelialization. The wound was getting smaller and healing. Although the IOU rate was around 0.6, the detection results in
Figure 3 precisely indicate the location and area of the granulation tissue after the second and third training sessions. Therefore, it has been affirmed by doctors and nurse specialists.
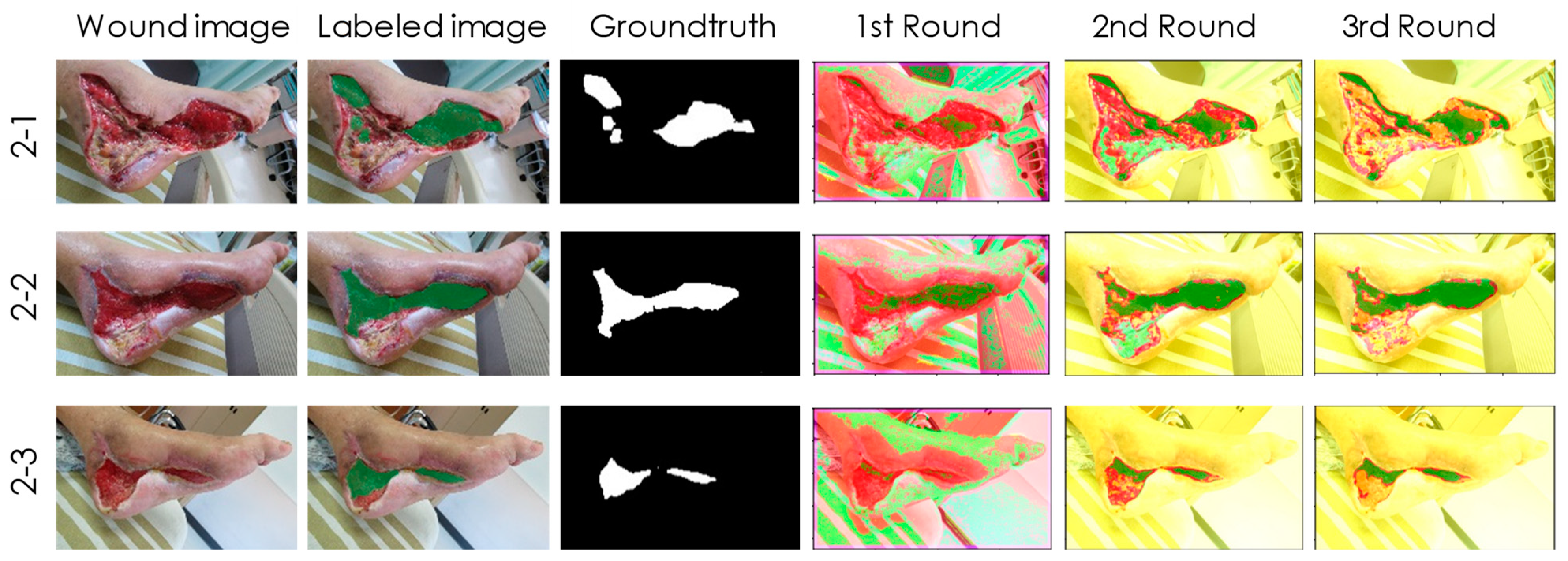
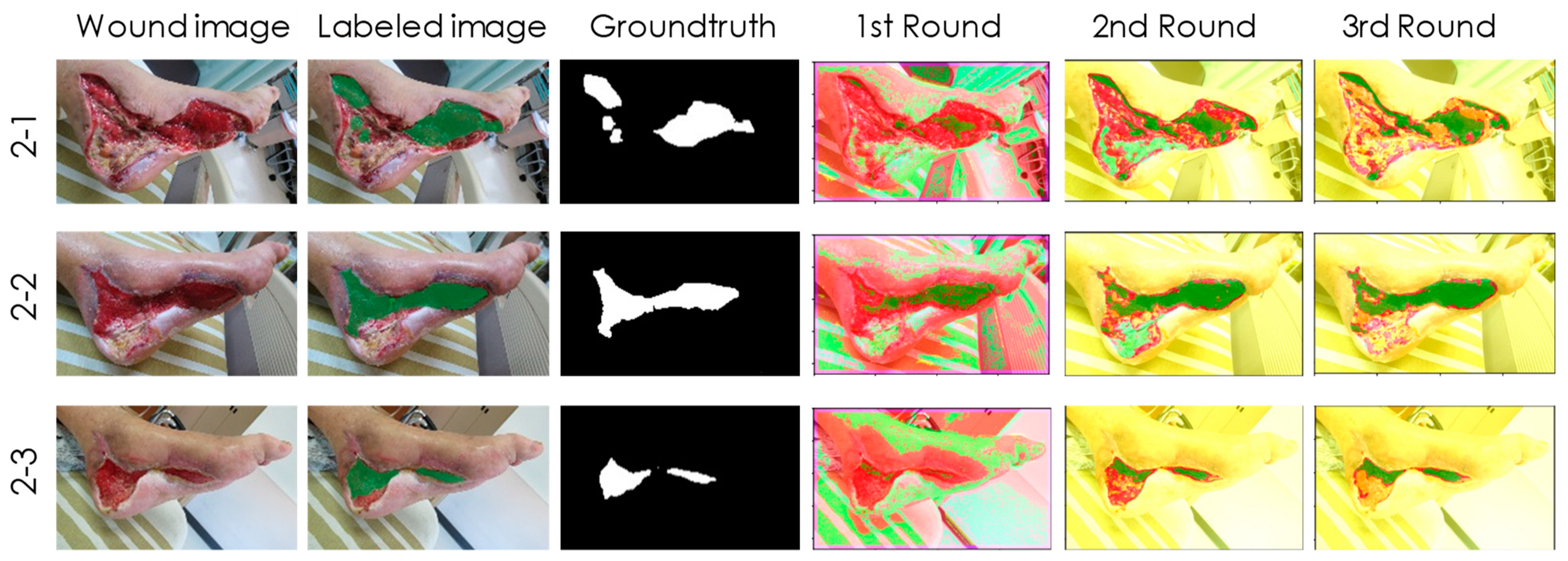
Case 2 (
Figure 4) is a 68-year-old, retired truck driver with poor DM control for more than 20 years. He has been diagnosed with DM nephropathy and undergoes regular dialysis three times a week. He suffered a motorcycle injury and laceration within two weeks. The plastic surgeons debrided a large area of infected, humid wound, followed by using Sulfasil cream and New Epi (growth factor) liquid wound dressing after debridement of inflammation and necrotic tissue, and then performed skin grafting. These treatments significantly improved wound healing with granulation tissue hyperplasia. The healing process is also traced by our detection model in
Figure 4. Interestingly, we found that the wound area near the heel was incorrectly classified from class 2 (non-granulation tissues) to class 3 (non-wound areas) after the third training session. However, this situation did not affect our detection for class 1 (granulation tissues).
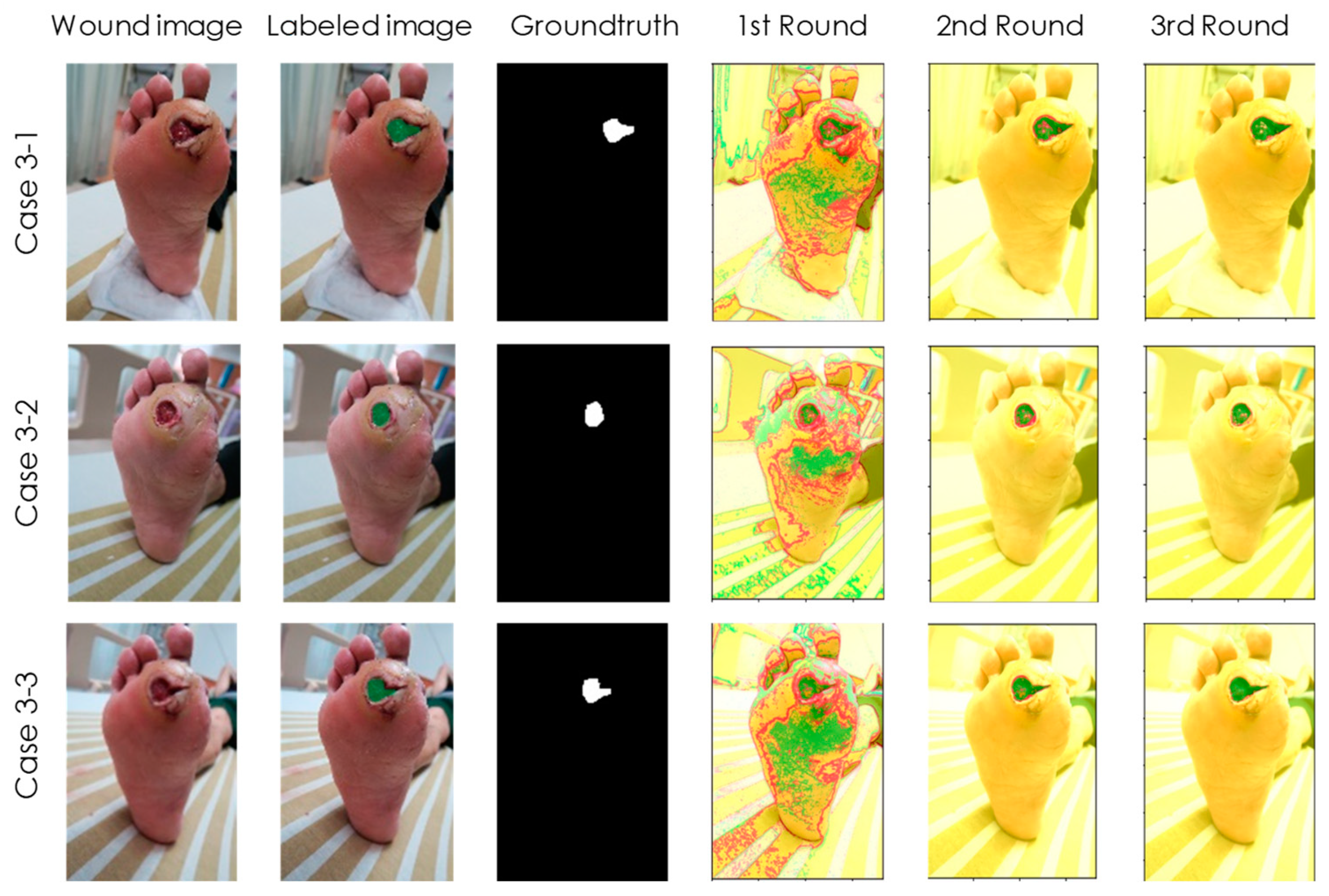
Case 3 (
Figure 5) is a 59-year-old female patient with a history of DM for over 15 years who was recently diagnosed with a poorly healing ulcer under the left toe. The wound looks small on the outside, but it is actually a deep, infected wound. After debridement, due to chronic renal insufficiency and neuropathy, osteomyelitis led to poor wound healing, which eventually led to toe amputation. In this case, our detection model accurately tracked the wound appearance on the outside, but it was unable to delve into the back of the skin, as shown in
Figure 5. Therefore, early warning cannot be given to prevent unfortunate events from happening.
4. Discussion
As mentioned earlier, our initial goal for this study was that the IOU rate must be higher than 0.5 compared to the ground truth. Although all our experimental results, except for case 2 and 3, achieved this goal, we are curious why the IOU cannot reach 0.8, 0.9, or higher. We think there are two possible reasons. First, for some tissue samples, it can be difficult to definitively determine whether it is a granulation tissue based on their appearance. Any decision may be the correct classification. In this case, half of the ambiguous samples can be placed outside the intersection area of the IOU.
The second reason may be that the class 2 (non-granulation tissues) has various types, such as infected abscess, hemorrhage, skin graft, blood clot, fascia, etc. As long as the granulation tissue appears to be close to these types, it may be misclassified. Therefore, the conditions for the successful classification of granulation tissues are relatively strict. To confirm this argument, we set the pixels within the granulation tissues of the ground truth image to be positive and other pixels to be negative, and then calculated the positive predictive value (PPV) of the experimental results. We found that even for case 2-3 (with IOU = 0.45), its PPV value reached 0.91. Therefore, our detection results could accurately determine the location of the granulation tissues.
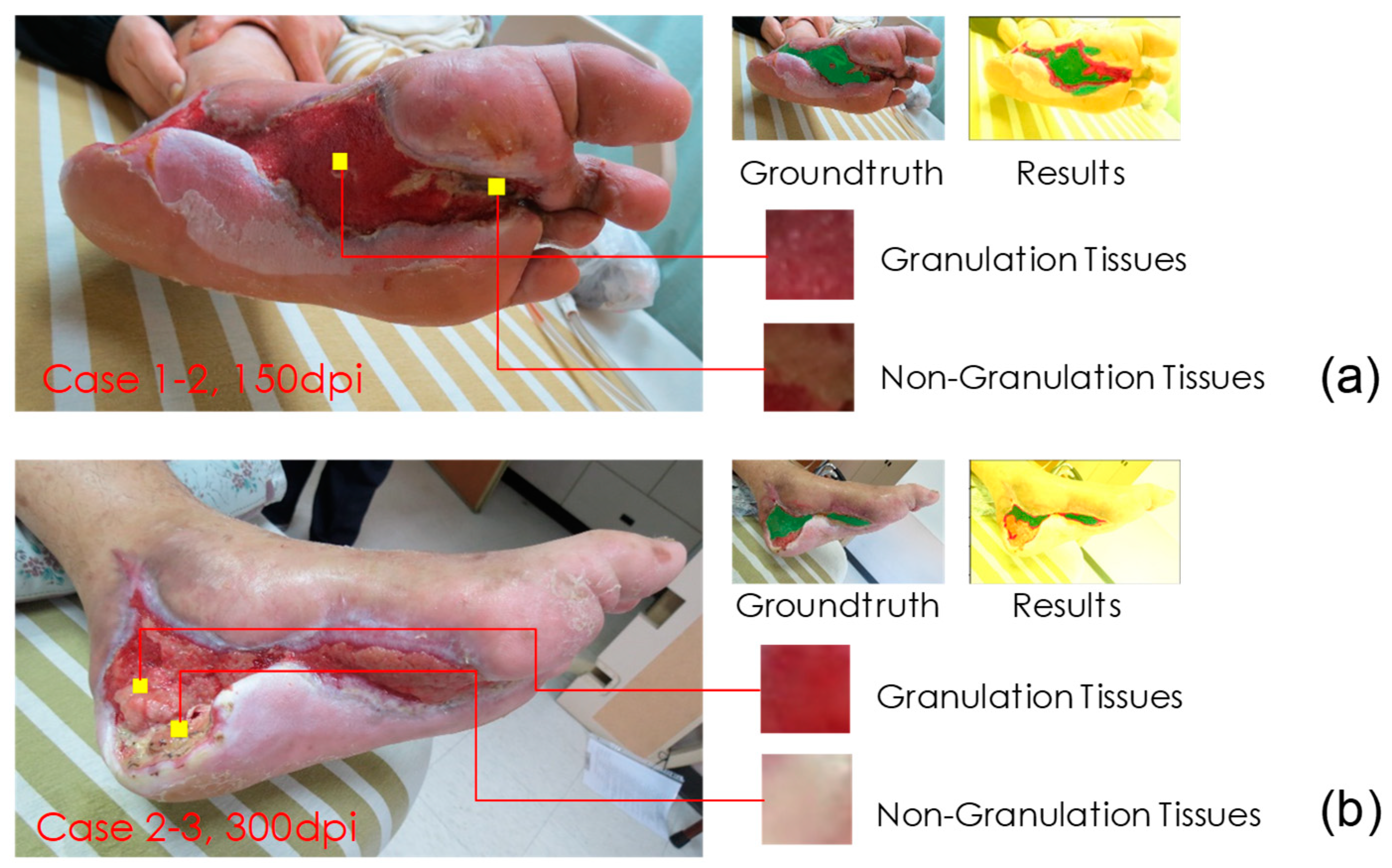
We also attempted to precisely detect non-granulation tissues (class 2) in our further research. By doing so, we can assess the proportion of granulation tissues in the wound bed. Here, let us discuss why we could not properly identify non-granulation tissues in case 2 and 3. As a comparison, we also review the successful detection example of case 1-2. We found that the main difference between these two cases is the resolution of the images. The image resolutions were 150 and 300 dpi for cases 1-2 and 2-3, respectively. These two images are compared in
Figure 6. In
Figure 6a, both granulation tissue and non-granulation tissue are clearly textured, while in
Figure 6b, the texture of both is relatively flat and approximates the appearance of class 3. Therefore, in the upcoming research, we can resize all images to a consistent resolution to improve training results.
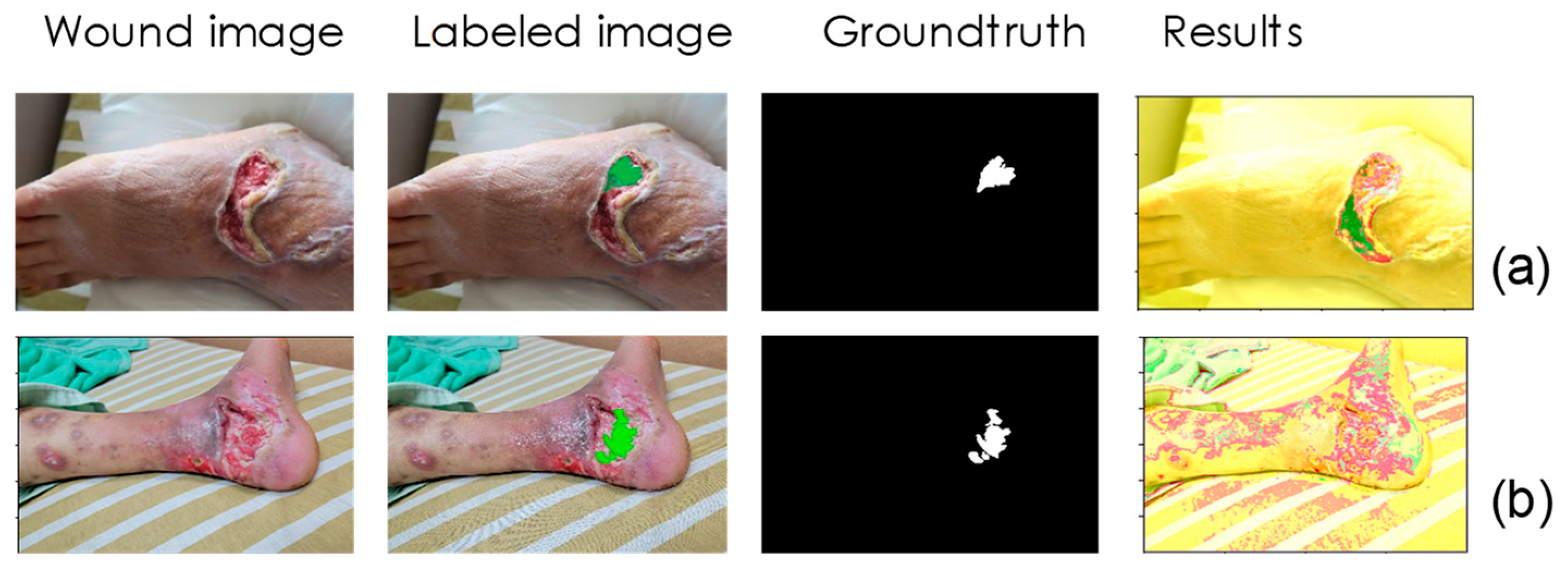
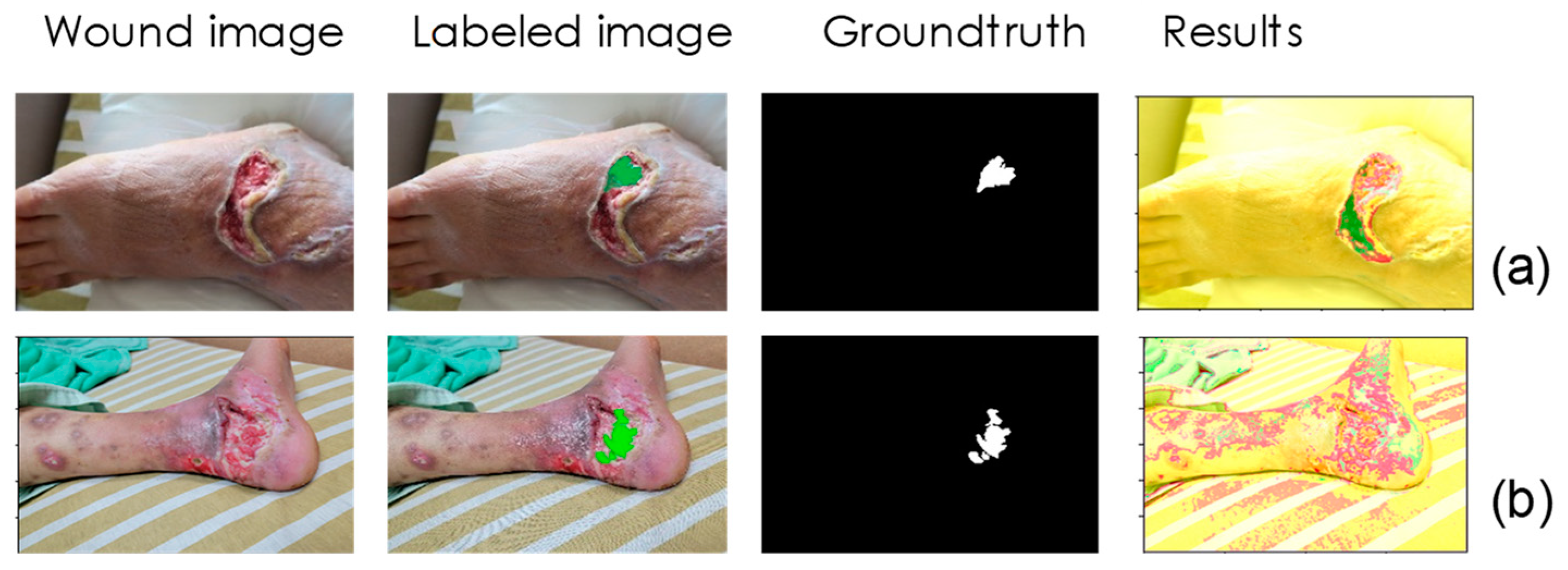
In addition to image resolution, we found other factors that contributed to misclassification. We removed images in the training data that could not be classified correctly even though they were used for training. As shown in
Figure 7a, wetter tissue is more likely to reflect light when photographed, thereby affecting the detection model.
Figure 7b is another example, which shows that in more complex wounds, granulation is not easily correctly detected due to mixing with other tissues. For the former, we can take several more images of different angles during detection to solve the reflection problem. For the latter, we can collect more training data—a fourth round of active learning may be performed to solve this problem.
5. Conclusions
In this research, we developed and tested a granulation tissue detection model. The kernel of this model is a simplified ResNet 18 network model, which consumes relatively few computing resources and thus can perform on basic mobile devices. The input data were 32 × 32 sub-images segmented from DM wound pictures, and the classification output was divided into three classes, i.e., the granulation tissues, non-granulation tissues, and non-wound areas. We conducted a three-round active learning process to save the labeling labor and to improve training efficiency. The experimental results revealed that most of our detection results of the granulation tissues had an IOU higher than 0.5 in comparison to the ground truth. The results can thus accurately locate the place of the granulation tissues in the wound bed. This is helpful to both the nursing staff and the DM patients’ wound healing, especially during the outbreak of COVID-19.
This research constructed a mHealth device and application for patients with DM foot ulcers or chronic wounds. The present R-CNN deep machine learning model for instant diabetes foot ulcer wound imaging, for wound classification and identification, contributes quickly and sufficiently to identify the wound condition by using photo image delivery from cellphones, especially for those patients who were hesitant to visit the doctor during the COVID-19 pandemic. Furthermore, this model provides patients, healthcare professionals, and case managers a tool for the assessment of the wound status. It can be used for self-monitoring by patients, taking pictures of wounds, and uploading the pictures to the e-health cloud as a personalized medical record, as well as it can break the limitations and inequality of medical services such as time and geography. Medical staff can also use the App to view all medical data and personalized information of patients, such as blood test results and images reports, immediately communicate and discuss with each other through the App at any time, and hence increase the medical care efficiency. If there is any abnormality, the App will immediately send a warning message notification to prevent critical conditions or to decrease the possibilities of amputation induced by wound infection.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}